

Abstract
Objective
To examine the correlation between smoking habit and lower urinary tract symptoms in women.
Methods
We first screened 10 000 female patients to examine their smoking habit. A total of 7004 samples were successfully collected for further analysis through a urinary continence survey. The ratio of current smoking to non‐smoking participants was set as 1:3 to allow thorough assessment of the impact of cigarette smoking on lower urinary tract symptoms.
Results
A total of 4756 complete responses were obtained for the Overactive Bladder Symptom Score and International Consultation on Incontinence Questionnaire‐Short Form questionnaire. The current smokers (2.54 ± 2.91, 2.48 ± 4.01) and ex‐smokers (2.27 ± 2.50, 2.25 ± 3.50) showed significantly higher Overactive Bladder Symptom Score and International Consultation on Incontinence Questionnaire‐Short Form scores than the non‐smokers (1.70 ± 2.05, 1.49 ± 2.73) (P < 0.0001, P < 0.0001 and P < 0.0001, P < 0.0001, respectively). The prevalence of urgency was affected by the smoking status. Younger participants (aged 20–39 years) showed a stronger influence of their smoking habit than older participants (aged ≥40 years). Urgency urinary incontinence was also affected by the smoking status.
Conclusions
The prevalence of urgency and urgency urinary incontinence is correlated with age and smoking habit, and both current and ex‐smokers show an increased prevalence of urgency and urgency urinary incontinence compared with non‐smokers, especially younger women.
Keywords: continence, lower urinary tract symptoms, overactive bladder, smoking, urgent urinary incontinence
Abbreviations & Acronyms
- ICIQ‐SF
International Consultation on Incontinence Questionnaire‐Short Form
- IRB
Institutional Review Board
- LUTS
lower urinary tract symptoms
- MUI
mixed urinary incontinence
- OAB
overactive bladder
- OABSS
Overactive Bladder Symptom Score
- PMD
post‐micturition dribble
- SUI
stress urinary incontinence
- UUI
urgency urinary incontinence
Introduction
OAB is defined as a symptom syndrome characterized by urgency, with or without urgency incontinence, usually with frequency and nocturia in the absence of confirmed infection or any other obvious pathology. 1 Some epidemiological studies have shown that LUTS, including OAB, occur commonly in both men and women, with an age‐related increase. 2 The prevalence of OAB is diversely reported depending on the characteristics of the patient group, such as the age, ethnicity and socioeconomic status, and range from as low as 2% to as high as 53%. 3 , 4 , 5 In Asian countries, 19.3% of Korean women according to Chae et al., and 11% of Japanese women aged >40 years according to Homma et al. have OAB. 6 However, most epidemiological studies have shown the prevalence of OAB to be correlated with age. 6 , 7
Previous studies have reported that LUTS, including OAB, is multifactorial in both men and women. 8 , 9 , 10 However, animal studies have shown that atherosclerosis causes chronic bladder ischemia, resulting in ischemia‐related bladder disfunction. 11 , 12 Smoking is a major risk factor of atherosclerosis, and previous reports have shown that smoking influenced LUTS in patients who underwent urodynamic testing and female participants aged approximately 68 years in a British birth cohort study. 13 , 14 Although the detailed mechanism underlying the association between cigarette smoking and LUTS is still unknown, smoking is thought to be associated with functional abnormalities of LUTS. 15 , 16 , 17
The present study examined the correlation between a smoking habit and LUTS in a population‐based study using a web‐based questionnaire.
Methods
Screening survey to select smoking habit
We first screened a total of 10 000 female monitors registered by a web‐based internet survey company (Freeasy; iBRIDGE Company, Tokyo, Japan) to determine their smoking habit. All monitors approved the web‐based survey at the time of the answering questionnaire and IRB of Yokohama City University Medical Center (Yokohama, Japan) approved this study (IRB No. B200300007).
We set the number of female participants based on the population‐based age distribution by government release. 18 The survey asked monitors about their smoking habit, which consisted of three categories: (i) non‐smokers; (ii) ex‐smokers; and (iii) current smokers. For ex‐smokers, an additional question of “When did you stop smoking?” was posed, and for current smokers, additional questions of “How many cigarettes do you smoke per day?” and “When did you start smoking?” were posed. A total of 7004 participants were collected. Among these participants, the responses of 3698 participants of aged 20–59 years were successfully collected, whereas 750 of the responses of 1831 (41.0%) participants in the 60–69 years age group and 308 of the responses of 1475 (20.9%) participants in the ≥70 years age group were not collected; hence, the numbers of elderly participants in the web‐based questionnaire monitoring lists were small (Fig. 1). The monitor registration information also included the age, marital status, child, household income, working status and prefecture of residence.
Fig. 1.
