

Abstract
While subfalcine, transtentorial, and transmagnal herniation are most often thought of as downward phenomena, brain herniation can also occur in the upward direction with similarly disastrous clinical consequences.
Keywords: brain injury, brainstem, transtentorial herniation, upward herniation
While subfalcine, transtentorial, and transmagnal herniation are most often thought of as downward phenomena, brain herniation can also occur in the upward direction with similarly disastrous clinical consequences.
1. CLINICAL IMAGE
Herein, the case of a coagulopathic patient with a spontaneous posterior fossa subdural hematoma resulting in fatal upward transtentorial herniation and brainstem compression is described.
A 47‐year‐old woman critically ill and coagulopathic immediately post‐liver transplant developed isolated bilateral cranial nerve VI palsies. Magnetic resonance imaging (MRI) of the brain revealed a small noncompressive subdural hematoma in the premedullary space (Figure 1A). The patient remained mechanically ventilated and sedated due to systemic illness. Four days later, she was noted to have lost all brainstem reflexes, and a repeat MRI demonstrated a large spontaneous posterior fossa subdural hematoma with ventral displacement and compression of the lower brainstem and significant upward transtentorial herniation of the cerebellum and rostral brainstem structures (Figure 1B). This was unfortunately a nonsurvivable neurological injury from which the patient ultimately expired. Although rarer than its downward transtentorial herniation counterpart, upward herniation can occur in the setting of posterior fossa pathology, either acutely or chronically, and can prove just as lethal via compression/shearing of neurovascular structures against the tentorium, with concurrent brainstem compression against the clivus and obstructive hydrocephalus. While it can occur spontaneously as demonstrated in this case, upward herniation is more commonly recognized clinically as an iatrogenic phenomenon, precipitated by the transtentorial pressure gradient created by supratentorial cerebrospinal fluid diversion in the setting of intra‐ or extra‐axial posterior fossa pathology. 1 , 2
Figure 1.
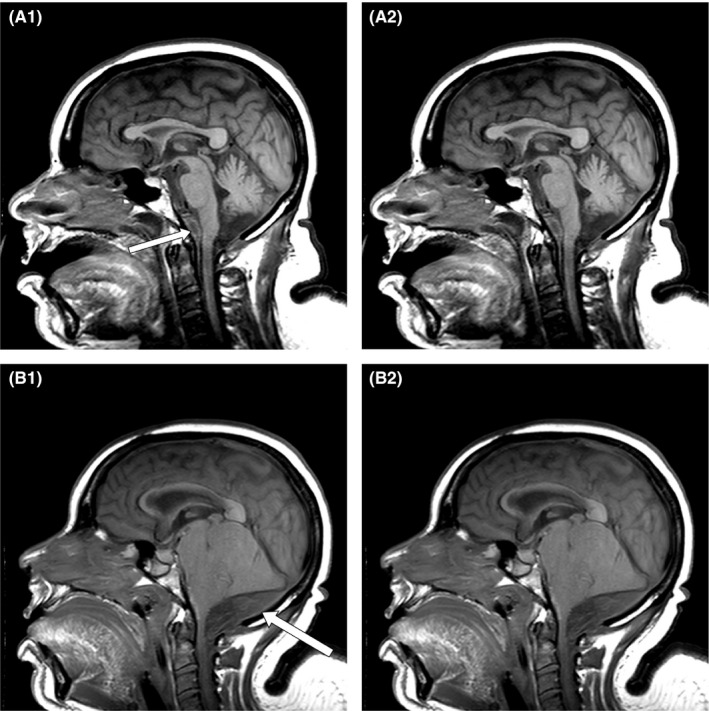
A. Initial MRI demonstrating a small subdural blood collection anterior to the medulla oblongata. B. Follow‐up MRI demonstrating a large subdural hematoma caudal to the cerebellum with resultant ascending herniation of neural structures through the tentorial incisura
CONFLICT OF INTEREST
None declared.
AUTHOR CONTRIBUTIONS
NBO: involved in case review and manuscript preparation. WSF III: involved in project oversight, review, and editing of the manuscript.
ETHICAL APPROVAL
Per the University of Alabama at Birmingham Institutional Review Board policy, single‐patient case reports that are devoid of the 18 HIPAA identifiers and imaging studies that have been thoroughly de‐identified do not require patient consent. The information contained within this report is in compliance with recognized standards.
ACKNOWLEDGMENTS
Published with written consent of the patient.
Omar NB, Fisher WS III. Upward transtentorial herniation. Clin Case Rep. 2020;8:3573–3574. 10.1002/ccr3.3237
REFERENCES
- 1. Munakomi S, Das JM. Brain Herniation In: StatPearls. Treasure Island, FL: StatPearls Publishing Copyright© 2020, StatPearls Publishing LLC; 2020. https://www.ncbi.nlm.nih.gov/books/NBK542246/ [Google Scholar]
- 2. Yadav G, Sisodia R, Khuba S, Mishra L. Anesthetic management of a case of transtentorial upward herniation: An uncommon emergency situation. J Anaesthesiol Clin Pharmacol. 2012;28(3):413‐415. [DOI] [PMC free article] [PubMed] [Google Scholar]