

Abstract
Background
As the coronavirus disease 2019 (COVID‐19) pandemic is sweeping across the globe, there is an urgent need to develop effective vaccines as the most powerful strategy to end the pandemic. This study aimed to examine how factors related to vaccine characteristics, their social normative influence and convenience of vaccination can affect the public's preference for the uptake of the COVID‐19 vaccine in China.
Methods
An online discrete choice experiment (DCE) survey was administered to a sample of China's general population. Participants were asked to make a series of hypothetical choices and estimate their preference for different attributes of the vaccine. A mixed logit regression model was used to analyse the DCE data. Willingness to pay for each attribute was also calculated.
Results
Data of 1236 participants who provided valid responses were included in the analysis. There was strong public preference for high effectiveness of the vaccine, followed by long protective duration, very few adverse events and being manufactured overseas. Price was the least important attribute affecting the public preference in selecting the COVID‐19 vaccine.
Conclusions
The strong public preferences detected in this study should be considered when developing COVID‐19 vaccination programme in China. The results provide useful information for policymakers to identify the individual and social values for a good vaccination strategy.
Patient or Public Contribution
The design of the experimental choices was fully based on interviews and focus group discussions participated by 26 Chinese people with diverse socio‐economic backgrounds. Without their participation, the study would not be possible.
Keywords: Chinese public, COVID‐19 pandemic, discrete choice experiment, vaccine, willingness to pay
1. INTRODUCTION
As of 24 August 2020, the novel severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) virus has infected more than 23 million people in 216 countries and regions, with a case fatality ratio (CFR) of approximately 3.4%. 1 Currently, there is no effective treatment for this disease, and relaxation of effective non‐pharmaceutical interventions often leads to resurgence of community outbreaks. 2 , 3 , 4 , 5 Thus, a vaccine seems to be the only solution to this problem. As vaccines are regarded as the most cost‐effective way of controlling infectious diseases, there are attempts to develop a coronavirus disease 2019 (COVID‐19) vaccine rapidly to catch up with the rate of the pandemic's spread. 6 On 20 July 2020, the so‐called Oxford vaccine (ChAdOx1 nCoV‐19) was announced as a front runner among 24 candidate vaccines in clinical evaluations worldwide. The reason is that it was proven in a stage 1/2, single‐blind, five‐site, randomized clinical trial that the vaccine could spike up antibodies and create a safe immune response in the body. 7
However, the path to introducing a new vaccine to the market can be politically and economically complicated. The COVID‐19 vaccine is no exception. Although insights and opinions of different stakeholders—such as policymakers and medical professionals—might affect the vaccine's uptake to some extent, 8 the most essential factor for any vaccination programme's successful adoption is the public's acceptance. Factors such as individual characteristics (eg high‐risk occupations and socio‐economic vulnerability) and disease‐specific characteristics (eg morbidity) play an important role in the individual's decision‐making process to select vaccination programmes. 9 , 10 A reasonable strategy should consider both the provider's affordability and consumer's preference. However, currently, studies investigating these factors and their effect on the public's preference in selecting the COVID‐19 vaccine are limited and fragmented. Obtaining such information is important for policymakers to understand the individual and social values to optimize strategies and design potential vaccination campaigns to address COVID‐19 as well as for pharmaceutical companies to estimate the expected benefit when managing the vaccine's development. 11 Moreover, the acceptance rate for a possible vaccine also reflects the public's willingness to be vaccinated. Thus, this study aimed to examine how the relative importance of factors related to vaccine characteristics, the social normative influence and convenience of vaccination affects the public's preference for the uptake of the COVID‐19 vaccine in China.
China was selected as the research location for two reasons. First, China is one of the leading candidates in the global vaccine development contest, as three of its vaccines were reported to have already completed the phase 2 clinical trials. At the end of June 2020, China's state‐run CanSino Biologics announced that their vaccine candidate demonstrated a 'good safety profile' with high levels of immune response in patients, and it is highly probable to be authorized for urgent use, including for front‐line medical professionals, at the end of this year. 12 Thus, a broader commercial use of the vaccine may not be too far off. Second, China's Wuhan City is regarded as the epicentre of the COVID‐19 pandemic. Moreover, China is one of the few countries recovering from the pandemic via careful manoeuvering to return to normal. Nevertheless, the pandemic's impact at the physical, psychological, social and economic levels is extensive and long‐lasting. Hence, this study provides empirical evidence to identify the optimal COVID‐19 vaccination programme for promoting the vaccine's uptake among the general Chinese population and indicates key attributes for consideration when other countries start to develop their own COVID‐19 vaccination programmes.
2. METHODS
To explore public preferences for the COVID‐19 vaccination programme, we used a discrete choice experiment (DCE) task administered online. 13 For each choice task, there were two options of hypothetical vaccination programme alternatives. To ensure all respondents make a choice and to detect their preference, no opt‐out alternative was provided. An example choice set is provided in Figure 1. The major benefit of using the stated preference method is that it allows us to understand and capture the public's preference for vaccination programmes that do not currently exist but could in future be available.
FIGURE 1.
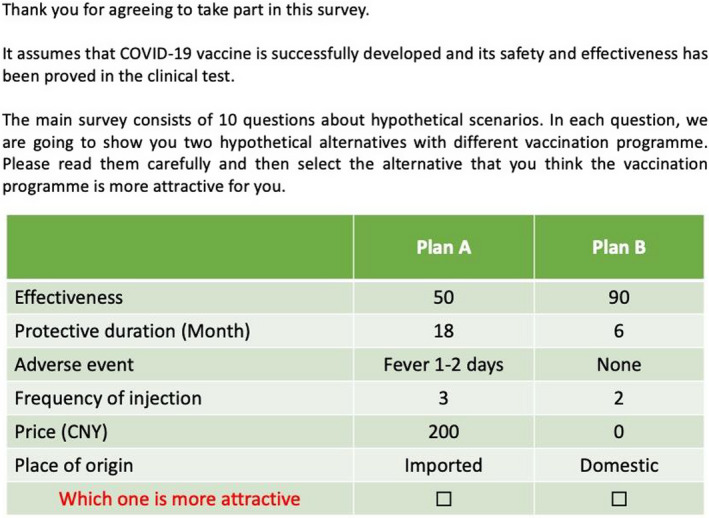
An example of choice set
2.1. Selection of attributes and levels
The criteria defined by Norman et al 14 were followed to develop the attributes and levels of our DCE questionnaire. According to these criteria, first, all levels and their combinations should be reasonable. Second, all levels and their combinations should be familiar to respondents in their current practice. Third, heterogeneity of the levels should be fully considered in the design to ensure the respondents can make some trade‐offs between them.
The attributes and levels were selected using a standard iterative process adopted by previous studies that used DCE. 13 , 15 , 16 First, the research team conducted a comprehensive literature review with articles extracted from the Cochrane Library, Web of Science, MEDLINE and EMBASE (1950‐2019), including academic articles using a variety of research methods such as quantitative and/or qualitative study designs, systematic reviews and randomized clinical trials, and the other government reports and policy briefings from Google, to explore important factors that affect the public's willingness and attitude when making decisions on vaccination uptake. The search target was not limited to the COVID‐19 and other pneumonia vaccines, but extended to other fields such as the influenza vaccine. Two researchers independently completed the literature review. All the team members discussed the findings, and four attributes—effectiveness, 17 , 18 , 19 , 20 protective duration, 17 , 19 , 20 , 21 adverse events 22 , 23 , 24 and frequency of injections 25 , 26 —were confirmed that potentially important for developing our DCE questionnaire. Then, on the basis of the findings from the literature review, six one‐to‐one interviews (three males and three females, aged between 28 and 62 years) and three focus group interviews with six to eight participants in each group (20 participants in total) as a sample of the Chinese general population were conducted to investigate their views and perspectives about the attributes of an 'ideal' COVID‐19 vaccine and its effectiveness at different levels. Several new insights were derived from the qualitative interviews. A new attribute—place of origin—that was considered to indirectly reflect the quality of the vaccine was added based on the interview results. The expression and explanations of the attributes and levels were modified according to the interviewees’ suggestions and comments. Third, a team of experts from relevant areas (clinical medicine, methodology, infectious disease and policy, five persons in total) was invited to discuss the findings from the previous steps. Two rounds of discussion were organized, experts and research team worked together to discuss how to modify and refine the attributes and levels to meet our criteria. Considering the majority of the adult vaccines are not free of charge in China, a cost parameter, which reflected the price of COVID‐19 vaccination programme, was included in the DCE questionnaire. An optimal mode of presenting choice sets to the respondents was also determined by experts to ensure the maximization of the face validity—the extent of a measure to capture what it is intended to measure—of the choice task. 27 Thus, finally, based on the literature review, general public interviews and expert discussions, six attributes with two to six levels for each were developed. The final set of attributes and levels is presented in Table 1.
TABLE 1.
The attributes and levels of the discrete choice experiment study
| Attribute | Levels |
|---|---|
| Effectiveness (%) | 50 |
| 70 | |
| 90 | |
| Duration of protection (month) | 6 |
| 12 | |
| 18 | |
| Adverse event | No reactions |
| Local reactions such as redness and/or swelling at the site of vaccination for 1‐2 d | |
| Fever 1‐2 d | |
| The total number of injections | 1 |
| 2 | |
| 3 | |
| Price (CNY) | 0 |
| 200 | |
| 400 | |
| 600 | |
| 800 | |
| 1000 | |
| Origin of product | Imported product |
| Domestic product |
Abbreviation: CNY, Chinese Yuan.
2.2. Experiment and questionnaire design
A full‐factorial design using all the attributes and levels results in 3 × 3×3 × 3 × 6 × 2 = 972 possible profiles, which provide 471 906 pairwise choice sets for selection. Using the STATA software (StataCorp LLC), 40 pairwise choice sets were constructed using a D‐optimality algorithm with the attribute coefficient set to zero. Only the main effect was estimated in this study. There is no standard guidance in the literature on the optimal number of DCE tasks that each respondent should complete. In this study, 40 choice sets were randomly assigned to four blocks, each of which had 10 choices. All of the choice sets were checked for plausibility, and no manual alteration of the design was required.
To assess the internal validity of DCE questions, a choice set with dominated pairs was presented (trap question) to all respondents. 28 In that choice task, one alternative was unambiguously better than the other alternative for all attributes. Only DCE data that the respondents correctly selected as the dominated alternative from this choice set would be included in the analysis.
The survey questionnaire's first page provided the study information. Participants were not allowed to continue the survey until they had read details of the informed consent and agreed to participate in the study by clicking the 'Agree' button at the bottom of the page. The questionnaire consisted of three sections. In the first section, respondents were advised that they would be providing information about their health conditions; their knowledge of, attitudes towards and experience with the COVID‐19 pandemic; and their previous experience of vaccination. In the second section, a dominated DCE task was presented to the respondents to check whether they understood the DCE design and provided a plausible answer. To reduce systematic selection biases, one of the four blocks with 10 standard DCE tasks for each was randomly chosen by the survey software and presented to the respondents. Each respondent was confronted with one block of 10 DCE questions. After completing the DCE questions, respondents were asked to provide a subjective assessment of the difficulty of the questions on a five‐point Likert scale ranging from 'very hard' to 'very easy'. The last part of the questionnaire included questions to collect information on the respondents’ demographics, socio‐economic status (SES) and an overall evaluation of their mental health status using the Patient Health Questionnaire‐2. 29
Before the formal study, a pilot DCE survey was conducted. A convenience sample of 10 members of the general public was invited to participate in the online survey. First, they were asked to complete the questionnaire independently through the same online platform as in the formal survey. Second, an interview was conducted immediately by the first two authors to understand their comments and suggestions on the survey and the approach.
2.3. Sample and survey administration
The survey was managed online via Wenjuanxing (WJX, https://www.wjx.cn/), the biggest online survey company in China, between June and July 2020. The questionnaire was developed by the research team using WJX’s survey design software built on its online survey platform. Participants were recruited by the same survey company via its members on the online panel. An online panel is a form of access panel and includes 'a sample database' consisting of registered participants who agree to occasionally participate in Internet‐based studies; these have become increasingly prevalent in academic research. 30 , 31 In this study, the inclusion criteria of participants was ≥18 years; Chinese citizen; and stay at China during the last six months. Although previous studies have indicated that using the Internet to collect data might lead to certain forms of interviewer bias, a growing number of researchers agree that web‐based surveys, which provide a quick and cost‐effective way to collect DCE data, are often preferred by participants than surveys administered by interviewers. 13 , 32 Thus, this study adopted a web‐based survey considering that nearly 0.8 billion Chinese people currently have access to the Internet. The Survey and Behavioural Research Ethics Committee of the Chinese University of Hong Kong approved the study protocol and informed consent (Reference No.: SBRE‐19‐690).
2.4. Data analysis
Descriptive statistics were used to present the participants’ demographics, SES, and physical and mental health status. The random utility theory provides the theoretical foundation for analysing the DCE data. The public's utility (U) associated with a particular vaccination programme had two components: the deterministic component (V) and the stochastic component (ε).
The model of utility for an individual n associated with vaccination programme i can be estimated as
The DCE data were binary, where '1' indicates that the alternative plan was chosen and '0' means that the other alternative plan was chosen. All attributes were dummy‐coded, and the coefficients of each level were estimated in the model and summarized to reflect the overall utility for each profile. The mixed logit regression (MXL) model was used to analyse the DCE data, as it estimates a distribution around each mean preference parameter to avoid potential bias of the estimated mean preference weights caused by unobserved heterogeneity. 33 The attribute of 'price' was specified as a continuous variable to facilitate the calculation of willingness to pay (WTP), which is the monetary value that people place on different attributes of the vaccination programme.
We calculated the utility value and relative predicted probabilities for all profiles of the experimental design, which allowed us to compare profiles that are more likely to be chosen by respondents with profiles that are less likely to be chosen. 34 This allowed us to convey the DCE results as easily understood information for the general public and policymakers. Subgroup analysis was also conducted to estimate the public's preference heterogeneity regarding vaccination programmes in terms of the respondents’ gender (men/women), family registry (urban/rural), parenting (yes/no) and personal vaccinated experience (yes/no). All statistical analyses were conducted using R (R Foundation, Austria) and STATA. The P‐value was set at ≤.05.
3. RESULTS
3.1. Responders’ characteristics
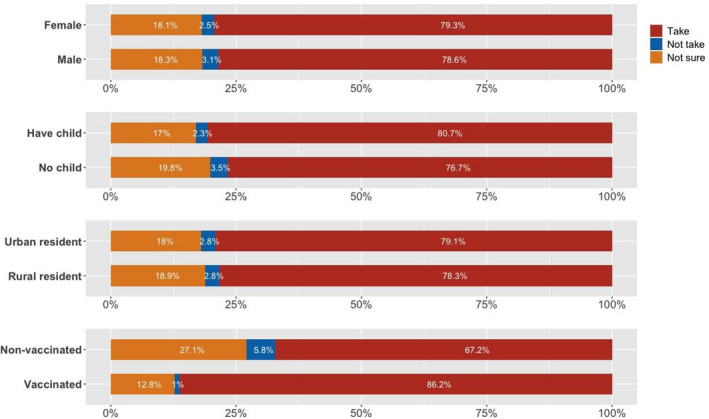
A total of 1694 individuals participated in the online survey, among whom, 177 did not consent or complete the questionnaire, 240 did not answer the trap item correctly, and 41 indicated the DCE questions are hard or very hard to be understood. These 458 answers were excluded from the analyses. Thus, data from 1236 individuals (72.96%) were elicited for our analyses. Four versions of the DCE questionnaire were completed by an approximately equal numbers of respondents (Appendix Table A1). Nearly half of the respondents were men, and the mean age was 30.27 years. The majority was married (60.6%) and lived in an urban area (72.18%). Most respondents were employed full time (78.4%), lived with their families (85.84%) and were protected by some form of medical insurance (98.62%). More than 80% reported a personal monthly income greater than the median monthly income in China (around 2200 Chinese Yuan [CNY]; 1 CNY = 0.14 USD) (Table 2). Compared with the national census data, our sample showed a similar sex ratio and proportion of medical insurance coverage, but higher educational attainment and proportion of living in the urban area. Figure 2 demonstrates that the respondents who were women (79.3%), had children (80.7%), lived in an urban area (79.1%) and were vaccinated in the past (86.2%) showed a more positive attitude towards taking the COVID‐19 vaccine.
TABLE A1.
All participants’ characteristics for each block (n = 1277)
| Block 1 (n = 322) | Block 2 (n = 313) | Block 3 (n = 322) | Block 4 (n = 320) | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | n | % | n | % | n | % | |
| Sex | ||||||||
| Male | 171 | 53.1 | 152 | 48.6 | 164 | 50.9 | 139 | 43.4 |
| Female | 151 | 46.9 | 161 | 51.4 | 158 | 49.1 | 181 | 56.6 |
| Age, mean (SD) | 28.9 | 7.5 | 30.2 | 7.5 | 31.0 | 8.6 | 30.0 | 6.8 |
| Educational level | ||||||||
| Secondary and below | 62 | 17.4 | 60 | 19.2 | 53 | 26.6 | 58 | 18.2 |
| Tertiary and above | 260 | 82.6 | 253 | 80.8 | 269 | 83.4 | 262 | 81.8 |
| Marital status | ||||||||
| Unmarried | 137 | 42.6 | 126 | 40.3 | 116 | 36 | 116 | 36.3 |
| Married | 183 | 56.8 | 185 | 59.1 | 205 | 63.7 | 202 | 61.1 |
| Divorced | 2 | 0.6 | 2 | 0.6 | 1 | 0.3 | 2 | 0.6 |
| Family register | ||||||||
| Urban area | 246 | 76.4 | 228 | 72.8 | 264 | 82 | 248 | 77.5 |
| Rural area | 75 | 23.3 | 85 | 27.2 | 58 | 18 | 72 | 22.5 |
| Number of children | ||||||||
| 0 | 154 | 47.8 | 142 | 45.4 | 131 | 40.7 | 129 | 40.3 |
| 1 | 131 | 40.7 | 145 | 46.3 | 166 | 51.6 | 158 | 49.4 |
| ≥2 | 37 | 11.5 | 26 | 8.3 | 25 | 7.7 | 33 | 10.3 |
| Living status | ||||||||
| Live along | 33 | 10.3 | 23 | 7.4 | 22 | 6.8 | 28 | 8.7 |
| Live with family | 263 | 81.7 | 272 | 87 | 285 | 88.5 | 227 | 88.6 |
| Live with friends | 22 | 6.8 | 18 | 5.6 | 12 | 3.7 | 15 | 4.7 |
| Others | 4 | 1.2 | ‐ | ‐ | 3 | 0.9 | ‐ | ‐ |
| Working status | ||||||||
| Full‐time employed | 249 | 77.3 | 254 | 81.2 | 250 | 77.6 | 245 | 76.6 |
| Part‐time employed | 12 | 3.7 | 11 | 3.5 | 10 | 3.1 | 14 | 4.4 |
| Farming | 2 | 0.6 | 3 | 0.9 | 3 | 0.9 | 2 | 0.6 |
| Students | 53 | 16.5 | 41 | 13.1 | 57 | 17.7 | 51 | 15.9 |
| Housewife | 1 | 0.3 | 2 | 0.6 | ‐ | ‐ | 1 | 0.3 |
| Retired | 2 | 0.6 | ‐ | ‐ | 1 | 0.3 | 1 | 0.3 |
| Unemployed | 3 | 0.9 | 2 | 0.6 | 1 | 0.3 | 6 | 1.9 |
| Medical insurance | ||||||||
| Yes | 317 | 98.4 | 306 | 97.8 | 319 | 99.1 | 315 | 98.4 |
| No | 5 | 1.6 | 7 | 2.2 | 3 | 0.9 | 5 | 1.6 |
| Personal income (CNY/month) | ||||||||
| <1000 | 23 | 7.1 | 25 | 7.9 | 29 | 9 | 23 | 7.2 |
| 1000‐1999 | 24 | 7.5 | 21 | 6.7 | 21 | 6.5 | 23 | 7.2 |
| 2000‐2999 | 25 | 7.8 | 17 | 5.4 | 9 | 2.8 | 24 | 7.5 |
| 3000‐3999 | 28 | 8.7 | 32 | 10.2 | 31 | 9.6 | 24 | 7.5 |
| 4000‐4999 | 20 | 6.2 | 21 | 6.7 | 18 | 5.6 | 28 | 8.7 |
| 5000‐5999 | 34 | 10.6 | 35 | 11.2 | 35 | 10.8 | 33 | 10.3 |
| 6000‐6999 | 32 | 9.9 | 34 | 10.9 | 32 | 9.9 | 29 | 9.1 |
| 7000‐7999 | 24 | 7.5 | 31 | 9.9 | 22 | 6.8 | 28 | 8.7 |
| 8000‐8999 | 35 | 10.9 | 30 | 9.6 | 36 | 11.2 | 40 | 12.5 |
| 9000‐9999 | 19 | 5.9 | 27 | 8.6 | 19 | 5.9 | 27 | 8.4 |
| ≥10 000 | 58 | 18.0 | 40 | 12.8 | 70 | 21.7 | 41 | 12.8 |
1277 including the participants who correctly answered the trap question, but indicated the discrete choice experiment questions are hard to be understood.
