

Abstract
Device‐related pressure injury (DRPI) is a serious problem that is affecting professionals working on the front lines against COVID‐19 due to the prolonged use of personal protective equipment (PPE). In addition to the physical and psychological integrity of professionals, these injuries can compromise the quality of care. Therefore, using technologies to prevent this adverse effect is an urgent matter. This is a parallel two‐arm randomized clinical trial without the use of a control group to compare the use of foam and extra‐thin hydrocolloid in preventing DRPI associated with the use of PPE by health professionals working on the front lines against coronavirus. In total, 88 professionals were divided into two groups: foam and hydrocolloid. Data were collected using two instruments and related to demographic and professional characteristics and skin evaluation. Each volunteer received one of the dressings, both with the same dimensions and arranged over similar regions, and data were gathered at baseline and after 6 or 12 hours. Descriptive and inferential analytic statistical methods were used; the significance level adopted was 5%. No participant developed DRPI, but four areas with hyperemia were observed in the foam group (two in the forehead, one in the cheeks, and one in the nose bridge), as well as four areas with hyperemia in the hydrocolloid group (two in the nose bridge, one in the right ear, and one in the left ear). There was no difference between the groups regarding skin conditions and discomfort (P > .05). The average cost obtained was $ 5.8/person and $ 4.4/person in the foam group and the hydrocolloid group, respectively, considering the dressing measurements. The results show that foam and extra‐thin hydrocolloid were effective in preventing DRPI associated with the use of PPE.
1. INTRODUCTION
The disease caused by the new coronavirus, COVID‐19, is a respiratory tract infection that led the World Health Organization to declare a pandemic on March 11, 2020. 1
Human transmission occurs through droplets of saliva, contact, and air. The recommendation to reduce transmission is effective isolation of the population, meaning that COVID‐19 causes not only a disruption in the health system but also a socioeconomic one given the necessary measures needed to control dissemination. 1
Due to its transmission route, 2 high rate of transmissibility, morbidity, and mortality, 3 the availability and correct use of personal protective equipment (PPE) are essential in maintaining the safety of health professionals. 1 However, due to the prolonged use of PPE, frontline professionals in the fight against COVID are at a high risk of developing a Device‐related pressure injury (DRPI). 4 , 5 , 6
Medical devices can cause humidity, heat, and pressure between the device and skin, leading to pressure‐related injuries from medical devices. 7 According to the National Pressure Injury Advisory Panel (NPIAP), DRPI is defined as a pressure injury caused by a device applied for therapeutic and diagnostic reasons. The injury may have a similar shape as the device. 8
These skin injuries can compromise the physical and psychological integrity of professionals, which compromises patient safety and the quality of care. 9 According to the literature, DRPI can be avoided with technologies that protect the exposed areas from these adverse events. 4 , 5 , 6 However, before the pandemic, most studies related to DRPI prevention were carried out with patients. 10 , 11
A three‐arm clinical trial investigated two different dressings, Tegasorb and Tegaderm, and a control group without dressings for pressure relief on the nose bridge in patients undergoing non‐invasive positive pressure ventilation. The results showed that the participants of the two groups that used dressings had a lower occurrence of pressure injury compared to the control group. However, the results were not significant. 10
Another preclinical study on the nasal occurrence of pressure injury induced by nasotracheal intubation found that a combination of Soft Liner and hydrocolloid reduced the size and severity of the injury. 12
Recently, a cross‐sectional study conducted with health professionals caring for patients with COVID‐19 investigated the types of skin injuries, anatomical sites, and preventive measures related to the use of PPE. The study included 4306 participants from 161 hospitals, with a prevalence of skin injuries of 42.8%, divided into 30.0% of DRPI, 10.8% of moisture‐associated skin damage (MASD), and 2.0% of skin tears (STs). Of the participants with DRPI, 1080 reported having two or more anatomical parts affected: 30.6% reported ulcers on the nose bridge, 28.8% on the cheeks, 25.5% on the ears, and 13.9% on the forehead. Regarding MASD, 29.4% occurred on the nose bridge, 27.3% on the cheeks, 25.0% in the ears, and 16.3% on the forehead. For ST, 74 participants reported lesions on the nose bridge and cheeks, 67 on the ears, and 51 on the forehead. 13
In evaluating the skin injuries of 1844 participants, 55.0% answered that they did not use preventive treatment and 45.0% received treatment with dressings, oil agents, or other methods. Among those who did not present skin injuries, 17.7% of the participants reported the use of prophylactic dressing for the prevention of skin injuries, including foam, hydrocolloids, oil, or cream, among others. 13
A systematic review of the use of prophylactic dressings to prevent pressure injuries suggested that their use decreased the incidence of this medical device‐associated event. However, there was no clinical evidence of which type of dressing was the most effective. 14
Given this context, DRPI prevention among professionals at the front lines of the fight against COVID is crucial, mainly to reduce the contamination risk due to the absence of cutaneous integrity and the inability to use PPE in the presence of pressure injury. However, the best dressing for preventing skin injuries remains unknown.
