

Abstract
Aims
Restrictions to alcohol availability during the first and second waves of the COVID‐19 pandemic in Australia included closures of businesses where alcohol is sold for on‐premises consumption (pubs, bars, restaurants and cafes), but not where alcohol is sold for off‐premises consumption (take‐away and home delivery). This study aimed to compare beer consumption before and after restrictions to alcohol availability during the first and second waves of COVID‐19 in Australia.
Design
Interrupted time–series analysis.
Setting
Australia.
Participants
Estimated resident population aged 15+ years.
Measurements
Seasonally adjusted estimates of beer per capita consumption measured in litres of alcohol (LALs) per week, disaggregated by on‐ and off‐premises sales.
Findings
First‐wave restrictions (week beginning 23 March 2020) were associated with a significant immediate reduction in on‐premises beer per capita consumption [−0.013 LALs, 95% confidence interval (CI) = −0.013 to –0.012, P = < 0.001], but no significant change in off‐premises beer per capita consumption. Partial removal of first‐wave restrictions (week beginning 18 May 2020) was associated with a significant immediate increase in on‐premises beer per capita consumption (+0.003 LALs, 95% CI = 0.001 to 0.004, P = 0.006), but no significant change in off‐premises beer per capita consumption. Second‐wave restrictions (week beginning 06 July 2020) were associated with a significant immediate reduction in on‐premises beer per capita consumption (−0.004 LALs, 95% CI = −0.006 to –0.002, P = 0.001) but, again, no significant change in off‐premises beer per capita consumption.
Conclusion
Restricting the availability of on‐premises alcohol during the first and second waves of the COVID‐19 pandemic in Australia was associated with significant reductions in on‐premises beer consumption, but no significant changes in off‐premises beer consumption.
Keywords: Alcohol consumption, Alcohol availability, Beer, Time series analysis, COVID‐19, pandemic
Introduction
The COVID‐19 pandemic has resulted in dramatic changes in people's lives and life‐styles world‐wide. Throughout 2020, populations in most countries have been subject to measures aimed at controlling the spread of COVID‐19, such as physical distancing or isolating at home. At the same time, a small number of countries (e.g. South Africa, Thailand) temporarily banned all alcohol sales, and in several jurisdictions (e.g. parts of Europe and North America, United Kingdom, Australia) on‐premises drinking venues have been temporarily closed or given reduced trading hours and patron numbers [ 1, 2, 3]. Meanwhile, off‐premises alcohol businesses have generally been permitted to continue trading. Internationally, there are concerns about alcohol consumption during the pandemic, including fears that social isolation may lead to increased psychological stress and subsequent increases in drinking [ 4]. In the United Kingdom, experts observed a spike in off‐premises alcohol sales at the start of the COVID‐19 outbreak in March 2020 and warned that without preventive action we may see a ‘toll of increased alcohol harm for a generation’ [ 5].
Despite these concerns, the impact of the pandemic on drinking remains unclear. Rehm and colleagues [ 1] outline plausible mechanisms for both increases and decreases in drinking during the pandemic, suggesting that a decrease is more likely. However, reliable evidence remains rare. Data from various sources report short‐term increases in dollars spent on alcohol, potentially driven by fears of greater restrictions [ 6, 7, 8]. However, these do not always capture corresponding declines in on‐premise sales, and are not easily converted into estimates of alcohol consumption. Survey data have produced mixed findings. A survey of 1555 British drinkers found that more people reported reductions in their drinking than increases [ 9], while a German study found the opposite, citing higher stress as a driver of increased drinking [ 10]. A large Canadian survey found approximately three‐quarters reported no change to their alcohol consumption during the pandemic, with only small proportions reporting increases or decreases [ 11].
In Australia, some self‐report surveys of adults conducted in April and May 2020 show similar proportions of respondents increasing or decreasing alcohol consumption since the COVID‐19 restrictions [ 12, 13, 14]. Increases were higher in certain demographic groups (e.g. women, younger age groups) [ 12, 13, 15], while decreases were higher in those who, before the pandemic, report usually drinking outside the home [ 16].