TABLE 2.
Characteristics of all respondents (n = 1236)
| Sample | General public a | ||
|---|---|---|---|
| n | % | % | |
| Sex | |||
| Male | 607 | 49.11 | 51.1 |
| Female | 629 | 50.89 | 48.9 |
| Age, mean (SD) | 30.27 | 7.66 | |
| Educational level (aged > 18) | |||
| Secondary and below | 176 | 14.24 | 85.9 |
| Tertiary and above | 1060 | 85.76 | 14.1 |
| Marital status | |||
| Unmarried | 480 | 38.83 | 18.2 |
| Married | 749 | 60.60 | 74.1 |
| Divorced/widow | 7 | 0.57 | 7.7 |
| Family register | |||
| Urban area | 954 | 77.18 | 59.9 |
| Rural area | 282 | 22.82 | 41.1 |
| Number of children | |||
| 0 | 556 | 43.54 | |
| 1 | 600 | 46.99 | |
| ≥2 | 121 | 9.47 | |
| Living status | |||
| Live along | 104 | 8.41 | |
| Live with family | 1061 | 85.84 | |
| Live with friends | 65 | 5.26 | |
| Others | 6 | 0.48 | |
| Working status | |||
| Full‐time employed | 969 | 78.4 | 96.3 |
| Part‐time employed | 44 | 3.56 | |
| Farming | 11 | 0.89 | |
| Students | 194 | 15.7 | |
| Housewife | 2 | 0.16 | |
| Retired | 4 | 0.32 | |
| Unemployed | 12 | 0.97 | |
| Medical insurance | |||
| Yes | 1219 | 98.62 | 96.5 |
| No | 17 | 1.38 | 3.5 |
| Personal income (CNY/month) | |||
| <1000 | 98 | 7.93 | |
| 1000‐1999 | 85 | 6.88 | |
| 2000‐2999 | 71 | 5.74 | |
| 3000‐3999 | 112 | 9.06 | |
| 4000‐4999 | 85 | 6.88 | |
| 5000‐5999 | 130 | 10.52 | |
| 6000‐6999 | 123 | 9.95 | |
| 7000‐7999 | 102 | 8.25 | |
| 8000‐8999 | 138 | 11.17 | |
| 9000‐9999 | 87 | 7.04 | |
| ≥10 000 | 205 | 16.59 | |
Abbreviations: CNY, China Yuan; SD, standard deviation.
Based on China Statistical Yearbook 2018.
FIGURE 2.
Respondents’ attitude towards COVID‐19 vaccine uptake
3.2. Results of the main effect model
Table 3 shows that the order and signs of all the attributes were as expected, and the coefficient of the attributes, except for the 'number of injections = 2', was statistically significant. The results demonstrated that the most important attribute was effectiveness. The coefficient of '90% effectiveness' was 3.138 (P < .001), followed by that of '70% effectiveness' (b = 1.416, P < .001). Although the COVID‐19 vaccine's price had a negative and significant effect on the respondents, it did not appear to be as important as the other attributes (b = −0.002, P < .001). Respondents’ preference for choosing a COVID‐19 vaccination programme increased with a longer protected duration but decreased with more adverse events and higher frequency of injections. In addition, we found that the place of manufacturing of the COVID‐19 vaccine affected the respondents’ preference—imported vaccine generated a higher utility score (b = 0.178, P < .001).
TABLE 3.
Main effects model and WTP (n = 1236)
| Coefficient (SE) | P‐value | SD (SE) | P‐value | WTP | 95% CI | ||
|---|---|---|---|---|---|---|---|
| Effect 70% | 1.416 (0.047) | <.001 | −0.201 (0.16) | .211 | 878.879 | 790.626 | 967.131 |
| Effect 90% | 3.138 (0.093) | <.001 | 1.739 (0.091) | <.001 | 1948.158 | 1766.113 | 2130.204 |
| Duration 12 mo | 0.491 (0.041) | <.001 | 0.053 (0.074) | .473 | 305.018 | 252.072 | 357.964 |
| Duration 18 mo | 0.719 (0.05) | <.001 | 0.409 (0.092) | <.001 | 446.663 | 379.633 | 513.693 |
| Moderate adverse event | 0.471 (0.044) | <.001 | 0.286 (0.1) | .004 | 292.175 | 236.172 | 348.178 |
| No adverse event | 1.042 (0.056) | <.001 | 0.93 (0.065) | <.001 | 647.029 | 565.525 | 728.533 |
| Injection 2 times | 0.059 (0.044) | .177 | −0.019 (0.109) | .859 | 36.791 | −16.956 | 90.537 |
| Injection 1 time | 0.159 (0.042) | <.001 | 0.317 (0.083) | <.001 | 98.417 | 47.56 | 149.273 |
| Imported | 0.178 (0.03) | <.001 | −0.081 (0.117) | .492 | 110.46 | 72.635 | 148.284 |
| Price | −0.002 (0) | <.001 | 0.002 (0.001) | <.001 | |||
Abbreviations: 95% CI, 95% confidence interval; SE, standard error; SD, standard deviation; WTP, willingness to pay.
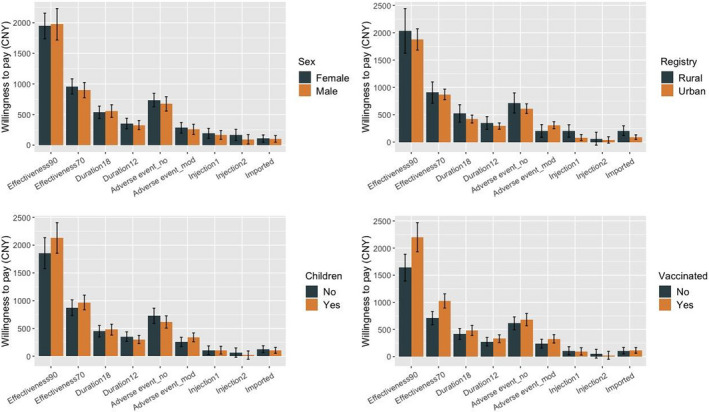
Results of the WTP estimation supported the comparisons of the respondents’ preferences from the monetary perspective. The results demonstrated that respondents prefer to pay more for effectiveness and longer protective duration than for the other attributes. On average, respondents were willing to pay around 1948 CNY and 446 CNY to take vaccines with 90% effectiveness and a protective duration of 18 months compared with 50% effectiveness and a protective duration of six months, respectively. In terms of the frequency of injections, respondents were willing to pay only 98 CNY to take one shot rather than take three shots. Table 4 and Figure 3 present results of the selective subgroup analysis. The COVID‐19 vaccine with higher effectiveness was more likely to lead to a higher utility value for respondents who were women, lived in a rural area, parenting children and had vaccinated experience. The utility values and probability of selection for all design profiles are presented in the Appendix (Table A2).
TABLE 4.
Results of subgroup analysis (n = 1236)
| Male | Female | |||
|---|---|---|---|---|
| Coefficient (SE) | SD (SE) | Coefficient (SE) | SD (SE) | |
| Effect 70% | 1.486 (0.076)*** | 0.593 (0.111)*** | 1.544 (0.073)*** | 0.225 (0.184) |
| Effect 90% | 3.279 (0.147)*** | 1.954 (0.129)*** | 3.391 (0.149)*** | 0.265 (0.187)*** |
| Duration 12 mo | 0.464 (0.06)*** | 0.011 (0.101) | 0.564 (0.059)*** | 1.866 (0.131) |
| Duration 18 mo | 0.601 (0.072)*** | 0.351 (0.135)* | 0.955 (0.079)*** | 0.081 (0.116)*** |
| Moderate adverse event | 0.524 (0.062)*** | 0.075 (0.136) | 0.444 (0.07)*** | 0.6 (0.123)*** |
| No adverse event | 0.951 (0.079)*** | 0.93 (0.096)** | 1.157 (0.085)*** | 0.71 (0.1)*** |
| Injection 2 times | −0.04 (0.065) | 0.319 (0.137) | 0.164 (0.066)*** | 1.156 (0.097) |
| Injection 1 time | 0.076 (0.059) | 0.066 (0.158) | 0.286 (0.062)* | 0.083 (0.115)* |
| Imported | 0.198 (0.045)*** | 0.085 (0.173) | 0.176 (0.046)*** | 0.317 (0.127) |
| Price | −0.001 (0.001)*** | 0.002 (0.001)*** | −0.002 (0.001)*** | 0.213 (0.113)*** |
| Urban resident | Rural resident | |||
|---|---|---|---|---|
| Coefficient (SE) | SD (SE) | Coefficient (SE) | SD (SE) | |
| Effect 70% | 1.488 (0.058)*** | 0.372 (0.102)*** | 1.44 (0.11)*** | 0.564 (0.191)** |
| Effect 90% | 3.235 (0.109)*** | 1.805 (0.101)*** | 3.208 (0.227)*** | 2.087 (0.233)*** |
| Duration 12 mo | 0.499 (0.047)*** | 0.041 (0.086) | 0.554 (0.089)*** | 0.1 (0.148) |
| Duration 18 mo | 0.718 (0.056)*** | 0.326 (0.122)** | 0.832 (0.118)** | 0.683 (0.182)*** |
| Moderate adverse event | 0.528 (0.052)*** | 0.423 (0.096)*** | 0.324 (0.093)*** | 0.196 (0.24) |
| No adverse event | 1.043 (0.064)*** | 0.933 (0.078)*** | 1.137 (0.126)*** | 0.968 (0.176)*** |
| Injection 2 times | 0.065 (0.051) | 0.02 (0.148) | 0.099 (0.095) | 0.07 (0.178) |
| Injection 1 time | 0.142 (0.048)** | 0.144 (0.128) | 0.323 (0.09)*** | 0.309 (0.202) |
| Imported | 0.154 (0.036)*** | 0.299 (0.07)*** | 0.331 (0.068)*** | 0.192 (0.141) |
| Price | −0.002 (0.001)*** | 0.002 (0)*** | −0.002 (0.001)*** | 0.002 (0.001)*** |
| Had children | No children | |||
|---|---|---|---|---|
| Coefficient (SE) | SD (SE) | Coefficient (SE) | SD (SE) | |
| Effect 70% | 1.558 (0.071)*** | 0.448 (0.126)*** | 1.411 (0.081)*** | 0.517 (0.127)*** |
| Effect 90% | 3.426 (0.139)*** | 2.015 (0.138)*** | 3.001 (0.141)*** | 1.782 (0.137)*** |
| Duration 12 months | 0.483 (0.057)*** | 0.081 (0.098) | 0.57 (0.065)*** | 0.123 (0.118) |
| Duration 18 months | 0.77 (0.072)*** | 0.606 (0.113)*** | 0.727 (0.076)*** | 0.292 (0.215) |
| Moderate adverse event | 0.546 (0.06)*** | 0.072 (0.155) | 0.413 (0.067)*** | 0.211 (0.295) |
| No adverse event | 0.991 (0.076)*** | 0.947 (0.092)*** | 1.176 (0.094)*** | 1.092 (0.101)*** |
| Injection 2 times | 0.031 (0.062) | 0.126 (0.129) | 0.105 (0.069) | 0.27 (0.145) |
| Injection 1 time | 0.175 (0.058)* | 0.336 (0.118)** | 0.176 (0.063)* | 0.115 (0.248) |
| Imported | 0.169 (0.043)*** | 0.286 (0.102)** | 0.204 (0.049)*** | 0.326 (0.088)*** |
| Price | −0.002 (0.001)*** | 0.002 (0.001)*** | −0.002 (0.001)*** | 0.002 (0.001)*** |
| Vaccinated | Non‐vaccinated | |||
|---|---|---|---|---|
| Coefficient (SE) | SD (SE) | Coefficient (SE) | SD (SE) | |
| Effect 70% | 1.601 (0.065)*** | 0.212 (0.157) | 1.259 (0.079)*** | 0.584 (0.128)*** |
| Effect 90% | 3.434 (0.129)*** | 1.911 (0.119) | 2.912 (0.151)*** | 1.809 (0.145)*** |
| Duration 12 months | 0.515 (0.053)*** | 0.116 (0.108) | 0.487 (0.066)*** | 0.051 (0.118) |
| Duration 18 months | 0.751 (0.066)*** | 0.392 (0.142) | 0.74 (0.081)*** | 0.473 (0.128)*** |
| Moderate adverse event | 0.512 (0.057)*** | 0.22 (0.167) | 0.423 (0.071)*** | 0.192 (0.133) |
| No adverse event | 1.064 (0.077)*** | 1.058 (0.088) | 1.087 (0.088)*** | 0.905 (0.107)*** |
| Injection 2 times | 0.037 (0.058) | 0.211 (0.158) | 0.094 (0.072) | 0.091 (0.132) |
| Injection 1 time | 0.149 (0.054)* | 0.222 (0.151) | 0.193 (0.067)* | 0.228 (0.133) |
| Imported | 0.179 (0.041)*** | 0.175 (0.094) | 0.194 (0.053)*** | 0.45 (0.084)*** |
| Price | −0.002 (0.001)*** | 0.002 (0.001) | −0.002 (0.001)*** | 0.002 (0.001)*** |
Abbreviations: SE, standard error; SD standard deviation.
<0.05;
<0.01;
<0.001.
FIGURE 3.
Willingness to pay estimation for subgroup population
TABLE A2.