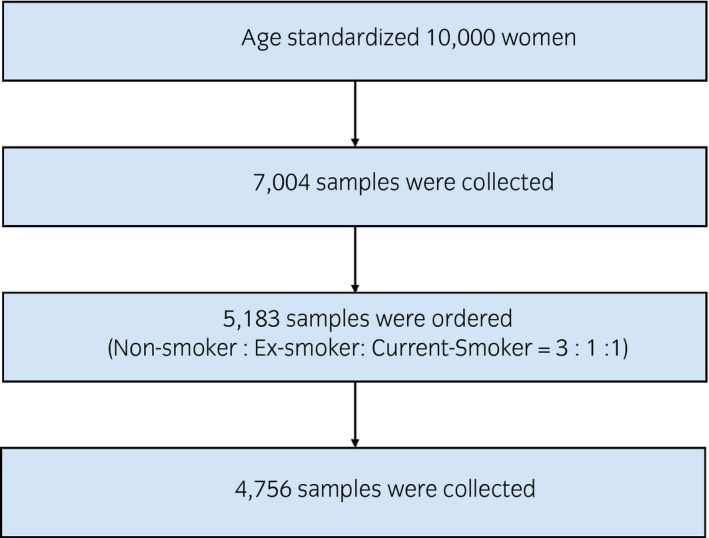
Study design and number of participants.
Continence survey
To examine the impact of cigarette smoking, we set the ratio of current smoking to non‐smoking participants number as 1:3. The number of ex‐smoker participants was almost the same as the number of current smokers, so the final ratio of non‐smokers, ex‐smokers and current smokers was 3:1:1. The non‐smokers were randomly selected based on their initial smoking status. The numbers of participants aged ≥60 years could not be obtained by population‐based calculations. We therefore set the number of participants ≥60 years at the maximum number. We asked a total of 5183 participants to respond to the LUTS questionnaire, and 4756 (91.8%) responded with a submission (Fig. 1).
Questionnaire
We assessed LUTS using the Japanese version of the validated OABSS and ICIQ‐SF. 19 , 20 The OABSS, originally developed in Japan, is a four‐item questionnaire that expresses OAB symptoms on a single scale. 19 The OABSS question items address individual symptoms as follows: daytime frequency, nocturia, urgency and urgency incontinence. Gotoh et al. reported that the OABSS was useful for assessing the effects of treatment on OAB symptoms and was responsive to treatment‐related changes. 21 The OABSS score was defined as the sum of the total OABSS scores. OAB was defined as the presence of both a total score of ≥3 and an OABSS Q3 score of ≥2. UUI was defined as an OABSS Q4 of ≥1. Daytime frequency and nocturia were defined as OABSS Q1 of ≥1 and Q2 of ≥2, respectively.
The ICIQ‐SF was developed to screen for incontinence, and to obtain a brief yet comprehensive summary of the level, impact and perceived causes of symptoms of incontinence, and facilitate patient–clinician discussions. 20 The ICIQ‐SF score was calculated as the sum of Q1, Q2 and Q3 scores. UUI (ICIQ‐SF definition) was defined in participants with a positive response for ICIQ‐SF “leaks occur before you can get to the toilet.” SUI was defined in participants with a positive response to at least one of the following: “leaks occur when you cough or sneeze” and “leaks occur when you are physically active/exercising.” MUI was defined as both UUI (ICIQ‐SF definition) and SUI. PMD was defined as a positive response to “leaks occur when you have finished urinating and are dressed.”
Statistical analysis
The participants’ characteristics and scores were analyzed by the Mann–Whitney U‐test and one‐factor analysis of variance (anova) tests, and the prevalence of daytime frequency, nocturia, urgency, UUI, SUI, MUI and PMD was analyzed by a χ2‐test using the GraphPad Prism software program (GraphPad Software, La Jolla, CA, USA). P‐values of <0.05 were considered to show statistical significance.
Results
We first screened 10 000 women with an age‐adjusted population, and 7004 shared their smoking status. At this screening, 4988 (71.2%) were non‐smokers, 1007 (14.3%) were ex‐smokers and 1009 (14.4%) were current smokers (Fig. 2a,b). We asked a total of 5183 participants to respond to the continence survey, and 4756 (91.8%) participants ultimately did so, including 2828 (59.5%) non‐smokers, 990 (19.7%) ex‐smokers and 938 (19.7%) current smokers (Fig. 2c). The prefecture of residence is shown in Table S1 and Figure S1. Participants’ background characteristics, including age, marital status, children, household income, working status and prefecture of residence, are listed in Table 1. A positive correlation was noted between the OABSS score and ICIQ‐SF score (r 2 = 0.551, P < 0.0001; Fig. S2).
