

Abstract
We conducted a cross‐sectional survey to better understand the barriers to attendance at canine rabies vaccination campaigns in Haiti. A structured community‐based questionnaire was conducted over a 15‐day period during May–June 2017, focused on socio‐economic status correlated with participation at canine rabies vaccination campaigns. Questions phrased as a bidding game were asked to determine individuals’ willingness to pay (WTP) for dog rabies vaccination and willingness to walk (WTW) to fixed‐point vaccination campaigns. The Kaplan–Meier estimator was applied to determine relationships between survey variables. Logistic regression was used to examine factors associated with participants’ WTP and WTW. A total of 748 households from eight communities were surveyed. Respondents were predominantly female (54.4%) and had a median age of 45 years. The total number of owned dogs reported from households was 926, yielding a human‐to‐dog ratio in dog‐owning households of 5.2:1. The majority of dogs (87.2%) were acquired for security, and 49% were allowed to roam freely; 42.0% of dog owners reported that they were unable to manage (or restrain) their dogs using a leash. Seventy per cent of dog owners were willing to pay up to 15.9 gourdes (0.25 USD) and/or walk up to 75 m to vaccinate their dogs. Households that owned free‐roaming dogs, owned dogs for the purpose of companionship and owned dogs that they were unable to walk on a leash were associated with a higher WTP for vaccination. Living in Artibonite Department, having a middle or higher household income, and owning a dog for security purpose were associated with a higher WTW for vaccination. Low leash use and propensity for dogs to roam freely are barriers to successful fixed‐point vaccination methods in Haiti, and alternative methods such as door to door (DD), capture–vaccinate–release (CVR) or oral vaccination should be explored. There may be some prospect for fee‐for‐service vaccination in Haiti; however, this programme should be introduced as a supplement, rather than a replacement for free rabies vaccination programmes so that mass dog vaccination is not discouraged.
Keywords: barriers, canine vaccination, disease control, Haiti, payment, Rabies, walk, zoonosis
1. INTRODUCTION
Rabies is one of the most lethal of all infectious diseases. It is characterized by encephalitis and generalized paresis. Rabies has a high case fatality rate, and deaths typically occur within 7–10 days after the onset of symptoms in the absence of supportive care (Fisher, Streicker, & Schnell, 2018; Fooks et al., 2014). Globally, rabies virus is responsible for more human deaths than any other zoonotic disease.
Canine rabies virus variant (CRVV), the virus that circulates among domestic dog populations, is endemic in at least 122 countries (Fisher et al., 2018; Fooks et al., 2014). Dog bites account for over 99% of human rabies deaths, making canine rabies responsible for an estimated 59,000 human deaths per year (Cleaveland & Hampson, 2017; Hampson et al., 2015; Wallace, Undurraga, Blanton, Cleaton, & Franka, 2017). Most cases of human rabies are documented in low‐income countries, with Africa and Asia responsible for the majority of the global rabies burden (Hampson et al., 2015; Wallace, Etheart, et al., 2017). In Latin America, rabies is considered one of the most important zoonoses for human and animal health. Although efforts led by the Pan American Health Organization (PAHO) helped to decrease the canine rabies burden by approximately 90%, Haiti is one of the few Latin American countries where canine rabies has not been successfully eliminated (Freire de Carvalho et al., 2018).
Haiti has the highest burden of human rabies deaths in the western hemisphere, where an estimated 130 human rabies deaths occur annually (Hampson et al., 2015; Wallace et al., 2015). The incidence of human and canine rabies in Haiti is still not clear, and limited surveillance and under‐reporting of cases are factors that contribute to the burden of rabies in Haiti (Etheart et al., 2017; Wallace, Undurraga, et al., 2017).
Effective strategies for rabies control such as large‐scale dog vaccination programmes, dog population management, and improved access to pre‐ and post‐exposure prophylaxis for dog‐bite victims, are cornerstones of successful rabies elimination programmes. Costs to implement these control measures are high, but many studies have shown that investing in these programmes is cost‐effective when considering the economic burden of rabies, which is estimated to be USD 8.6 billion per year globally (Anderson & Shwiff, 2015; Hampson et al., 2015; Wallace, Undurraga, et al., 2017).
Dog vaccination campaigns free of charge have been practiced in Haiti for over a decade, but are rarely evaluated for coverage or effectiveness. To achieve adequate herd immunity for rabies elimination, previous studies have shown that at least 70% of dogs from a specific area must be vaccinated against rabies every year (Cleaveland & Hampson, 2017; Wallace, Undurraga, et al., 2017). Fixed‐point vaccination campaigns conducted in 2014 and 2015 were estimated to have reached approximately 40% of the dog population, and there was no meaningful decline in the number of human or animal cases following the campaign (Wallace, Etheart, et al., 2017). More recently, in 2018, Haiti adopted a combined vaccination strategy of fixed point, door to door (DD), and capture–vaccinate–release (CVR), which was estimated to achieve 74% dog vaccination coverage (Cleaton et al., 2018). Furthermore, both human and animal rabies cases declined in the following months (Monroe et al., under review). This mixed‐methods approach requires advanced planning and technical support as compared to fixed‐point vaccination methods, in which dog owners bring dogs to a pre‐announced location to be vaccinated. While mixed methods may always be required in a setting such as Haiti, improving attendance at fixed‐point or mobile fixed‐point vaccination campaigns could reduce the cost and duration of the national vaccination campaign. In this study, we investigated the perceived barriers to attending fixed‐point vaccination campaigns, with the goal of identifying approaches to improve their effectiveness in Haiti.
2. METHODS
2.1. Study design and population
A community‐based cross‐sectional study was conducted in urban areas of Haiti over a 15‐day period in May–June 2017, focused on identifying the socio‐economic barriers to attendance at canine rabies fixed‐point vaccination campaigns. Surveys were conducted in two of Haiti's 10 departments (Nord and Artibonite) shortly after canine rabies vaccination campaigns were finished (Figure 1). We aimed to survey 634 households based on an expected proportion of the households that owns dogs in Haiti of 50%, an alpha value of 0.05, a design effect of 1.5 and a non‐response rate of 10%. A modified cluster design was used for this study. Communes in Haiti are subdivided into enumeration areas (EA) by the Haitian Institute of Statistics and Information. EA were assigned a numerical value, and a random number generated was used to select 23 EAs for survey activities. Centroids of the EAs were used to start the surveys. GPS coordinates were also collected during survey activities for mapping purposes. The survey was conducted per household, and interviewers requested to speak with the head of household at each residence or a resident being greater than or equal to 18 years of age when the head of household was not available. Participants were not offered payment for their participation. Fingerprinted or signed informed consent was obtained for all respondents (see Ethical Considerations, below).
FIGURE 1.