Utility score of all the profiles in this study design
| No. | Effect | Duration | Adverse | Injection | Cost | Place | Utility | Percentage (%) |
|---|---|---|---|---|---|---|---|---|
| 1 | 90 | 18 | No | 1 | 400 | Imported | 8.083 | 1.128 |
| 2 | 90 | 18 | No | 3 | 400 | Imported | 8.083 | 1.128 |
| 3 | 90 | 18 | No | 1 | 600 | Imported | 8.081 | 1.126 |
| 4 | 90 | 18 | No | 2 | 1000 | Imported | 8.077 | 1.122 |
| 5 | 90 | 18 | No | 1 | 0 | Domestic | 7.909 | 0.948 |
| 6 | 90 | 18 | No | 1 | 200 | Domestic | 7.907 | 0.946 |
| 7 | 90 | 18 | No | 2 | 200 | Domestic | 7.907 | 0.946 |
| 8 | 90 | 18 | No | 2 | 400 | Domestic | 7.905 | 0.944 |
| 9 | 90 | 18 | No | 2 | 800 | Domestic | 7.901 | 0.941 |
| 10 | 90 | 18 | No | 1 | 1000 | Domestic | 7.899 | 0.939 |
| 11 | 90 | 18 | No | 3 | 1000 | Domestic | 7.899 | 0.939 |
| 12 | 90 | 12 | No | 3 | 200 | Imported | 7.857 | 0.9 |
| 13 | 90 | 12 | No | 1 | 400 | Imported | 7.855 | 0.898 |
| 14 | 90 | 12 | No | 2 | 400 | Imported | 7.855 | 0.898 |
| 15 | 90 | 12 | No | 2 | 600 | Imported | 7.853 | 0.896 |
| 16 | 90 | 12 | No | 1 | 800 | Imported | 7.851 | 0.895 |
| 17 | 90 | 12 | No | 3 | 800 | Imported | 7.851 | 0.895 |
| 18 | 90 | 12 | No | 1 | 1000 | Imported | 7.849 | 0.893 |
| 19 | 90 | 12 | No | 3 | 1000 | Imported | 7.849 | 0.893 |
| 20 | 90 | 12 | No | 1 | 0 | Domestic | 7.681 | 0.755 |
| 21 | 90 | 12 | No | 2 | 0 | Domestic | 7.681 | 0.755 |
| 22 | 90 | 12 | No | 1 | 200 | Domestic | 7.679 | 0.753 |
| 23 | 90 | 12 | No | 2 | 200 | Domestic | 7.679 | 0.753 |
| 24 | 90 | 12 | No | 3 | 400 | Domestic | 7.677 | 0.752 |
| 25 | 90 | 12 | No | 3 | 600 | Domestic | 7.675 | 0.75 |
| 26 | 90 | 12 | No | 2 | 1000 | Domestic | 7.671 | 0.747 |
| 27 | 90 | 18 | Moderate | 3 | 0 | Imported | 7.516 | 0.64 |
| 28 | 90 | 18 | Moderate | 3 | 200 | Imported | 7.514 | 0.639 |
| 29 | 90 | 18 | Moderate | 2 | 800 | Imported | 7.508 | 0.635 |
| 30 | 90 | 18 | Moderate | 3 | 800 | Imported | 7.508 | 0.635 |
| 31 | 90 | 18 | Moderate | 3 | 1000 | Imported | 7.506 | 0.634 |
| 32 | 90 | 6 | No | 1 | 400 | Imported | 7.364 | 0.55 |
| 33 | 90 | 6 | No | 3 | 800 | Imported | 7.36 | 0.548 |
| 34 | 90 | 18 | Moderate | 1 | 0 | Domestic | 7.338 | 0.536 |
| 35 | 90 | 18 | Moderate | 2 | 0 | Domestic | 7.338 | 0.536 |
| 36 | 90 | 18 | Moderate | 2 | 200 | Domestic | 7.336 | 0.535 |
| 37 | 90 | 18 | Moderate | 1 | 400 | Domestic | 7.334 | 0.534 |
| 38 | 90 | 18 | Moderate | 2 | 400 | Domestic | 7.334 | 0.534 |
| 39 | 90 | 18 | Moderate | 3 | 400 | Domestic | 7.334 | 0.534 |
| 40 | 90 | 18 | Moderate | 2 | 600 | Domestic | 7.332 | 0.532 |
| 41 | 90 | 18 | Moderate | 3 | 600 | Domestic | 7.332 | 0.532 |
| 42 | 90 | 18 | Moderate | 1 | 1000 | Domestic | 7.328 | 0.53 |
| 43 | 90 | 12 | Moderate | 2 | 200 | Imported | 7.286 | 0.509 |
| 44 | 90 | 12 | Moderate | 2 | 800 | Imported | 7.28 | 0.505 |
| 45 | 90 | 6 | No | 2 | 0 | Domestic | 7.19 | 0.462 |
| 46 | 90 | 6 | No | 3 | 0 | Domestic | 7.19 | 0.462 |
| 47 | 90 | 6 | No | 3 | 200 | Domestic | 7.188 | 0.461 |
| 48 | 90 | 6 | No | 2 | 400 | Domestic | 7.186 | 0.46 |
| 49 | 90 | 6 | No | 3 | 400 | Domestic | 7.186 | 0.46 |
| 50 | 90 | 6 | No | 3 | 600 | Domestic | 7.184 | 0.459 |
| 51 | 90 | 6 | No | 1 | 1000 | Domestic | 7.18 | 0.457 |
| 52 | 90 | 6 | No | 2 | 1000 | Domestic | 7.18 | 0.457 |
| 53 | 90 | 12 | Moderate | 2 | 0 | Domestic | 7.11 | 0.426 |
| 54 | 90 | 12 | Moderate | 1 | 200 | Domestic | 7.108 | 0.426 |
| 55 | 90 | 12 | Moderate | 3 | 200 | Domestic | 7.108 | 0.426 |
| 56 | 90 | 12 | Moderate | 3 | 400 | Domestic | 7.106 | 0.425 |
| 57 | 90 | 12 | Moderate | 1 | 600 | Domestic | 7.104 | 0.424 |
| 58 | 90 | 12 | Moderate | 1 | 800 | Domestic | 7.102 | 0.423 |
| 59 | 90 | 12 | Moderate | 3 | 800 | Domestic | 7.102 | 0.423 |
| 60 | 90 | 18 | No | 1 | 0 | Imported | 7.087 | 0.417 |
| 61 | 90 | 18 | No | 3 | 0 | Imported | 7.087 | 0.417 |
| 62 | 90 | 18 | No | 1 | 200 | Imported | 7.085 | 0.416 |
| 63 | 90 | 18 | No | 3 | 200 | Imported | 7.085 | 0.416 |
| 64 | 90 | 18 | No | 2 | 400 | Imported | 7.083 | 0.415 |
| 65 | 90 | 18 | No | 1 | 800 | Imported | 7.079 | 0.413 |
| 66 | 90 | 18 | No | 3 | 800 | Imported | 7.079 | 0.413 |
| 67 | 90 | 18 | Severe | 2 | 0 | Imported | 7.045 | 0.4 |
| 68 | 90 | 18 | Severe | 2 | 200 | Imported | 7.043 | 0.399 |
| 69 | 90 | 18 | Severe | 1 | 600 | Imported | 7.039 | 0.397 |
| 70 | 90 | 18 | Severe | 3 | 600 | Imported | 7.039 | 0.397 |
| 71 | 90 | 18 | No | 2 | 0 | Domestic | 6.909 | 0.349 |
| 72 | 90 | 18 | No | 1 | 400 | Domestic | 6.905 | 0.347 |
| 73 | 90 | 18 | No | 3 | 400 | Domestic | 6.905 | 0.347 |
| 74 | 90 | 18 | No | 2 | 600 | Domestic | 6.903 | 0.347 |
| 75 | 90 | 18 | No | 3 | 600 | Domestic | 6.903 | 0.347 |
| 76 | 90 | 18 | Severe | 3 | 0 | Domestic | 6.867 | 0.334 |
| 77 | 90 | 18 | Severe | 1 | 200 | Domestic | 6.865 | 0.334 |
| 78 | 90 | 18 | Severe | 3 | 400 | Domestic | 6.863 | 0.333 |
| 79 | 90 | 18 | Severe | 2 | 600 | Domestic | 6.861 | 0.332 |
| 80 | 90 | 12 | No | 1 | 0 | Imported | 6.859 | 0.332 |
| 81 | 90 | 12 | No | 2 | 0 | Imported | 6.859 | 0.332 |
| 82 | 90 | 12 | No | 3 | 0 | Imported | 6.859 | 0.332 |
| 83 | 90 | 18 | Severe | 1 | 800 | Domestic | 6.859 | 0.332 |
| 84 | 90 | 12 | No | 2 | 200 | Imported | 6.857 | 0.331 |
| 85 | 90 | 18 | Severe | 1 | 1000 | Domestic | 6.857 | 0.331 |
| 86 | 90 | 18 | Severe | 2 | 1000 | Domestic | 6.857 | 0.331 |
| 87 | 90 | 12 | No | 3 | 400 | Imported | 6.855 | 0.33 |
| 88 | 90 | 12 | No | 3 | 600 | Imported | 6.853 | 0.33 |
| 89 | 90 | 12 | No | 2 | 1000 | Imported | 6.849 | 0.328 |
| 90 | 90 | 12 | Severe | 2 | 0 | Imported | 6.817 | 0.318 |
| 91 | 90 | 12 | Severe | 3 | 0 | Imported | 6.817 | 0.318 |
| 92 | 90 | 12 | Severe | 3 | 200 | Imported | 6.815 | 0.318 |
| 93 | 90 | 12 | Severe | 2 | 400 | Imported | 6.813 | 0.317 |
| 94 | 90 | 12 | Severe | 2 | 600 | Imported | 6.811 | 0.316 |
| 95 | 90 | 12 | Severe | 3 | 1000 | Imported | 6.807 | 0.315 |
| 96 | 90 | 6 | Moderate | 1 | 0 | Imported | 6.797 | 0.312 |
| 97 | 90 | 6 | Moderate | 3 | 0 | Imported | 6.797 | 0.312 |
| 98 | 90 | 6 | Moderate | 1 | 200 | Imported | 6.795 | 0.311 |
| 99 | 90 | 6 | Moderate | 3 | 200 | Imported | 6.795 | 0.311 |
| 100 | 90 | 6 | Moderate | 2 | 600 | Imported | 6.791 | 0.31 |
| 101 | 90 | 6 | Moderate | 1 | 800 | Imported | 6.789 | 0.309 |
| 102 | 90 | 6 | Moderate | 1 | 1000 | Imported | 6.787 | 0.309 |
| 103 | 90 | 12 | No | 1 | 400 | Domestic | 6.677 | 0.277 |
| 104 | 90 | 12 | No | 2 | 400 | Domestic | 6.677 | 0.277 |
| 105 | 90 | 12 | No | 1 | 600 | Domestic | 6.675 | 0.276 |
| 106 | 90 | 12 | No | 1 | 800 | Domestic | 6.673 | 0.275 |
| 107 | 90 | 12 | No | 2 | 800 | Domestic | 6.673 | 0.275 |
| 108 | 90 | 12 | No | 3 | 800 | Domestic | 6.673 | 0.275 |
| 109 | 90 | 12 | No | 1 | 1000 | Domestic | 6.671 | 0.275 |
| 110 | 90 | 12 | Severe | 1 | 200 | Domestic | 6.637 | 0.266 |
| 111 | 90 | 12 | Severe | 1 | 400 | Domestic | 6.635 | 0.265 |
| 112 | 90 | 12 | Severe | 1 | 600 | Domestic | 6.633 | 0.265 |
| 113 | 90 | 12 | Severe | 3 | 600 | Domestic | 6.633 | 0.265 |
| 114 | 90 | 12 | Severe | 1 | 800 | Domestic | 6.631 | 0.264 |
| 115 | 90 | 12 | Severe | 2 | 800 | Domestic | 6.631 | 0.264 |
| 116 | 90 | 12 | Severe | 1 | 1000 | Domestic | 6.629 | 0.264 |
| 117 | 90 | 12 | Severe | 2 | 1000 | Domestic | 6.629 | 0.264 |
| 118 | 90 | 6 | Moderate | 2 | 200 | Domestic | 6.617 | 0.26 |
| 119 | 90 | 6 | Moderate | 1 | 400 | Domestic | 6.615 | 0.26 |
| 120 | 90 | 6 | Moderate | 1 | 600 | Domestic | 6.613 | 0.259 |
| 121 | 90 | 6 | Moderate | 3 | 600 | Domestic | 6.613 | 0.259 |
| 122 | 90 | 6 | Moderate | 2 | 800 | Domestic | 6.611 | 0.259 |
| 123 | 90 | 6 | Moderate | 2 | 1000 | Domestic | 6.609 | 0.258 |
| 124 | 90 | 6 | Moderate | 3 | 1000 | Domestic | 6.609 | 0.258 |
| 125 | 90 | 18 | Moderate | 2 | 200 | Imported | 6.514 | 0.235 |
| 126 | 90 | 18 | Moderate | 2 | 400 | Imported | 6.512 | 0.235 |
| 127 | 90 | 18 | Moderate | 3 | 400 | Imported | 6.512 | 0.235 |
| 128 | 90 | 18 | Moderate | 3 | 600 | Imported | 6.51 | 0.234 |
| 129 | 90 | 18 | Moderate | 1 | 800 | Imported | 6.508 | 0.234 |
| 130 | 90 | 6 | No | 1 | 0 | Imported | 6.368 | 0.203 |
| 131 | 90 | 6 | No | 1 | 200 | Imported | 6.366 | 0.203 |
| 132 | 90 | 6 | No | 3 | 200 | Imported | 6.366 | 0.203 |
| 133 | 90 | 6 | No | 3 | 400 | Imported | 6.364 | 0.202 |
| 134 | 70 | 18 | No | 1 | 200 | Imported | 6.363 | 0.202 |
| 135 | 70 | 18 | No | 3 | 200 | Imported | 6.363 | 0.202 |
| 136 | 90 | 6 | No | 1 | 800 | Imported | 6.36 | 0.201 |
| 137 | 90 | 6 | No | 2 | 800 | Imported | 6.36 | 0.201 |
| 138 | 70 | 18 | No | 1 | 800 | Imported | 6.357 | 0.201 |
| 139 | 70 | 18 | No | 3 | 800 | Imported | 6.357 | 0.201 |
| 140 | 70 | 18 | No | 1 | 1000 | Imported | 6.355 | 0.2 |
| 141 | 90 | 18 | Moderate | 3 | 0 | Domestic | 6.338 | 0.197 |
| 142 | 90 | 18 | Moderate | 1 | 200 | Domestic | 6.336 | 0.197 |
| 143 | 90 | 18 | Moderate | 3 | 200 | Domestic | 6.336 | 0.197 |
| 144 | 90 | 18 | Moderate | 1 | 600 | Domestic | 6.332 | 0.196 |
| 145 | 90 | 18 | Moderate | 2 | 800 | Domestic | 6.33 | 0.195 |
| 146 | 90 | 18 | Moderate | 3 | 800 | Domestic | 6.33 | 0.195 |
| 147 | 90 | 18 | Moderate | 2 | 1000 | Domestic | 6.328 | 0.195 |
| 148 | 90 | 6 | Severe | 2 | 0 | Imported | 6.326 | 0.195 |
| 149 | 90 | 6 | Severe | 1 | 600 | Imported | 6.32 | 0.194 |
| 150 | 90 | 12 | Moderate | 1 | 0 | Imported | 6.288 | 0.187 |
| 151 | 90 | 12 | Moderate | 3 | 0 | Imported | 6.288 | 0.187 |
| 152 | 90 | 12 | Moderate | 2 | 400 | Imported | 6.284 | 0.187 |
| 153 | 90 | 12 | Moderate | 2 | 600 | Imported | 6.282 | 0.186 |
| 154 | 90 | 12 | Moderate | 1 | 800 | Imported | 6.28 | 0.186 |
| 155 | 90 | 6 | No | 2 | 200 | Domestic | 6.188 | 0.17 |
| 156 | 70 | 18 | No | 3 | 0 | Domestic | 6.187 | 0.169 |
| 157 | 90 | 6 | No | 1 | 400 | Domestic | 6.186 | 0.169 |
| 158 | 70 | 18 | No | 2 | 200 | Domestic | 6.185 | 0.169 |
| 159 | 90 | 6 | No | 1 | 600 | Domestic | 6.184 | 0.169 |
| 160 | 90 | 6 | No | 2 | 600 | Domestic | 6.184 | 0.169 |
| 161 | 70 | 18 | No | 1 | 400 | Domestic | 6.183 | 0.169 |
| 162 | 90 | 6 | No | 3 | 800 | Domestic | 6.182 | 0.169 |
| 163 | 70 | 18 | No | 1 | 600 | Domestic | 6.181 | 0.168 |
| 164 | 70 | 18 | No | 2 | 600 | Domestic | 6.181 | 0.168 |
| 165 | 90 | 6 | No | 3 | 1000 | Domestic | 6.18 | 0.168 |
| 166 | 70 | 18 | No | 2 | 800 | Domestic | 6.179 | 0.168 |
| 167 | 90 | 6 | Severe | 1 | 0 | Domestic | 6.148 | 0.163 |
| 168 | 90 | 6 | Severe | 3 | 0 | Domestic | 6.148 | 0.163 |
| 169 | 90 | 6 | Severe | 1 | 400 | Domestic | 6.144 | 0.162 |
| 170 | 90 | 6 | Severe | 2 | 600 | Domestic | 6.142 | 0.162 |
| 171 | 90 | 6 | Severe | 3 | 600 | Domestic | 6.142 | 0.162 |
| 172 | 90 | 6 | Severe | 2 | 800 | Domestic | 6.14 | 0.162 |
| 173 | 90 | 6 | Severe | 3 | 800 | Domestic | 6.14 | 0.162 |
| 174 | 90 | 6 | Severe | 3 | 1000 | Domestic | 6.138 | 0.161 |
| 175 | 70 | 12 | No | 2 | 0 | Imported | 6.137 | 0.161 |
| 176 | 70 | 12 | No | 2 | 200 | Imported | 6.135 | 0.161 |
| 177 | 70 | 12 | No | 3 | 600 | Imported | 6.131 | 0.16 |
| 178 | 70 | 12 | No | 1 | 800 | Imported | 6.129 | 0.16 |
| 179 | 70 | 12 | No | 2 | 800 | Imported | 6.129 | 0.16 |
| 180 | 70 | 12 | No | 2 | 1000 | Imported | 6.127 | 0.16 |
| 181 | 90 | 12 | Moderate | 1 | 400 | Domestic | 6.106 | 0.156 |
| 182 | 90 | 12 | Moderate | 3 | 600 | Domestic | 6.104 | 0.156 |
| 183 | 90 | 12 | Moderate | 2 | 800 | Domestic | 6.102 | 0.156 |
| 184 | 90 | 12 | Moderate | 1 | 1000 | Domestic | 6.1 | 0.155 |
| 185 | 90 | 12 | Moderate | 2 | 1000 | Domestic | 6.1 | 0.155 |
| 186 | 90 | 12 | Moderate | 3 | 1000 | Domestic | 6.1 | 0.155 |
| 187 | 90 | 18 | No | 2 | 0 | Imported | 6.087 | 0.153 |
| 188 | 90 | 18 | No | 2 | 200 | Imported | 6.085 | 0.153 |
| 189 | 90 | 18 | No | 2 | 600 | Imported | 6.081 | 0.152 |
| 190 | 90 | 18 | No | 3 | 600 | Imported | 6.081 | 0.152 |
| 191 | 90 | 18 | No | 2 | 800 | Imported | 6.079 | 0.152 |
| 192 | 90 | 18 | No | 1 | 1000 | Imported | 6.077 | 0.152 |
| 193 | 90 | 18 | No | 3 | 1000 | Imported | 6.077 | 0.152 |
| 194 | 90 | 18 | Severe | 3 | 0 | Imported | 6.045 | 0.147 |
| 195 | 90 | 18 | Severe | 1 | 200 | Imported | 6.043 | 0.147 |
| 196 | 90 | 18 | Severe | 1 | 400 | Imported | 6.041 | 0.146 |
| 197 | 90 | 18 | Severe | 2 | 400 | Imported | 6.041 | 0.146 |
| 198 | 90 | 18 | Severe | 1 | 800 | Imported | 6.037 | 0.146 |
| 199 | 90 | 18 | Severe | 3 | 800 | Imported | 6.037 | 0.146 |
| 200 | 90 | 18 | Severe | 1 | 1000 | Imported | 6.035 | 0.146 |
| 201 | 90 | 18 | Severe | 3 | 1000 | Imported | 6.035 | 0.146 |
| 202 | 70 | 12 | No | 1 | 0 | Domestic | 5.959 | 0.135 |
| 203 | 70 | 12 | No | 1 | 200 | Domestic | 5.957 | 0.135 |
| 204 | 70 | 12 | No | 3 | 200 | Domestic | 5.957 | 0.135 |
| 205 | 70 | 12 | No | 1 | 400 | Domestic | 5.955 | 0.134 |
| 206 | 70 | 12 | No | 2 | 400 | Domestic | 5.955 | 0.134 |
| 207 | 70 | 12 | No | 1 | 600 | Domestic | 5.953 | 0.134 |
| 208 | 70 | 12 | No | 2 | 600 | Domestic | 5.953 | 0.134 |
| 209 | 70 | 12 | No | 3 | 800 | Domestic | 5.951 | 0.134 |
| 210 | 70 | 12 | No | 3 | 1000 | Domestic | 5.949 | 0.134 |
| 211 | 90 | 18 | No | 3 | 0 | Domestic | 5.909 | 0.128 |
| 212 | 90 | 18 | No | 3 | 200 | Domestic | 5.907 | 0.128 |
| 213 | 90 | 18 | No | 1 | 600 | Domestic | 5.903 | 0.128 |
| 214 | 90 | 18 | No | 1 | 800 | Domestic | 5.901 | 0.127 |
| 215 | 90 | 18 | No | 3 | 800 | Domestic | 5.901 | 0.127 |