Fig. 2.
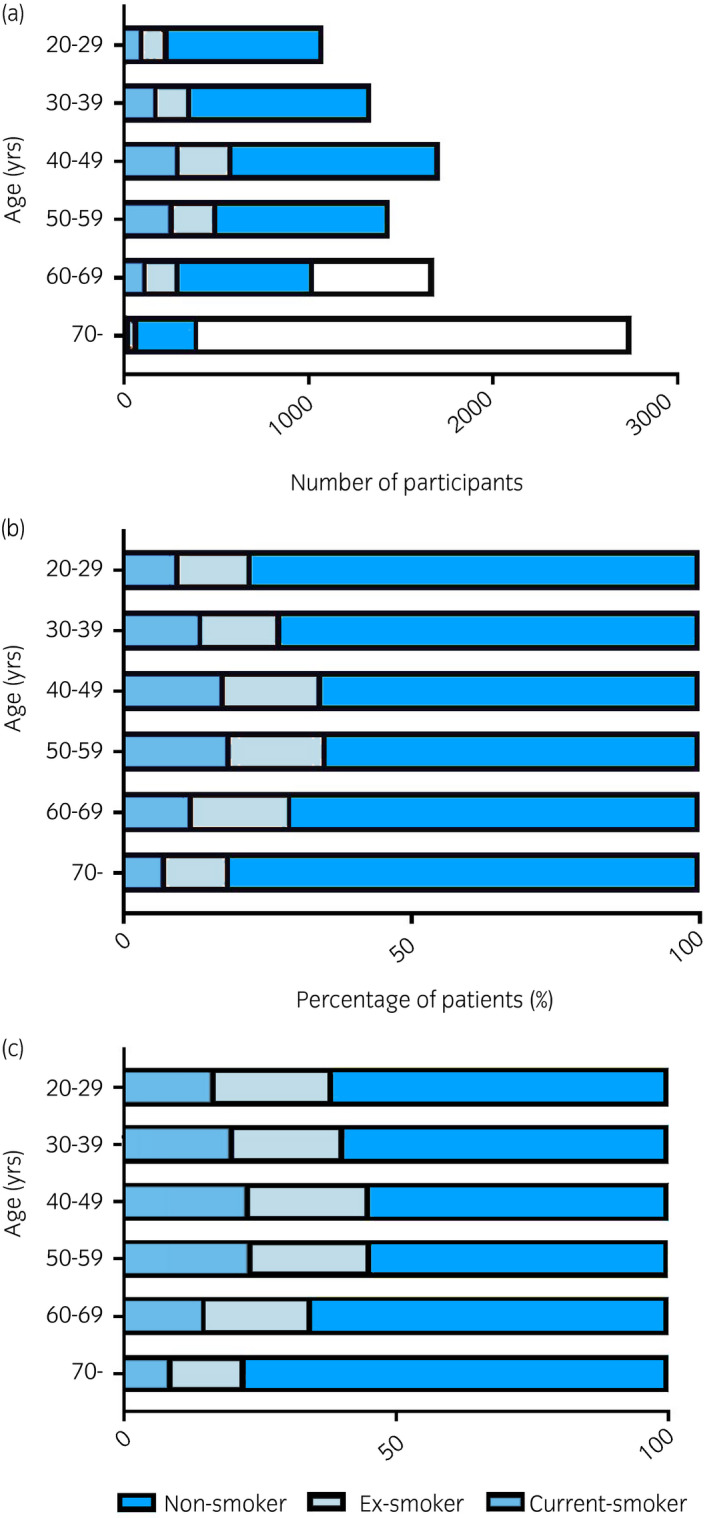
(a) Number of target screening participants. The white bars in the 60–69 years and ≥70 years age groups show the difference between the ideal number of participants based on the same age group in the Japanese population and the number of participants in this study. (b) Ratio of smoking habit. (c) Final ratio of participants.
Table 1.