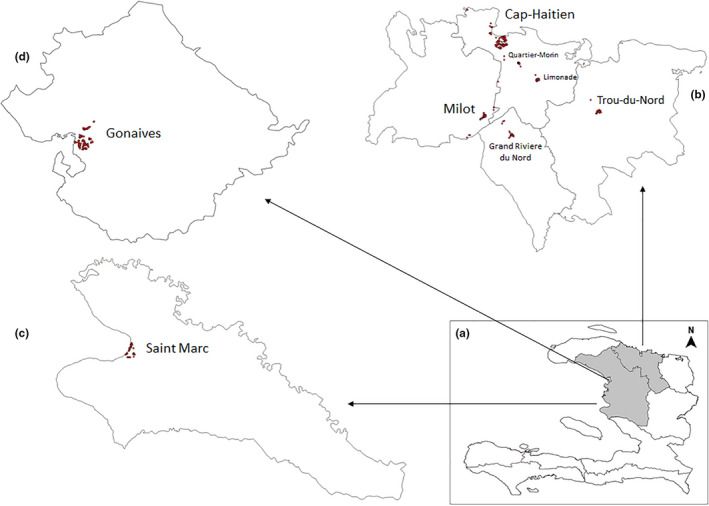
An overview of the communities surveyed in this study. (a) Map of Haiti showing North and Artibonite Departments highlighted in grey. (b) The North Department. (c and d) Artibonite Department showing Saint Marc and Gonaives area, respectively. Locations of the surveyed communities are marked with red dots
2.2. Questionnaire
A structured questionnaire was developed in English, translated into Haitian Creole and reviewed by native Haitian collaborators. The questionnaire was developed to explore socio‐economic factors that could be associated with lack of attendance at canine rabies fixed‐point vaccination campaigns. Each questionnaire consisted of 17 questions, which fell into one of four sections: socio‐demographics, economic status of households, dog‐ownership characteristics and barriers to attendance at the canine rabies vaccination campaign. Interviews were conducted in Haitian Creole by trained interview teams from Ministry of Agriculture, Natural Resources and Rural Development (MARNDR), Ministry of Public Health and the Population (MSPP), or Christian Veterinary Mission (CVM). Responses were recorded using a smartphone application (WVS App) (Gibson et al., 2016). Respondents were not provided answers from which to choose. Open‐ended questions allowed for multiple responses.
2.3. Income score
An income score was calculated based on reported ownership of nine common household items and toilet facility characteristics (Table S1). As each household item can have a different monetary value between or within countries, we calculated a weighted sum of owned items, with the weight equal to the item's rank (1–9), where 1 represented least valuable and 9 represented most valuable. A maximum of 45 points was possible, representing a household that has all listed items. For statistical analysis, we normalized this score by dividing it by 45.
We used a similar procedure to calculate the toilet facility score. Initial points ranged from 0 (no facility) to 3 (toilet connected to plumbing system). The toilet facility points were then normalized by dividing by 3, such that the final score points ranged from 0 to 1 (Table S1). The household items and toilet facility scores combined had a maximum of 2 and a minimum of 0 points. We used the sum of these values to quantify the household economic status relative to the studied population and then categorized into quartiles representing 'Poorest', 'Lower', 'Middle' and 'Richest' households. Descriptive parametric and non‐parametric statistics such as mean and median scores, standard deviation, and 95% confidence intervals were calculated.
We assessed variable ranking system and variance in scored for correlation using principal component analysis (PCA) (Balen et al., 2010; Howe et al., 2012). The results from our PCA were consistent with our ranking. Hence, the ranking system was chosen for statistical analysis out of consideration of parsimony.
2.4. Dog ownership
Among households that owned dogs, we assessed the dog's age, sex and reported confinement status (always stays at home, roams unsupervised at least part of the time, always roams unsupervised), and primary purpose (companionship, security, wealth). Owners were asked about resources they provide to their dogs as well as to dogs they do not own, including food, water, shelter and veterinary care. To assess perceptions regarding dogs belonging to a household, we asked owners if they had affection for their dog(s), if they were able to walk their dog(s) on a leash and if they felt their dog(s) were easy to replace. Human‐to‐dog ratios were calculated as the sum of the number of owned dogs divided by the total number of household members as captured in the survey.
2.5. Willingness questions
We assessed willingness to pay (WTP) for dog rabies vaccination and willingness to walk (WTW) to fixed‐point vaccination campaigns to receive the rabies vaccine for their dog(s). To quantify the maximum price (in Haitian Gourdes, HTG) and distance (in metres) one was willing to pay and walk, respectively, we used a bidding game method (Figure 2a,b) with a series of yes/no questions, following previous work detailed elsewhere (Birhane, Miranda, Dyer, Blanton, & Recuenco, 2016; Dong, Kouyate, Cairns, & Sauerborn, 2003; Watanabe, 2010). During the bidding process, 10 bid levels, each increasing and decreasing level separated by 20 HTG (~0.30 US dollars, USD), were presented to determine WTP (Figure 2a), and 8 bid levels, each increasing by 500 m and decreasing by 50 m, were presented to determine WTW (Figure 2b). Potential starting point bias was also applied as detailed by Birhane et al. (2016).
FIGURE 2.
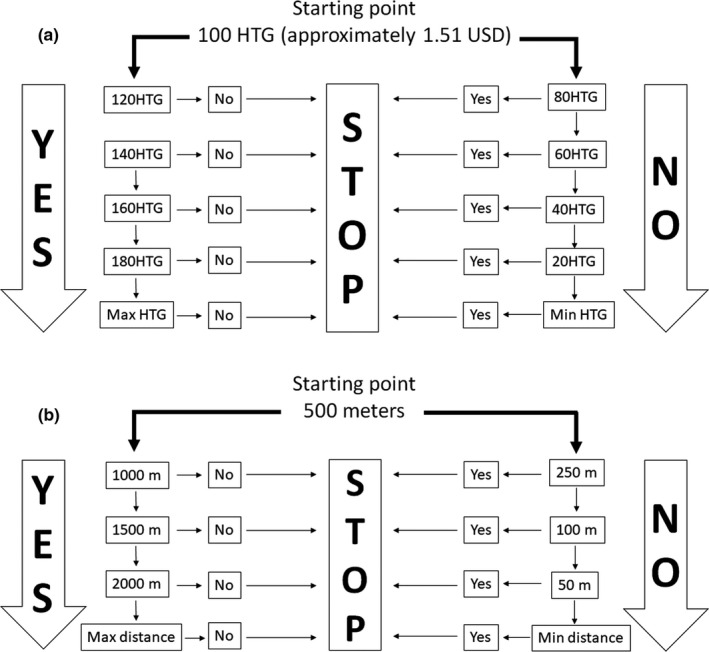
The bidding game algorithm. Two examples of the bidding game algorithm with a static generated starting point of 100 HTG (1.51 USD) used to obtain participants' maximum WTP for dog rabies vaccination (a), and a static generated starting point of 500 m used to obtain participants' maximum WTW to fixed‐point vaccination campaigns (b)
2.6. Statistical analysis
Payment and distance variables extracted from WTP and WTW questions were analysed for associations with socio‐economic status and dog‐ownership characteristics. To compare WTP and WTW between multiple subgroups, we developed Kaplan–Meier curves. Kaplan–Meier curves are traditionally used to evaluate the time to a particular event (e.g. participation in a fixed‐point vaccination). Here, we generated Kaplan–Meier curves exchanging time for payment and time for distance. A log‐rank test was used to assess statistical differences in the Kaplan–Meier curves between multiple groups, with a significance level of 5% (p ≤ .05) applied. All variables that showed a significance level of 5% in the log‐rank test were tested again in a logistic regression model to study the associations among monetary value (WTP) and distance (WTW) with socio‐economic status and dog‐ownership characteristics. Relative odds ratio and 95% confidence intervals were calculated when applicable. Analysis was performed on EPI‐INFO software version 7.2 (http://www.cdc.gov/epiinfo/). Data were collected on a smartphone application (WVS App) (Gibson et al., 2016). WTP was calculated in US Dollars and as a percentage of per capita monthly gross domestic product (GDP).
3. RESULTS
3.1. Demographic characteristics of study population
A total of 748 households were enrolled into the survey. Households were surveyed in eight urban areas: Gonaives and Saint Marc, located in Artibonite Department; Cap Haitien, Quartier‐Morin, Limonade, Milot, Grand Riviere du Nord and Trou‐du‐Nord, located in North Department (Figure 1). Since questions were also asked about all household members, the 748 surveyed households captured information about 4,809 persons (6.4 people per household). Demographic characteristics of the respondents and household characteristics are presented in Table 1.