| 216 | 90 | 18 | No | 2 | 1000 | Domestic | 5.899 | 0.127 |
| 217 | 90 | 18 | Severe | 1 | 0 | Domestic | 5.867 | 0.123 |
| 218 | 90 | 18 | Severe | 2 | 0 | Domestic | 5.867 | 0.123 |
| 219 | 90 | 18 | Severe | 3 | 200 | Domestic | 5.865 | 0.123 |
| 220 | 90 | 18 | Severe | 2 | 800 | Domestic | 5.859 | 0.122 |
| 221 | 90 | 12 | No | 1 | 200 | Imported | 5.857 | 0.122 |
| 222 | 90 | 12 | No | 1 | 600 | Imported | 5.853 | 0.121 |
| 223 | 90 | 12 | No | 2 | 800 | Imported | 5.851 | 0.121 |
| 224 | 90 | 12 | Severe | 1 | 0 | Imported | 5.817 | 0.117 |
| 225 | 90 | 12 | Severe | 1 | 600 | Imported | 5.811 | 0.116 |
| 226 | 90 | 12 | Severe | 3 | 600 | Imported | 5.811 | 0.116 |
| 227 | 90 | 12 | Severe | 1 | 800 | Imported | 5.809 | 0.116 |
| 228 | 90 | 12 | Severe | 2 | 800 | Imported | 5.809 | 0.116 |
| 229 | 90 | 12 | Severe | 3 | 800 | Imported | 5.809 | 0.116 |
| 230 | 90 | 12 | Severe | 2 | 1000 | Imported | 5.807 | 0.116 |
| 231 | 90 | 6 | Moderate | 2 | 200 | Imported | 5.795 | 0.114 |
| 232 | 70 | 18 | Moderate | 3 | 0 | Imported | 5.794 | 0.114 |
| 233 | 90 | 6 | Moderate | 1 | 400 | Imported | 5.793 | 0.114 |
| 234 | 90 | 6 | Moderate | 2 | 400 | Imported | 5.793 | 0.114 |
| 235 | 90 | 6 | Moderate | 3 | 400 | Imported | 5.793 | 0.114 |
| 236 | 90 | 6 | Moderate | 1 | 600 | Imported | 5.791 | 0.114 |
| 237 | 70 | 18 | Moderate | 3 | 400 | Imported | 5.79 | 0.114 |
| 238 | 90 | 6 | Moderate | 2 | 800 | Imported | 5.789 | 0.114 |
| 239 | 70 | 18 | Moderate | 3 | 600 | Imported | 5.788 | 0.114 |
| 240 | 90 | 6 | Moderate | 2 | 1000 | Imported | 5.787 | 0.114 |
| 241 | 90 | 12 | No | 3 | 0 | Domestic | 5.681 | 0.102 |
| 242 | 90 | 12 | No | 3 | 200 | Domestic | 5.679 | 0.102 |
| 243 | 90 | 12 | No | 2 | 600 | Domestic | 5.675 | 0.102 |
| 244 | 90 | 12 | No | 3 | 1000 | Domestic | 5.671 | 0.101 |
| 245 | 70 | 6 | No | 1 | 200 | Imported | 5.644 | 0.098 |
| 246 | 90 | 12 | Severe | 2 | 0 | Domestic | 5.639 | 0.098 |
| 247 | 90 | 12 | Severe | 3 | 0 | Domestic | 5.639 | 0.098 |
| 248 | 70 | 6 | No | 1 | 800 | Imported | 5.638 | 0.098 |
| 249 | 90 | 12 | Severe | 2 | 200 | Domestic | 5.637 | 0.098 |
| 250 | 90 | 12 | Severe | 2 | 400 | Domestic | 5.635 | 0.098 |
| 251 | 90 | 12 | Severe | 3 | 400 | Domestic | 5.635 | 0.098 |
| 252 | 90 | 12 | Severe | 2 | 600 | Domestic | 5.633 | 0.097 |
| 253 | 90 | 6 | Moderate | 1 | 0 | Domestic | 5.619 | 0.096 |
| 254 | 90 | 6 | Moderate | 2 | 0 | Domestic | 5.619 | 0.096 |
| 255 | 90 | 6 | Moderate | 3 | 0 | Domestic | 5.619 | 0.096 |
| 256 | 90 | 6 | Moderate | 1 | 200 | Domestic | 5.617 | 0.096 |
| 257 | 70 | 18 | Moderate | 1 | 200 | Domestic | 5.614 | 0.096 |
| 258 | 70 | 18 | Moderate | 2 | 200 | Domestic | 5.614 | 0.096 |
| 259 | 70 | 18 | Moderate | 1 | 400 | Domestic | 5.612 | 0.095 |
| 260 | 70 | 18 | Moderate | 2 | 400 | Domestic | 5.612 | 0.095 |
| 261 | 90 | 6 | Moderate | 1 | 800 | Domestic | 5.611 | 0.095 |
| 262 | 90 | 6 | Moderate | 3 | 800 | Domestic | 5.611 | 0.095 |
| 263 | 70 | 18 | Moderate | 2 | 600 | Domestic | 5.61 | 0.095 |
| 264 | 70 | 18 | Moderate | 1 | 800 | Domestic | 5.608 | 0.095 |
| 265 | 70 | 18 | Moderate | 2 | 800 | Domestic | 5.608 | 0.095 |
| 266 | 70 | 18 | Moderate | 3 | 800 | Domestic | 5.608 | 0.095 |
| 267 | 70 | 18 | Moderate | 2 | 1000 | Domestic | 5.606 | 0.095 |
| 268 | 70 | 18 | Moderate | 3 | 1000 | Domestic | 5.606 | 0.095 |
| 269 | 70 | 12 | Moderate | 1 | 0 | Imported | 5.566 | 0.091 |
| 270 | 70 | 12 | Moderate | 3 | 0 | Imported | 5.566 | 0.091 |
| 271 | 70 | 12 | Moderate | 1 | 200 | Imported | 5.564 | 0.091 |
| 272 | 70 | 12 | Moderate | 2 | 600 | Imported | 5.56 | 0.091 |
| 273 | 90 | 18 | Moderate | 1 | 0 | Imported | 5.516 | 0.087 |
| 274 | 90 | 18 | Moderate | 2 | 0 | Imported | 5.516 | 0.087 |
| 275 | 90 | 18 | Moderate | 1 | 200 | Imported | 5.514 | 0.086 |
| 276 | 90 | 18 | Moderate | 1 | 400 | Imported | 5.512 | 0.086 |
| 277 | 90 | 18 | Moderate | 1 | 600 | Imported | 5.51 | 0.086 |
| 278 | 90 | 18 | Moderate | 2 | 600 | Imported | 5.51 | 0.086 |
| 279 | 90 | 18 | Moderate | 1 | 1000 | Imported | 5.506 | 0.086 |
| 280 | 90 | 18 | Moderate | 2 | 1000 | Imported | 5.506 | 0.086 |
| 281 | 70 | 6 | No | 1 | 0 | Domestic | 5.468 | 0.083 |
| 282 | 70 | 6 | No | 2 | 200 | Domestic | 5.466 | 0.082 |
| 283 | 70 | 6 | No | 3 | 200 | Domestic | 5.466 | 0.082 |
| 284 | 70 | 6 | No | 2 | 400 | Domestic | 5.464 | 0.082 |
| 285 | 70 | 6 | No | 3 | 400 | Domestic | 5.464 | 0.082 |
| 286 | 70 | 6 | No | 3 | 600 | Domestic | 5.462 | 0.082 |
| 287 | 70 | 6 | No | 2 | 800 | Domestic | 5.46 | 0.082 |
| 288 | 70 | 6 | No | 3 | 800 | Domestic | 5.46 | 0.082 |
| 289 | 70 | 6 | No | 3 | 1000 | Domestic | 5.458 | 0.082 |
| 290 | 70 | 12 | Moderate | 2 | 0 | Domestic | 5.388 | 0.076 |
| 291 | 70 | 12 | Moderate | 2 | 400 | Domestic | 5.384 | 0.076 |
| 292 | 70 | 12 | Moderate | 1 | 600 | Domestic | 5.382 | 0.076 |
| 293 | 70 | 12 | Moderate | 3 | 600 | Domestic | 5.382 | 0.076 |
| 294 | 70 | 12 | Moderate | 3 | 800 | Domestic | 5.38 | 0.076 |
| 295 | 70 | 12 | Moderate | 1 | 1000 | Domestic | 5.378 | 0.075 |
| 296 | 90 | 6 | No | 2 | 0 | Imported | 5.368 | 0.075 |
| 297 | 90 | 6 | No | 3 | 0 | Imported | 5.368 | 0.075 |
| 298 | 90 | 6 | No | 2 | 200 | Imported | 5.366 | 0.075 |
| 299 | 70 | 18 | No | 1 | 0 | Imported | 5.365 | 0.074 |
| 300 | 70 | 18 | No | 2 | 0 | Imported | 5.365 | 0.074 |
| 301 | 90 | 6 | No | 2 | 400 | Imported | 5.364 | 0.074 |
| 302 | 90 | 6 | No | 1 | 600 | Imported | 5.362 | 0.074 |
| 303 | 90 | 6 | No | 2 | 600 | Imported | 5.362 | 0.074 |
| 304 | 90 | 6 | No | 3 | 600 | Imported | 5.362 | 0.074 |
| 305 | 70 | 18 | No | 1 | 400 | Imported | 5.361 | 0.074 |
| 306 | 70 | 18 | No | 3 | 400 | Imported | 5.361 | 0.074 |
| 307 | 70 | 18 | No | 1 | 600 | Imported | 5.359 | 0.074 |
| 308 | 70 | 18 | No | 3 | 600 | Imported | 5.359 | 0.074 |
| 309 | 90 | 6 | No | 1 | 1000 | Imported | 5.358 | 0.074 |
| 310 | 90 | 6 | No | 2 | 1000 | Imported | 5.358 | 0.074 |
| 311 | 90 | 6 | No | 3 | 1000 | Imported | 5.358 | 0.074 |
| 312 | 70 | 18 | No | 2 | 800 | Imported | 5.357 | 0.074 |
| 313 | 90 | 18 | Moderate | 1 | 800 | Domestic | 5.33 | 0.072 |
| 314 | 90 | 18 | Moderate | 3 | 1000 | Domestic | 5.328 | 0.072 |
| 315 | 90 | 6 | Severe | 1 | 0 | Imported | 5.326 | 0.072 |
| 316 | 70 | 18 | Severe | 1 | 0 | Imported | 5.323 | 0.071 |
| 317 | 90 | 6 | Severe | 2 | 400 | Imported | 5.322 | 0.071 |
| 318 | 90 | 6 | Severe | 3 | 400 | Imported | 5.322 | 0.071 |
| 319 | 70 | 18 | Severe | 1 | 200 | Imported | 5.321 | 0.071 |
| 320 | 70 | 18 | Severe | 2 | 400 | Imported | 5.319 | 0.071 |
| 321 | 90 | 6 | Severe | 1 | 800 | Imported | 5.318 | 0.071 |
| 322 | 70 | 18 | Severe | 2 | 600 | Imported | 5.317 | 0.071 |
| 323 | 90 | 6 | Severe | 1 | 1000 | Imported | 5.316 | 0.071 |
| 324 | 90 | 6 | Severe | 3 | 1000 | Imported | 5.316 | 0.071 |
| 325 | 70 | 18 | Severe | 1 | 1000 | Imported | 5.313 | 0.071 |
| 326 | 70 | 18 | Severe | 3 | 1000 | Imported | 5.313 | 0.071 |
| 327 | 90 | 12 | Moderate | 2 | 0 | Imported | 5.288 | 0.069 |
| 328 | 90 | 12 | Moderate | 1 | 200 | Imported | 5.286 | 0.069 |
| 329 | 90 | 12 | Moderate | 3 | 200 | Imported | 5.286 | 0.069 |
| 330 | 90 | 12 | Moderate | 1 | 400 | Imported | 5.284 | 0.069 |
| 331 | 90 | 12 | Moderate | 3 | 400 | Imported | 5.284 | 0.069 |
| 332 | 90 | 12 | Moderate | 1 | 600 | Imported | 5.282 | 0.069 |
| 333 | 90 | 12 | Moderate | 3 | 600 | Imported | 5.282 | 0.069 |
| 334 | 90 | 12 | Moderate | 3 | 800 | Imported | 5.28 | 0.068 |
| 335 | 90 | 12 | Moderate | 1 | 1000 | Imported | 5.278 | 0.068 |
| 336 | 90 | 12 | Moderate | 2 | 1000 | Imported | 5.278 | 0.068 |
| 337 | 90 | 12 | Moderate | 3 | 1000 | Imported | 5.278 | 0.068 |
| 338 | 90 | 6 | No | 1 | 0 | Domestic | 5.19 | 0.063 |
| 339 | 90 | 6 | No | 1 | 200 | Domestic | 5.188 | 0.062 |
| 340 | 70 | 18 | No | 2 | 400 | Domestic | 5.183 | 0.062 |
| 341 | 90 | 6 | No | 1 | 800 | Domestic | 5.182 | 0.062 |
| 342 | 90 | 6 | No | 2 | 800 | Domestic | 5.182 | 0.062 |
| 343 | 70 | 18 | No | 1 | 800 | Domestic | 5.179 | 0.062 |
| 344 | 70 | 18 | No | 3 | 800 | Domestic | 5.179 | 0.062 |
| 345 | 70 | 18 | No | 2 | 1000 | Domestic | 5.177 | 0.062 |
| 346 | 70 | 18 | No | 3 | 1000 | Domestic | 5.177 | 0.062 |
| 347 | 90 | 6 | Severe | 2 | 0 | Domestic | 5.148 | 0.06 |
| 348 | 90 | 6 | Severe | 1 | 200 | Domestic | 5.146 | 0.06 |
| 349 | 90 | 6 | Severe | 2 | 200 | Domestic | 5.146 | 0.06 |
| 350 | 90 | 6 | Severe | 3 | 200 | Domestic | 5.146 | 0.06 |
| 351 | 70 | 18 | Severe | 2 | 0 | Domestic | 5.145 | 0.06 |
| 352 | 70 | 18 | Severe | 2 | 200 | Domestic | 5.143 | 0.06 |
| 353 | 70 | 18 | Severe | 3 | 200 | Domestic | 5.143 | 0.06 |
| 354 | 70 | 18 | Severe | 3 | 400 | Domestic | 5.141 | 0.06 |
| 355 | 70 | 18 | Severe | 1 | 600 | Domestic | 5.139 | 0.059 |
| 356 | 90 | 6 | Severe | 2 | 1000 | Domestic | 5.138 | 0.059 |
| 357 | 70 | 18 | Severe | 3 | 800 | Domestic | 5.137 | 0.059 |
| 358 | 70 | 12 | No | 1 | 200 | Imported | 5.135 | 0.059 |
| 359 | 70 | 12 | No | 3 | 200 | Imported | 5.135 | 0.059 |
| 360 | 70 | 18 | Severe | 2 | 1000 | Domestic | 5.135 | 0.059 |
| 361 | 70 | 12 | No | 1 | 400 | Imported | 5.133 | 0.059 |
| 362 | 70 | 12 | No | 2 | 400 | Imported | 5.133 | 0.059 |
| 363 | 70 | 12 | No | 3 | 400 | Imported | 5.133 | 0.059 |
| 364 | 70 | 12 | No | 2 | 600 | Imported | 5.131 | 0.059 |
| 365 | 70 | 12 | No | 3 | 800 | Imported | 5.129 | 0.059 |
| 366 | 70 | 12 | No | 3 | 1000 | Imported | 5.127 | 0.059 |
| 367 | 90 | 12 | Moderate | 1 | 0 | Domestic | 5.11 | 0.058 |
| 368 | 90 | 12 | Moderate | 3 | 0 | Domestic | 5.11 | 0.058 |
| 369 | 90 | 12 | Moderate | 2 | 200 | Domestic | 5.108 | 0.058 |
| 370 | 90 | 12 | Moderate | 2 | 400 | Domestic | 5.106 | 0.057 |
| 371 | 90 | 12 | Moderate | 2 | 600 | Domestic | 5.104 | 0.057 |
| 372 | 70 | 12 | Severe | 2 | 400 | Imported | 5.091 | 0.057 |
| 373 | 70 | 12 | Severe | 3 | 400 | Imported | 5.091 | 0.057 |
| 374 | 70 | 12 | Severe | 3 | 600 | Imported | 5.089 | 0.057 |
| 375 | 70 | 12 | Severe | 2 | 800 | Imported | 5.087 | 0.056 |
| 376 | 70 | 12 | Severe | 2 | 1000 | Imported | 5.085 | 0.056 |
| 377 | 70 | 6 | Moderate | 1 | 0 | Imported | 5.075 | 0.056 |
| 378 | 70 | 6 | Moderate | 2 | 0 | Imported | 5.075 | 0.056 |
| 379 | 70 | 6 | Moderate | 2 | 200 | Imported | 5.073 | 0.056 |
| 380 | 70 | 6 | Moderate | 1 | 400 | Imported | 5.071 | 0.056 |
| 381 | 70 | 6 | Moderate | 3 | 400 | Imported | 5.071 | 0.056 |
| 382 | 70 | 6 | Moderate | 1 | 600 | Imported | 5.069 | 0.055 |
| 383 | 70 | 6 | Moderate | 3 | 600 | Imported | 5.069 | 0.055 |
| 384 | 70 | 6 | Moderate | 2 | 1000 | Imported | 5.065 | 0.055 |
| 385 | 90 | 18 | Severe | 1 | 0 | Imported | 5.045 | 0.054 |
| 386 | 90 | 18 | Severe | 3 | 200 | Imported | 5.043 | 0.054 |
| 387 | 90 | 18 | Severe | 3 | 400 | Imported | 5.041 | 0.054 |
| 388 | 90 | 18 | Severe | 2 | 600 | Imported | 5.039 | 0.054 |
| 389 | 90 | 18 | Severe | 2 | 800 | Imported | 5.037 | 0.054 |
| 390 | 90 | 18 | Severe | 2 | 1000 | Imported | 5.035 | 0.054 |
| 391 | 70 | 12 | No | 2 | 0 | Domestic | 4.959 | 0.05 |
| 392 | 70 | 12 | No | 3 | 0 | Domestic | 4.959 | 0.05 |
| 393 | 70 | 12 | No | 2 | 200 | Domestic | 4.957 | 0.05 |
| 394 | 70 | 12 | No | 1 | 800 | Domestic | 4.951 | 0.049 |
| 395 | 70 | 12 | No | 2 | 800 | Domestic | 4.951 | 0.049 |
| 396 | 50 | 18 | No | 2 | 0 | Imported | 4.949 | 0.049 |
| 397 | 70 | 12 | No | 1 | 1000 | Domestic | 4.949 | 0.049 |
| 398 | 50 | 18 | No | 2 | 200 | Imported | 4.947 | 0.049 |
| 399 | 50 | 18 | No | 1 | 600 | Imported | 4.943 | 0.049 |
| 400 | 50 | 18 | No | 3 | 600 | Imported | 4.943 | 0.049 |
| 401 | 70 | 12 | Severe | 1 | 0 | Domestic | 4.917 | 0.048 |
| 402 | 70 | 12 | Severe | 2 | 0 | Domestic | 4.917 | 0.048 |
| 403 | 70 | 12 | Severe | 3 | 0 | Domestic | 4.917 | 0.048 |
| 404 | 70 | 12 | Severe | 2 | 200 | Domestic | 4.915 | 0.047 |
| 405 | 70 | 12 | Severe | 3 | 200 | Domestic | 4.915 | 0.047 |
| 406 | 70 | 12 | Severe | 1 | 600 | Domestic | 4.911 | 0.047 |
| 407 | 70 | 12 | Severe | 1 | 800 | Domestic | 4.909 | 0.047 |
| 408 | 70 | 12 | Severe | 1 | 1000 | Domestic | 4.907 | 0.047 |
| 409 | 70 | 12 | Severe | 3 | 1000 | Domestic | 4.907 | 0.047 |
| 410 | 70 | 6 | Moderate | 3 | 0 | Domestic | 4.897 | 0.047 |
| 411 | 70 | 6 | Moderate | 3 | 200 | Domestic | 4.895 | 0.047 |
| 412 | 70 | 6 | Moderate | 2 | 600 | Domestic | 4.891 | 0.046 |
| 413 | 70 | 6 | Moderate | 1 | 800 | Domestic | 4.889 | 0.046 |
| 414 | 70 | 6 | Moderate | 1 | 1000 | Domestic | 4.887 | 0.046 |
| 415 | 70 | 6 | Moderate | 3 | 1000 | Domestic | 4.887 | 0.046 |
| 416 | 90 | 18 | Severe | 2 | 200 | Domestic | 4.865 | 0.045 |
| 417 | 90 | 18 | Severe | 1 | 400 | Domestic | 4.863 | 0.045 |
| 418 | 90 | 18 | Severe | 2 | 400 | Domestic | 4.863 | 0.045 |
| 419 | 90 | 18 | Severe | 1 | 600 | Domestic | 4.861 | 0.045 |
| 420 | 90 | 18 | Severe | 3 | 600 | Domestic | 4.861 | 0.045 |
| 421 | 90 | 18 | Severe | 3 | 800 | Domestic | 4.859 | 0.045 |
| 422 | 90 | 18 | Severe | 3 | 1000 | Domestic | 4.857 | 0.045 |
| 423 | 90 | 12 | Severe | 1 | 200 | Imported | 4.815 | 0.043 |
| 424 | 90 | 12 | Severe | 2 | 200 | Imported | 4.815 | 0.043 |
| 425 | 90 | 12 | Severe | 1 | 400 | Imported | 4.813 | 0.043 |
| 426 | 90 | 12 | Severe | 3 | 400 | Imported | 4.813 | 0.043 |
| 427 | 90 | 12 | Severe | 1 | 1000 | Imported | 4.807 | 0.043 |