This study this aimed to compare the use of foam and extra‐thin hydrocolloid in the prevention of DRPI associated with the use of PPE by health professionals working on the front line against coronavirus.
2. MATERIALS AND METHODS
2.1. Study design
This is a parallel two‐arm randomized clinical trial without a control group. The following steps were carried out: consultation of the Consolidated Statement of Reporting Trials (CONSORT) for randomization, group follow‐up, blinding, and data analysis. 15 The study was registered on the Brazilian Clinical Trials platform (ReBEC), available at http://www.ensaiosclinicos.gov.br, under number RBR‐7 drpyr.
2.2. Sample
The study participants were professionals working in the Adult Intensive Care Units of a teaching hospital at the University of Campinas, Brazil. The sample size was calculated considering the objective of comparing prophylactic dressing groups (foam × hydrocolloid), according to the presence of a pressure ulcer (without ulcer, with ulcer). The calculation was made considering the methodology of a sample calculation for a Pearson's Chi‐square test. 14 In this estimate, a 5% significance level, an 80% test power, a 0.30° of freedom, and effect size were assumed, which can be considered a medium degree effect size. 16 The sample size obtained was 88 professionals (44 per group). The software PASS 13 17 was used.
The study included professionals who provided direct care (nurses, physicians, and physical therapists) or indirect care (cleaning staff) to patients with suspected or diagnosed coronavirus and needed to use PPE (face shield, gloves, caps, and particulate respirator) for six or 12 consecutive hours.
The following professionals were excluded from the sample: those who did not finish the shift, those who needed to remove the dressing due to discomfort or signs of allergy, the presence of skin damage in the region of the face, and those who did not complete the checklist received along with the dressing to prevent DRPI resulting from the use of PPE. Despite the professionals' skill and knowledge levels, all the participants received theoretical and practical training about the personal protective device before this research.
2.3. Recruitment, randomization, and allocation of participants
The selection of participants was random and considered the inclusion criteria. Eighty‐eight opaque envelopes were prepared by a team member who had no contact with the participants. The envelopes contained the dressing to be used by the professional and were then randomly distributed using the website http://www.randomization.com/. The professionals were then allocated to the respective groups.
2.4. Blinding
The statistician who performed the data analysis was blind to the denomination of the groups.
2.5. Data collection instruments
This study used an instrument for personal and professional characterizations of the sample that included the variables: age, sex, skin color, presence of comorbidities, profession, and time of experience in the profession and the unit.
The data on skin characteristics were collected using a form specifically designed for this study after reviewing the literature. This form had its face validity evaluated by three specialists, selected for convenience. The form included the following information: characteristics of the skin (intact without hyperemia, intact with hyperemia that pales with digit pressure, or pressure injury classified by I to IV stages IV3), types of PPE used (N95 masks, hats, and goggles/visors), the time of use of PPE (6 or 12 hours), and identification of the protection technology, as well as the time of installation and removal. It was completed before the installation of the technology and at the time of removal.