TABLE 1.
Demographic characteristics of the 748 surveyed households from North and Artibonite Departments, Haiti, 2017
| Variables | All households | Nord Department | Artibonite Department | χ 2 | ||
|---|---|---|---|---|---|---|
| n = 748 | n = 437 (58.4%) | n = 311 (41.6%) | ||||
|
Cap Haitien n = 187 |
Others in North a n = 250 |
Gonaives n = 157 |
Saint Marc n = 154 |
|||
| Gender | ||||||
| Female | 407 (54.4) | 101 (54.0) | 119 (47.6) | 91 (58.0) | 96 (62.3) | .02 |
| Male | 341 (45.6) | 86 (46.0) | 131 (52.4) | 66 (42.0) | 58 (37.7) | |
| Age | ||||||
| 18–20 | 42 (5.6) | 8 (4.3) | 4 (1.6) | 13 (8.3) | 17 (11.0) | <.0001 |
| 21–40 | 351 (46.9) | 81 (43.3) | 97 (38.8) | 89 (56.7) | 84 (54.6) | |
| 41–60 | 289 (38.6) | 83 (44.4) | 120 (48.0) | 39 (24.8) | 47 (30.5) | |
| >60 | 66 (8.8) | 15 (8.0) | 29 (11.6) | 16 (10.2) | 6 (3.9) | |
| Respondent education | ||||||
| None | 79 (10.6) | 14 (7.5) | 33 (13.2) | 14 (8.9) | 18 (11.7) | .0001 |
| Primary | 222 (29.7) | 71 (38.0) | 86 (34.4) | 37 (23.6) | 28 (18.2) | |
| Secondary | 360 (48.1) | 89 (47.6) | 109 (43.6) | 79 (50.3) | 83 (53.9) | |
| Higher | 16 (2.1) | 13 (7.0) | 22 (8.8) | 27 (17.2) | 25 (16.2) | |
| Household education | ||||||
| None | 39 (5.2) | 11 (5.9) | 16 (6.4) | 3 (1.9) | 8 (5.2) | .001 |
| Primary | 167 (22.6) | 61 (32.6) | 55 (22.0) | 24 (15.3) | 27 (17.5) | |
| Secondary | 352 (47.1) | 82 (43.8) | 116 (46.4) | 76 (48.4) | 78 (50.6) | |
| Higher | 190 (25.4) | 33 (17.6) | 63 (25.2) | 54 (34.4) | 40 (26.0) | |
| No. of people per household | ||||||
| 1–5 | 324 (43.3) | 86 (46.0) | 118 (47.2) | 30 (19.1) | 90 (58.4) | <.0001 |
| 6–10 | 343 (45.8) | 73 (39.0) | 117 (46.8) | 91 (58.0) | 62 (40.3) | |
| >11 | 81 (10.8) | 28 (15.0) | 15 (6.0) | 36 (22.9) | 2 (1.3) | |
| Income score | ||||||
| Poorest | 195 (26.1) | 43 (23.0) | 37 (14.8) | 35 (22.3) | 80 (51.9) | <.0001 |
| Lower | 195 (26.1) | 53 (28.3) | 58 (23.2) | 67 (42.7) | 17 (11.0) | |
| Middle | 184 (24.6) | 42 (22.5) | 77 (30.8) | 34 (21.6) | 31 (20.1) | |
| Richest | 174 (23.2) | 49 (26.2) | 78 (31.2) | 21 (13.4) | 26 (16.9) | |
Totals may not add up to 100% due to missing or not reported data.
The median age of respondents was 45.2 years (ranging from 18 to 85 years). Most respondents were female (54.4%), and the most common education level of interviewed individuals (48.1%) and household members (47.1%) was completion of secondary education only. Illiteracy was reported by 10.6% of respondents. Among all surveyed households, the mean income score was 0.83, ranging from 0.04 to 1.91.
3.2. Dog‐ownership characteristics
Survey respondents reported owning 926 dogs at the time the survey was conducted. The average number of dogs owned per household was 1.2, and the human‐to‐dog ratio was 5.2:1. The median age of an owned dog was 3.2 years (ranging from 2 months to 10 years), and most owned dogs were male (68.8%). The most common confinement status reported for owned dogs was 'always roaming freely' (49.7%), whereas <10.0% of dogs were reportedly always confined. Furthermore, almost 90.0% of the dogs were acquired for security purposes (Figure 2).
Nearly all respondents (97.6%) reported that their dogs are part of family. However, 46.6% of respondents reported feeling that their dogs are easily replaceable. The majority of respondents (78.2%) reported they provided at least one of the following services to their dogs: food, water, shelter and veterinary care (Table 2). A large proportion of dog owners (42.0%) reported that they were unable to walk their dogs on a leash. Indeed, dogs unable to be walked on a leash were almost 26 times more likely to roam freely at all times (OR = 25.7, 95% CI = 10.7–61.4) and almost 4 times more likely to roam freely part of the time (OR = 3.6, 95% CI = 1.5–8.9) compared to those dogs that were able to be walked on a leash (p < .00001).
TABLE 2.
Care provided to owned dogs from North and Artibonite Departments, Haiti, 2017
| Type of care | All Households | North Cap Haitien | Others in North | Gonaives | Saint Marc | χ 2 |
|---|---|---|---|---|---|---|
| n = 748 (%) | n = 187 (%) | n = 250 (%) | n = 157 (%) | n = 154 (%) | ||
| Care combination | ||||||
| No care provided | 3 (0.4) | 0 | 0 | 2 (1.3) | 1 (0.6) | |
| Partial care provided | 157 (21.0) | 58 (31.0) | 58 (23.2) | 143 (91.1) | 121 (78.6) | <0.0001 |
| Full care provided | 585 (78.2) | 129 (69.0) | 192 (76.8) | 9 (5.7) | 32 (21.0) | <0.0001 |
| No response | 3 (0.4) | 0 | 0 | 3 (1.9) | 0 | |
| Type of care provided a | ||||||
| Food | 739 (98.8) | 187 (100.0) | 249 (99.6) | 151 (96.2) | 152 (98.7) | 0.17 |
| Water | 699 (93.4) | 185 (98.9) | 248 (99.2) | 128 (81.5) | 138 (89.6) | <0.0001 |
| Shelter | 252 (33.7) | 73 (39.0) | 75 (30.0) | 35 (22.3) | 69 (44.8) | 0.0001 |
| Veterinary care | 193 (25.8) | 60 (32.1) | 58 (23.2) | 25 (15.9) | 50 (32.4) | 0.001 |
| None | 3 (0.4) | 0 | 0 | 2 (1.3) | 1 (0.6) | |
Multiple responses allowed. Totals may not add up to 100%.
3.3. Willingness to pay for dog rabies vaccination and willingness to walk to fixed‐point vaccination campaigns
Bidding games were completed by all dog‐owning households included in this survey, to elicit their maximum WTP for dog rabies vaccination and WTW to fixed‐point vaccination campaigns. More than 99% of the WTP for dog rabies vaccination and WTW to fixed‐point vaccination campaigns responses were above zero. Figure 3 displays the proportion of the population willing to pay a given price or more for dog rabies vaccination and willing to walk a given distance or more to fixed‐point vaccination campaigns. The reported willingness for dog vaccination falls gradually as price and distance increase. The median values for the WTP for dog rabies vaccination and WTW to fixed‐point vaccination campaigns were estimated to be 66 HTG (0.95 USD and 1.5% of per capita monthly GDP) and 370 m, respectively. Seventy per cent of the population, the target for dog vaccination programmes, were willing to pay at least 16 HTG (0.25 USD and 0.4% of per capita monthly GDP) and walk at least 75 m.