Participants’ background characteristics
| Variables | Non‐smoker | Ex‐smoker | Current smoker | P‐value (vs non‐smoker) |
|---|---|---|---|---|
| No. patients | 2828 | 990 | 938 | |
| Age (years) | 48 (48.3 ± 14.5) | 47 (46.9 ± 13.3) | 47 (46.5 ± 12.1) | 0.005, <0.001 |
| Married | 1842 (65.1%) | 648 (65.5%) | 565 (60.2%) | 0.856, 0.007 |
| Child | 1490 (52.7%) | 556 (56.2%) | 490 (52.2%) | 0.059, 0.812 |
| Household income (/year) (JPY) | ||||
| 0−2 000 000 | 462 (16.3%) | 154 (15.6%) | 189 (20.1%) | 0.092, 0.147 |
| 2 000 000–4 000 000 | 739 (26.1%) | 279 (28.2%) | 236 (25.2%) | |
| 4 000 000–6 000 000 | 648 (22.9%) | 244 (24.6%) | 212 (22.6%) | |
| 6 000 000–8 000 000 | 426 (15.1%) | 159 (16.1%) | 137 (14.6%) | |
| 8 000 000–10 000 000 | 273 (9.7%) | 80 (8.1%) | 77 (8.2%) | |
| >10 000 000 | 280 (9.9%) | 74 (7.5%) | 87 (9.3%) | |
| Employment status | ||||
| Home duties | 1000 (35.4%) | 323 (32.6%) | 250 (26.7%) | |
| Employee | 492 (17.4%) | 162 (16.4%) | 194 (20.7%) | |
| Part‐time job | 599 (21.2%) | 224 (22.6%) | 215 (22.9%) | |
| Temporary job | 159 (5.6%) | 68 (6.9%) | 65 (6.9%) | |
| No occupation | 269 (9.5%) | 100 (10.1%) | 100 (10.7%) | |
| Other | 309 (10.9%) | 113 (11.4%) | 114 (12.2%) | |
The current smokers and ex‐smokers showed significantly higher OABSS and ICIQ‐SF scores than the non‐smokers (P < 0.0001, P < 0.0001). Regarding differences between ex‐smokers and current smokers, daytime frequency (OABSS Q1) and urgency (Q3) in current smokers were significantly higher than in ex‐smokers (P = 0.040, P = 0.014 and P = 0.032), whereas the nocturia (OABSS Q2) and UUI (Q4) in current smokers showed non‐significantly higher scores than in ex‐smokers (P = 0.874, P = 0.082, respectively). The percentage of patients with a total OABSS score of ≥1 was higher in ex‐smokers (720/990; 72.7%) and current smokers (714/938; 76.1%) than in non‐smokers (1875/2828; 66.3%; P < 0.0001, P < 0.0001; Table 2). The total ICIQ‐SF score was significantly higher in current and ex‐smokers than in non‐smokers (P < 0.0001, P < 0.0001). Each ISIQ‐SF questionnaire score was significantly higher in current and ex‐smokers than in non‐smokers (P < 0.0001, P < 0.0001, P < 0.0001, P < 0.0001, respectively), although no significance was noted between current and ex‐smokers (P = 0.091, P = 0.706, P = 0.134 and P = 0.178, respectively; Table 3). The ratio of participants with ≥1 of ICIQ‐SF score were 378 of 938 (40.3%) in current smokers, 402 of 990 (40.6%) in ex‐smokers and 881 of 2828 (31.2%) in non‐smokers (P < 0.0001, P < 0.0001; Table 3).
Table 2.
OABSS scores for non‐smokers, ex‐smokers and current smokers
| Variables | Non‐smoker | Ex‐smoker | Current smoker | P‐value (non‐smoker vs ex‐smoker, non‐smoker vs current smoker, ex‐smoker vs current smoker) |
|---|---|---|---|---|
| n = 2828 | n = 990 | n = 938 | ||
| OABSS Q1 | ||||
| Mean ± SD | 0.43 ± 0.55 | 0.48 ± 0.57 | 0.53 ± 0.61 | 0.026, <0.0001, 0.040 |
| Score ≥1, n (%) | 1133 (40.1%) | 434 (43.8%) | 441 (47.0%) | |
| OABSS Q2 | ||||
| Mean ± SD | 0.51 ± 0.73 | 0.66 ± 0.79 | 0.67 ± 0.85 | <0.0001, <0.0001, 0.874 |
| Score ≥1, n (%) | 1116 (39.5%) | 489 (49.4%) | 439 (46.8%) | |
| OABSS Q3 | ||||
| Mean ± SD | 0.51 ± 0.89 | 0.71 ± 1.07 | 0.84 ± 1.21 | <0.0001, <0.0001, 0.014 |
| Score ≥1, n (%) | 949 (33.6%) | 400 (40.4%) | 415 (44.2%) | |
| OABSS Q4 | ||||
| Mean ± SD | 0.25 ± 0.66 | 0.42 ± 0.89 | 0.50 ± 1.03 | <0.0001, <0.0001, 0.082 |
| Score ≥1, n (%) | 481 (17.0%) | 241 (24.3%) | 246 (26.2%) | |
| OABSS total score | ||||
| Mean ± SD | 1.70 ± 2.05 | 2.27 ± 2.50 | 2.54 ± 2.91 | <0.0001, <0.0001, 0.032 |
| Score ≥1, n (%) | 1875 (66.3%) | 720 (72.7%) | 714 (76.1%) | |
Table 3.