Setting
Australia is among several countries that have experienced an apparent first and second wave of COVID‐19 cases [ 17]. Australia's first wave of new daily COVID‐19 cases peaked on March 28 (n = 464) [ 18]. Case numbers then declined in April and remained low from May to mid‐June, but increased from mid‐June with an apparent second wave that peaked on August 5 (n = 698). Among the public health interventions implemented during the first wave of COVID‐19 in Australia was the mandatory closure of pubs, bars, restaurants and cafes from 23 March, effectively prohibiting on‐premises alcohol consumption (see details of COVID‐19 restrictions in Supporting information, Table S1). Major events (e.g. sports) where on‐premises alcohol would usually be available were also prohibited. Consequently, the availability of alcohol was restricted to off‐premises sales (i.e. takeaway, home‐delivery), as this sector was permitted to trade. While these restrictions were prescribed by Australia's federal government, regulatory responsibility for alcohol availability in Australia rests with state and territory governments. As the first wave subsided, some restrictions were partially relaxed. From 15 May, on‐premises alcohol outlets re‐opened in most states and territories, albeit with partial restrictions (e.g. maximum patron numbers, physical distancing rules, drinking permitted only when dining). As the second wave of COVID‐19 worsened from mid‐June, partial restrictions for on‐premises alcohol sales remained across the country. Additionally, in the state of Victoria, where the second‐wave outbreak was concentrated, on‐premises alcohol outlets were ordered to close from 9 July, and from 2 August a night‐time curfew and movement restrictions were introduced in the metropolitan area.
Economic and employment conditions in Australia deteriorated during the pandemic. The national unemployment rate increased from 5.2% in March to 7.5% in July, surpassing unemployment during the global financial crisis (June 2009: 5.9%) [ 19]. The Australian government implemented several employment and income support programmes during the pandemic, including two stimulus payments to low‐/limited‐income individuals (12 and 22 March), fortnightly wage subsidies for businesses affected by COVID‐19 (from 30 March) and increases in fortnightly unemployment benefits (from 27 April).
Despite concerns about the potential for increased alcohol use during the first and second waves of COVID‐19, the evidence to date is inconclusive regarding the overall impact on consumption levels in Australia and elsewhere. The aim of this study is to compare beer consumption before and after the first and second waves of COVID‐19 restrictions to alcohol availability in Australia.
Methods
Data
We utilize time–series data on domestic beer sales volumes for the weeks beginning 27 July 2015 to 5 October 2020 from the Australian Tax Office [ 20]. These data are timely, offer a high degree of precision and are disaggregated by on‐ and off‐premises sales, which is pertinent to our study aims. Using data on alcohol sales administered by the government taxation agency, we generally avoid the problem of measurement error (i.e. under‐counting or recall biases) inherent in self‐reported consumption measures. Additionally, these high‐frequency data (i.e. weekly observations) can potentially detect temporal effects that may be obscured in monthly or quarterly data. Because beer has a relatively short shelf‐life, and is therefore potentially less likely to be stockpiled than expensive alcohol (e.g. spirits) [ 21], we assume that weekly beer sales are generally proximal to same‐week consumption. Comparable data are not available for wine and spirits, and therefore we cannot examine changes in consumption among those categories or total alcohol consumption. However, because beer represents the largest share (39.0%) of total alcohol consumed in Australia [ 22], changes to beer consumption potentially impact overall consumption in the population, notwithstanding the possibility of some substitution with other categories. Importantly, beer is disproportionately involved in risky drinking in Australia [ 23].
Measures
Our outcome measure is the estimated level of beer per capita consumption (BPC) in litres of pure alcohol (LALs) per week in Australia. Using published estimates of alcohol content in beer [ 22], we calculated gross LALs from the taxed volume of alcohol in beer, disaggregated by trade sector (on‐premises and off‐premises). Per capita LALs were calculated using the estimated resident population of Australia aged 15+ years [ 24]. Prior to analysis, we seasonally adjusted the weekly BPC time series in EViews 11 [ 25] using STL decomposition [ 26].