| 428 | 90 | 6 | Moderate | 2 | 0 | Imported | 4.797 | 0.042 |
| 429 | 70 | 18 | Moderate | 1 | 0 | Imported | 4.794 | 0.042 |
| 430 | 70 | 18 | Moderate | 2 | 0 | Imported | 4.794 | 0.042 |
| 431 | 90 | 6 | Moderate | 3 | 600 | Imported | 4.791 | 0.042 |
| 432 | 90 | 6 | Moderate | 3 | 800 | Imported | 4.789 | 0.042 |
| 433 | 70 | 18 | Moderate | 2 | 600 | Imported | 4.788 | 0.042 |
| 434 | 90 | 6 | Moderate | 3 | 1000 | Imported | 4.787 | 0.042 |
| 435 | 70 | 18 | Moderate | 2 | 800 | Imported | 4.786 | 0.042 |
| 436 | 70 | 18 | Moderate | 3 | 800 | Imported | 4.786 | 0.042 |
| 437 | 70 | 18 | Moderate | 3 | 1000 | Imported | 4.784 | 0.042 |
| 438 | 50 | 18 | No | 3 | 0 | Domestic | 4.771 | 0.041 |
| 439 | 50 | 18 | No | 1 | 200 | Domestic | 4.769 | 0.041 |
| 440 | 50 | 18 | No | 3 | 400 | Domestic | 4.767 | 0.041 |
| 441 | 50 | 18 | No | 2 | 600 | Domestic | 4.765 | 0.041 |
| 442 | 50 | 18 | No | 1 | 800 | Domestic | 4.763 | 0.041 |
| 443 | 50 | 18 | No | 1 | 1000 | Domestic | 4.761 | 0.041 |
| 444 | 50 | 18 | No | 2 | 1000 | Domestic | 4.761 | 0.041 |
| 445 | 50 | 12 | No | 2 | 0 | Imported | 4.721 | 0.039 |
| 446 | 50 | 12 | No | 3 | 0 | Imported | 4.721 | 0.039 |
| 447 | 50 | 12 | No | 3 | 200 | Imported | 4.719 | 0.039 |
| 448 | 50 | 12 | No | 2 | 400 | Imported | 4.717 | 0.039 |
| 449 | 50 | 12 | No | 2 | 600 | Imported | 4.715 | 0.039 |
| 450 | 50 | 12 | No | 3 | 1000 | Imported | 4.711 | 0.039 |
| 451 | 70 | 6 | No | 2 | 0 | Imported | 4.646 | 0.036 |
| 452 | 70 | 6 | No | 3 | 0 | Imported | 4.646 | 0.036 |
| 453 | 70 | 6 | No | 1 | 400 | Imported | 4.642 | 0.036 |
| 454 | 70 | 6 | No | 1 | 600 | Imported | 4.64 | 0.036 |
| 455 | 70 | 6 | No | 3 | 600 | Imported | 4.64 | 0.036 |
| 456 | 90 | 12 | Severe | 1 | 0 | Domestic | 4.639 | 0.036 |
| 457 | 70 | 6 | No | 3 | 800 | Imported | 4.638 | 0.036 |
| 458 | 90 | 12 | Severe | 3 | 200 | Domestic | 4.637 | 0.036 |
| 459 | 90 | 12 | Severe | 3 | 800 | Domestic | 4.631 | 0.036 |
| 460 | 90 | 12 | Severe | 3 | 1000 | Domestic | 4.629 | 0.036 |
| 461 | 90 | 6 | Moderate | 3 | 200 | Domestic | 4.617 | 0.035 |
| 462 | 70 | 18 | Moderate | 3 | 0 | Domestic | 4.616 | 0.035 |
| 463 | 90 | 6 | Moderate | 2 | 400 | Domestic | 4.615 | 0.035 |
| 464 | 90 | 6 | Moderate | 3 | 400 | Domestic | 4.615 | 0.035 |
| 465 | 70 | 18 | Moderate | 3 | 200 | Domestic | 4.614 | 0.035 |
| 466 | 90 | 6 | Moderate | 2 | 600 | Domestic | 4.613 | 0.035 |
| 467 | 70 | 18 | Moderate | 3 | 400 | Domestic | 4.612 | 0.035 |
| 468 | 70 | 18 | Moderate | 1 | 600 | Domestic | 4.61 | 0.035 |
| 469 | 70 | 18 | Moderate | 3 | 600 | Domestic | 4.61 | 0.035 |
| 470 | 90 | 6 | Moderate | 1 | 1000 | Domestic | 4.609 | 0.035 |
| 471 | 70 | 18 | Moderate | 1 | 1000 | Domestic | 4.606 | 0.035 |
| 472 | 70 | 6 | Severe | 2 | 400 | Imported | 4.6 | 0.035 |
| 473 | 70 | 6 | Severe | 1 | 1000 | Imported | 4.594 | 0.034 |
| 474 | 70 | 12 | Moderate | 2 | 0 | Imported | 4.566 | 0.033 |
| 475 | 70 | 12 | Moderate | 1 | 400 | Imported | 4.562 | 0.033 |
| 476 | 70 | 12 | Moderate | 3 | 400 | Imported | 4.562 | 0.033 |
| 477 | 70 | 12 | Moderate | 2 | 800 | Imported | 4.558 | 0.033 |
| 478 | 70 | 12 | Moderate | 2 | 1000 | Imported | 4.556 | 0.033 |
| 479 | 50 | 12 | No | 1 | 200 | Domestic | 4.541 | 0.033 |
| 480 | 50 | 12 | No | 1 | 400 | Domestic | 4.539 | 0.033 |
| 481 | 50 | 12 | No | 1 | 600 | Domestic | 4.537 | 0.033 |
| 482 | 50 | 12 | No | 3 | 600 | Domestic | 4.537 | 0.033 |
| 483 | 50 | 12 | No | 1 | 800 | Domestic | 4.535 | 0.032 |
| 484 | 50 | 12 | No | 2 | 800 | Domestic | 4.535 | 0.032 |
| 485 | 50 | 12 | No | 1 | 1000 | Domestic | 4.533 | 0.032 |
| 486 | 50 | 12 | No | 2 | 1000 | Domestic | 4.533 | 0.032 |
| 487 | 70 | 6 | No | 2 | 600 | Domestic | 4.462 | 0.03 |
| 488 | 70 | 6 | No | 1 | 800 | Domestic | 4.46 | 0.03 |
| 489 | 70 | 6 | No | 1 | 1000 | Domestic | 4.458 | 0.03 |
| 490 | 70 | 6 | No | 2 | 1000 | Domestic | 4.458 | 0.03 |
| 491 | 70 | 6 | Severe | 3 | 0 | Domestic | 4.426 | 0.029 |
| 492 | 70 | 6 | Severe | 1 | 200 | Domestic | 4.424 | 0.029 |
| 493 | 70 | 6 | Severe | 1 | 400 | Domestic | 4.422 | 0.029 |
| 494 | 70 | 6 | Severe | 3 | 400 | Domestic | 4.422 | 0.029 |
| 495 | 70 | 6 | Severe | 1 | 800 | Domestic | 4.418 | 0.029 |
| 496 | 70 | 6 | Severe | 2 | 1000 | Domestic | 4.416 | 0.029 |
| 497 | 70 | 6 | Severe | 3 | 1000 | Domestic | 4.416 | 0.029 |
| 498 | 70 | 12 | Moderate | 1 | 0 | Domestic | 4.388 | 0.028 |
| 499 | 70 | 12 | Moderate | 3 | 0 | Domestic | 4.388 | 0.028 |
| 500 | 70 | 12 | Moderate | 2 | 200 | Domestic | 4.386 | 0.028 |
| 501 | 70 | 12 | Moderate | 3 | 200 | Domestic | 4.386 | 0.028 |
| 502 | 70 | 12 | Moderate | 1 | 800 | Domestic | 4.38 | 0.028 |
| 503 | 50 | 18 | Moderate | 1 | 0 | Imported | 4.378 | 0.028 |
| 504 | 70 | 12 | Moderate | 3 | 1000 | Domestic | 4.378 | 0.028 |
| 505 | 50 | 18 | Moderate | 3 | 400 | Imported | 4.374 | 0.028 |
| 506 | 50 | 18 | Moderate | 3 | 800 | Imported | 4.37 | 0.028 |
| 507 | 50 | 18 | Moderate | 3 | 1000 | Imported | 4.368 | 0.027 |
| 508 | 70 | 18 | No | 3 | 0 | Imported | 4.365 | 0.027 |
| 509 | 70 | 18 | No | 2 | 200 | Imported | 4.363 | 0.027 |
| 510 | 70 | 18 | No | 2 | 400 | Imported | 4.361 | 0.027 |
| 511 | 70 | 18 | No | 2 | 600 | Imported | 4.359 | 0.027 |
| 512 | 70 | 18 | No | 2 | 1000 | Imported | 4.355 | 0.027 |
| 513 | 70 | 18 | No | 3 | 1000 | Imported | 4.355 | 0.027 |
| 514 | 90 | 6 | Severe | 3 | 0 | Imported | 4.326 | 0.026 |
| 515 | 90 | 6 | Severe | 1 | 200 | Imported | 4.324 | 0.026 |
| 516 | 90 | 6 | Severe | 2 | 200 | Imported | 4.324 | 0.026 |
| 517 | 90 | 6 | Severe | 3 | 200 | Imported | 4.324 | 0.026 |
| 518 | 70 | 18 | Severe | 2 | 0 | Imported | 4.323 | 0.026 |
| 519 | 90 | 6 | Severe | 1 | 400 | Imported | 4.322 | 0.026 |
| 520 | 70 | 18 | Severe | 2 | 200 | Imported | 4.321 | 0.026 |
| 521 | 90 | 6 | Severe | 2 | 600 | Imported | 4.32 | 0.026 |
| 522 | 90 | 6 | Severe | 3 | 600 | Imported | 4.32 | 0.026 |
| 523 | 70 | 18 | Severe | 3 | 400 | Imported | 4.319 | 0.026 |
| 524 | 90 | 6 | Severe | 2 | 800 | Imported | 4.318 | 0.026 |
| 525 | 90 | 6 | Severe | 3 | 800 | Imported | 4.318 | 0.026 |
| 526 | 70 | 18 | Severe | 1 | 600 | Imported | 4.317 | 0.026 |
| 527 | 90 | 6 | Severe | 2 | 1000 | Imported | 4.316 | 0.026 |
| 528 | 70 | 18 | Severe | 1 | 800 | Imported | 4.315 | 0.026 |
| 529 | 70 | 18 | Severe | 2 | 800 | Imported | 4.315 | 0.026 |
| 530 | 50 | 6 | No | 2 | 0 | Imported | 4.23 | 0.024 |
| 531 | 50 | 6 | No | 1 | 600 | Imported | 4.224 | 0.024 |
| 532 | 50 | 18 | Moderate | 2 | 0 | Domestic | 4.2 | 0.023 |
| 533 | 50 | 18 | Moderate | 3 | 0 | Domestic | 4.2 | 0.023 |
| 534 | 50 | 18 | Moderate | 3 | 200 | Domestic | 4.198 | 0.023 |
| 535 | 50 | 18 | Moderate | 1 | 600 | Domestic | 4.194 | 0.023 |
| 536 | 50 | 18 | Moderate | 2 | 600 | Domestic | 4.194 | 0.023 |
| 537 | 50 | 18 | Moderate | 1 | 800 | Domestic | 4.192 | 0.023 |
| 538 | 50 | 18 | Moderate | 2 | 800 | Domestic | 4.192 | 0.023 |
| 539 | 50 | 18 | Moderate | 2 | 1000 | Domestic | 4.19 | 0.023 |
| 540 | 70 | 18 | No | 1 | 0 | Domestic | 4.187 | 0.023 |
| 541 | 70 | 18 | No | 2 | 0 | Domestic | 4.187 | 0.023 |
| 542 | 70 | 18 | No | 1 | 200 | Domestic | 4.185 | 0.023 |
| 543 | 70 | 18 | No | 3 | 200 | Domestic | 4.185 | 0.023 |
| 544 | 70 | 18 | No | 3 | 400 | Domestic | 4.183 | 0.023 |
| 545 | 70 | 18 | No | 3 | 600 | Domestic | 4.181 | 0.023 |
| 546 | 70 | 18 | No | 1 | 1000 | Domestic | 4.177 | 0.023 |
| 547 | 50 | 12 | Moderate | 1 | 400 | Imported | 4.146 | 0.022 |
| 548 | 50 | 12 | Moderate | 3 | 400 | Imported | 4.146 | 0.022 |
| 549 | 70 | 18 | Severe | 1 | 0 | Domestic | 4.145 | 0.022 |
| 550 | 70 | 18 | Severe | 3 | 0 | Domestic | 4.145 | 0.022 |
| 551 | 50 | 12 | Moderate | 1 | 600 | Imported | 4.144 | 0.022 |
| 552 | 90 | 6 | Severe | 2 | 400 | Domestic | 4.144 | 0.022 |
| 553 | 90 | 6 | Severe | 3 | 400 | Domestic | 4.144 | 0.022 |
| 554 | 90 | 6 | Severe | 1 | 600 | Domestic | 4.142 | 0.022 |
| 555 | 70 | 18 | Severe | 1 | 400 | Domestic | 4.141 | 0.022 |
| 556 | 70 | 18 | Severe | 2 | 400 | Domestic | 4.141 | 0.022 |
| 557 | 50 | 12 | Moderate | 2 | 1000 | Imported | 4.14 | 0.022 |
| 558 | 90 | 6 | Severe | 1 | 800 | Domestic | 4.14 | 0.022 |
| 559 | 70 | 18 | Severe | 3 | 600 | Domestic | 4.139 | 0.022 |
| 560 | 90 | 6 | Severe | 1 | 1000 | Domestic | 4.138 | 0.022 |
| 561 | 70 | 12 | No | 1 | 0 | Imported | 4.137 | 0.022 |
| 562 | 70 | 12 | No | 3 | 0 | Imported | 4.137 | 0.022 |
| 563 | 70 | 12 | No | 1 | 600 | Imported | 4.131 | 0.022 |
| 564 | 70 | 12 | No | 1 | 1000 | Imported | 4.127 | 0.022 |
| 565 | 70 | 12 | Severe | 2 | 0 | Imported | 4.095 | 0.021 |
| 566 | 70 | 12 | Severe | 3 | 0 | Imported | 4.095 | 0.021 |
| 567 | 70 | 12 | Severe | 3 | 200 | Imported | 4.093 | 0.021 |
| 568 | 70 | 12 | Severe | 1 | 400 | Imported | 4.091 | 0.021 |
| 569 | 70 | 12 | Severe | 1 | 1000 | Imported | 4.085 | 0.021 |
| 570 | 70 | 12 | Severe | 3 | 1000 | Imported | 4.085 | 0.021 |
| 571 | 70 | 6 | Moderate | 3 | 0 | Imported | 4.075 | 0.021 |
| 572 | 70 | 6 | Moderate | 3 | 200 | Imported | 4.073 | 0.02 |
| 573 | 70 | 6 | Moderate | 2 | 600 | Imported | 4.069 | 0.02 |
| 574 | 70 | 6 | Moderate | 1 | 800 | Imported | 4.067 | 0.02 |
| 575 | 70 | 6 | Moderate | 2 | 800 | Imported | 4.067 | 0.02 |
| 576 | 70 | 6 | Moderate | 3 | 800 | Imported | 4.067 | 0.02 |
| 577 | 70 | 6 | Moderate | 1 | 1000 | Imported | 4.065 | 0.02 |
| 578 | 50 | 6 | No | 1 | 0 | Domestic | 4.052 | 0.02 |
| 579 | 50 | 6 | No | 3 | 0 | Domestic | 4.052 | 0.02 |
| 580 | 50 | 6 | No | 1 | 400 | Domestic | 4.048 | 0.02 |
| 581 | 50 | 6 | No | 2 | 600 | Domestic | 4.046 | 0.02 |
| 582 | 50 | 6 | No | 3 | 600 | Domestic | 4.046 | 0.02 |
| 583 | 50 | 6 | No | 2 | 800 | Domestic | 4.044 | 0.02 |
| 584 | 50 | 6 | No | 3 | 800 | Domestic | 4.044 | 0.02 |
| 585 | 50 | 6 | No | 3 | 1000 | Domestic | 4.042 | 0.02 |
| 586 | 50 | 12 | Moderate | 1 | 0 | Domestic | 3.972 | 0.018 |
| 587 | 50 | 12 | Moderate | 1 | 200 | Domestic | 3.97 | 0.018 |
| 588 | 50 | 12 | Moderate | 2 | 200 | Domestic | 3.97 | 0.018 |
| 589 | 50 | 12 | Moderate | 2 | 400 | Domestic | 3.968 | 0.018 |
| 590 | 50 | 12 | Moderate | 2 | 800 | Domestic | 3.964 | 0.018 |
| 591 | 50 | 12 | Moderate | 1 | 1000 | Domestic | 3.962 | 0.018 |
| 592 | 50 | 12 | Moderate | 3 | 1000 | Domestic | 3.962 | 0.018 |
| 593 | 70 | 12 | No | 3 | 400 | Domestic | 3.955 | 0.018 |
| 594 | 70 | 12 | No | 3 | 600 | Domestic | 3.953 | 0.018 |
| 595 | 50 | 18 | No | 3 | 0 | Imported | 3.949 | 0.018 |
| 596 | 70 | 12 | No | 2 | 1000 | Domestic | 3.949 | 0.018 |
| 597 | 50 | 18 | No | 1 | 200 | Imported | 3.947 | 0.018 |
| 598 | 50 | 18 | No | 1 | 400 | Imported | 3.945 | 0.018 |
| 599 | 50 | 18 | No | 2 | 400 | Imported | 3.945 | 0.018 |
| 600 | 50 | 18 | No | 1 | 800 | Imported | 3.941 | 0.018 |
| 601 | 50 | 18 | No | 3 | 800 | Imported | 3.941 | 0.018 |
| 602 | 50 | 18 | No | 1 | 1000 | Imported | 3.939 | 0.018 |
| 603 | 50 | 18 | No | 3 | 1000 | Imported | 3.939 | 0.018 |
| 604 | 70 | 12 | Severe | 1 | 200 | Domestic | 3.915 | 0.017 |
| 605 | 70 | 12 | Severe | 2 | 400 | Domestic | 3.913 | 0.017 |
| 606 | 70 | 12 | Severe | 3 | 400 | Domestic | 3.913 | 0.017 |
| 607 | 70 | 12 | Severe | 2 | 600 | Domestic | 3.911 | 0.017 |
| 608 | 70 | 12 | Severe | 2 | 800 | Domestic | 3.909 | 0.017 |
| 609 | 70 | 12 | Severe | 3 | 800 | Domestic | 3.909 | 0.017 |
| 610 | 70 | 12 | Severe | 2 | 1000 | Domestic | 3.907 | 0.017 |
| 611 | 50 | 18 | Severe | 2 | 200 | Imported | 3.905 | 0.017 |
| 612 | 50 | 18 | Severe | 1 | 400 | Imported | 3.903 | 0.017 |
| 613 | 50 | 18 | Severe | 1 | 600 | Imported | 3.901 | 0.017 |
| 614 | 50 | 18 | Severe | 2 | 800 | Imported | 3.899 | 0.017 |
| 615 | 50 | 18 | Severe | 2 | 1000 | Imported | 3.897 | 0.017 |
| 616 | 70 | 6 | Moderate | 1 | 0 | Domestic | 3.897 | 0.017 |
| 617 | 70 | 6 | Moderate | 2 | 0 | Domestic | 3.897 | 0.017 |
| 618 | 70 | 6 | Moderate | 1 | 200 | Domestic | 3.895 | 0.017 |
| 619 | 70 | 6 | Moderate | 1 | 400 | Domestic | 3.893 | 0.017 |
| 620 | 70 | 6 | Moderate | 2 | 400 | Domestic | 3.893 | 0.017 |
| 621 | 70 | 6 | Moderate | 3 | 400 | Domestic | 3.893 | 0.017 |
| 622 | 70 | 6 | Moderate | 1 | 600 | Domestic | 3.891 | 0.017 |
| 623 | 70 | 18 | Moderate | 1 | 200 | Imported | 3.792 | 0.015 |
| 624 | 70 | 18 | Moderate | 2 | 200 | Imported | 3.792 | 0.015 |
| 625 | 70 | 18 | Moderate | 3 | 200 | Imported | 3.792 | 0.015 |
| 626 | 70 | 18 | Moderate | 1 | 400 | Imported | 3.79 | 0.015 |
| 627 | 70 | 18 | Moderate | 2 | 400 | Imported | 3.79 | 0.015 |
| 628 | 70 | 18 | Moderate | 1 | 600 | Imported | 3.788 | 0.015 |
| 629 | 70 | 18 | Moderate | 1 | 800 | Imported | 3.786 | 0.015 |
| 630 | 70 | 18 | Moderate | 1 | 1000 | Imported | 3.784 | 0.015 |
| 631 | 70 | 18 | Moderate | 2 | 1000 | Imported | 3.784 | 0.015 |
| 632 | 50 | 18 | No | 1 | 0 | Domestic | 3.771 | 0.015 |
| 633 | 50 | 18 | No | 2 | 0 | Domestic | 3.771 | 0.015 |
| 634 | 50 | 18 | No | 3 | 200 | Domestic | 3.769 | 0.015 |
| 635 | 50 | 18 | No | 2 | 800 | Domestic | 3.763 | 0.015 |
| 636 | 50 | 18 | Severe | 1 | 0 | Domestic | 3.729 | 0.015 |
| 637 | 50 | 18 | Severe | 1 | 200 | Domestic | 3.727 | 0.014 |
| 638 | 50 | 18 | Severe | 3 | 200 | Domestic | 3.727 | 0.014 |
| 639 | 50 | 18 | Severe | 2 | 400 | Domestic | 3.725 | 0.014 |
| 640 | 50 | 18 | Severe | 2 | 600 | Domestic | 3.723 | 0.014 |