ICIQ‐SF scores in non‐smokers, ex‐smokers and current smokers
| Variables | Non‐smoker | Ex‐smoker | Current smoker | P‐value (non‐smoker vs ex‐smoker, non‐smoker vs current smoker, ex‐smoker vs current smoker) |
|---|---|---|---|---|
| n = 2828 | n = 990 | n = 938 | ||
| ICIQ‐SF1 | ||||
| Mean ± SD | 0.32 ± 0.71 | 0.47 ± 0.89 | 0.55 ± 1.01 | <0.0001, <0.0001, 0.091 |
| Score ≥1, n (%) | 635 (22.5%) | 298 (30.1%) | 297 (31.7%) | |
| ICIQ‐SF2 | ||||
| Mean ± SD | 0.54 ± 0.98 | 0.80 ± 1.16 | 0.82 ± 1.25 | <0.0001, <0.0001, 0.706 |
| Score ≥1, n (%) | 708 (25.0%) | 353 (35.7%) | 323 (34.4%) | |
| ICIQ‐SF3 | ||||
| Mean ± SD | 0.60 ± 1.41 | 0.98 ± 1.84 | 1.12 ± 2.16 | <0.0001, <0.0001, 0.134 |
| Score ≥1, n (%) | 689 (24.4%) | 340 (34.3%) | 304 (32.4%) | |
| ICIQ‐SF total score | ||||
| Mean ± SD | 1.49 ± 2.73 | 2.25 ± 3.50 | 2.48 ± 4.01 | <0.0001, <0.0001, 0.178 |
| Score ≥1, n (%) | 881 (31.2%) | 402 (40.6%) | 378 (40.3%) | |
The prevalence of urgency, daytime frequency, nocturia, UUI (OABSS definition), UUI (ICIQ‐SF definition), MUI, PMD and smoking status is shown in Figure 3. The relative risks of ex‐ and current smokers were 1.7 and 2.0 in OAB, 1.1 and 1.2 in daytime frequency, 1.5 and 1.7 in nocturia, 1.4 and 1.5 in UUI (OABSS definition), 1.3 and 1.3 in UUI (ISIQ‐SF definition), 1.2 and 1.1 in SUI, 1.4 and 0.9 in MUI, and 2.0 and 2.4 in PMD, respectively. The prevalence of OAB, daytime frequency, nocturia, UUI (OABSS definition), UUI (ICIQ‐SF definition), UUI, SUI, MUI and PMD was increased in ex‐ and current smokers. Taken together, these findings suggest that the smoking status has a strong influence on LUTS, especially OAB and UUI (OABSS definition).
Fig. 3.
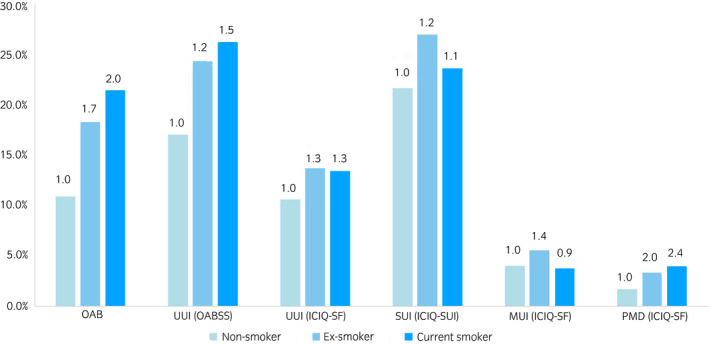
The prevalence of OAB, daytime frequency, nocturia, UUI (OABSS definition), UUI (ICIQ‐SF definition), SUI, MUI and PMD among the different smoking habit groups.
The impact of smoking status in each age group on OAB is shown in Figure 4. The prevalence of OAB was high in those aged 20–29 years (17.7%), and decreased with age (14.6% in those aged 30–39 years, 14.0% in those aged 40–49 years, 14.0% in those aged 50–59 years and 12.9% in those aged 60–69 years) before increasing in those aged ≥70 years (15.6%). When the risk was set as 1 for non‐smokers, the respective values for ex‐ and current smokers were 1.8 and 3.3 at age 20–29 years, 2.0 and 2.4 at age 30–39 years, 2.1 and 2.3 at age 40–49 years, 1.2 and 1.4 at age 50–59 years, 1.7 and 1.5 at age 60–69 years, and 1.3 and 1.6 at age ≥70 years. The younger participants (e.g. aged 20–39 years) showed a stronger influence of their smoking habit than those aged ≥40 years.
Fig. 4.