2.6. Intervention
For the foam group, the participants received a material based on polyurethane foam, which was placed over the forehead (15 cm × 3 cm), nose bridge and cheeks (15 cm × 3 cm), and ears (5 cm × 3 cm). In the hydrocolloid group, the participant received extra‐thin hydrocolloid plates with the same dimensions, which were installed over the same regions. The areas for installing the dressings and the cuts that were made on the plates were chosen according to recommendations from the literature. 18 , 19 The outcome was the evaluation of the presence or absence of skin injuries in the regions covered with foam or hydrocolloid.
Both groups were approached only once, and, to maintain the safety requirements established in the guidelines, 20 , 21 the following guidelines and care were reinforced when installing the dressing before entering the work environment: hand hygiene, installation of the technology in the recommended places, placing the N95 mask on the face, and performing the sealing test according to the manufacturer's recommendations.
2.7. Statistical analysis
The absolute and relative frequencies of categorical variables and measures of position and dispersion of continuous variables were calculated. The associations between groups with the variables of professional characterization and evaluation of skin characteristics were assessed using Mann Whitney and Fisher's exact test. The significance level adopted was 5%.
For analyzing the costs related to the dressings, the cost for the purchase of products and the measurement of cuts established for each participant were considered.
2.8. Ethical aspects
This study was approved by the Research Ethics Committee of the University of Campinas and followed all Brazilian and international standards for research involving human beings under number 4074115. All study participants provided written consent.
3. RESULTS
Eighty‐eight participants were recruited and eligible, of which 44 were randomized in the foam group and 44 in the extra‐thin hydrocolloid group. However, four participants were excluded from the foam group. Three were excluded because the dressing unstuck before the end of the shift, and the other participant did not complete the checklist. Thus, the study ended with 40 participants in the foam group and 44 in the hydrocolloid group, as shown in Figure 1.
FIGURE 1.
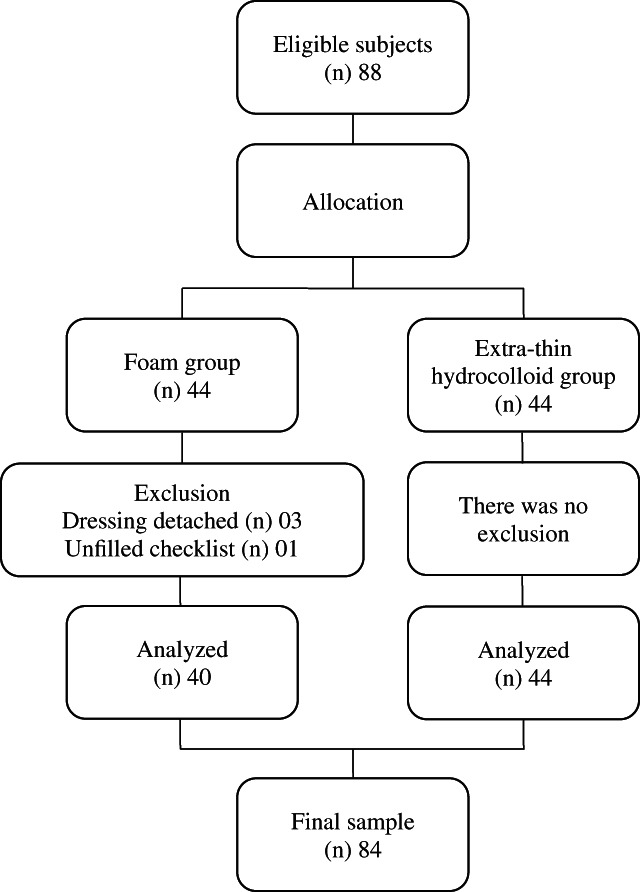
Flowchart of inclusion, allocation, and analysis of participants
The mean age of the 84 participants was 38.0 (SD = 9.0) years. Most were female (69, 82.1%) who declared themselves white (55, 65.5%) and without a chronic disease (73, 86.9%). The mean time of experience was 13.2 (SD = 7.3) years and with 5.8 ± 6.8 years working in the unit. The other variables of professional characterization of the sample are in Table 1.