FIGURE 3.
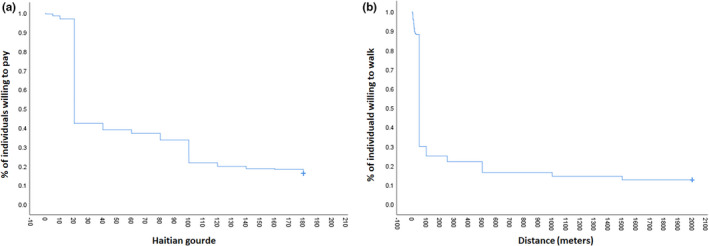
Distribution of the maximum WTP (a) for canine rabies vaccination and (b) distribution of the maximum WTW to fixed‐point vaccination campaigns in Haiti, 2017
The lowest median values for the WTP and WTW were observed in Nord Department (22 HTG, 95% CI = 21–23 and 80.1 m, 95% CI = 58–116, respectively), while the highest were observed in Saint Marc, Artibonite Department (138 HTG, 95% CI = 132–145 and 937 m, 95% CI = 790–1,083, respectively) (p < .0001) (Table 4). Younger respondents (average age = 19) were willing to pay (86 HTG, 95% CI = 66–105) (p = .001) and walk (554 m, 95% CI = 332–776) (p = .007) more than older individuals (average age = 66) (58 HTG, 95% CI = 43–73; and 301 m, 95% CI = 322–418). Female survey respondents were willing to pay more (71 HTG, 95% CI = 64–77) than male respondents (59 HTG 95% CI = 53–66) (p = .02), but no significant differences were observed for WTW by gender (Table 3). Households with 6–10 people reported that they would walk an average of 294 m compared to households with 1–5 or >11 people who would walk much farther (435 and 434 m, respectively). Participants with a higher level of education were also willing to pay and walk more than those with a lower level of education (at both the respondent and household level). Individuals with a higher‐income level were willing to pay and walk more than individuals with a lower‐income level (p < .0001 and p = .001, respectively) (Table 3).
TABLE 4.
Univariate analysis of dog‐ownership status per household associated with willingness to pay (WTP) and walk (WTW) for dog rabies vaccination campaigns in Haiti, 2017
| Variables | Median WTP (HTG) | 95% CI | p value a | Median WTW (m) | 95% CI | p value a |
|---|---|---|---|---|---|---|
| Number of dogs | ||||||
| 1 | 70.0 | 63.4–76.6 | .002 | 308.2 | 242.3–374.2 | .79 |
| 2 | 56.3 | 46.8–65.7 | 308.9 | 204.0–413.8 | ||
| ≥3 | 49.1 | 36.9–61.3 | 239.7 | 113.0–366.5 | ||
| Gender | ||||||
| Female only | 83.6 | 71.8–95.5 | .002 | 453.3 | 323.3–583.3 | .017 |
| Male only | 57.2 | 51.0–63.4 | 234.4 | 176.2–292.7 | ||
| Female and male | 58.9 | 48.1–69.6 | 306.2 | 185.3–427.1 | ||
| Confinement status | ||||||
| Always confined | 31.6 | 22.7–40.4 | <.0001 | 140.4 | 51.1–229.6 | .002 |
| Always free | 65.6 | 59.1–72.1 | 338.3 | 264.5–412.2 | ||
| Sometimes free | 68.4 | 58.3–68.6 | 237.2 | 155.0–319.3 | ||
| Primary purpose | ||||||
| Companionship | 123.6 | 110.3–137.0 | <.0001 | 281.8 | 154.1–409.6 | .002 |
| Security | 54.7 | 49.5–59.8 | 311.9 | 253.7–370.1 | ||
| Wealth | 74.1 | 45.5–102.9 | 95.8 | 53.3–138.4 | ||
| Dogs are part of family | ||||||
| Agree | 60.8 | 56.3–65.2 | <.0001 | 303.5 | 258.8–348.2 | <.0001 |
| Disagree | 143.0 | 125.8–160.1 | 1,440.1 | 1,212.2–1,668.1 | ||
| Feel affection for the dogs | ||||||
| Agree | 65.3 | 60.7–70.0 | .016 | 361.8 | 313.7–410.0 | .004 |
| Disagree | 123.3 | 86.0–160.8 | 808.3 | 251.8–1,364.8 | ||
| Dog easy to replace | ||||||
| Agree | 57.0 | 50.3–63.3 | <.0001 | 338.6 | 269.3–408.0 | .25 |
| Disagree | 72.1 | 66.0–78.4 | 384.0 | 317.1–450.8 | ||
| Dog accustomed to leash | ||||||
| Agree | 60.0 | 54.3–65.7 | .015 | 318.8 | 258.3–379.3 | .67 |
| Disagree | 72.7 | 65.2–80.1 | 431.2 | 352.4–510.0 | ||
Abbreviation: HTG, Haitian Goude.
p value was calculated through Kaplan–Meier log‐rank test.
TABLE 3.
Univariate analysis of demographic factors associated with willingness to pay (WTP) and walk (WTW) for dog rabies vaccination campaigns in Haiti, 2017
| Variables | Median WTP (HTG) | CI 95% | p value a | Median WTW (m) | CI 95% | p value a |
|---|---|---|---|---|---|---|
| Location | ||||||
| North Cap Haitien | 26.2 | 23.4–29.0 | <.0001 | 94.7 | 43.8–116.3 | <.0001 |
| Others in North | 21.7 | 20.7–22.7 | 80.1 | 58.1–131.3 | ||
| Gonaives | 110.8 | 100.2–121.4 | 598.4 | 490.0–706.9 | ||
| Saint Marc | 138.4 | 132.1–144.8 | 937.0 | 790.0–1,082.9 | ||
| Age | ||||||
| 18–20 | 85.5 | 66.1–104.8 | .001 | 554.0 | 331.7–776.2 | .007 |
| 21–40 | 72.7 | 66.1–79.4 | 412.6 | 339.1–486.1 | ||
| 41–60 | 55.7 | 48.8–62.6 | 307.7 | 237.1–378.4 | ||
| >60 | 57.8 | 42.7–73.0 | 301.3 | 322.3–418.1 | ||
| Gender | ||||||
| Female | 70.7 | 64.4–77.1 | .02 | 394.0 | 327.4–460.5 | .87 |
| Male | 59.4 | 53.1–65.7 | 341.8 | 273.3–410.3 | ||
| No. of People per Household | ||||||
| 1–5 | 66.1 | 59.0–73.1 | .86 | 434.8 | 355.0–514.6 | .03 |
| 6–10 | 65.3 | 58.8–71.7 | 294.0 | 231.6–356.5 | ||
| >11 | 65.0 | 50.7–79.2 | 434.3 | 288.6–580.1 | ||
| Respondent education | ||||||
| None | 41.7 | 30.5–53.0 | <.0001 | 275.0 | 146.2–404.0 | .003 |
| Primary | 48.7 | 41.9–55.6 | 260.0 | 185.4–334.0 | ||
| Secondary | 77.6 | 70.7–84.4 | 431.6 | 358.0–505.4 | ||
| Higher | 80.5 | 66.1–94.8 | 484.3 | 330.8–637.8 | ||
| Household education | ||||||
| None | 28.7 | 18.3–39.1 | <.0001 | 152.6 | 14.2–291.1 | .03 |
| Primary | 34.8 | 28.4–41.3 | 300.0 | 206.5–393.6 | ||
| Secondary | 79.4 | 72.5–86.3 | 441.9 | 365.6–518.2 | ||
| Higher | 73.7 | 64.5–83.0 | 333.9 | 249.3–418.6 | ||
| Income score | ||||||
| Poorest | 47.3 | 41.3–53.3 | <.0001 | 192.7 | 133.2–252.2 | .001 |
| Lower | 45.4 | 37.2–53.6 | 276.5 | 182.4–370.6 | ||
| Middle | 89.2 | 79.1–99.4 | 525.6 | 414.8–636.5 | ||
| Richest | 80.8 | 70.1–90.9 | 511.9 | 322.3–418.0 | ||
Abbreviation: HTG, Haitian Goude.
p value was calculated through Kaplan–Meier log‐rank test.
