

Abstract
Background:
Hemifacial spasm (HFS) caused by vertebral artery (VA) aneurysms is rare. Several cases of HFS caused by VA aneurysms treated by endovascular parent artery occlusion (PAO) have been reported. Recently, we treated a rare case of HFS caused by a saccular VA aneurysm at the bifurcation of the posterior inferior cerebellar artery (PICA), which was successfully treated by endovascular coil embolization, preserving the parent artery, and PICA. We discuss endovascular treatment for HFS induced by VA aneurysms with a literature review.
Case Description:
A 59-year-old man presented with the left HFS persisting for 2 months. Magnetic resonance imaging revealed a left saccular VA-PICA aneurysm and demonstrated that a left facial nerve was compressed by the aneurysm at the root exit zone. Angiography revealed that the PICA was branching from the aneurysm neck. Endovascular coil embolization was performed using the balloon remodeling technique to preserve the left VA and PICA. HFS disappeared after treatment.
Conclusion:
Although microvascular decompression was commonly accepted for the standard treatment of HFS, coil embolization of aneurysms without PAO may be an effective treatment for HFS caused by VA aneurysms.
Keywords: Aneurysm, Coil embolization, Endovascular treatment, Hemifacial spasm, Vertebral artery

INTRODUCTION
Hemifacial spasm (HFS) is usually caused by compression of the facial nerve at the root exit zone (REZ) with branches of the vertebrobasilar system or tortuously elongated vertebral artery (VA) itself. On the other hand, a VA aneurysm is a rare cause of HFS. Eight cases of HFS caused by VA aneurysms treated by endovascular therapy have been reported in English.[1,10,11,14-16,19,20] Recently, we encountered a case of HFS caused by a saccular VA aneurysm at the bifurcation of the posterior inferior cerebellar artery (PICA), and successfully treated by endovascular simple coil embolization with preservation of the VA and PICA. In this report, we describe our treatment of the patient and discuss endovascular treatment for HFS induced by VA aneurysms with a literature review.
CASE DESCRIPTION
A 59-year-old man with hypertension and diabetes mellitus was referred to our hospital with a 2-month history of the left HFS. The patient had no neurological deficit except for left HFS. There was no episode of severe occipitalgia to suggest VA dissection. Magnetic resonance angiography (MRA) demonstrated a left saccular VA aneurysm, and the left VA was dominant [Figure 1a]. The VA aneurysm compressed the REZ of the facial nerve on magnetic resonance imaging (MRI)-constructive interference in a steady-state [Figure 1b]. A left saccular VA aneurysm with a diameter of 5.5 mm was found on angiography and the PICA arose from the aneurysm neck [Figure 2]. No findings indicating VA dissection, such as intimal flap or double lumen, were observed. Based on these findings, the HFS due to compression of the REZ by the VA-PICA aneurysm was diagnosed. Prevention of aneurysm rupture and treatment of HFS were considered. Although several reported cases were treated by endovascular parent artery occlusion (PAO), PAO was unable to be performed in our case because the left VA was dominant and the PICA arose from the aneurysm neck. Clipping of the VA-PICA aneurysm, followed by additional microvascular decompression (MVD), was considered not easy, because the lesion was located in the paramedian region and there may be small perforating branches from VA in this area. Thus, we initially planned to perform endovascular coil embolization with preservation of the VA and PICA to prevent aneurysm rupture. Then, if HFS did not disappear after treatment, MVD was planned.
Figure 1:
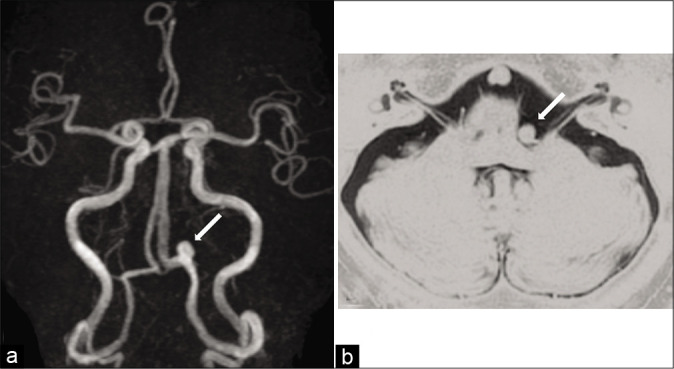
(a) Magnetic resonance angiography showing a left saccular vertebral artery (VA) aneurysm (arrow). (b) Magnetic resonance imaging-constructive interference showing that the left side of the pons and root exit zone of the facial nerve are compressed by a VA aneurysm (arrow).