Analysis
We use interrupted time–series (ITS) analysis to compare BPC levels before and after the first and second waves of COVID‐19 restrictions to alcohol availability. ITS analysis is considered the strongest, quasi‐experimental design to evaluate longitudinal effects of time‐delimited interventions [ 27]. ITS analysis is suitable for investigating the effect of population‐level alcohol policy interventions not amenable to using randomized controlled trials (RCTs), particularly where only aggregate data are available. The approach is useful for estimating not only the effect of introducing an intervention, but also the effect of full or partial removal of an intervention [ 28].
A methodological challenge we face is the lack of a comparison group, as the outcome is measured nationally. However, ITS analysis is well suited for these single‐group situations, as it projects the pre‐intervention trend into the treatment period as the counterfactual [ 27]. Furthermore, the long pre‐intervention period in our analysis (n = 247 weekly observations) significantly increases the power of the ITS model in detecting secular trends [ 29]. Our single‐group ITS model is an OLS regression with BPC on‐ and off‐premises as the dependent variables, and three independent indicator variables representing the timing (week beginning) of the interventions (pre‐intervention periods 0, otherwise 1). This model estimates the immediate effect (i.e. change in level) of each intervention and the effect over time (i.e. change in trend) following each intervention.
To identify possible autocorrelation in the time–series, we use the Cumby–Huizinga test [ 30]. This guided appropriate lag specifications that we included in models to adjust for autocorrelation. We assume the interventions were fully implemented in the nominated week, and that any time‐varying unmeasured confounders (e.g. changes in household disposable income) are more slowly changing and therefore distinguishable from the sudden change in the indicator variables. Notwithstanding this, for sensitivity testing we include pseudo start‐ and end‐times of the interventions (e.g. 1 and 2 weeks before and after the expected implementation of the interventions) and dates of potential confounders (e.g. changes in unemployment benefits). Analysis was undertaken in Stata 15 [ 31] using the ‘itsa’ command [ 32]. Analysis was not pre‐registered, and our results should be considered exploratory.
Results
In the 5 years prior to the first‐wave restrictions, on‐ and off‐premises BPC on average represented 23.3% (0.014 LALs) and 76.7% (0.045 LALs) of total weekly BPC, respectively. The long‐term pre‐intervention trends for on‐ and off‐premises BPC were close to flat (see Table 1).
Table 1.
Interrupted time–series analysis: estimated effect on beer per capita consumption (BPC) per week (LALs) of the first‐ and second‐wave COVID‐19 restrictions in Australia
| n | On‐premises BPC | Off‐premises BPC | ||||||
|---|---|---|---|---|---|---|---|---|
| Date (week beginning) | LALs | P‐value | 95% CI | LALs | P‐value | 95% CI | ||
| Starting level (pre‐intervention intercept) | 27 July 2015 | 0.0139 | < 0.001 | 0.013, 0.014 | 0.0480 | < 0.001 | 0.047, 0.050 | |
| Trend before first‐wave restrictions | 27 July 2015–16 March 2020 | 247 | < −0.0001 | 0.463 | < −0.001, < −0.001 | < −0.0001 | 0.001 | < −0.001, < 0.001 |
| Intervention 1 | ||||||||
| Level change after first‐wave restrictions | 23 March 2020 | −0.0129 | < 0.001 | −0.013, −0.012 | +0.0057 | 0.610 | −0.016, 0.028 | |
| Trend change after first‐wave restrictions | 23 March–11 May 2020 | 8 | < 0.0001 | 0.770 | −0.001, < 0.002 | −0.0009 | 0.673 | −0.005, 0.003 |
| Intervention 2 | ||||||||
| Level change after partial removal of first‐wave restrictions | 18 May 2020 | +0.0026 | 0.006 | 0.001, 0.004 | +0.0101 | 0.198 | −0.005, 0.025 | |
| Trend change after partial removal of first‐wave restrictions | 18 May–29 June 2020 | 7 | +0.0015 | < 0.001 | 0.001, 0.002 | +0.0002 | 0.926 | −0.004, 0.005 |
| Intervention 3 | ||||||||
| Level change after second‐wave restrictions | 6 July 2020 | −0.0041 | 0.001 | −0.006, −0.002 | +0.0049 | 0.384 | −0.006, 0.016 | |
| Trend change after second‐wave restrictions | 6 July–5 October 2020 | 14 | −0.0015 | < 0.001 | −0.002, −0.001 | +0.0006 | 0.287 | < 0.001, 0.002 |
Total n = 276 (weeks beginning 27 July 2015–5 October 2020, inclusive).