In regard to dog ownership (Table 4), individuals who reported having only one dog were willing to pay more for dog vaccination than individuals who had 2 or more dogs in their households. The presence of female dogs only was significantly related to a higher payment for vaccination and a higher distance to fixed‐point campaigns. In general, owning a free‐roaming dog, having affection for one's dog, owning a dog for security or companionship purposes, and dogs not considered to be part of family were all associated with a higher willingness to pay and walk for vaccination.
3.4. Factors linked to maximum WTP for dog rabies vaccination and maximum wtw to fixed‐point vaccination campaigns
Variables independently associated with maximum WTP for dog rabies vaccination in logistic regression were location, income, confinement status and reason for ownership (Table 5). Individuals more likely to pay for dog rabies vaccination were those owning a free‐roaming dog, for companionship purpose and not able to walk the owned dog on a leash.
TABLE 5.
Characteristics associated with willingness to pay for canine rabies vaccine in logistic regression in Haiti, 2017
| Variables | Median WTP (HTG) a | Odds Ratio (90% CI) | p value |
|---|---|---|---|
| Confinement (ref. Always confined = 31.6) | |||
| Sometimes free | 68.4 | 0.8 (0.3–2.2) | .8 |
| Always free | 65.6 | 2.6 (1.0–6.6) | .09 |
| Primary purpose (ref. Companionship = 123.6) | |||
| Security | 54.7 | 6.1 (3.6–10.4) | <.0001 |
| Wealth | 74.1 | 9.9 (1.7–58.1) | .03 |
| Can walk dogs on a leash (ref. No = 72.7) | |||
| Yes | 60.0 | 2.3 (1.5–3.4) | .0005 |
Number of individuals willing to pay 200 HTG ($ 2.93) to achieve 70% of vaccination coverage.
Additionally, variables independently associated with maximum WTW to fixed‐point vaccination campaigns were location, income and primary purpose (Table 6). Individuals more likely to walk to fixed‐point vaccination campaigns were those from Gonaives and Saint Marc in Artibonite Department, living with a middle or higher income, and owning a dog for security purpose (Figure 4).
TABLE 6.
Characteristics associated with willingness to walk for canine rabies vaccination campaigns by logistic regression model in Haiti, 2017
| Variables | Median WTW (m) a | Odds Ratio (90% CI) | p value |
|---|---|---|---|
| Location (ref. North others = 80.1) | |||
| North Cap Haitien | 94.7 | 0.7 (0.2–2.5) | .7 |
| 598.4 | 19.3 (8.7–42.7) | <.0001 | |
| Saint Marc | 937.0 | 67.0 (29.0–155.0) | <.0001 |
| Income (ref. Poor = 270.3) | |||
| Lower | 341.3 | 2.2 (0.9–4.7) | .1 |
| Middle | 423.5 | 4.6 (2.7–8.3) | <.0001 |
| Richest | 411.2 | 4.1 (2.3–8.3) | .0002 |
| Primary purpose (ref. Companionship = 281.8) | |||
| Security | 311.9 | 2.5 (1.1–5.4) | .06 |
| Wealth | 95.8 | 0.1 (0.01–1.0) | .9 |
Number of individuals willing to walk 1,000 m or higher to achieve 70% of vaccination coverage.
FIGURE 4.
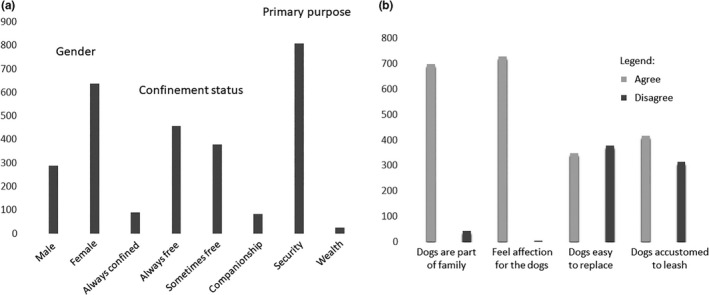
Demographics of owned dogs in community members from North and Artibonite Departments, Haiti, 2017
3.5. Reasons do not attend canine rabies vaccination campaign
Among the 175 dog owners that did not attend the canine rabies vaccination campaign (those owners that, for any reason, were not able to bring one or more of their dogs to the fixed point for vaccination), most (46.3%) stated that they were unaware of the campaign before it occurred as their primary reason for non‐vaccination (Table 7). Thirty‐four individuals (19.4%) reported they were unavailable during the campaign, and 21 individuals (12.0%) reported they already had vaccinated their dogs. Seven individuals (4.0%) mentioned that they did not find their dogs during the time of the campaign, whereas five individuals (2.9%) mentioned that the vaccination point was too far, and eight individuals (4.6%) mentioned that is not important to vaccinate their dogs. Additionally, two (1.1%) individuals reported it was difficult to transport their dogs to the vaccination point that their dogs were too young to be vaccinated, and they do not trust in the vaccine. The risk of dogs fighting and a long line at the vaccination point were not reported as reasons do not attend a canine rabies vaccination campaign.
TABLE 7.
Reported reasons do not vaccinate owned dogs according to 175 surveyed households that did not attend canine rabies vaccination campaign in North and Artibonite Departments, Haiti, 2017
| Main reasons reported | Agree | Disagree |
|---|---|---|
| Unaware | 81 (46.3%) | 94 (54.7%) |
| Unavailable | 34 (19.4%) | 141 (80.6%) |
| Already vaccinated my dog | 21 (12.0%) | 154 (88.0%) |
| Do not believe vaccine is important | 8 (4.6%) | 167 (97.1%) |
| Dog not found | 7 (4.0%) | 168 (96.0%) |
| Vaccination point too far | 5 (2.9%) | 170 (97.1%) |
| Transport the dog is difficult | 2 (1.1%) | 173 (98.9%) |
| Dog too young | 2 (1.1%) | 173 (98.9%) |
| Do not trust vaccine | 2 (1.1%) | 173 (98.9%) |
| Long line at the vaccination point | 0 | 173 (100.0%) |
| Risk of dog fight at the vaccination point | 0 | 173 (100.0%) |
4. DISCUSSION
Human rabies transmitted by dogs poses a heavy burden on the most disadvantaged populations in the world (Fooks et al., 2014; Hampson et al., 2015; Wallace, Undurraga, et al., 2017). Although dog and human rabies have decreased significantly in Latin American countries in the last several decades, Haiti is one of the few countries that continue to report high rates of dog‐mediated human rabies deaths (Tran et al., 2018). In average, four canine and seven human rabies cases have been reported by Haiti's national surveillance system; however, the burden of rabies still remains underestimate (Hampson et al., 2015; Wallace et al., 2015). The lack of healthcare‐seeking behaviours among persons bitten by dogs, inadequate access to post‐exposure prophylaxis, limited knowledge about this disease among healthcare professionals and community members, and low attendance to vaccination campaigns are some key barriers/factors to rabies elimination and control (Etheart et al., 2017; Osinubi et al., 2018; Wallace et al., 2015, 2016).