TABLE 1.
Professional characterization of the sample
| Variables | n | % |
|---|---|---|
| Profession | ||
| Nursing technician | 48 | 57.1 |
| Nurse | 20 | 23.8 |
| Physical therapist | 7 | 8.3 |
| Physician | 4 | 4.8 |
| Cleaning assistant | 3 | 3.6 |
| Others | 2 | 2.4 |
| Work shift | ||
| Morning | 32 | 38.1 |
| Afternoon | 24 | 28.6 |
| Night | 28 | 33.3 |
Regarding the use of PPE, most participants (78, 92.9%) received training on the use of this equipment while providing care to patients with symptoms or diagnosis of COVID‐19. All professionals (100%) used N95 masks during their shifts, and 81 (96.4%) used a cap and face shield.
The average time using the cover in the foam group was 7.04 hours (SD = 2.57), and in the hydrocolloid group, 7.47 hours (SD = 2.98). The difference between the average time for using the covers between the groups was not significant (P = .6827). No participant developed skin injuries; however, four areas with hyperemia were observed in the foam group (two on the forehead, one on the cheeks, and one on the nose bridge) and four areas with hyperemia in the hydrocolloid group (two on the nose bridge, one on the right ear, and one on the left ear). Table 2 shows the relationship between the skin conditions of the participants at the end of the shift and the use of dressing.
TABLE 2.
Association between skin conditions and discomfort presented by the participants and the use of dressings
| Variable | Dressing | P‐value a | |||
|---|---|---|---|---|---|
| Foam | Hydrocolloid | ||||
| n | % | n | % | ||
| Forehead | .2238 | ||||
| Whole | 38 | 95.0 | 44 | 100.0 | |
| Hyperemia | 2 | 5.0 | 0 | 0 | |
| R Ear | 1.0000 | ||||
| Whole | 40 | 100.0 | 43 | 97.7 | |
| Hyperemia | 0 | 0 | 1 | 2.3 | |
| L Ear | 1.0000 | ||||
| Whole | 40 | 100.0 | 43 | 97.7 | |
| Hyperemia | 0 | 0 | 1 | 2.3 | |
| Cheeks | .4762 | ||||
| Whole | 39 | 97.5 | 44 | 100.0 | |
| Hyperemia | 1 | 2.5 | 0 | 0 | |
| Nose bridge | |||||
| Whole | 39 | 97.5 | 42 | 95.4 | 1.0000 |
| Hyperemia | 1 | 2.5 | 2 | 4.6 | |
| Discomfort | |||||
| Yes | 20 | 50.00 | 24 | 54.55 | .8271 |
| No | 20 | 50.00 | 20 | 45.45 | |
Fisher's exact test.
When asked about the discomfort related to the use of the dressings, the participants reported difficulties when removing the dressing, as well as itching, problems with the mask moving and sealing, among others (Table 3).
TABLE 3.
Discomfort reported by professionals related to the use of dressing
| Discomfort | Foam | Hydrocolloid | ||
|---|---|---|---|---|
| n | % | n | % | |
| Itching | 3 | 14.3 | 7 | 21.9 |
| Pain | 0 | 0‐ | 4 | 12.5 |
| Detachment | 14 | 66.7 | 0 | 0‐ |
| Mask issues | 3 | 14.3 | 2 | 6.3 |
| Heating | 1 | 4.8 | 0 | 0‐ |
| Uncomfortable use | 0 | 0‐ | 4 | 12.5 |
| Difficulty removing dressing | 0 | 0‐ | 10 | 31.3 |
| Stretched skin | 0 | 0‐ | 3 | 9.4 |
| Others | 0 | 0‐ | 2 | 6.3 |
| Total | 21 | 100.0 | 32 | 100.0 |
The mean cost was $5.8/person for the foam group and $4.4/person for the hydrocolloid group, based on the dressing measures used to prevent skin injuries in each studied region (nose bridge, right and left ears, cheeks, and forehead).