BPC = beer per capita consumption;
LALs: litres of pure alcohol.
Per capita is based on the Australian population aged 15+ years.
On‐premises: beer supplied from containers > 48 litres (e.g. kegs). Off‐premises: beer supplied from containers < 48 litres (e.g. cans, bottles).
Models adjusted for autocorrelation with lag length based on Cumby–Huizinga test: on‐premises BPC (lag 3, P‐value = 0.0003); off‐premises BPC (lag 1, P‐value = 0.0032).
Interrupted times–series analysis found the first‐wave restrictions, measured from 23 March 2020, were associated with a significant immediate level reduction in on‐premises BPC (−0.013 LALs, P < 0.001) (see Fig. 1). In contrast, no significant level change in off‐premises BPC was found. Changes in the trend for both on‐ and off‐premises BPC were small and not significant.
Figure 1.
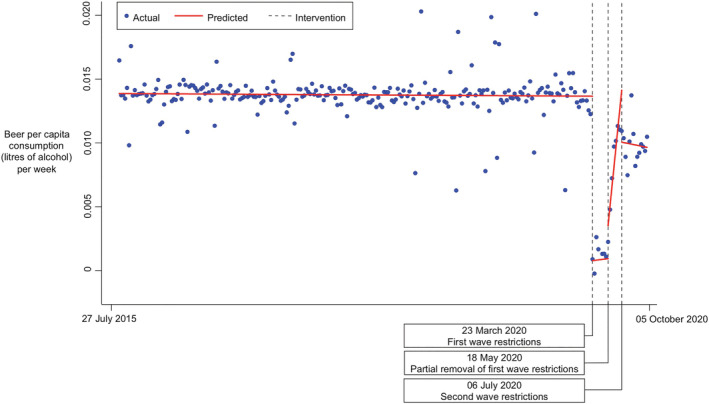
Interrupted time–series analysis: on‐premises beer per capita consumption per week in Australia before and after first and second wave of COVID‐19 restrictions. [Colour figure can be viewed at wileyonlinelibrary.com]
Partial removal of the first‐wave restrictions, measured from 18 May 2020, was associated with a significant immediate level increase in on‐premises beer consumption (+0.003 LALs, P = 0.006), but no significant change in off‐premises beer consumption was found. For on‐premises BPC, partial removal of first‐wave restrictions was also associated with a significant increase in the weekly trend (+0.002 LALs, P < 0.001). In contrast, the change in trend for off‐premises BPC was not significant.
Second‐wave restrictions, measured from 06 July 2020, were associated with a significant immediate level reduction in on‐premises beer consumption (−0.004 LALs, P = 0.001). However, no significant level change in off‐premises consumption was found. Second‐wave restrictions were also associated with a significant decrease in the weekly trend in on‐premises BPC (−0.002 LALs, P < 0.001), but no significant change in the off‐premises BPC trend was found.
Sensitivity testing using pseudo start‐ and end‐dates for each intervention and possible confounders (e.g. timing of increased unemployment benefits, wage subsidies) did not produce significant estimates that differed widely from our results. As a robustness test of our findings, we fitted Prais–Winsten AR(1) regression models with robust standard errors as an alternative specification (results not shown). These alternative models for on‐ and off‐premises BPC adjusted well for autocorrelation (Durbin–Watson statistics: 2.02 and 2.02, respectively) and produced estimates close to our original model.