In the present study, we elucidated the maximum amount residents of North and Artibonite Departments, Haiti were willing to pay or walk for dog rabies vaccination at fixed‐point vaccination campaigns. Vaccination campaigns targeting 70%–80% of the dog population is an effective measure to eliminate canine rabies (Cleaveland & Hampson, 2017; Wallace, Undurraga, et al., 2017). Our findings give policymakers some useful information on how much residents may be willing to contribute financially and socially towards dog vaccination in Haiti and other communities with similar attitudes towards dogs and vaccination practices. Although cost and distance to attend fixed‐point vaccination campaigns were not noted as prominent causes for non‐participation, to achieve at least 70% vaccination coverage, our results suggest that the cost of the vaccine should not exceed 16 HTG (0.25 US Dollars), and vaccinators must come within 75 m of a dog owner's home to achieve maximum vaccination coverages. The values found in this study were much lower than what was found in previous studies in other countries using a similar approach (Birhane et al., 2016; Dürr, Meltzer, Mindekem, & Zinsstag, 2008; Durr et al., 2009; Fitzpatrick et al., 2014; Kadowaki et al., 2018). This is likely a reflection of the high rates of poverty in Haiti combined with the propensity for owners to allow dogs to roam freely and lack of familiarity with leash walking. These barriers are also noted in many other canine rabies‐endemic countries with large free‐roaming dog populations (Castillo‐Neyra et al., 2017; Dürr et al., 2008; Durr et al., 2009; Kadowaki et al., 2018).
The median stated maximum WTP for vaccination (0.95 USD) was found to be lower than the overall estimated per dog vaccination cost for most Asian, African and Latin American countries (1.55 USD) (Anderson & Shwiff, 2015). In comparison with specific rabies‐endemic countries, the average WTP in Haiti was found to be lower than the estimated per dog vaccination cost in Tanzania (1.73 USD–5.55 USD), N'Djamena and Chad (2.90–3.80 USD), but higher to that reported in Thailand (0.52 USD) (Durr et al., 2009; Fitzpatrick et al., 2014; Léchenne et al., 2016). That the average WTP is low, adds evidence to findings presented via other publications on canine rabies‐endemic countries that suggest rabies elimination through mass vaccination of dogs could be optimally addressed as a government responsibility, funded by health authorities for the public good (Borse et al., 2018; Durr et al., 2009; Kazadi, Tshilenge, Mbao, Njoumemi, & Masumu, 2017; Léchenne et al., 2016). The value of vaccination does not appear to be lost on dog owners, as 99% of respondents would be willing to pay for vaccination and the median value willing to pay for vaccination, as a function of per capita monthly GDP, was twice that of a study from the Philippines (1.5% versus 0.8%, respectively) (Birhane et al., 2016). However, the value that 70% of those surveyed would be willing to pay (0.25 USD) accounts for only about 12% of the average cost to vaccinate a dog. Given these findings, charging dog owners during vaccination campaigns should be approached cautiously as minimal charges are unlikely to offset the cost of vaccination programmes, but may have significant impacts probably resulting on much lower dog vaccination coverage rates than the recommended ≥70%. However, a 'pay as you can' scheme may show promise, and the funds could be used to support additional rabies control efforts that often go unfunded, such as education, surveillance and post‐exposure prophylaxis funds (Castillo‐Neyra et al., 2017; Dürr et al., 2008; Durr et al., 2009; Jibat, Hogeveen, & Mourits, 2015; Kazadi et al., 2017).
The fixed‐point vaccination method has been shown to be successful in many high‐ and middle‐income countries, where leash laws and dog‐ownership practices favour responsibly owned pets that can be walked by leash and receive routine veterinary care (Balogh, Wandeler, & Meslin, 1993; Kayali et al., 2003; Léchenne et al., 2016; Taylor et al., 2017). Fixed‐point vaccination campaigns are less labour‐intensive compared to door‐to‐door and capture–vaccinate–release methods. These latter methods require highly skilled animal health professionals who can traverse through a community, often on foot, and restrain dogs long enough to apply vaccination (Gibson et al., 2019). As a result, fixed‐point vaccination is often a less costly method, although post‐vaccination coverages may not be adequate when this method is applied to certain dog populations. Results of this study do show that a sizeable proportion of dogs should be reachable by a fixed‐point campaign, with over half of dog owners reporting that they can walk their dogs by leash and a median distance willing to walk of 370 m. However, these results show that there are major barriers to reaching >70% vaccination coverage utilizing the fixed‐point method alone. A large proportion of dog owners cannot walk their dogs by leash, meaning that vaccinators will need to utilize DD or CVR methods to reach them. Furthermore, the distance at least 70% of dog owners were willing to walk was only 75 m, which would be the equivalent of having a fixed‐point vaccination centre on every city block throughout Haiti; clearly, this is an unreasonable expectation for any national vaccination strategy. While unowned and community owned dogs are not thought to represent a large proportion of the dog population in Haiti, they are present and they would not be reached through fixed‐point vaccination campaigns, thereby further diluting the vaccination coverage if only this method was utilized.
Perceptions towards dogs were highly favourable among the surveyed population in this study. Nearly all dog owners considered dogs to be an affectionate member of their family. Yet, despite dog owner's fond feelings for their companions, vaccination rates have historically been well under required levels for elimination of rabies. This indicates that other barriers could be at play. Among the variables assessed in this study, it would appear that dog owners with a high propensity to allow their dogs to roam freely and lack of ability to walk them by leash negatively impact vaccination rates. Dog owners were not willing to pay a large amount for vaccination, but campaigns in Haiti are government sponsored and free to owners, so this is unlikely to be a barrier under the current vaccination programme.
A large proportion of dogs were owned for security, yet more favourable WTP and WTW results were reported for dogs owned for companionship. This may indicate that programmes that transition the perception of dogs from security to companions may also improve attendance at rabies vaccination campaigns. Another approach may be to pursue educational campaigns that focus on the importance of rabies vaccination to keep dogs healthy so they can continue to serve as good protectors of the owner's domicile.
The results of this study show that fixed‐point vaccination methods should be a component of Haiti's vaccination campaign, but to achieve adequate herd immunity for rabies elimination additional considerations must be made. Societal changes to improve the value of dogs and dog vaccination could improve attendance, but these types of changes can take many years to develop and are often associated with improvements in the economic health of a society (Arias‐Orozco et al., 2018; Bardosh, 2018). Animal welfare changes, such as training dog owners to walk dogs on leashes or implementing laws to require dogs to remain leashed, could improve the effectiveness of fixed‐point vaccination methods. However, in countries with limited infrastructure and limited ability to enforce legislation, these changes are unlikely to occur without larger societal and economic windfalls. The results from this study suggest that the most feasible and timely solution to eliminate rabies in Haiti would be to adopt a mixed‐methods vaccination approach, which includes fixed‐point campaigns in combination with methods that target free‐roaming dogs (i.e. CVR) and dogs whose owners do not feel they can bring their dog to a clinic (i.e. DD). A mixed‐methods approach was conducted in Haiti in 2018, and vaccination coverages were found to be approximately 75%, further supporting the findings from this study (Monroe et al., under review).