4. DISCUSSION
Until now, research about the use of prophylactic dressing in the prevention of skin injuries by medical devices was done in patients. 10 , 11 However, the current situation caused the development of DRPI related PPE use by health professionals to become a concern; thus, research on this topic has recently started.
This study showed that both prophylactic dressings were effective in preventing DRPI on the nose bridge, forehead, cheeks, and ears since no participant had skin injuries. Nevertheless, four occurrences of hyperemia were observed in each group (foam and hydrocolloid). Even though there was no difference between the groups examined in this study, who used the dressing for 6‐ to 12‐hour periods, hyperemia must be highlighted as a signal within the development chain of the DRPI.
Previous research to investigating the use of PPE and the occurrence of DRPI showed that the prevalence of skin injuries was higher in physicians, people who sweat more, males, aged over 35 years old, and who used PPE for more than 4 hours. 13 However, since no participant developed skin injuries in our study, it is impossible to compare the findings.
Most professionals in the institution where this study was conducted continuously used the N95 mask during their shift. Considering a series of cases that demonstrated the relationship between the occurrence of pressure injuries on the nose bridge and the use of N95 mask over 4 hours, 22 we can infer that the use of prophylactic dressing led to the prevention of this occurrence.
Although these prophylactic dressings were initially developed to prevent pressure ulcers in bone prominences of bedridden patients, 23 , 24 they also had positive effects when adapted to prevent this event in professionals working in health settings, perhaps because the mechanical forces involved in the development of skin injuries are the same for patients and professionals who use PPE for prolonged periods. 3 , 4 , 25 , 26
The literature presents a divergence of opinion among researchers regarding the use of these dressings to prevent DRPI by using PPE. 3 , 18 , 19 , 27 The most cautious ones emphasize the increased risk of professional contamination by coronavirus when a dressing is placed under a particulate respirator. 3 However, to reduce this risk, those in favor recommend using dressings that are thin, non‐traumatic in the removal, absorbent, and adaptable to the contours of the facial structures, thus ensuring the correct sealing of the mask. 18 , 19 , 27
Although authors claim that these characteristics are found in thin foam dressings with silicone, hydrocolloid, and film, 18 , 28 the absence of some of these attributes reported by the professionals who participated in this study was noted.
Despite being known for having a better capacity to absorb, retain, and release moisture, thus maintaining the proper balance in preserving dry skin, 28 the polyurethane foam had several reports of detachments that even culminated in the exclusion of three participants.
In the group that used hydrocolloid, the reports of discomfort were higher compared to the foam group, highlighting the difficulty in removing the dressing, followed by the sensation of itching and pain.
One can assume that such discomforts may contribute to increasing the risk of contamination by COVID‐19 or other diseases, as there may be greater contact between the professionals' hands and their face. However, there are no studies that have analyzed discomfort regarding the use of prophylactic dressing in healthcare professionals. On the other hand, a study that compared two dressings, Tegasorb and Tegaderm, in the prevention of pressure injury on the nose bridge and around the mask concluded that the dressings prevented these injuries and increased the patients' tolerance and comfort. 10
The choice of an efficient and safe dressing is crucial since the development of skin injuries increases the risk of infection, 18 in addition to being uncomfortable and causing pain. Furthermore, the development of DRPI in professionals can lead to a public health problem as it can cause not only physical, but also financial, emotional, psychological, and social impacts. 4 , 29
Although both dressings demonstrated effectiveness in preventing DRPI, we have to consider the small sample size in this study. Future research should on a larger sample size can lead to a better understanding of the effectiveness of these dressing and preventing DRPI. The cost of these materials is also a factor that should be considered by health managers to incorporate these dressings into clinical practice. Furthermore, one must emphasize the need to pay attention to the quality of the PPE used, particularly face masks, respirators, and goggles, since the anatomical characteristics of the face can influence the development of skin injuries. 4
Limitations of this study include being conducted without a control group and using professionals from a single health institution who were only followed up with once. Another characteristic that requires careful evaluation is the facial anatomical characteristics of each individual, which may have influenced the reports of discomfort. Therefore, the products must be rethought to meet the specificities of each audience.