Discussion
There had been no prior analysis of objective empirical data to compare alcohol consumption before and after restrictions to alcohol availability during the first and second waves of the COVID‐19 pandemic in Australia. We find that the first‐ and second‐wave restrictions were associated with large and significant reductions in weekly on‐premises beer consumption but no significant change in off‐premises beer consumption. The partial removal of first‐wave restrictions was associated with a significant increase in on‐premises beer consumption, but this was small and did not fully offset the reductions that occurred following the first‐wave restrictions.
These findings are not directly comparable to the early research on alcohol use during COVID‐19 restrictions in Australia, as those involved surveys of individuals and relied upon self‐reported changes in drinking [ 12, 13, 14, 15, 16]. However, interestingly, the Australian survey research suggests that some reductions in alcohol consumption during COVID‐19 restrictions were driven by individuals’ reduced consumption outside the home (e.g. on‐premises), particularly in young men and high‐risk drinkers [ 16]. Our analysis, focusing on beer consumption, probably reflects changes in men's drinking and is broadly consistent with those survey findings. The lack of data on wine or spirits represents a key limitation, as there is some possibility that substitution between beer and these categories may have occurred during the restrictions. However, our study nonetheless provides a detailed assessment of how consumption of the largest alcohol category—beer—has changed before and after the first and second waves of COVID‐19 restrictions in Australia. Where possible, we tested for potential confounding factors that may bias our results (e.g. changes to unemployment benefits), although data limitations precluded examining some factors (e.g. changes in household disposable income). Furthermore, while we estimate the effects on national aggregate beer consumption, the effects are likely to differ between individuals (e.g. heavy drinkers) and beverage categories, and between state and territories, depending on the extent of alcohol availability restrictions and other contextual factors.
The most plausible explanation for the reductions in on‐premises beer consumption we found during the first and second waves of the COVID‐19 pandemic is reduced availability due to full closures or partial restrictions of on‐premise alcohol outlets. However, other factors should be considered. Previous research shows that, during economic crises, budget constraints due to job loss or reduced income can lower drinking [ 33], even when the plausible drivers of drinking such as stress are increased [ 4]. The increasing rate of unemployment in Australia during the pandemic underlines the salience of this factor, especially given the disproportionate rate of job losses among relatively low‐paid casual workers [ 34]. However, in the current pandemic, financial constraints on drinking may have been partially offset by government assistance, including temporary increases in unemployment benefit payments, wage subsidies, the provision of free child care and permitting individuals to apply for early access to retirement savings. Also, increases in income among those who remained employed (or became over‐employed) may have affected consumption. However, there have also been reduced opportunities to drink during the pandemic that are likely to have contributed to lower consumption, including the cancellation of major events (e.g. sports, festivals), reduced tourism, physical distancing rules, bans on large gatherings and directives to work from home.
From a public health perspective, the apparent reductions in beer consumption represent an unexpected benefit from the COVID‐19 restrictions. It is estimated that 4.5% of the total burden of disease in Australia is due to alcohol use, ranking it as the sixth leading contributor to disease burden [ 35]. If the reductions in beer consumption are maintained and occur similarly in other categories (e.g. wine, spirits), then substantial longer‐term public health benefits are possible. Ongoing research is necessary to assess how consumption might change as COVID‐19‐related restrictions change in the coming months, alongside research to identify vulnerable groups who may have experienced increases in drinking and harm during the pandemic.
Declaration of interest
None.
Author contributions
Brian Vandenberg: Conceptualization; data curation; formal analysis; investigation; methodology; writing‐original draft; writing‐review & editing. Michael Livingston: Resources; writing‐review & editing. Kerry O'Brien: Resources; writing‐review & editing.
Supporting information
Table S1 Changes to alcohol availability in Australia during the first and second waves of the COVID‐19 pandemic.