We also identified specific reasons for not attending canine rabies vaccination campaigns. The campaign conducted in 2017 was primarily door‐to‐door vaccination. While WTW was low among the respondents in this study, walking the dog on leash and distance to the vaccination centre were rarely listed as barriers during this 2017 campaign. These findings likely support the WTW findings that barriers such as leash walking and distance can be overcome through adjusting vaccination campaign strategies to more active methods (DD and CVR). Addressing these reasons is also important to implement solutions that aim to improve campaign effectiveness. In this study, most of surveyed individuals were unaware of the vaccination campaign. This finding corroborates previous studies that showed the lack of awareness as a reason for low participation in canines rabies vaccination campaigns (Arias‐Orozco et al., 2018; Bardosh, 2018; Birhane et al., 2016; Castillo‐Neyra et al., 2017; Cleaton et al., 2018; Kazadi et al., 2017; Lembo et al., 2010). Indeed, better education is needed on how vaccination should be conducted every year, highlighting the importance of implementing educational programmes in vulnerable populations to increase rabies awareness and facilitate control interventions.
As reported by Cleaton et al, during a canine vaccination campaign in Haiti, a combination of communication methods of awareness is needed to increase population awareness and consequently improve the vaccination campaign to achieve a >70% coverage (Cleaton et al., 2018). Furthermore, implementing educational measures could also be helpful to reduce other barriers related to poor knowledge regarding rabies risks, increasing control interventions (Castillo‐Neyra et al., 2017; Osinubi et al., 2018). Additionally, a combination of vaccination strategies such as fixed point supplemented by door‐to‐door methodology could increase the attendance to vaccination campaigns (Gibson et al., 2016; Taylor et al., 2017), therefore reducing barriers related to location, and dog owners not accustomed to using leashes. The use of collars and leashes could also be implemented to reduce the barrier of owners not using leashes.
5. CONCLUSION
In conclusion, our findings provide useful information regarding attendance at canine rabies vaccination campaigns in Haiti, which could be applied to national rabies prevention campaigns. This study could help to assist public health authorities to better understand that variables are the most important ones and what proportion of the people could potentially intend to vaccinate their dogs in order to achieve a successful vaccination campaign. The lack of familiarity with leashes and propensity for dogs to roam freely are barriers to successful fixed‐point vaccination methods in Haiti and alternative methods such as door‐to‐door, capture–vaccinate–release or oral vaccination should be explored. There may be some prospect for fee‐for‐service vaccination in Haiti; however, additional methods could be adopted to supplement free canine rabies vaccination campaigns instead of replace it in order to maintain high coverage rates.
CONFLICTS OF INTEREST
None.
ETHICAL APPROVAL
The study was approved by the Centers for Disease Control and Prevention's Human Research Office (NCEZID tracking number 051517BM). As this activity is to evaluate the implementation of a public health intervention (mass dog vaccination), it is consistent with non‐research public health programme evaluation per CDC guidance. A voluntary fingerprint or signed informed consent was obtained from each participant prior to beginning the interview. An informed consent about the risks of participation in the study was also provided.
DISCLAIMER
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Supporting information
Barbosa Costa G, Ludder F, Monroe B, et al. Barriers to attendance of canine rabies vaccination campaigns in Haiti, 2017. Transbound Emerg Dis. 2020;67:2679–2691. 10.1111/tbed.13622
This article has been contributed to by US Government employees and their work is in the public domain in the USA.
Funding information
The authors received no specific funding for this work. Activities were funded by the U.S. Government.
DATA AVAILABILITY STATEMENT
These data were collected on behalf of the U.S. federal agency, the Centers for Disease Control, and as such the authors are not permitted to make the data set publicly available. Requests for data may be sent to Rabies@cdc.gov.
REFERENCES
- Anderson, A. , & Shwiff, S. A. (2015). The cost of canine rabies on four continents. Transboundary and Emerging Diseases, 62, 446–452. 10.1111/tbed.12168 [DOI] [PubMed] [Google Scholar]
- Arias‐Orozco, P. , Bástida‐González, F. , Cruz, L. , Villatoro, J. , Espinoza, E. , Zárate‐Segura, P. B. , & Recuenco, S. (2018). Spatiotemporal analysis of canine rabies in El Salvador: Violence and poverty as social factors of canine rabies. PLoS One, 13, e0201305 10.1371/journal.pone.0201305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balen, J. , McManus, D. P. , Li, Y.‐S. , Zhao, Z.‐Y. , Yuan, L.‐P. , Utzinger, J. , … Raso, G. (2010). Comparison of two approaches for measuring household wealth via an asset‐based index in rural and peri‐urban settings of Hunan province, China. Emerging Themes in Epidemiology, 7, 7 10.1186/1742-7622-7-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bardosh, K. L. (2018). Towards a science of global health delivery: A socio‐anthropological framework to improve the effectiveness of neglected tropical disease interventions. PLoS Neglected Tropical Diseases, 12, e0006537 10.1371/journal.pntd.0006537 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birhane, M. G. , Miranda, M. E. G. , Dyer, J. L. , Blanton, J. D. , & Recuenco, S. (2016). Willingness to pay for dog rabies vaccine and registration in Ilocos Norte, Philippines (2012). PLoS Neglected Tropical Diseases, 10, e0004486 10.1371/journal.pntd.0004486 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borse, R. H. , Atkins, C. Y. , Gambhir, M. , Undurraga, E. A. , Blanton, J. D. , Kahn, E. B. , … Meltzer, M. I. (2018). Cost‐effectiveness of dog rabies vaccination programs in East Africa. PLoS Neglected Tropical Diseases, 12, e0006490 10.1371/journal.pntd.0006490 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castillo‐Neyra, R. , Brown, J. , Borrini, K. , Arevalo, C. , Levy, M. Z. , Buttenheim, A. , … Paz‐Soldan, V. A. (2017). Barriers to dog rabies vaccination during an urban rabies outbreak: Qualitative findings from Arequipa, Peru. PLOS Neglected Tropical Diseases, 11, e0005460 10.1371/journal.pntd.0005460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cleaton, J. M. , Wallace, R. M. , Crowdis, K. , Gibson, A. , Monroe, B. , Ludder, F. , … King, A. (2018). Impact of community‐delivered SMS alerts on dog‐owner participation during a mass rabies vaccination campaign, Haiti 2017. Vaccine, 36, 2321–2325. 10.1016/j.vaccine.2018.03.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cleaveland, S. , & Hampson, K. (2017). Rabies elimination research: Juxtaposing optimism, pragmatism and realism. Proceedings of the Royal Society of London. Series B, Biological Sciences, 284, 20171880 10.1098/rspb.2017.1880 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Balogh, K. K. , Wandeler, A. , & Meslin, F. (1993). A dog ecology study in an urban and a semi‐rural area of Zambia. Onderstepoort Journal of Veterinary Research, 60, 437–443. [PubMed] [Google Scholar]
- Dong, H. , Kouyate, B. , Cairns, J. , & Sauerborn, R. (2003). A comparison of the reliability of the take‐it‐or‐leave‐it and the bidding game approaches to estimating willingness‐to‐pay in a rural population in West Africa. Social Science and Medicine, 56, 2181–2189. 10.1016/S0277-9536(02)00234-4 [DOI] [PubMed] [Google Scholar]