In conclusion, foam and extra‐thin hydrocolloid proved to be effective in preventing the DRPI associated with the use of PPE by health professionals working on the front line against coronavirus. Discomfort related to the use of the dressing was reported in both groups, but no significant differences were found.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
ACKNOWLEDGMENTS
This study was supported by grants from the University of Campinas Research Fund ‐ Faepex (Grant No. 2374/20).
Gasparino RC, Lima MHM, de Souza Oliveira‐Kumakura AR, da Silva VA, de Jesus Meszaros M, Antunes IR. Prophylactic dressings in the prevention of pressure ulcer related to the use of personal protective equipment by health professionals facing the COVID‐19 pandemic: A randomized clinical trial. Wound Rep Reg. 2021;29:183–188. 10.1111/wrr.12877
REFERENCES
- 1. World Health Organization . COVID‐19 strategy update; April 14, 2020. Available from: https://www.who.int/publications-detail/strategic-preparedness-and-response-plan-for-the-new-coronavirus . [Cited August 11, 2020].
- 2. Jin YH, Cai L, Cheng ZS, et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019‐nCoV) infected pneumonia (standard version). Mil Med Res. 2020;7(4):1‐23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. National Pressure Injury Advisory Panel . NPIAP position statements on preventing injury with N95 masks; 2020. Available from: https://cdn.ymaws.com/npiap.com/resource/resmgr/position_statements/Mask_Position_Paper_FINAL_fo.pdf. [Cited August 1, 2020]
- 4. Gefen A, Ousey K. Update to device‐related pressure ulcers: SECURE prevention. COVID‐19, face masks and skin damage. J Wound Care. 2020;29(5):245‐259. [DOI] [PubMed] [Google Scholar]
- 5. Mills J. Medics left with sore marks all over their skin from coronavirus face masks. Metro; February 5, 2020. [Cited August 12, 2020]. Available from: https://metro.co.uk/2020/02/05/medics-left-sore-marks-skin-coronavirus-face-masks-12188952/
- 6. Field MH, Rashbrook JP, Rodrigues JN. Hydrocolloid dressing strip over bridge of nose to relieve pain and pressure from filtered face piece (FFP) masks during the coronavirus (COVID‐19) pandemic. Ann R Coll Surg Engl. 2020;102(5):394‐396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Black J, Kalowes P. Medical device‐related pressure ulcers. Chronic Wound Care Management and Research. 2016;3:91‐99. [Google Scholar]
- 8. National Pressure Ulcer Advisory Panel . NPUAP for immediate release: change in terminology and staging updates; 2016. Available at: http://www.npuap.org/national-pressure-ulcer-advisory-panel-npuap-announces-a-change-in-terminology-from-pressure-ulcer-to-pressure-injury-and-updates-the-stages-of-pressure-injury. [Cited October 15, 2020].