Vandenberg, B. , Livingston, M. , and O'Brien, K. (2021) When the pubs closed: beer consumption before and after the first and second waves of COVID‐19 in Australia. Addiction, 116: 1709–1715. 10.1111/add.15352
References
- 1. Rehm J., Kilian C., Ferreira‐Borges C., Jernigan D., Monterio M., Parry C. D. H., et al. Alcohol use in times of the COVID‐19: implications for monitoring and policy. Drug Alcohol Rev 2020; 39: 301–304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Hobin E., Smith B. Is another public health crisis brewing beneath the COVID‐19 pandemic? Can J Public Health 2020; 111: 392–396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Reynolds J., Wilkinson C. Accessibility of ‘essential alcohol’ in the time of COVID‐19: casting light on the blind spots of licensing? Drug Alcohol Rev 2020; 39: 305–308. [DOI] [PubMed] [Google Scholar]
- 4. Clay J. M., Parker M. O. Alcohol use and misuse during the COVID‐19 pandemic: a potential public health crisis. Lancet 2020; 5: e259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Finlay I., Gilmore I. COVID‐19 and alcohol—a dangerous cocktail. BMJ 2020; 10.1136/bmj.m1987 [DOI] [PubMed] [Google Scholar]
- 6. Australian Bureau of Statistics (ABS) . Retail Trade, Australia, September 2020, Cat. no. 8501.0. Canberra, Commonwealth of Australia: ABS; 2020.
- 7. CommBank . An early look at how coronavirus is affecting household spending, 30 March 2020. Available at: https://www.commbank.com.au/guidance/business/an‐early‐look‐at‐how‐the‐coronavirus‐is‐affecting‐household‐spen‐202003.html (accessed 01 April 2020).
- 8. Office of National Statistics (ONS) . Retail Sales, Great Britain: March 2020. London: ONS; 2020. Available at: https://www.ons.gov.uk/businessindustryandtrade/retailindustry/bulletins/retailsales/march2020#retail‐sales‐in‐march
- 9. Alcohol Change UK . Drinking During Lockdown: Headline Findings. London: Alcohol Change UK; 2020. Available at: https://alcoholchange.org.uk/blog/2020/covid19‐drinking‐during‐lockdown‐headline‐findings
- 10. Koopmann A., Georgiadou E., Kiefer F., Hillemacher T. Did the general population in Germany drink more alcohol during the COVID‐19 pandemic lockdown? Alcohol Alcohol 2020; 55: 698–699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Statistics Canada . Canadians who report lower self‐perceived mental health during the COVID‐19 pandemic more likely to report increased use of cannabis, alcohol and tobacco. Ottowa: Statistics Canada, 2020. Available at: https://www150.statcan.gc.ca/n1/pub/45‐28‐0001/2020001/article/00008‐eng.htm?HPA=1
- 12. Australian Bureau of Statistics (ABS) . Household Impacts of COVID‐19 Survey, 29 April–4 May 2020. Cat no. 4940.0. Canberra: Commonwealth of Australia: ABS; 2020.
- 13. Biddle N., Edwards B., Gray M., Sollis K. Alcohol Consumption During the COVID‐19 period: May 2020. Canberra: ANU Centre for Social Research and Methods; 2020. Available at: https://csrm.cass.anu.edu.au/research/publications/alcohol‐consumption‐during‐covid‐19‐period‐may‐2020 (accessed 09 June 2020). [Google Scholar]
- 14. YouGov Galaxy . Alcohol sales and use during COVID‐19, Polling Snapshot. Canberra: Foundation for Alcohol Research and Education (FARE); 2020. Available at: https://fare.org.au/wp‐content/uploads/COVID‐19‐POLL.pdf
- 15. Callinan S., Smit K., Mojica‐Perez Y., D'Aquino S., Moore D., Kuntsche E. Shift in alcohol consumption during the COVID‐19 pandemic: early indications from Australia. Addiction 2020. 10.1111/add.15275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Callinan S., Mojica‐Perez Y., Wright C. J., Livingston M., Kuntsche S., Laslett A., et al. Purchasing, consumption, demographic and socioeconomic variables associated with shifts in alcohol consumption during the COVID‐19 pandemic. Drug Alcohol Rev 2020; 10.1111/dar.13200 [DOI] [PubMed] [Google Scholar]
- 17. World Health Organization (WHO) . WHO Coronavirus Disease (COVID‐19) Dashboard, 2020. Available at: https://covid19.who.int
- 18. Department of Health . Coronavirus (COVID‐19) Current Situation and Case Numbers. Canberra: Australian Government, 2020. Available at: https://www.health.gov.au/news/health‐alerts/novel‐coronavirus‐2019‐ncov‐health‐alert/coronavirus‐covid‐19‐current‐situation‐and‐case‐numbers
- 19. Australian Bureau of Statistics (ABS) . Labour Force, Australia, September 2020. Cat. no. 6202.0. Canberra: Commonwealth of Australia; 2020.