- Dürr, S. , Meltzer, M. I. , Mindekem, R. , & Zinsstag, J. (2008). Owner valuation of rabies vaccination of dogs, Chad. Emerging Infectious Diseases, 14, 1650–1652. 10.3201/eid1410.071490 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durr, S. , Mindekem, R. , Kaninga, Y. , Doumagoum moto, D. , Meltzer, M. I. , Vounatsou, P. , & Zinsstag, J. (2009). Effectiveness of dog rabies vaccination programmes: Comparison of owner‐charged and free vaccination campaigns. Epidemiology and Infection, 137, 1558–1567. 10.1017/S0950268809002386 [DOI] [PubMed] [Google Scholar]
- Etheart, M. D. , Kligerman, M. , Augustin, P. D. , Blanton, J. D. , Monroe, B. , Fleurinord, L. , … Wallace, R. M. (2017). Effect of counselling on health‐care‐seeking behaviours and rabies vaccination adherence after dog bites in Haiti, 2014–15: A retrospective follow‐up survey. Lancet Global Health, 5, e1017–e1025. 10.1016/S2214-109X(17)30321-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher, C. R. , Streicker, D. G. , & Schnell, M. J. (2018). The spread and evolution of rabies virus: Conquering new frontiers. Nature Reviews Microbiology, 16, 241–255. 10.1038/nrmicro.2018.11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzpatrick, M. C. , Hampson, K. , Cleaveland, S. , Mzimbiri, I. , Lankester, F. , Lembo, T. , … Galvani, A. P. (2014). Cost‐effectiveness of canine vaccination to prevent human rabies in rural Tanzania. Annals of Internal Medicine, 160, 91–100. 10.7326/M13-0542 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fooks, A. R. , Banyard, A. C. , Horton, D. L. , Johnson, N. , McElhinney, L. M. , & Jackson, A. C. (2014). Current status of rabies and prospects for elimination. Lancet, 384, 1389–1399. 10.1016/S0140-6736(13)62707-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freire de Carvalho, M. , Vigilato, M. A. N. , Pompei, J. A. , Rocha, F. , Vokaty, A. , Molina‐Flores, B. , … Del Rio Vilas, V. J. (2018). Rabies in the Americas: 1998–2014. PLoS Neglected Tropical Diseases, 12(3), 1998–2014. 10.1371/journal.pntd.0006271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson, A. D. , Handel, I. G. , Shervell, K. , Roux, T. , Mayer, D. , Muyila, S. , … Gamble, L. (2016). The vaccination of 35,000 dogs in 20 working days using combined static point and door‐to‐door methods in Blantyre, Malawi. PLOS Neglected Tropical Diseases, 10, e0004824 10.1371/journal.pntd.0004824 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson, A. D. , Yale, G. , Vos, A. , Corfmat, J. , Airikkala‐Otter, I. , King, A. , … Mazeri, S. (2019). Oral bait handout as a method to access roaming dogs for rabies vaccination in Goa, India: A proof of principle study. Vaccine, 1, 100015 10.1016/j.jvacx.2019.100015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hampson, K. , Coudeville, L. , Lembo, T. , Sambo, M. , Kieffer, A. , Attlan, M. , … Global Alliance for Rabies Control Partners for Rabies Prevention (2015). Estimating the global burden of endemic canine rabies. PLoS Neglected Tropical Diseases, 9, e0003709 10.1371/journal.pntd.0003709 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howe, L. D. , Galobardes, B. , Matijasevich, A. , Gordon, D. , Johnston, D. , Onwujekwe, O. , … Hargreaves, J. R. (2012). Measuring socio‐economic position for epidemiological studies in low‐ and middle‐income countries: A method of measurement in epidemiology paper. International Journal of Epidemiology, 41, 871–886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jibat, T. , Hogeveen, H. , & Mourits, M. C. M. (2015). Review on Dog Rabies Vaccination Coverage in Africa: A Question of Dog Accessibility or Cost Recovery? PLoS Neglected Tropical Diseases, 9, e0003447 10.1371/journal.pntd.0003447 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kadowaki, H. , Duc, P. P. , Sato, K. , Phuong, P. T. M. , Hagiwara, K. , & Makita, K. (2018). Socio‐economic factors associated with voluntary rabies control measures in Vietnam. Preventive Veterinary Medicine, 157, 105–114. 10.1016/j.prevetmed.2018.06.006 [DOI] [PubMed] [Google Scholar]
- Kayali, U. , Mindekem, R. , Yemadji, N. , Oussiguéré, A. , Naïssengar, S. , Ndoutamia, A. G. , & Zinsstag, J. (2003). Incidence of canine rabies in N'Djamena, Chad. Preventive Veterinary Medicine, 61, 227–233. [DOI] [PubMed] [Google Scholar]
- Kazadi, E. K. , Tshilenge, G. M. , Mbao, V. , Njoumemi, Z. , & Masumu, J. (2017). Determinants of dog owner‐charged rabies vaccination in Kinshasa, Democratic Republic of Congo. PLoS One, 12, e0186677 10.1371/journal.pone.0186677 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Léchenne, M. , Oussiguere, A. , Naissengar, K. , Mindekem, R. , Mosimann, L. , Rives, G. , … Zisstag, J. (2016). Operational performance and analysis of two rabies vaccination campaigns in N'Djamena, Chad. Vaccine, 34, 571–577. 10.1016/j.vaccine.2015.11.033 [DOI] [PubMed] [Google Scholar]
- Lembo, T. , Hampson, K. , Kaare, M. T. , Ernest, E. , Knobel, D. , Kazwala, R. R. , … Cleaveland, S. (2010). The feasibility of canine rabies elimination in Africa: Dispelling doubts with data. PLoS Neglected Tropical Diseases, 4, e626 10.1371/journal.pntd.0000626 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Osinubi, M. O. V. , Fenelon, N. , Dyer, J. L. , Franka, R. , Etheart, M. , Ali, A. , … Johnson, V. R. (2018). Meeting the urgent need for rabies education in Haiti. Zoonoses Public Health, 65, 662–668. 10.1111/zph.12474 [DOI] [PubMed] [Google Scholar]
- Taylor, L. H. , Wallace, R. M. , Balaram, D. , Lindenmayer, J. M. , Eckery, D. C. , Mutonono‐Watkiss, B. , … Nel, L. H. (2017). The role of dog population management in rabies elimination: A review of current approaches and future opportunities. Frontiers in Veterinary Science, 4, 109 10.3389/fvets.2017.00109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tran, C. H. , Etheart, M. D. , Andrecy, L. L. , Augustin, P. D. , Kligerman, M. , Crowdis, K. , … Wallace, R. M. (2018). Investigation of canine‐mediated human rabies death, Haiti, 2015. Emerging Infectious Diseases, 24, 156–158. 10.3201/eid2401.161555 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace, R. M. , Etheart, M. D. , Doty, J. , Monroe, B. , Crowdis, K. , Augustin, P. D. , … Fenelon, N. (2016). Dog‐mediated human rabies death, Haiti, 2016. Emerging Infectious Diseases, 22, 1963–1965. 10.3201/eid2211.160826 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace, R. , Etheart, M. , Ludder, F. , Augustin, P. , Fenelon, N. , Franka, R. , … Millien, M. (2017). The health impact of rabies in Haiti and recent developments on the path toward elimination, 2010–2015. American Journal of Tropical Medicine and Hygiene, 97, 76–83. 10.4269/ajtmh.16-0647 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace, R. M. , Reses, H. , Franka, R. , Dilius, P. , Fenelon, N. , Orciari, L. , … Millien, M. (2015). Establishment of a canine rabies burden in Haiti through the Implementation of a Novel Surveillance Program. PLoS Neglected Tropical Diseases, 9, e0004245 10.1371/journal.pntd.0004245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace, R. M. , Undurraga, E. A. , Blanton, J. D. , Cleaton, J. , & Franka, R. (2017). Elimination of dog‐mediated human rabies deaths by 2030: Needs assessment and alternatives for progress based on dog vaccination. Frontiers in Veterinary Science, 4, 9 10.3389/fvets.2017.00009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watanabe, M. (2010). Nonparametric estimation of mean willingness to pay from discrete response valuation data. American Journal of Agricultural Economics, 92, 1114–1135. 10.1093/ajae/aaq034 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
These data were collected on behalf of the U.S. federal agency, the Centers for Disease Control, and as such the authors are not permitted to make the data set publicly available. Requests for data may be sent to Rabies@cdc.gov.