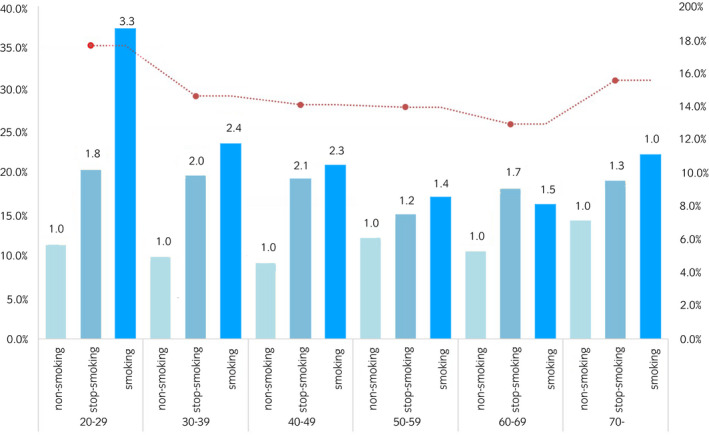
The prevalence of OAB in each smoking habit group.
The impact of smoking status in each age group on UUI is shown in Figure 5. The prevalence of UUI gradually increased with age: 17.9% in those aged 20–29 years, 16.4% in those aged 30–39 years, 18.5% in those aged 40–49 years, 22.9% in those aged 50–59 years, 22.0% in those aged 60–69 years, and 30.5% in those aged ≥70 years. When the risk was set at 1 for non‐smokers, the respective values for ex‐ and current smokers were 1.6 and 2.6 at age 20–29 years, 1.6 and 2.1 at age 30–39 years, 1.5 and 1.7 at age 40–49 years, 1.2 and 1.2 at age 50–59 years, 1.6 and 1.5 at age 60–69 years, and 1.4 and 1.3 at age ≥70 years. These trends were also observed in daytime frequency and nocturia (Fig. S3a,b). Smoking had a large influence on the risk of both OAB and UUI in the younger age group (aged 20–39 years).
Fig. 5.
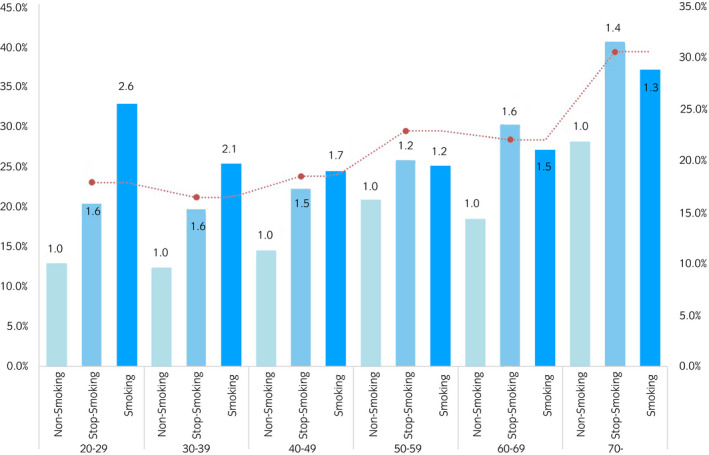
The prevalence of UUI in each smoking habit group.
The influence of the duration of smoking cessation and volume of smoking were analyzed in 750 women aged 20–49 years whose symptoms tended to be affected by their smoking habit; this age group was also selected to exclude the effect of post‐menopause status. The 197 ex‐smokers who had not smoked for 5–6 years showed a low prevalence of urgency and UUI compared with those with shorter durations of smoking cessation, but not significantly (urgency 23.3% for 0–2 years’ cessation, 17.2% for 3–4 years’ cessation and 10.2% for 5–6 years’ cessation, P = 0.374, P = 0.058; UUI 23.3% for 0–2 years’ cessation, 17.2% for 3–4 years’ cessation and 14.3% for 5–6 years’ cessation, P = 0.374, P = 0.204; Fig. 6). There was no correlation between the smoking cessation time and the prevalence of daytime frequency and nocturia among young women (Fig. S3c). For the 553 current smokers, the Brinkman index (years of smoking multiplied by the number of cigarettes smoked per day) was categorized as follows: <400, 400–699 and ≥700. There was no correlation between the smoking volume and prevalence of urgency, UUI, daytime frequency and nocturia among young women (Fig. 7; Fig. S3d).
Fig. 6.

The prevalence of OAB and UUI for the participants who stopped smoking for different durations of smoking cessation.
Fig. 7.