| 641 | 50 | 18 | Severe | 3 | 600 | Domestic | 3.723 | 0.014 |
| 642 | 50 | 12 | No | 1 | 0 | Imported | 3.721 | 0.014 |
| 643 | 50 | 18 | Severe | 3 | 800 | Domestic | 3.721 | 0.014 |
| 644 | 50 | 18 | Severe | 1 | 1000 | Domestic | 3.719 | 0.014 |
| 645 | 50 | 12 | No | 1 | 600 | Imported | 3.715 | 0.014 |
| 646 | 50 | 12 | No | 3 | 600 | Imported | 3.715 | 0.014 |
| 647 | 50 | 12 | No | 1 | 800 | Imported | 3.713 | 0.014 |
| 648 | 50 | 12 | No | 2 | 800 | Imported | 3.713 | 0.014 |
| 649 | 50 | 12 | No | 3 | 800 | Imported | 3.713 | 0.014 |
| 650 | 50 | 12 | No | 2 | 1000 | Imported | 3.711 | 0.014 |
| 651 | 50 | 12 | Severe | 3 | 0 | Imported | 3.679 | 0.014 |
| 652 | 50 | 12 | Severe | 3 | 200 | Imported | 3.677 | 0.014 |
| 653 | 50 | 12 | Severe | 2 | 800 | Imported | 3.671 | 0.014 |
| 654 | 50 | 12 | Severe | 3 | 800 | Imported | 3.671 | 0.014 |
| 655 | 50 | 12 | Severe | 3 | 1000 | Imported | 3.669 | 0.014 |
| 656 | 50 | 6 | Moderate | 3 | 200 | Imported | 3.657 | 0.013 |
| 657 | 50 | 6 | Moderate | 1 | 400 | Imported | 3.655 | 0.013 |
| 658 | 50 | 6 | Moderate | 2 | 400 | Imported | 3.655 | 0.013 |
| 659 | 50 | 6 | Moderate | 2 | 600 | Imported | 3.653 | 0.013 |
| 660 | 50 | 6 | Moderate | 1 | 800 | Imported | 3.651 | 0.013 |
| 661 | 50 | 6 | Moderate | 3 | 800 | Imported | 3.651 | 0.013 |
| 662 | 50 | 6 | Moderate | 1 | 1000 | Imported | 3.649 | 0.013 |
| 663 | 50 | 6 | Moderate | 3 | 1000 | Imported | 3.649 | 0.013 |
| 664 | 70 | 6 | No | 1 | 0 | Imported | 3.646 | 0.013 |
| 665 | 70 | 6 | No | 2 | 200 | Imported | 3.644 | 0.013 |
| 666 | 70 | 6 | No | 3 | 200 | Imported | 3.644 | 0.013 |
| 667 | 70 | 6 | No | 2 | 400 | Imported | 3.642 | 0.013 |
| 668 | 70 | 6 | No | 3 | 400 | Imported | 3.642 | 0.013 |
| 669 | 70 | 6 | No | 2 | 600 | Imported | 3.64 | 0.013 |
| 670 | 70 | 6 | No | 2 | 800 | Imported | 3.638 | 0.013 |
| 671 | 70 | 6 | No | 1 | 1000 | Imported | 3.636 | 0.013 |
| 672 | 70 | 6 | No | 2 | 1000 | Imported | 3.636 | 0.013 |
| 673 | 70 | 6 | No | 3 | 1000 | Imported | 3.636 | 0.013 |
| 674 | 70 | 18 | Moderate | 1 | 0 | Domestic | 3.616 | 0.013 |
| 675 | 70 | 18 | Moderate | 2 | 0 | Domestic | 3.616 | 0.013 |
| 676 | 70 | 6 | Severe | 2 | 0 | Imported | 3.604 | 0.013 |
| 677 | 70 | 6 | Severe | 2 | 200 | Imported | 3.602 | 0.013 |
| 678 | 70 | 6 | Severe | 1 | 400 | Imported | 3.6 | 0.013 |
| 679 | 70 | 6 | Severe | 2 | 800 | Imported | 3.596 | 0.013 |
| 680 | 70 | 6 | Severe | 3 | 800 | Imported | 3.596 | 0.013 |
| 681 | 70 | 12 | Moderate | 2 | 200 | Imported | 3.564 | 0.012 |
| 682 | 70 | 12 | Moderate | 3 | 200 | Imported | 3.564 | 0.012 |
| 683 | 70 | 12 | Moderate | 2 | 400 | Imported | 3.562 | 0.012 |
| 684 | 70 | 12 | Moderate | 1 | 600 | Imported | 3.56 | 0.012 |
| 685 | 70 | 12 | Moderate | 3 | 600 | Imported | 3.56 | 0.012 |
| 686 | 70 | 12 | Moderate | 1 | 800 | Imported | 3.558 | 0.012 |
| 687 | 70 | 12 | Moderate | 3 | 800 | Imported | 3.558 | 0.012 |
| 688 | 70 | 12 | Moderate | 1 | 1000 | Imported | 3.556 | 0.012 |
| 689 | 70 | 12 | Moderate | 3 | 1000 | Imported | 3.556 | 0.012 |
| 690 | 50 | 12 | No | 2 | 0 | Domestic | 3.543 | 0.012 |
| 691 | 50 | 12 | No | 3 | 0 | Domestic | 3.543 | 0.012 |
| 692 | 50 | 12 | No | 2 | 200 | Domestic | 3.541 | 0.012 |
| 693 | 50 | 12 | No | 2 | 400 | Domestic | 3.539 | 0.012 |
| 694 | 50 | 12 | No | 3 | 400 | Domestic | 3.539 | 0.012 |
| 695 | 50 | 12 | No | 2 | 600 | Domestic | 3.537 | 0.012 |
| 696 | 50 | 12 | Severe | 1 | 0 | Domestic | 3.501 | 0.012 |
| 697 | 50 | 12 | Severe | 2 | 0 | Domestic | 3.501 | 0.012 |
| 698 | 50 | 12 | Severe | 2 | 200 | Domestic | 3.499 | 0.012 |
| 699 | 50 | 12 | Severe | 1 | 400 | Domestic | 3.497 | 0.012 |
| 700 | 50 | 12 | Severe | 2 | 400 | Domestic | 3.497 | 0.012 |
| 701 | 50 | 12 | Severe | 3 | 400 | Domestic | 3.497 | 0.012 |
| 702 | 50 | 12 | Severe | 2 | 600 | Domestic | 3.495 | 0.011 |
| 703 | 50 | 12 | Severe | 3 | 600 | Domestic | 3.495 | 0.011 |
| 704 | 50 | 12 | Severe | 1 | 1000 | Domestic | 3.491 | 0.011 |
| 705 | 50 | 6 | Moderate | 1 | 0 | Domestic | 3.481 | 0.011 |
| 706 | 50 | 6 | Moderate | 2 | 0 | Domestic | 3.481 | 0.011 |
| 707 | 50 | 6 | Moderate | 1 | 200 | Domestic | 3.479 | 0.011 |
| 708 | 50 | 6 | Moderate | 2 | 200 | Domestic | 3.479 | 0.011 |
| 709 | 50 | 6 | Moderate | 3 | 400 | Domestic | 3.477 | 0.011 |
| 710 | 50 | 6 | Moderate | 3 | 600 | Domestic | 3.475 | 0.011 |
| 711 | 50 | 6 | Moderate | 2 | 1000 | Domestic | 3.471 | 0.011 |
| 712 | 70 | 6 | No | 2 | 0 | Domestic | 3.468 | 0.011 |
| 713 | 70 | 6 | No | 3 | 0 | Domestic | 3.468 | 0.011 |
| 714 | 70 | 6 | No | 1 | 200 | Domestic | 3.466 | 0.011 |
| 715 | 70 | 6 | No | 1 | 400 | Domestic | 3.464 | 0.011 |
| 716 | 70 | 6 | No | 1 | 600 | Domestic | 3.462 | 0.011 |
| 717 | 70 | 6 | Severe | 1 | 0 | Domestic | 3.426 | 0.011 |
| 718 | 70 | 6 | Severe | 3 | 200 | Domestic | 3.424 | 0.011 |
| 719 | 70 | 6 | Severe | 2 | 400 | Domestic | 3.422 | 0.011 |
| 720 | 70 | 6 | Severe | 1 | 600 | Domestic | 3.42 | 0.011 |
| 721 | 70 | 6 | Severe | 2 | 600 | Domestic | 3.42 | 0.011 |
| 722 | 70 | 6 | Severe | 3 | 600 | Domestic | 3.42 | 0.011 |
| 723 | 70 | 12 | Moderate | 1 | 200 | Domestic | 3.386 | 0.01 |
| 724 | 70 | 12 | Moderate | 1 | 400 | Domestic | 3.384 | 0.01 |
| 725 | 70 | 12 | Moderate | 3 | 400 | Domestic | 3.384 | 0.01 |
| 726 | 70 | 12 | Moderate | 2 | 600 | Domestic | 3.382 | 0.01 |
| 727 | 70 | 12 | Moderate | 2 | 800 | Domestic | 3.38 | 0.01 |
| 728 | 50 | 18 | Moderate | 3 | 0 | Imported | 3.378 | 0.01 |
| 729 | 70 | 12 | Moderate | 2 | 1000 | Domestic | 3.378 | 0.01 |
| 730 | 50 | 18 | Moderate | 1 | 400 | Imported | 3.374 | 0.01 |
| 731 | 50 | 18 | Moderate | 2 | 400 | Imported | 3.374 | 0.01 |
| 732 | 50 | 18 | Moderate | 2 | 1000 | Imported | 3.368 | 0.01 |
| 733 | 70 | 18 | Severe | 3 | 0 | Imported | 3.323 | 0.01 |
| 734 | 70 | 18 | Severe | 3 | 200 | Imported | 3.321 | 0.01 |
| 735 | 70 | 18 | Severe | 1 | 400 | Imported | 3.319 | 0.01 |
| 736 | 70 | 18 | Severe | 3 | 600 | Imported | 3.317 | 0.01 |
| 737 | 70 | 18 | Severe | 3 | 800 | Imported | 3.315 | 0.01 |
| 738 | 70 | 18 | Severe | 2 | 1000 | Imported | 3.313 | 0.01 |
| 739 | 50 | 6 | No | 1 | 0 | Imported | 3.23 | 0.009 |
| 740 | 50 | 6 | No | 2 | 400 | Imported | 3.226 | 0.009 |
| 741 | 50 | 6 | No | 3 | 400 | Imported | 3.226 | 0.009 |
| 742 | 50 | 6 | No | 1 | 800 | Imported | 3.222 | 0.009 |
| 743 | 50 | 6 | No | 1 | 1000 | Imported | 3.22 | 0.009 |
| 744 | 50 | 6 | No | 3 | 1000 | Imported | 3.22 | 0.009 |
| 745 | 50 | 18 | Moderate | 1 | 0 | Domestic | 3.2 | 0.009 |
| 746 | 50 | 18 | Moderate | 1 | 200 | Domestic | 3.198 | 0.009 |
| 747 | 50 | 18 | Moderate | 2 | 200 | Domestic | 3.198 | 0.009 |
| 748 | 50 | 18 | Moderate | 3 | 400 | Domestic | 3.196 | 0.009 |
| 749 | 50 | 18 | Moderate | 3 | 600 | Domestic | 3.194 | 0.008 |
| 750 | 50 | 18 | Moderate | 3 | 800 | Domestic | 3.192 | 0.008 |
| 751 | 50 | 18 | Moderate | 1 | 1000 | Domestic | 3.19 | 0.008 |
| 752 | 50 | 18 | Moderate | 3 | 1000 | Domestic | 3.19 | 0.008 |
| 753 | 50 | 6 | Severe | 2 | 200 | Imported | 3.186 | 0.008 |
| 754 | 50 | 6 | Severe | 2 | 800 | Imported | 3.18 | 0.008 |
| 755 | 50 | 12 | Moderate | 1 | 0 | Imported | 3.15 | 0.008 |
| 756 | 50 | 12 | Moderate | 3 | 0 | Imported | 3.15 | 0.008 |
| 757 | 50 | 12 | Moderate | 1 | 200 | Imported | 3.148 | 0.008 |
| 758 | 50 | 12 | Moderate | 3 | 200 | Imported | 3.148 | 0.008 |
| 759 | 50 | 12 | Moderate | 2 | 400 | Imported | 3.146 | 0.008 |
| 760 | 70 | 18 | Severe | 1 | 200 | Domestic | 3.143 | 0.008 |
| 761 | 50 | 12 | Moderate | 1 | 800 | Imported | 3.142 | 0.008 |
| 762 | 50 | 12 | Moderate | 3 | 800 | Imported | 3.142 | 0.008 |
| 763 | 70 | 18 | Severe | 2 | 600 | Domestic | 3.139 | 0.008 |
| 764 | 70 | 18 | Severe | 1 | 800 | Domestic | 3.137 | 0.008 |
| 765 | 70 | 18 | Severe | 2 | 800 | Domestic | 3.137 | 0.008 |
| 766 | 70 | 18 | Severe | 1 | 1000 | Domestic | 3.135 | 0.008 |
| 767 | 70 | 18 | Severe | 3 | 1000 | Domestic | 3.135 | 0.008 |
| 768 | 70 | 12 | Severe | 1 | 0 | Imported | 3.095 | 0.008 |
| 769 | 70 | 12 | Severe | 1 | 200 | Imported | 3.093 | 0.008 |
| 770 | 70 | 12 | Severe | 2 | 200 | Imported | 3.093 | 0.008 |
| 771 | 70 | 12 | Severe | 1 | 600 | Imported | 3.089 | 0.008 |
| 772 | 70 | 12 | Severe | 2 | 600 | Imported | 3.089 | 0.008 |
| 773 | 70 | 12 | Severe | 1 | 800 | Imported | 3.087 | 0.008 |
| 774 | 70 | 12 | Severe | 3 | 800 | Imported | 3.087 | 0.008 |
| 775 | 70 | 6 | Moderate | 1 | 200 | Imported | 3.073 | 0.008 |
| 776 | 70 | 6 | Moderate | 2 | 400 | Imported | 3.071 | 0.008 |
| 777 | 70 | 6 | Moderate | 3 | 1000 | Imported | 3.065 | 0.007 |
| 778 | 50 | 6 | No | 2 | 0 | Domestic | 3.052 | 0.007 |
| 779 | 50 | 6 | No | 1 | 200 | Domestic | 3.05 | 0.007 |
| 780 | 50 | 6 | No | 2 | 200 | Domestic | 3.05 | 0.007 |
| 781 | 50 | 6 | No | 3 | 200 | Domestic | 3.05 | 0.007 |
| 782 | 50 | 6 | No | 2 | 1000 | Domestic | 3.042 | 0.007 |
| 783 | 50 | 6 | Severe | 2 | 0 | Domestic | 3.01 | 0.007 |
| 784 | 50 | 6 | Severe | 1 | 200 | Domestic | 3.008 | 0.007 |
| 785 | 50 | 6 | Severe | 3 | 200 | Domestic | 3.008 | 0.007 |
| 786 | 50 | 6 | Severe | 3 | 400 | Domestic | 3.006 | 0.007 |
| 787 | 50 | 6 | Severe | 1 | 600 | Domestic | 3.004 | 0.007 |
| 788 | 50 | 6 | Severe | 1 | 800 | Domestic | 3.002 | 0.007 |
| 789 | 50 | 6 | Severe | 3 | 800 | Domestic | 3.002 | 0.007 |
| 790 | 50 | 12 | Moderate | 2 | 0 | Domestic | 2.972 | 0.007 |
| 791 | 50 | 12 | Moderate | 1 | 400 | Domestic | 2.968 | 0.007 |
| 792 | 50 | 12 | Moderate | 3 | 400 | Domestic | 2.968 | 0.007 |
| 793 | 50 | 12 | Moderate | 2 | 600 | Domestic | 2.966 | 0.007 |
| 794 | 50 | 12 | Moderate | 3 | 600 | Domestic | 2.966 | 0.007 |
| 795 | 50 | 18 | No | 1 | 0 | Imported | 2.949 | 0.007 |
| 796 | 50 | 18 | No | 3 | 200 | Imported | 2.947 | 0.007 |
| 797 | 50 | 18 | No | 3 | 400 | Imported | 2.945 | 0.007 |
| 798 | 50 | 18 | No | 2 | 600 | Imported | 2.943 | 0.007 |
| 799 | 50 | 18 | No | 2 | 800 | Imported | 2.941 | 0.007 |
| 800 | 50 | 18 | No | 2 | 1000 | Imported | 2.939 | 0.007 |
| 801 | 70 | 12 | Severe | 1 | 400 | Domestic | 2.913 | 0.006 |
| 802 | 70 | 12 | Severe | 3 | 600 | Domestic | 2.911 | 0.006 |
| 803 | 50 | 18 | Severe | 1 | 0 | Imported | 2.907 | 0.006 |
| 804 | 50 | 18 | Severe | 2 | 0 | Imported | 2.907 | 0.006 |
| 805 | 50 | 18 | Severe | 3 | 0 | Imported | 2.907 | 0.006 |
| 806 | 50 | 18 | Severe | 1 | 200 | Imported | 2.905 | 0.006 |
| 807 | 50 | 18 | Severe | 2 | 400 | Imported | 2.903 | 0.006 |
| 808 | 50 | 18 | Severe | 2 | 600 | Imported | 2.901 | 0.006 |
| 809 | 50 | 18 | Severe | 3 | 800 | Imported | 2.899 | 0.006 |
| 810 | 50 | 18 | Severe | 1 | 1000 | Imported | 2.897 | 0.006 |
| 811 | 70 | 6 | Moderate | 2 | 200 | Domestic | 2.895 | 0.006 |
| 812 | 70 | 6 | Moderate | 3 | 600 | Domestic | 2.891 | 0.006 |
| 813 | 70 | 6 | Moderate | 2 | 800 | Domestic | 2.889 | 0.006 |
| 814 | 70 | 6 | Moderate | 3 | 800 | Domestic | 2.889 | 0.006 |
| 815 | 70 | 6 | Moderate | 2 | 1000 | Domestic | 2.887 | 0.006 |
| 816 | 50 | 18 | No | 2 | 200 | Domestic | 2.769 | 0.006 |
| 817 | 50 | 18 | No | 1 | 400 | Domestic | 2.767 | 0.006 |
| 818 | 50 | 18 | No | 2 | 400 | Domestic | 2.767 | 0.006 |
| 819 | 50 | 18 | No | 1 | 600 | Domestic | 2.765 | 0.006 |
| 820 | 50 | 18 | No | 3 | 600 | Domestic | 2.765 | 0.006 |
| 821 | 50 | 18 | No | 3 | 800 | Domestic | 2.763 | 0.006 |
| 822 | 50 | 18 | No | 3 | 1000 | Domestic | 2.761 | 0.006 |
| 823 | 50 | 18 | Severe | 1 | 400 | Domestic | 2.725 | 0.005 |
| 824 | 50 | 18 | Severe | 3 | 400 | Domestic | 2.725 | 0.005 |
| 825 | 50 | 18 | Severe | 1 | 800 | Domestic | 2.721 | 0.005 |
| 826 | 50 | 18 | Severe | 2 | 800 | Domestic | 2.721 | 0.005 |
| 827 | 50 | 12 | No | 1 | 200 | Imported | 2.719 | 0.005 |
| 828 | 50 | 12 | No | 2 | 200 | Imported | 2.719 | 0.005 |
| 829 | 50 | 18 | Severe | 3 | 1000 | Domestic | 2.719 | 0.005 |
| 830 | 50 | 12 | No | 1 | 400 | Imported | 2.717 | 0.005 |
| 831 | 50 | 12 | No | 3 | 400 | Imported | 2.717 | 0.005 |
| 832 | 50 | 12 | No | 1 | 1000 | Imported | 2.711 | 0.005 |
| 833 | 50 | 12 | Severe | 2 | 200 | Imported | 2.677 | 0.005 |
| 834 | 50 | 12 | Severe | 2 | 400 | Imported | 2.675 | 0.005 |
| 835 | 50 | 12 | Severe | 3 | 400 | Imported | 2.675 | 0.005 |
| 836 | 50 | 12 | Severe | 3 | 600 | Imported | 2.673 | 0.005 |
| 837 | 50 | 12 | Severe | 1 | 800 | Imported | 2.671 | 0.005 |
| 838 | 50 | 6 | Moderate | 1 | 0 | Imported | 2.659 | 0.005 |
| 839 | 50 | 6 | Moderate | 2 | 0 | Imported | 2.659 | 0.005 |
| 840 | 50 | 6 | Moderate | 3 | 0 | Imported | 2.659 | 0.005 |
| 841 | 50 | 6 | Moderate | 2 | 200 | Imported | 2.657 | 0.005 |
| 842 | 50 | 6 | Moderate | 3 | 400 | Imported | 2.655 | 0.005 |
| 843 | 50 | 6 | Moderate | 3 | 600 | Imported | 2.653 | 0.005 |
| 844 | 50 | 6 | Moderate | 2 | 1000 | Imported | 2.649 | 0.005 |
| 845 | 70 | 6 | Severe | 1 | 0 | Imported | 2.604 | 0.005 |
| 846 | 70 | 6 | Severe | 3 | 0 | Imported | 2.604 | 0.005 |
| 847 | 70 | 6 | Severe | 1 | 200 | Imported | 2.602 | 0.005 |
| 848 | 70 | 6 | Severe | 3 | 200 | Imported | 2.602 | 0.005 |
| 849 | 70 | 6 | Severe | 3 | 400 | Imported | 2.6 | 0.005 |
| 850 | 70 | 6 | Severe | 1 | 600 | Imported | 2.598 | 0.005 |
| 851 | 70 | 6 | Severe | 2 | 600 | Imported | 2.598 | 0.005 |
| 852 | 70 | 6 | Severe | 3 | 600 | Imported | 2.598 | 0.005 |