Figure 2:
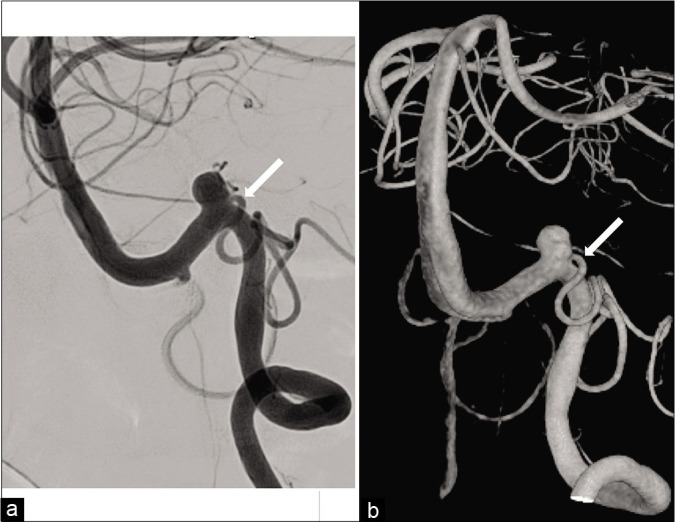
Angiography showing the left posterior inferior cerebellar artery originating from the aneurysm neck (arrow). (a) Conventional image, (b) Three-dimensional rotational angiography.
Antiplatelet drug administration of aspirin at 100 mg/day and clopidogrel at 75 mg/day was started 1 week before treatment. Procedures were performed under general anesthesia. An 8-Fr. long sheath introducer was inserted into the right femoral artery. Systemic heparinization was introduced and the activated clotting time was maintained at 200–250 s. A 6-Fr. guiding catheter (FUBUKI, Asahi Intecc, Aichi, Japan) was guided into the left VA. Coil embolization was performed by the balloon-assisted technique to preserve the left PICA and VA. A balloon catheter (Scepter XC, 4 × 11 mm, Terumo, Tokyo, Japan) was advanced into the VA distal to the neck of the aneurysm, and a microcatheter (Excelsior SL-10, Stryker, Kalamazoo, MI, USA) was inserted into the aneurysm using a microguidewire (CHIKAI 14, Asahi Intecc). A platinum coil (Target 360 soft, 5 mm × 10 cm, Stryker) as the first coil was deployed in the aneurysm after the micro-balloon was placed at the aneurysm neck and inflated. A total of 12 coils were inserted serially, and the aneurysm was obliterated while preserving the PICA and parent artery [Figure 3].
Figure 3:
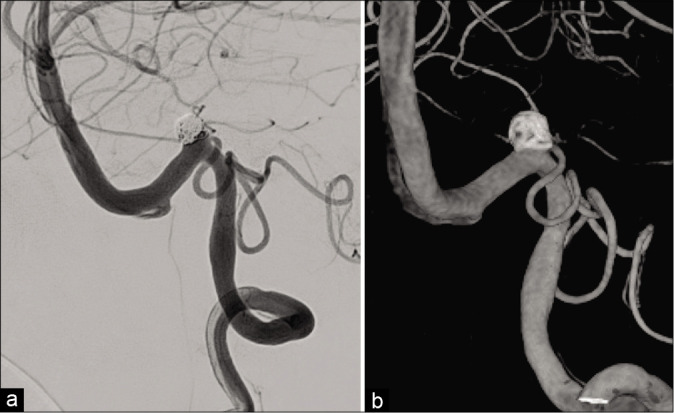
Postoperative angiography showing obliteration of the aneurysm, and preservation of the vertebral artery and posterior inferior cerebellar artery. (a) Conventional image, (b) Three-dimensional rotational angiography.
His postoperative course was uneventful. No new neurological symptoms developed, and ischemic lesions were not identified on diffusion-weighted MRI. The spasm of the left eyelid muscle persisted on the day of surgery. The frequency of HFS decreased the next day after treatment, and HFS disappeared 2 days later. Postoperative MRA demonstrated no blood flow within the aneurysm [Figure 4]. HFS has not recurred for 1 year after treatment.
Figure 4:
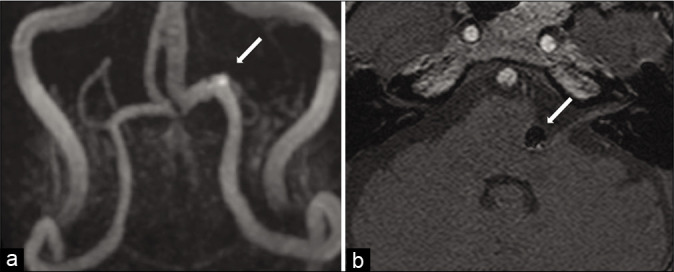
Magnetic resonance angiography (MRA) showing no blood flow in the aneurysm (arrow). (a) MRA reconstructed image, (b) A raw image.