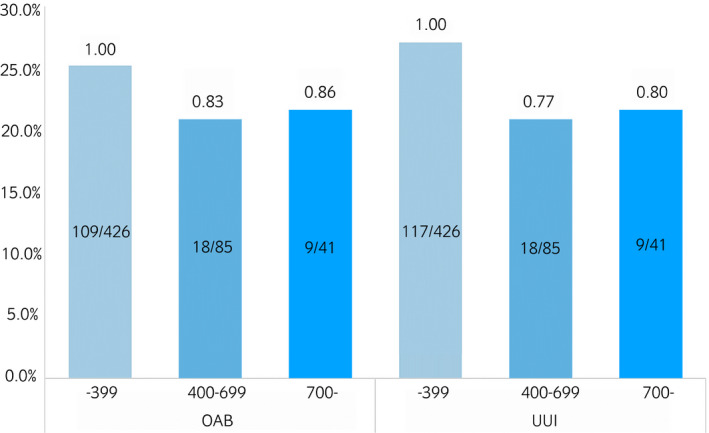
The prevalence of OAB and UUI among current smokers aged 20–49 years, according to the Brinkman index.
Discussion
The present study showed that a smoking habit worsened the daytime frequency, nocturia, urgency and UUI, especially among the younger population (aged <40 years), and the prevalence of those symptoms were relatively higher than previously reported among a total of 4756 female participants. The cessation of smoking might reversely decrease the prevalence of urgency and UUI, but not daytime frequency and nocturia. Smoking volume likely had no influence on symptom severity of urgency and UUI in current smoking group. This study was the first large‐scale study to show the correlation between the smoking habit and LUTS in non‐hospitalized participants. As in a previous population‐based study by Homma et al. in 2005 for Japanese participants, the prevalence of OAB and UUI was found to correlate with age. 6 A previous large study showed that the prevalence of OAB among female participants was 11% (n = 2380, Japan, letter), 19.3% (n = 822, Korea, interview), 16.9% (n = 5204, USA, telephone interview), 19% (n = 1253, Taiwan, interview) and 17.4% (n = 9728, six European countries, interview); that value in the present study was 14.5% (n = 4756, Japan, web‐based survey). 3 , 6 , 22 , 23 The median age was 61 years in the study by Homma et al., and 48 years in the present study. Although the prevalence of OAB was higher in older participants than in younger participants, the present cohort showed a higher prevalence than previous Japanese studies. 6 In young women aged 20–29 years, the prevalence of OAB was >30%. It was not possible to compare the present study with other studies, because no previous large studies have focused on young female patients. In the present study, the definition of OAB was based on the OABSS. A previous study by Homma defined OAB as eight or more voids/day and at least one episode of urinary urgency/week. The difference of OAB definition might influence the difference comparing to the previous studies. Furthermore, the younger participants who answered the questionnaire might have been interested in urinary symptoms; thus, the prevalence might have been overestimated. Further study is required. The present study involved a web‐based internet survey using a website or apps with a tablet or smartphone, and OAB was diagnosed by a self‐administrated questionnaire and might have been influenced by psychographics; the differences in survey methods might therefore have influenced the findings.
The present study showed that a smoking habit was a risk factor for LUTS in women. Young women in particular (aged 20–49 years) showed a markedly increased risk of LUTS when coupled with a smoking habit. In older women, the association between a smoking habit and continence decreased. Regarding ex‐smokers, the urgency and UUI prevalence decreased in correlation with the duration of smoking cessation among young women. In current smokers, there was no marked correlation between the smoking volume and the prevalence of urgency and UUI. Although a Norwegian cross‐sectional population‐based study found an increased association with urinary incontinence in both ex‐ and current smokers, other studies have found no such association between a smoking habit and urinary incontinence. 24 , 25 The multifactorial causes of OAB and UUI are reflected in the wide range of risk factors, including age, the diagnosis of depression, alcohol intake, physical strength, obesity and so on. 3 , 26 , 27 In the elderly, aging‐associated changes in the pelvic vasculature, such as atherosclerosis, might play an important role in bladder activity, so the difference of smoking habit was shown clearly in the young female group. 28
The present study suggested that smoking cessation improved urinary symptoms in younger participants. Smoking is considered a major lifestyle risk factor for cancer, coronary heart disease and LUTS. 13 Although the detailed mechanism is still unknown, smoking‐induced atherosclerosis is thought to be a pathway influencing the development of LUTS. Arterial occlusive disease might lead to chronic bladder ischemia, bladder hyperactivity and morphological bladder wall changes. 29 Aging usually reduces the bladder blood flow and causes vascular endothelial dysfunction, resulting in atherosclerosis and hypertension. 30 Smoking might also play a role in the pathogenesis of pelvic flow dysfunction and urinary incontinence. 14 LUTS was affected by several factors correlated with aging, including diabetes mellitus, hypertension, post‐menopausal status and other factors. We therefore hypothesized that for young women, smoking would have a large influence on LUTS, and that smoking cessation would show higher efficacy in this age group for the same reason.