- 9. Phan LT, Maita D, Mortiz DC, Weber R, Pedicini CF, Bleasdale SC. Personal protective equipment doffing practices of healthcare workers. J Occup Environ Hyg. 2019;16(8):575‐581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Weng MH. The effect of protective treatment in reducing pressure ulcers for non‐invasive ventilation patients. Intensive Crit Care Nurs. 2008;24(5):295‐299. [DOI] [PubMed] [Google Scholar]
- 11. Miske LJ, Stetzer M, Garcia M, Stellar JJ. Airways and injuries protecting our pediatric patients from respiratory device related pressure injuries. Crit Care Nurs Clin N Am. 2017;29:187‐204. [DOI] [PubMed] [Google Scholar]
- 12. Huang TT, Tseng CE, Lee TM, Yeh JY, Lai YY. Preventing pressure sores of the nose ala after nasotracheal tube intubation: from animal model to clinical application. J Oral Maxillofac Surg. 2009;67(3):543‐551. [DOI] [PubMed] [Google Scholar]
- 13. Jiang Q, Song S, Zhou J, et al. The prevalence, characteristics, and prevention status of skin injury caused by personal protective equipment among medical staff in fighting COVID‐19: a multicenter, cross‐sectional study. Adv Wound Care. 2020;9(7):357‐364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Clark M, Black J, Alves P, et al. Systematic review of the use of prophylactic dressings in the prevention of pressure ulcers. Int Wound J. 2014;11(5):460‐471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Schulz KF , Altman DG, Moher D, CONSORT Group . CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;c332:340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Cohen J. A power primer. Psychol Bull. 1992;112(1):155‐159. [DOI] [PubMed] [Google Scholar]
- 17. Hintze J. PASS 13; 2014. NCSS, LLC, Kaysville, UT.
- 18. Alves P, Gefen A, Moura A, Vaz A, Ferreira A, Beeckman D, et al. PRPPE | COVID 19 – UPDATE. Prevention of skin lesions caused by personal protective equipment (face masks, respirators, visors, and protection glasses). Associação Portuguesa de Tratamento de Feridas; 2020.
- 19. Ramalho AO, Rosa TS, González CVS, Freitas PSS. Skin injuries related to use of personal protection equipment in health care professionals: prevention strategies for facing the covid pandemic. April 2020. Available from: http://www.sobest.org.br/arquivos/Manual_LPRDM_versa__oingle__s_2.pdf
- 20. Center for Disease Control and Prevention . Filtering out Confusion: Frequently asked questions about respiratory protection, user seal check. Pittsburgh, PA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH); 2018.
- 21. World Health Organization . Rational use of personal protective equipment (PPE) for coronavirus disease (COVID‐19): interim guidance. Available from: https://apps.who.int/iris/handle/10665/331498. [Cited August 8, 2020].
- 22. Lam UM, Siddik NSFMM, Yussof SJM, Ibrahim S. N95 respirator associated pressure ulcer amongst COVID‐19 health care workers. Int Wound J. 2020;5:1‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Ramundo J, Pike C, Pittman J. Do prophylactic foam dressings reduce heel pressure injuries? J Wound Ostomy Continence Nurs. 2018;45(1):75‐82. [DOI] [PubMed] [Google Scholar]
- 24. Jackson M, Verano J, Fry J, Rodriguez A, Russian C. Skin preparation process for the prevention of skin breakdown in patients who are intubated and treated with rotoprone. Respir Care. 2012;57(2):311‐314. [DOI] [PubMed] [Google Scholar]
- 25. Black JM, Cuddigan JE, Walko MA, Didier LA, Lander MJ, Kelpe MR. Medical device related pressure ulcers in hospitalised patients. Int Wound J. 2010;7(5):358‐365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Lemyze M, Mallat J, Nigeon O, et al. Rescue therapy by switching to total face mask after failure of face mask‐delivered noninvasive ventilation in do‐not‐intubate patients in acute respiratory failure. Crit Care Med. 2013;41(2):481‐488. [DOI] [PubMed] [Google Scholar]
- 27. Ramalho AO, Freitas PSS, Nogueira PC. Medical device‐related pressure injury in health care professionals in times of pandemic. ESTIMA, Braz. J Enterostomal Ther. 2020;18:e0120. [Google Scholar]
- 28. Galetto SGS, Nascimento ERP, Hermida PMV, Malfussi LBH. Medical device‐related pressure injuries: an integrative literature review. Rev Bras Enferm. 2019;72(2):505‐512. [DOI] [PubMed] [Google Scholar]
- 29. Jackson D, Sarki AM, Betteridge R, Brooke J. Medical device‐related pressure ulcers: a systematic review and meta‐analysis. Int J Nurs Stud. 2019;92:109‐120. [DOI] [PubMed] [Google Scholar]