- 20. Australian Tax Office (ATO) . Excise Beer Clearance Data 2015/16–2020/21. Canberra: Commonwealth of Australia; 2020.
- 21. Robinson M., Thorpe R., Beeston C., McCartney G. A review of the validity and reliability of alcohol retail sales data for monitoring population levels of alcohol consumption: a Scottish perspective. Alcohol Alcohol 2012; 48: 231–240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Australian Bureau of Statistics (ABS) . Apparent Consumption of Alcohol 2017/18. Canberra: Commonwealth of Australia; 2019.
- 23. Australian Institute of Health and Welfare (AIHW) . National Drug Strategy Household survey 2016—Key Findings, Canberra: AIHW; 2017.
- 24. Australian Bureau of Statistics (ABS) . Australian Demographic Statistics, December 2019. Cat no. 3101.0. Canberra: Commonwealth of Australia; 2020.
- 25. IHS Global Inc . EViews 11. Irvine, CA: IHS Global Inc.; 2019.
- 26. Cleveland R. B., Cleveland W. S., McRae J. E., Terpenning I. J. STL: a seasonal‐trend decomposition procedure based on loess. J Off Stat 1990; 6: 3–33. [Google Scholar]
- 27. Kontopantelis E., Doran T., Buchan I. Regression based quasi‐experimental approach when randomisation is not an option: interrupted time series analysis. BMJ 2015; 350: h2750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Craig P., Gibson M., Campbell M., Popham F., Katikireddi S. V. Making the most of natural experiments: what can studies of the withdrawal of public health interventions offer? Prev Med 2018; 108: 17–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Ramsey C. R., Matowe L., Grilli R., Grimshaw J. M., Thomas R. E. Interrupted time series designs in health technology assessment: lessons from two systematic reviews of behaviour change strategies. Int J Technol Assess Health Care 2003; 19: 613–623. [DOI] [PubMed] [Google Scholar]
- 30. Cumby R. E., Huizinga J. Testing the autocorrelation structure of disturbances in ordinary least squares and instrumental variables regressions. Econometrica 1992; 60: 185–195. [Google Scholar]
- 31. StataCorp STATA version 15.0. College Station, TX, USA: Stata Corp; 2015. [Google Scholar]
- 32. Linden A., Arbor A. Conducting interrupted time‐series analysis for single‐ and multiple‐group comparisons. Stata J 2015; 15: 480–500. [Google Scholar]
- 33. de Goeij M. C. M., Suhrcke M., Toffolutti V., van de Mheen D., Schoenmakers T. M., Kunst A. E. How economic crises affect alcohol consumption and alcohol‐related health problems: a realist systematic review. Soc Sci Med 2015; 131: 131–146. [DOI] [PubMed] [Google Scholar]
- 34. Gilfillan G. COVID‐19: Impacts on Casual Workers in Australia—a Statistical Snapshot. Canberra: Parliamentary Library, Commonwealth of Australia, 2020. Available at: https://parlinfo.aph.gov.au/parlInfo/download/library/prspub/7262636/upload_binary/7262636.pdf (accessed 08 May 2020).
- 35. Australian Institute of Health and Welfare (AIHW) . Australian Burden of Disease Study 2015. Canberra: AIHW, 2019.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1 Changes to alcohol availability in Australia during the first and second waves of the COVID‐19 pandemic.