DISCUSSION
HFS is usually caused by compression of the facial nerve REZ where the central and peripheral myelin connects. The cause of compression is generally vessels, and occasionally tumors,[9] hemangiomas,[2] cerebral arteriovenous malformations,[8] or aneurysms. HFS caused by a VA aneurysm is rare with an incidence of 0.2–0.5%.[22] Several reports describing direct surgery as treatment have been published.[3,4,12,13,17,22-24] However, endovascularly treated cases were rare, and only nine, including ours, have been reported in English [Table 1].[1,10,11,14-16,19,20] Of these nine cases, six were successfully treated by endovascular PAO. The treatment options of endovascular PAO were embolization of VA including the aneurysm in three cases,[10,16,20] embolization on the proximal VA alone in one case,[15] and trapping of VA without embolization of the aneurysm in two cases.[11,14] One case of HFS induced by a VA aneurysm was treated by endovascular flow diversion.[19] Arisawa et al. reported a case of HFS caused by a VA-PICA aneurysm, which was treated by stent-assisted coil embolization.[1] In their case, although complete disappearance of symptoms was not achieved, HFS markedly improved after treatment. Endovascular PAO may be an effective radical treatment for HFS. However, it cannot be performed on all patients due to anatomical variations. In our patient, the left VA was dominant and the left PICA arose from the aneurysm neck. Therefore, we performed endovascular coil embolization of the aneurysm while preserving the VA and PICA. As a result, HFS was ameliorated after treatment without MVD.
Table 1:
Summary of cases of HFS caused by a VA aneurysm treated endovascularly.

HFS commonly disappears immediately after direct surgery, such as MVD,[22,24] whereas endovascular treatment requires time for HFS to improve. Regarding endovascular PAO, it takes 3–6 months to improve symptoms after treatment in five cases. On the other hand, in our patient, HFS disappeared within 2 days after treatment. Kugai et al. reported that HFS disappeared immediately after endovascular PAO.[10] Interestingly, patients who recovered nearly immediately after treatment had shorter intervals between symptom onset and endovascular occlusion than patients who experienced gradual improvement over time [Table 1]. Moreover, Arisawa et al. reported that HFS slightly recurred 1 month after stent-assisted coil embolization and complete disappearance of HFS could not be obtained. In their case, the length of HFS before treatment was 3 years.[1] Although the nerves are different, Gu et al. reported that the length and degree of oculomotor nerve palsy (ONP) before treatment had significant relation to recovery of oculomotor nerve function.[5] In cases of HFS, the duration of symptoms before treatment may also be related to complete HFS recovery and their time to resolution.
In our case, reduction of compression was not achieved, but HFS disappeared after coil embolization. It was suggested that pulsation rather than compression has more influence on HFS. In cases of ONP, Guresir et al. reported that the rate of complete ONP resolution did not differ between patients undergoing simple clipping and those who underwent clipping with nerve decompression, and the resolution of ONP is inversely correlated with the initial severity of ONP.[6] Other recent studies found that resolution of symptoms was achieved by endovascular treatment, and the pulsation has more influence on cranial nerve dysfunction than direct compression.[5,7,18]
Santiago-Dieppa et al. reported a case of endovascular flow diversion for a VA aneurysm inducing HFS.[19] They suggested that pulsation plays a more important role than compression in pathogenetic mechanisms of HFS. The placement of the flow diverter induced the decrease of hemodynamic flow into the aneurysm and resolved nerve irritation. Thus, the improvement of neuropathy was considered to result from the reduced intra-aneurysmal flow. Suzuki et al. reported a successful case of endovascular coil embolization of a VA-PICA aneurysm causing facial nerve palsy.[21] They evaluated the association of aneurysmal wall pulsation and cranial nerve dysfunction using fluid structure interaction and indicated that aneurysmal wall motion and pulsations at the facial nerve fibers in the pons played an important role in facial nerve palsy. They performed simple coil embolization of the VA-PICA aneurysm preserving PICA, and fascial nerve palsy was completely improved 1 month after the treatment. Although our patient presented HFS, not facial nerve palsy, the improvement of HFS after coil embolization may have been related to reduced flow into the aneurysm and pulsation of the aneurysmal wall.
CONCLUSION
HFS caused by VA aneurysms is rare. Although coil embolization of the aneurysm was unable to reduce compression, HFS caused by the VA-PICA aneurysm improved after endovascular treatment. HFS was suggested to be mainly induced by pulsation of a VA aneurysm rather than direct compression of the REZ, and coil embolization of such aneurysms without PAO may be an effective treatment.