| 853 | 70 | 6 | Severe | 1 | 800 | Imported | 2.596 | 0.005 |
| 854 | 70 | 6 | Severe | 2 | 1000 | Imported | 2.594 | 0.005 |
| 855 | 70 | 6 | Severe | 3 | 1000 | Imported | 2.594 | 0.005 |
| 856 | 50 | 12 | No | 1 | 0 | Domestic | 2.543 | 0.004 |
| 857 | 50 | 12 | No | 3 | 200 | Domestic | 2.541 | 0.004 |
| 858 | 50 | 12 | No | 3 | 800 | Domestic | 2.535 | 0.004 |
| 859 | 50 | 12 | No | 3 | 1000 | Domestic | 2.533 | 0.004 |
| 860 | 50 | 12 | Severe | 3 | 0 | Domestic | 2.501 | 0.004 |
| 861 | 50 | 12 | Severe | 1 | 200 | Domestic | 2.499 | 0.004 |
| 862 | 50 | 12 | Severe | 3 | 200 | Domestic | 2.499 | 0.004 |
| 863 | 50 | 12 | Severe | 1 | 600 | Domestic | 2.495 | 0.004 |
| 864 | 50 | 12 | Severe | 2 | 800 | Domestic | 2.493 | 0.004 |
| 865 | 50 | 12 | Severe | 3 | 800 | Domestic | 2.493 | 0.004 |
| 866 | 50 | 12 | Severe | 2 | 1000 | Domestic | 2.491 | 0.004 |
| 867 | 50 | 6 | Moderate | 1 | 400 | Domestic | 2.477 | 0.004 |
| 868 | 50 | 6 | Moderate | 2 | 400 | Domestic | 2.477 | 0.004 |
| 869 | 50 | 6 | Moderate | 1 | 600 | Domestic | 2.475 | 0.004 |
| 870 | 50 | 6 | Moderate | 1 | 800 | Domestic | 2.473 | 0.004 |
| 871 | 50 | 6 | Moderate | 2 | 800 | Domestic | 2.473 | 0.004 |
| 872 | 50 | 6 | Moderate | 3 | 800 | Domestic | 2.473 | 0.004 |
| 873 | 50 | 6 | Moderate | 1 | 1000 | Domestic | 2.471 | 0.004 |
| 874 | 70 | 6 | Severe | 2 | 0 | Domestic | 2.426 | 0.004 |
| 875 | 70 | 6 | Severe | 2 | 200 | Domestic | 2.424 | 0.004 |
| 876 | 70 | 6 | Severe | 2 | 800 | Domestic | 2.418 | 0.004 |
| 877 | 70 | 6 | Severe | 3 | 800 | Domestic | 2.418 | 0.004 |
| 878 | 70 | 6 | Severe | 1 | 1000 | Domestic | 2.416 | 0.004 |
| 879 | 50 | 18 | Moderate | 2 | 0 | Imported | 2.378 | 0.004 |
| 880 | 50 | 18 | Moderate | 1 | 200 | Imported | 2.376 | 0.004 |
| 881 | 50 | 18 | Moderate | 2 | 200 | Imported | 2.376 | 0.004 |
| 882 | 50 | 18 | Moderate | 3 | 200 | Imported | 2.376 | 0.004 |
| 883 | 50 | 18 | Moderate | 1 | 600 | Imported | 2.372 | 0.004 |
| 884 | 50 | 18 | Moderate | 2 | 600 | Imported | 2.372 | 0.004 |
| 885 | 50 | 18 | Moderate | 3 | 600 | Imported | 2.372 | 0.004 |
| 886 | 50 | 18 | Moderate | 1 | 800 | Imported | 2.37 | 0.004 |
| 887 | 50 | 18 | Moderate | 2 | 800 | Imported | 2.37 | 0.004 |
| 888 | 50 | 18 | Moderate | 1 | 1000 | Imported | 2.368 | 0.004 |
| 889 | 50 | 6 | No | 3 | 0 | Imported | 2.23 | 0.003 |
| 890 | 50 | 6 | No | 1 | 200 | Imported | 2.228 | 0.003 |
| 891 | 50 | 6 | No | 2 | 200 | Imported | 2.228 | 0.003 |
| 892 | 50 | 6 | No | 3 | 200 | Imported | 2.228 | 0.003 |
| 893 | 50 | 6 | No | 1 | 400 | Imported | 2.226 | 0.003 |
| 894 | 50 | 6 | No | 2 | 600 | Imported | 2.224 | 0.003 |
| 895 | 50 | 6 | No | 3 | 600 | Imported | 2.224 | 0.003 |
| 896 | 50 | 6 | No | 2 | 800 | Imported | 2.222 | 0.003 |
| 897 | 50 | 6 | No | 3 | 800 | Imported | 2.222 | 0.003 |
| 898 | 50 | 6 | No | 2 | 1000 | Imported | 2.22 | 0.003 |
| 899 | 50 | 18 | Moderate | 1 | 400 | Domestic | 2.196 | 0.003 |
| 900 | 50 | 18 | Moderate | 2 | 400 | Domestic | 2.196 | 0.003 |
| 901 | 50 | 6 | Severe | 1 | 0 | Imported | 2.188 | 0.003 |
| 902 | 50 | 6 | Severe | 3 | 0 | Imported | 2.188 | 0.003 |
| 903 | 50 | 6 | Severe | 2 | 400 | Imported | 2.184 | 0.003 |
| 904 | 50 | 6 | Severe | 2 | 600 | Imported | 2.182 | 0.003 |
| 905 | 50 | 6 | Severe | 1 | 800 | Imported | 2.18 | 0.003 |
| 906 | 50 | 12 | Moderate | 2 | 0 | Imported | 2.15 | 0.003 |
| 907 | 50 | 12 | Moderate | 2 | 200 | Imported | 2.148 | 0.003 |
| 908 | 50 | 12 | Moderate | 2 | 600 | Imported | 2.144 | 0.003 |
| 909 | 50 | 12 | Moderate | 3 | 600 | Imported | 2.144 | 0.003 |
| 910 | 50 | 12 | Moderate | 2 | 800 | Imported | 2.142 | 0.003 |
| 911 | 50 | 12 | Moderate | 1 | 1000 | Imported | 2.14 | 0.003 |
| 912 | 50 | 12 | Moderate | 3 | 1000 | Imported | 2.14 | 0.003 |
| 913 | 50 | 6 | No | 2 | 400 | Domestic | 2.048 | 0.003 |
| 914 | 50 | 6 | No | 3 | 400 | Domestic | 2.048 | 0.003 |
| 915 | 50 | 6 | No | 1 | 600 | Domestic | 2.046 | 0.003 |
| 916 | 50 | 6 | No | 1 | 800 | Domestic | 2.044 | 0.003 |
| 917 | 50 | 6 | No | 1 | 1000 | Domestic | 2.042 | 0.003 |
| 918 | 50 | 6 | Severe | 1 | 400 | Domestic | 2.006 | 0.003 |
| 919 | 50 | 6 | Severe | 3 | 600 | Domestic | 2.004 | 0.003 |
| 920 | 50 | 6 | Severe | 2 | 800 | Domestic | 2.002 | 0.003 |
| 921 | 50 | 6 | Severe | 1 | 1000 | Domestic | 2 | 0.003 |
| 922 | 50 | 6 | Severe | 2 | 1000 | Domestic | 2 | 0.003 |
| 923 | 50 | 6 | Severe | 3 | 1000 | Domestic | 2 | 0.003 |
| 924 | 50 | 12 | Moderate | 3 | 0 | Domestic | 1.972 | 0.003 |
| 925 | 50 | 12 | Moderate | 3 | 200 | Domestic | 1.97 | 0.002 |
| 926 | 50 | 12 | Moderate | 1 | 600 | Domestic | 1.966 | 0.002 |
| 927 | 50 | 12 | Moderate | 1 | 800 | Domestic | 1.964 | 0.002 |
| 928 | 50 | 12 | Moderate | 3 | 800 | Domestic | 1.964 | 0.002 |
| 929 | 50 | 12 | Moderate | 2 | 1000 | Domestic | 1.962 | 0.002 |
| 930 | 50 | 18 | Severe | 3 | 200 | Imported | 1.905 | 0.002 |
| 931 | 50 | 18 | Severe | 3 | 400 | Imported | 1.903 | 0.002 |
| 932 | 50 | 18 | Severe | 3 | 600 | Imported | 1.901 | 0.002 |
| 933 | 50 | 18 | Severe | 1 | 800 | Imported | 1.899 | 0.002 |
| 934 | 50 | 18 | Severe | 3 | 1000 | Imported | 1.897 | 0.002 |
| 935 | 50 | 18 | Severe | 2 | 0 | Domestic | 1.729 | 0.002 |
| 936 | 50 | 18 | Severe | 3 | 0 | Domestic | 1.729 | 0.002 |
| 937 | 50 | 18 | Severe | 2 | 200 | Domestic | 1.727 | 0.002 |
| 938 | 50 | 18 | Severe | 1 | 600 | Domestic | 1.723 | 0.002 |
| 939 | 50 | 18 | Severe | 2 | 1000 | Domestic | 1.719 | 0.002 |
| 940 | 50 | 12 | Severe | 1 | 0 | Imported | 1.679 | 0.002 |
| 941 | 50 | 12 | Severe | 2 | 0 | Imported | 1.679 | 0.002 |
| 942 | 50 | 12 | Severe | 1 | 200 | Imported | 1.677 | 0.002 |
| 943 | 50 | 12 | Severe | 1 | 400 | Imported | 1.675 | 0.002 |
| 944 | 50 | 12 | Severe | 1 | 600 | Imported | 1.673 | 0.002 |
| 945 | 50 | 12 | Severe | 2 | 600 | Imported | 1.673 | 0.002 |
| 946 | 50 | 12 | Severe | 1 | 1000 | Imported | 1.669 | 0.002 |
| 947 | 50 | 12 | Severe | 2 | 1000 | Imported | 1.669 | 0.002 |
| 948 | 50 | 6 | Moderate | 1 | 200 | Imported | 1.657 | 0.002 |
| 949 | 50 | 6 | Moderate | 1 | 600 | Imported | 1.653 | 0.002 |
| 950 | 50 | 6 | Moderate | 2 | 800 | Imported | 1.651 | 0.002 |
| 951 | 50 | 12 | Severe | 1 | 800 | Domestic | 1.493 | 0.002 |
| 952 | 50 | 12 | Severe | 3 | 1000 | Domestic | 1.491 | 0.002 |
| 953 | 50 | 6 | Moderate | 3 | 0 | Domestic | 1.481 | 0.002 |
| 954 | 50 | 6 | Moderate | 3 | 200 | Domestic | 1.479 | 0.002 |
| 955 | 50 | 6 | Moderate | 2 | 600 | Domestic | 1.475 | 0.002 |
| 956 | 50 | 6 | Moderate | 3 | 1000 | Domestic | 1.471 | 0.002 |
| 957 | 50 | 6 | Severe | 2 | 0 | Imported | 1.188 | 0.001 |
| 958 | 50 | 6 | Severe | 1 | 200 | Imported | 1.186 | 0.001 |
| 959 | 50 | 6 | Severe | 3 | 200 | Imported | 1.186 | 0.001 |
| 960 | 50 | 6 | Severe | 1 | 400 | Imported | 1.184 | 0.001 |
| 961 | 50 | 6 | Severe | 3 | 400 | Imported | 1.184 | 0.001 |
| 962 | 50 | 6 | Severe | 1 | 600 | Imported | 1.182 | 0.001 |
| 963 | 50 | 6 | Severe | 3 | 600 | Imported | 1.182 | 0.001 |
| 964 | 50 | 6 | Severe | 3 | 800 | Imported | 1.18 | 0.001 |
| 965 | 50 | 6 | Severe | 1 | 1000 | Imported | 1.178 | 0.001 |
| 966 | 50 | 6 | Severe | 2 | 1000 | Imported | 1.178 | 0.001 |
| 967 | 50 | 6 | Severe | 3 | 1000 | Imported | 1.178 | 0.001 |
| 968 | 50 | 6 | Severe | 1 | 0 | Domestic | 1.01 | 0.001 |
| 969 | 50 | 6 | Severe | 3 | 0 | Domestic | 1.01 | 0.001 |
| 970 | 50 | 6 | Severe | 2 | 200 | Domestic | 1.008 | 0.001 |
| 971 | 50 | 6 | Severe | 2 | 400 | Domestic | 1.006 | 0.001 |
| 972 | 50 | 6 | Severe | 2 | 600 | Domestic | 1.004 | 0.001 |
4. DISCUSSION
This study reports the results of a DCE study quantifying the general public's stated preference for the COVID‐19 vaccination programme. To our knowledge, this is the first study to investigate the public's preference for selecting such vaccination programmes in China and worldwide. Results of the DCE study showed that the respondents’ vaccination probability increased with an increase in the vaccine's effectiveness and protective duration as well as with a decrease in the severity of adverse events and price. The MXL estimates further suggest the existence of preference heterogeneity in five out of six attributes.
We contribute to the existing literature by finding that the Chinese population showed higher preference for an imported rather than a domestically manufactured COVID‐19 vaccine product. This is not a surprising result, as some previous studies have indicated the Chinese people's high preference for imported vaccine. 35 , 36 In the past few years, China has had several vaccine‐related scandals that severely diminished the general public's trust in the quality and effectiveness of domestically manufactured health products. 22 , 37 Moreover, several public health scandals have recently raised concerns about the government's protectionist policy against foreign imports of vaccines. Confidence in domestic medical product manufacturers and distributors reached a new low in 2018 after a major manufacturer was found to be selling faulty rabies and 'diphtheria, tetanus and pertussis' shots, which were supposed to save lives and protect infants. 38 Our findings confirmed that despite some Chinese pharmaceutical companies now taking a leading position in the race to develop the COVID‐19 vaccine, the long‐term vaccine crisis has had a significantly negative influence on the public's willingness to select a domestic vaccine. This is in line with the findings of previous studies that anxiety about vaccine safety reduces and even eliminates public's willingness towards taking vaccination. 24 , 39 , 40 However, we found that there appeared to be trade‐offs between attributes that participants considered to maximize the vaccines’ utility. For example, when the other conditions were unchanged, a domestic vaccine that was priced lower could result in a higher probability to be selected than an imported vaccine.
The public's WTP for a COVID‐19 vaccine is rarely reported; only a recent study indicated that the Chilean public's WTP for a COVID‐19 vaccine is nearly 184 USD. 11 In our study, both the main effect model and subgroup analyses confirmed that price has a limited influence on the public's preference for selecting a vaccine, and the highest price contributed only little to the decrease in the individuals’ overall utility. Although the leaders of several countries have already promised that the future COVID‐19 vaccines will be provided as 'public goods' and that their development will be paid for with taxes, we still include the price parameter in our DCE study. This is because, first, the way to translate these political statements into a concrete plan to provide a vaccine without charge to the public is yet to be determined. Moreover, governments of some countries, such as the United States, have confirmed that the COVID‐19 vaccine would have an actual price tag, which would limit its availability for many Americans. 41 The second reason is related to the development of the coronavirus. A new study has confirmed that mutations can make the SARS‐CoV‐2 virus more infectious. 42 If this is true, development of the COVID‐19 vaccine would not be a one‐off effort, but a long‐term process. The cost of providing a free COVID‐19 vaccine to the public season by season would then be a significant financial burden and an impossible mission for some developing countries. Therefore, our WTP estimations provide useful information for policymakers to develop a reasonable pricing strategy to commoditize the COVID‐19 vaccine in the market. In addition, we should not neglect the effect of 'free‐riding' behaviours, which were reported by previous studies about vaccination decisions. 16 , 43 , 44 Price is likely to only have a slight influence on individuals’ vaccination preference, not because they do not care about the cost of vaccination but because they would not get vaccinated and hope to be covered by herd immunity. Herd immunity is developed when other people take the vaccine and create a sufficiently high coverage to protect everyone. Further, the price of vaccination in our study was limited to five levels, and the public's decisions on the choices might be affected by this predefined price range. However, at the time of conducting the study, no COVID‐19 vaccine was available in the market. The price range was informed by (1) the prices of the other vaccines, such as influenza and pneumonia, that are available in China, and (2) suggestions from experts who had knowledge and experience in vaccine pricing and procurement. Yet, the effect of different price range on the public's preference over vaccines should be further investigated in follow‐up studies.
The subgroup analysis further demonstrated that the female respondents were more likely to select a COVID‐19 vaccine with higher effectiveness, longer protective duration, fewer adverse events and fewer injections than the male respondents. However, the females’ preference for vaccination seemed to be more sensitive to increased price. Although previous studies indicated that females are more likely to take up other vaccines than males, 45 , 46 none discussed the effect of price on the decision making between males and females. Some possible explanations for this might be differences in the SES and health status, and provider bias.