Footnotes
How to cite this article: Iida Y, Mori K, Kawahara Y, Fukui I, Abe K, Takeda M, et al. Hemifacial spasm caused by vertebral artery aneurysm treated by endovascular coil embolization. Surg Neurol Int 2020;11:431.
Contributor Information
Yu Iida, Email: yuiida1204@gmail.com.
Kentaro Mori, Email: squad1979@me.com.
Yosuke Kawahara, Email: yosuke0815@gmail.com.
Issei Fukui, Email: i-fukui@yokohamasakae.jp.
Katsuya Abe, Email: fu.kuluton.8@gmail.com.
Mutsuki Takeda, Email: januarytks@yahoo.co.jp.
Tastu Nakano, Email: tatsu_nkn@yahoo.co.jp.
Hiroki Taguchi, Email: taguchi-clinic@mocha.ocn.ne.jp.
Motohiro Nomura, Email: nomura413jp@yahoo.co.jp.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Arisawa K, Ochi T, Goto Y, Nanbu S, Shojima M, Maeda K. Coil embolization of VA-PICA aneurysm presenting with hemifacial spasm with assistance of abnormal muscle response monitoring. J Neuroendovasc Ther. 2020;14:146–50. doi: 10.5797/jnet.cr.2019-0012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Asaoka K, Sawamura Y, Tada M, Abe H. Hemifacial spasm caused by a hemangioma at the geniculate ganglion: Case report. Neurosurgery. 1997;41:1195–7. doi: 10.1097/00006123-199711000-00036. [DOI] [PubMed] [Google Scholar]
- 3.Choi SK, Rhee BA, Park BJ, Lim YJ. Hemifacial spasm caused by fusiform aneurysm at vertebral artery-posterior inferior cerebellar artery junction. J Korean Neurosurg Soc. 2008;44:399–400. doi: 10.3340/jkns.2008.44.6.399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Furtado SV, Thakar S, Saikiran NA, Hegde AS. Hemifacial spasm and jugular foramen syndrome caused by diametrically opposite aneurysms on the vertebral artery. Neurol Sci. 2013;34:1809–10. doi: 10.1007/s10072-012-1280-x. [DOI] [PubMed] [Google Scholar]
- 5.Gu DQ, Luo B, Zhang X, Long XA, Duan CZ. Recovery of posterior communicating artery aneurysm-induced oculomotor nerve paresis after endovascular treatment. Clin Neurol Neurosurg. 2012;114:1238–42. doi: 10.1016/j.clineuro.2012.03.016. [DOI] [PubMed] [Google Scholar]
- 6.Guresir E, Schuss P, Seifert V, Vatter H. Oculomotor nerve palsy by posterior communicating artery aneurysms: Influence of surgical strategy on recovery. J Neurosurg. 2012;117:904–10. doi: 10.3171/2012.8.JNS111239. [DOI] [PubMed] [Google Scholar]
- 7.Hassan T, Hamimi A. Successful endovascular management of brain aneurysms presenting with mass effect and cranial nerve palsy. Neurosurg Rev. 2013;36:87–97. doi: 10.1007/s10143-012-0404-3. discussion 97. [DOI] [PubMed] [Google Scholar]
- 8.Konan AV, Roy D, Raymond J. Endovascular treatment of hemifacial spasm associated with a cerebral arteriovenous malformation using transvenous embolization: Case report. Neurosurgery. 1999;44:663–6. doi: 10.1097/00006123-199903000-00130. [DOI] [PubMed] [Google Scholar]
- 9.Kudo A, Suzuki M, Kubo N, Kuroda K, Ogawa A, Iwasaki Y. Schwannoma arising from the intermediate nerve and manifesting as hemifacial spasm. Case report. J Neurosurg. 1996;84:277–9. doi: 10.3171/jns.1996.84.2.0277. [DOI] [PubMed] [Google Scholar]
- 10.Kugai M, Suyama T, Inui T, Yamazato K, Kitano M, Hasegawa H, et al. A case of vertebral artery aneurysm causing hemifacial spasm rapidly improved after parent artery occlusion. J Neuroendovasc Ther. 2019;13:288–92. [Google Scholar]
- 11.Matsumoto K, Kimura S, Kakita K. Endovascular treatment of vertebral artery aneurysm manifesting as progressive hemifacial spasm. Neurol Med Chir (Tokyo) 2005;45:360–2. doi: 10.2176/nmc.45.360. [DOI] [PubMed] [Google Scholar]
- 12.Matsumoto K, Saijo T, Kuyama H, Asari S, Nishimoto A. Hemifacial spasm caused by a spontaneous dissecting aneurysm of the vertebral artery. Case report. J Neurosurg. 1991;74:650–2. doi: 10.3171/jns.1991.74.4.0650. [DOI] [PubMed] [Google Scholar]
- 13.Moriuchi S, Nakagawa H, Yamada M, Kadota T. Hemifacial spasm due to compression of the facial nerve by vertebral artery-posterior inferior cerebellar artery aneurysm and elongated vertebral artery-case report. Neurol Med Chir (Tokyo) 1996;36:884–7. doi: 10.2176/nmc.36.884. [DOI] [PubMed] [Google Scholar]
- 14.Murakami H, Kawaguchi T, Fukuda M, Ito Y, Hasegawa H, Tanaka R. Monitoring of the lateral spread response in the endovascular treatment of a hemifacial spasm caused by an unruptured vertebral artery aneurysm. Case report. J Neurosurg. 2004;101:861–3. doi: 10.3171/jns.2004.101.5.0861. [DOI] [PubMed] [Google Scholar]
- 15.Nagashima H, Orz Y, Okudera H, Kobayashi S, Ichinose Y. Remission of hemifacial spasm after proximal occlusion of vertebrobasilar dissecting aneurysm with coils: Case report. J Clin Neurosci. 2001;8:43–5. doi: 10.1054/jocn.2000.0814. [DOI] [PubMed] [Google Scholar]
- 16.Nakagawa I, Takayama K, Kurokawa S, Wada T, Nakagawa H, Kichikawa K, et al. Hemifacial spasm due to contralateral aneurysmal compression of the facial nerve successfully treated with endovascular coil embolization: Case report. Neurosurgery. 2011;69:E768–71. doi: 10.1227/NEU.0b013e318218db06. discussion E771-62. [DOI] [PubMed] [Google Scholar]
- 17.Ou C, Wang S, Chen Y, Mo J, Zhao X. Microvascular decompression for hemifacial spasm induced by vertebral artery dissecting aneurysm: One case report. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2016;45:536–9. doi: 10.3785/j.issn.1008-9292.2016.09.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rodriguez-Catarino M, Frisen L, Wikholm G, Elfverson J, Quiding L, Svendsen P. Internal carotid artery aneurysms, cranial nerve dysfunction and headache: The role of deformation and pulsation. Neuroradiology. 2003;45:236–40. doi: 10.1007/s00234-002-0934-4. [DOI] [PubMed] [Google Scholar]
- 19.Santiago-Dieppa DR, McDonald MA, Brandel MG, Rennert RC, Khalessi AA, Olson SE. Endovascular flow diversion for hemifacial spasm induced by a vertebral artery aneurysm: First experience. Oper Neurosurg (Hagerstown) 2019;17:E115–8. doi: 10.1093/ons/opy359. [DOI] [PubMed] [Google Scholar]
- 20.Sato K, Ezura M, Takahashi A, Yoshimoto T. Fusiform aneurysm of the vertebral artery presenting hemifacial spasm treated by intravascular embolization: Case report. Surg Neurol. 2001;56:52–5. doi: 10.1016/s0090-3019(01)00496-7. [DOI] [PubMed] [Google Scholar]
- 21.Suzuki T, Takao H, Suzuki T, Kambayashi Y, Watanabe M, Shinohara S, et al. Fluid structure interaction analysis reveals facial nerve palsy caused by vertebral-posterior inferior cerebellar artery aneurysm. Comput Biol Med. 2015;66:263–8. doi: 10.1016/j.compbiomed.2015.09.016. [DOI] [PubMed] [Google Scholar]
- 22.Takahara M, Abe H, Ohkawa M, Iwaasa M, Ueba T, Higashi T, et al. Hemifacial spasm caused by a dissecting aneurysm of the vertebral artery, and resulting in acute exacerbation. No Shinkei Geka. 2013;41:241–6. [PubMed] [Google Scholar]
- 23.Tsuchiya D, Kayama T, Saito S, Sato S. Hemifacial spasm due to a compression of the facial nerve by a fusiform aneurysm of the vertebral artery: Case report. No To Shinkei. 2000;52:517–21. [PubMed] [Google Scholar]
- 24.Uchino M, Nomoto J, Ohtsuka T, Kuramitsu T. Fusiform aneurysm of the vertebral artery presenting with hemifacial spasm treated by microvascular decompression. Acta Neurochir (Wien) 2005;147:901–3. doi: 10.1007/s00701-005-0553-z. [DOI] [PubMed] [Google Scholar]