This study showed that urban residents preferred a vaccine with higher effectiveness, whereas rural residents preferred longer protective duration. Although several previous studies have reported low vaccination coverage in rural populations, 47 , 48 , 49 none compared the individual vaccination preferences between the rural and the urban areas. The distribution of high‐quality health‐care resources is highly uneven in China. 50 Regarding the COVID‐19 vaccine, urban residents in this study preferred a product with higher efficiency, indicating that they are able and confident about affording another shot when the protective duration expires. However, for rural residents, health‐care systems often struggle to meet their needs. 51 Compared with urban residents, the limited selection for rural residents makes them prefer a vaccine without very high efficiency but with a longer protective duration to reduce the frequency of visits and costs. Our findings indicate that although urban and rural people's preference to uptake a vaccine is similar to some extent, as previous studies have revealed, the main determinant of the vaccination choice remains different since high‐quality health‐care resources are perceived to be more difficult to approach in rural areas. 46 , 52 , 53
Methodologically, in this study, we chose to use DCE over another stated preference method—contingent valuation (CV)—for three reasons. First, DCE provides more information than CV and allows the estimation of the marginal WTP for different levels and attributes. 54 Second, unlike CV which directly elicits the monetary value of a product, DCE mitigates certain ethical concerns in survey research. 55 Third, compared with CV, DCE provides better opportunities for researchers to identify people's trade‐offs between different attributes of a product. 56 However, it is worth noting that DCE usually generates a higher cognitive burden than CV, especially when the design of a DCE is complicated or the sample size is a relatively small one.
5. LIMITATIONS OF THE STUDY
Several limitations of our research must be addressed. First, our data were collected from an online survey, which means that people who did not have access to the Internet were excluded from the survey, which is likely to lead to a selection bias. Second, compared with the Chinese general population, our sample is much younger, better educated and has a higher income. Nearly 80% of them reported having an average monthly income greater than the national median. Methodologically, an inherent characteristic of DCE is that respondents have to make a choice between two hypothetical profiles. However, in the real world, they might be presented with more options. Hence, the generalizability of our findings is limited. Third, the low utility of adverse events in our study might be resulted from setting up the range of adverse events at relatively milder levels in the first place. Furthermore, although explanations on the attributes and levels of the profiles were provided in the survey, some participants might not read them carefully or even misunderstood the profiles. Therefore, the validity of our findings is not without concern. Finally, a more heterogeneous approach is needed in future studies by including different stated preference methods such as CV, or statistical techniques such as hierarchical Bayes.
6. CONCLUSIONS
This study found that 80% of the Chinese public who participated in the survey preferred to receive the COVID‐19 vaccination when it is available. More than 40% of them indicated that the elderly should be prioritized for the vaccination programme. When the participants were facing trade‐offs between two COVID‐19 vaccination programmes, effectiveness was regarded as the most important attribute, followed by long protective duration, very few adverse events and being manufactured overseas. Interestingly, price was the least important attribute affecting the public preference in selecting the COVID‐19 vaccine.
However, such findings need to be interpreted with caution. The distribution of income levels among our sample was skewed towards the higher end of national average. The public with lower incomes who will be more sensitive to prices was in fact unrepresented. Moreover, since the SARS‐CoV‐2 is still mutating, it is hard to predict the effectiveness of the vaccines that are currently under development, and thus, the final prices of these vaccines are largely unknown. Therefore, we suggest that price should not be considered as less important when the industry and the government design and implement marketing and policy strategies related to the COVID‐19 vaccines. It is also worth noting that different population subgroups had heterogeneous or varied preferences on the vaccine, which further reminds us of the importance of taking individuals’ or a certain social group's needs into consideration for any vaccination programme. Follow‐up studies from other countries are needed to investigate how the public's acceptance and preference for COVID‐19 vaccination change over time as the pandemic progresses. Not only does the development of vaccines against COVID‐19 has to be a global effort, building trust in and promoting equity access to the COVID‐19 vaccines also require co‐operation at the global level.
CONFLICT OF INTEREST
All the authors declare no conflict of interest.
AUTHOR CONTRIBUTIONS
DD, RHX, DF and SW conceptualized and designed the research protocol of the study. EW, CH, EY and FZC commented on the research design and helped revise the design. DD and RHX implemented data collection and interpretation. DD and RHX wrote the first draft of the manuscript. CH ad SW revised the first draft. All authors were involved in revising the article in the third round and approved the final manuscript.
ETHICAL APPROVAL
The study was approved by the Survey and Behavioural Research Ethics Committee of the Chinese University of Hong Kong. The ethics approval code is SBRE‐19‐690.
7. APPENDIX
7.1.
ACKNOWLEDGEMENTS
The authors would like to thank participants for interviews and focus groups for sharing their perceptions of and experience with vaccines.
Dong D, Xu RH, Wong EL, et al. Public preference for COVID‐19 vaccines in China: A discrete choice experiment. Health Expect. 2020;23:1543–1578. 10.1111/hex.13140
Dong Dong and Richard Huan Xu contributed equally to this article.
Eng‐kiong Yeoh and Samuel Yeung‐shan Wong co‐senior authorship.
Funding information
This research was funded by the Centre for Health Systems and Policy Research of the Chinese University of Hong Kong. The Centre was supported by the Tung Foundation (Project code: 6905422).
Contributor Information
Dong Dong, Email: dongdong@cuhk.edu.hk.
Richard Huan Xu, Email: richardhxu@cuhk.edu.hk.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
REFERENCES
- 1. Coronavirus disease (COVID‐19) – World Health Organization . https://www.who.int/emergencies/diseases/novel-coronavirus-2019?gclid=Cj0KCQjwp4j6BRCRARIsAGq4yMHitmMOYXc6GhGAdMENT3d7oGWDHCwICe3BXTQlLcLGBXcnIi8hj2IaAi6pEALw_wcB. Updated August 23, 2020. Accessed August 24, 2020.
- 2. Cheung E.What does Hong Kong’s ‘third wave’ of Covid‐19 infections mean for life in the city, and what is being done. South China Morning Post July 10, 2020. https://www.scmp.com/news/hong-kong/health-environment/article/3092542/what-does-hong-kongs-third-wave-covid-19. Accessed August 23, 2020.
- 3. Wu Y, Yan X, Dong D, Chung RY, Yeoh E. Equitable exit strategy is required: lessons learnt from Hong Kong’s current resurgence of local outbreaks among individuals from highly deprived neighbourhoods. Journal of Epidemiology and Community Health. 2020;jech–2020. 10.1136/jech-2020-215347 [DOI] [PubMed] [Google Scholar]
- 4. Flaxman S, Mishra S, Gandy A, et al. Report 13: Estimating the Number of Infections and the Impact of Non‐pharmaceutical Interventions on COVID‐19 in 11 European Countries. Ferguson NM, Laydon D, Nedjati‐Gilani G, et al. eds. 2020. 10.25561/77482 [DOI] [Google Scholar]
- 5. European Centre for Disease Prevention and Control . Resurgence of Reported Cases of COVID‐19 in the EU/EEA, the UK and EU Candidate and Potential Candidates. Stockholm; 2 July/2020. [Google Scholar]
- 6. Lurie N, Saville M, Hatchett R, Halton J. Developing Covid‐19 vaccines at pandemic speed. N Engl J Med. 2020;382(21):1969‐1973. 10.1056/NEJMp2005630 [DOI] [PubMed] [Google Scholar]
- 7. Folegatti PM, Ewer KJ, Aley PK, et al. Safety and immunogenicity of the ChAdOx1 nCoV‐19 vaccine against SARS‐CoV‐2: a preliminary report of a phase ½, single‐blind, randomised controlled trial. Lancet. 2020. 10.1016/S0140-6736(20)31604-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. de Bekker‐Grob EW, Veldwijk J, Jonker M, et al. The impact of vaccination and patient characteristics on influenza vaccination uptake of elderly people: a discrete choice experiment. Vaccine. 2018;36(11):1467‐1476. 10.1016/j.vaccine.2018.01.054 [DOI] [PubMed] [Google Scholar]
- 9. Nagata JM, Hernández‐Ramos I, Kurup AS, Albrecht D, Vivas‐Torrealba C, Franco‐Paredes C. Social determinants of health and seasonal influenza vaccination in adults ≥65 years: a systematic review of qualitative and quantitative data. BMC Public Health. 2013;13(1): 10.1186/1471-2458-13-388 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Eilers R, Krabbe PFM, de Melker HE. Factors affecting the uptake of vaccination by the elderly in Western society. Prev Med. 2014;69:224‐234. 10.1016/j.ypmed.2014.10.017 [DOI] [PubMed] [Google Scholar]
- 11. García LY, Cerda AA. Contingent assessment of the COVID‐19 vaccine. Vaccine. 2020;38(34):5424‐5429. 10.1016/j.vaccine.2020.06.068 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. McGregor G.China’s military approves coronavirus vaccine for its own use. Fortune June 29, 2020. https://fortune.com/2020/06/29/china-coronavirus-vaccine-military/. Accessed August 24, 2020.
- 13. Ryan M, Gerard K. Using Discrete Choice Experiments to Value Health and Health Care. Dordrecht: Springer; 2007. The Economics of Non‐Market Goods and Resources; vol. 11. [Google Scholar]
- 14. Norman R, Moorin R, Maxwell S, Robinson S, Brims F. Public attitudes on lung cancer screening and radiation risk: a best‐worst experiment. Value Health. 2020;23(4):495‐505. 10.1016/j.jval.2019.11.006 [DOI] [PubMed] [Google Scholar]
- 15. Reed Johnson F, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete‐choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3‐13. 10.1016/j.jval.2012.08.2223 [DOI] [PubMed] [Google Scholar]
- 16. Liao Q, Ng TWY, Cowling BJ. What influenza vaccination programmes are preferred by healthcare personnel? A discrete choice experiment. Vaccine. 2020;38(29):4557‐4563. 10.1016/j.vaccine.2020.05.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Kudo R, Yamaguchi M, Sekine M, et al. Bivalent human papillomavirus vaccine effectiveness in a japanese population: high vaccine‐type‐specific effectiveness and evidence of cross‐protection. J Infect Dis. 2019;219(3):382‐390. 10.1093/infdis/jiy516 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Jackson ML, Chung JR, Jackson LA, et al. Influenza vaccine effectiveness in the United States during the 2015–2016 season. N Engl J Med. 2017;377(6):534‐543. 10.1056/NEJMoa1700153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Butler AM, Layton JB, Krueger WS, Kshirsagar AV, McGrath LJ. Assessing residual bias in estimating influenza vaccine effectiveness: comparison of high‐dose versus standard‐dose vaccines. Med Care. 2019;57(1):73‐78. 10.1097/MLR.0000000000001018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Zimmerman RK, Nowalk MP, Chung J, et al. 2014–2015 influenza vaccine effectiveness in the united states by vaccine type. Clin Infect Dis. 2016;63(12):1564‐1573. 10.1093/cid/ciw635 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Ultsch B, Damm O, Beutels P, et al. Methods for health economic evaluation of vaccines and immunization decision frameworks: a consensus framework from a European vaccine economics community. Pharmacoeconomics. 2016;34(3):227‐244. 10.1007/s40273-015-0335-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Zhou M, Qu S, Zhao L, Kong N, Campy KS, Wang S. Trust collapse caused by the Changsheng vaccine crisis in China. Vaccine. 2019;37(26):3419‐3425. 10.1016/j.vaccine.2019.05.020 [DOI] [PubMed] [Google Scholar]
- 23. Shono A, Kondo M. Parents’ preferences for seasonal influenza vaccine for their children in Japan. Vaccine. 2014;32(39):5071‐5076. 10.1016/j.vaccine.2014.07.002 [DOI] [PubMed] [Google Scholar]
- 24. Fung IC‐H, Cheung C‐N, Fu K‐W, Ip P, Tse ZTH. Vaccine safety and social media in China. Am J Infect Control. 2016;44(10):1194‐1195. 10.1016/j.ajic.2016.04.248 [DOI] [PubMed] [Google Scholar]
- 25. Anywaine Z, Whitworth H, Kaleebu P, et al. Safety and immunogenicity of a 2‐dose heterologous vaccination regimen with Ad26.ZEBOV and MVA‐BN‐Filo Ebola vaccines: 12‐month data from a phase 1 randomized clinical trial in Uganda and Tanzania. J Infect Dis. 2019;220(1):46‐56. 10.1093/infdis/jiz070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Guo N, Zhang G, Zhu D, Wang J, Shi L. The effects of convenience and quality on the demand for vaccination: results from a discrete choice experiment. Vaccine. 2017;35(21):2848‐2854. 10.1016/j.vaccine.2017.04.006 [DOI] [PubMed] [Google Scholar]
- 27. Connell J, Carlton J, Grundy A, et al. The importance of content and face validity in instrument development: lessons learnt from service users when developing the Recovering Quality of Life measure (ReQoL). Qual Life Res. 2018;27(7):1893‐1902. 10.1007/s11136-018-1847-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Johnson FR, Yang J‐C, Reed SD. The internal validity of discrete choice experiment data: a testing tool for quantitative assessments. Value in Health. 2019;22(2):157‐160. 10.1016/j.jval.2018.07.876 [DOI] [PubMed] [Google Scholar]
- 29. Kroenke K, Spitzer RL, Williams JBW. The patient health questionnaire‐2. Med Care. 2003;41(11):1284‐1292. 10.1097/01.MLR.0000093487.78664.3C [DOI] [PubMed] [Google Scholar]
- 30. Joinson AN, Ed. The Oxford Handbook of Internet Psychology. Oxford, New York: Oxford University Press; 2007. Oxford handbooks. [Google Scholar]
- 31. Callegaro M, Baker RP, Bethlehem J, Göritz AS, Krosnick JA, Lavrakas PJ, eds. Wiley series in survey methodology Online Panel Research: A Data Quality Perspective (pp. 1–2). Hoboken: Wiley; 2014. [Google Scholar]
- 32. Determann D, Lambooij MS, Steyerberg EW, de Bekker‐Grob EW, de Wit GA. Impact of survey administration mode on the results of a health‐related discrete choice experiment: online and paper comparison. Value Health. 2017;20(7):953‐960. 10.1016/j.jval.2017.02.007 [DOI] [PubMed] [Google Scholar]
- 33. Liu S, Li S, Yang R, Liu T, Chen G. Job preferences for medical students in China. Medicine. 2018;97(38):e12358 10.1097/MD.0000000000012358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Green C, Gerard K. Exploring the social value of health‐care interventions: a stated preference discrete choice experiment. Health Econ. 2009;18(8):951‐976. 10.1002/hec.1414 [DOI] [PubMed] [Google Scholar]
- 35. Li R, Xie R, Yang C, Rainey J, Song Y, Greene C. Identifying ways to increase seasonal influenza vaccine uptake among pregnant women in China: A qualitative investigation of pregnant women and their obstetricians. Vaccine. 2018;36(23):3315‐3322. 10.1016/j.vaccine.2018.04.060 [DOI] [PubMed] [Google Scholar]
- 36. Huang Z, Sun X, Wagner AL, et al. Parent and caregiver perceptions about the safety and effectiveness of foreign and domestic vaccines in Shanghai, China. PLoS One. 2018;13(5):e0197437 10.1371/journal.pone.0197437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Sun J, Hu CJ, Stuntz M, Hogerzeil H, Liu Y. A review of promoting access to medicines in China – problems and recommendations. BMC Health Serv Res. 2018;18(1): 10.1186/s12913-018-2875-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Murphy F. China vaccine scandal: investigations begin into faulty rabies and DTaP shots. BMJ. 2018;362:k3244 10.1136/bmj.k3244 [DOI] [PubMed] [Google Scholar]
- 39. Gold MS, MacDonald NE, McMurtry CM, et al. Immunization stress‐related response – redefining immunization anxiety‐related reaction as an adverse event following immunization. Vaccine. 2020;38(14):3015‐3020. 10.1016/j.vaccine.2020.02.046 [DOI] [PubMed] [Google Scholar]
- 40. Loharikar A, Suragh TA, MacDonald NE, et al. Anxiety‐related adverse events following immunization (AEFI): a systematic review of published clusters of illness. Vaccine. 2018;36(2):299‐305. 10.1016/j.vaccine.2017.11.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Rosenthal E.Opinion | How a Covid‐19 vaccine could cost Americans dearly. The New York Times July 6, 2020. https://www.nytimes.com/2020/07/06/opinion/coronavirus-vaccine-cost.html. Accessed August 23, 2020.
- 42. Korber B, Fischer WM, Gnanakaran S, et al. Tracking changes in SARS‐CoV‐2 Spike: evidence that D614G increases infectivity of the COVID‐19 virus. Cell. 2020;182(4):812‐827.e19. 10.1016/j.cell.2020.06.043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Kabir KA, Tanimoto J. Evolutionary vaccination game approach in metapopulation migration model with information spreading on different graphs. Chaos, Solitons Fractals. 2019;120:41‐55. 10.1016/j.chaos.2019.01.013 [DOI] [Google Scholar]
- 44. Liao Q, Lam WWT, Wong CKH, Lam C, Chen J, Fielding R. The relative effects of determinants on Chinese adults’ decision for influenza vaccination choice: What is the effect of priming? Vaccine. 2019;37(30):4124‐4132. 10.1016/j.vaccine.2019.05.072 [DOI] [PubMed] [Google Scholar]
- 45. Galarce EM, Minsky S, Viswanath K. Socioeconomic status, demographics, beliefs and A(H1N1) vaccine uptake in the United States. Vaccine. 2011;29(32):5284‐5289. 10.1016/j.vaccine.2011.05.014 [DOI] [PubMed] [Google Scholar]
- 46. Jiménez‐García R, Hernández‐Barrera V, de Andres AL, Jimenez‐Trujillo I, Esteban‐Hernández J, Carrasco‐Garrido P. Gender influence in influenza vaccine uptake in Spain: time trends analysis (1995–2006). Vaccine. 2010;28(38):6169‐6175. 10.1016/j.vaccine.2010.07.029 [DOI] [PubMed] [Google Scholar]
- 47. Zhang X, Syeda ZI, Jing Z, et al. Rural‐urban disparity in category II vaccination among children under five years of age: evidence from a survey in Shandong, China. Int J Equity Health. 2018;17(1): 10.1186/s12939-018-0802-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Hu Y, Wang Y, Chen Y, Liang H. Analyzing the urban‐rural vaccination coverage disparity through a fair decomposition in Zhejiang Province, China. IJERPH. 2019;16(22):4575 10.3390/ijerph16224575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Wang Y, Cheng M, Wang S, et al. Vaccination coverage with the pneumococcal and influenza vaccine among persons with chronic diseases in Shanghai, China, 2017. BMC Public Health. 2020;20(1): 10.1186/s12889-020-8388-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Yu M, He S, Wu D, Zhu H, Webster C. Examining the multi‐scalar unevenness of high‐quality healthcare resources distribution in China. IJERPH. 2019;16(16). 10.3390/ijerph1616281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Wu J, Li X, Song Y, et al. The impact of a bundled policy intervention on improving the performance of rural healthcare in China. Int J Equity Health. 2016;15(1): 10.1186/s12939-016-0334-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Barnett S. Interrelations between three proxies of health care need at the small area level: an urban/rural comparison. J Epidemiol Community Health. 2002;56(10):754‐761. 10.1136/jech.56.10.754 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Pohar SL, Majumdar SR, Johnson JA. Health care costs and mortality for canadian urban and rural patients with diabetes: population‐based trends from 1993–2001. Clin Ther. 2007;29(6):1316‐1324. 10.1016/j.clinthera.2007.07.001 [DOI] [PubMed] [Google Scholar]
- 54. Hoyos D. The state of the art of environmental valuation with discrete choice experiments. Ecol Econ. 2010;69(8):1595‐1603. 10.1016/j.ecolecon.2010.04.011 [DOI] [Google Scholar]
- 55. Hanley N, Mourato S, Wright RE. Choice modelling approaches: a superior alternative for environmental valuation? J Econ Surv. 2001;15(3):435‐462. 10.1111/1467-6419.00145 [DOI] [Google Scholar]
- 56. Mahieu P‐A, Andersson H, Beaumais O, Crastes R, Wolff F‐C. Is Choice Experiment Becoming more Popular than Contingent Valuation? A Systematic Review in Agriculture, Environment and Health. Unpublished. 2015. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding authors upon reasonable request.