Several limitations associated with the present study warrant mention. First, this study used a web‐based self‐administrated questionnaire. The monitor participants answered this questionnaire using a computer or an app on a tablet or smartphone. Our study, therefore, failed to obtain the satisfactory number of participants calculated by population‐based numbers, especially for participants aged ≥70 years. However, we did collect participants aged ≤65 years old, and the present study showed that prevalence of LUTS in the younger group (aged 20–49 years) tended to be affected by smoking as a risk factor. In addition, this web‐based anonymous self‐administrated interview collected detailed results with no risk of communication bias. In LUTS‐related studies, a non‐communicated examination would achieve higher accuracy of patients' intention. Therefore, despite the aforementioned limitation, we obtained sufficient data among non‐elderly participants. Second, the present study did not evaluate any smoking‐related factors, such as alcohol intake, caffeine consumption or other health‐related problems, including hypertension and psychiatric disorder. The present study showed that the risk of smoking tended to be present for all age groups, with a marked difference in smoking habit among young women. In young ex‐smokers, the duration of smoking cessation was found to be correlated with a lower incidence of an urgency or UUI diagnosis, but in smokers, the volume of smoking was not correlated with either an urgency, daytime frequency, nocturia or UUI diagnosis. We therefore speculated that a smoking habit worsens LUTS symptoms in women, but this influence might have been hidden by other factors with aging. The present study excluded male participants, because prostate hyperplasia would have had a large effect on LUTS. In Japan, the rate of smoking among men is approximately three times higher than that among women. Further study is required to investigate the effects of the smoking status on LUTS in men.
In conclusion, the prevalence of LUTS, including OAB and UUI, increases with age. Furthermore, a smoking habit exacerbates LUTS symptoms, especially among young women.
Conflict of interest
None declared.
Supporting information
Figure S1. Regional distribution of participants.
{kind=link}
Figure S2. The correlation between the OABSS score and ICIQ‐SF score.
{kind=link}
Figure S3. The prevalence of (a) daytime frequency and (b) nocturia in each smoking habit group. (c) The prevalence of daytime frequency and nocturia in ex‐smokers with different durations of smoking cessation. (d) The prevalence of OAB and UUI among current smokers of aged 20–39 years, according to the Brinkman index.
Table S1. Prefecture of residence of participants by smoking habit.
Table S2. Raw data.
References
- 1. Abrams P, Cardozo L, Fall M et al The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub‐committee of the International Continence Society. Neurourol. Urodyn. 2002; 21: 167–78. [DOI] [PubMed] [Google Scholar]
- 2. Irwin DE, Kopp ZS, Agatep B, Milsom I, Abrams P. Worldwide prevalence estimates of lower urinary tract symptoms, overactive bladder, urinary incontinence and bladder outlet obstruction. BJU Int. 2011; 108: 1132–8. [DOI] [PubMed] [Google Scholar]
- 3. Stewart WF, Van Rooyen JB, Cundiff GW et al Prevalence and burden of overactive bladder in the United States. World J. Urol. 2003; 20: 327–36. [DOI] [PubMed] [Google Scholar]
- 4. Irwin DE, Milsom I, Hunskaar S et al Population‐based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur. Urol. 2006; 50: 1306–14. [DOI] [PubMed] [Google Scholar]
- 5. Lugo Salcedo F, Sanchez Borrego R; Group GUIAS . Assessment of female prevalence of overactive bladder (OAB) in Barcelona using a self‐administered screening questionnaire: the Cuestionario de Autoevaluacion del Control de la Vejiga (CACV). Int. Urogynecol. J. 2013; 24: 1559–66. [DOI] [PubMed] [Google Scholar]
- 6. Homma Y, Yamaguchi O, Hayashi K. Neurogenic Bladder Society C. An epidemiological survey of overactive bladder symptoms in Japan. BJU Int. 2005; 96: 1314–8. [DOI] [PubMed] [Google Scholar]
- 7. Grimby A, Milsom I, Molander U, Wiklund I, Ekelund P. The influence of urinary incontinence on the quality of life of elderly women. Age Ageing 1993; 22: 82–9. [DOI] [PubMed] [Google Scholar]
- 8. Roosen A, Chapple CR, Dmochowski RR et al A refocus on the bladder as the originator of storage lower urinary tract symptoms: a systematic review of the latest literature. Eur. Urol. 2009; 56: 810–9. [DOI] [PubMed] [Google Scholar]
- 9. Banakhar MA, Al‐Shaiji TF, Hassouna MM. Pathophysiology of overactive bladder. Int. Urogynecol. J. 2012; 23: 975–82. [DOI] [PubMed] [Google Scholar]
- 10. Kawahara T, Board IJUE. Re: Quality of life in patients aged 65 years and older with overactive bladder treated with mirabegron across eight European countries: Secondary analysis of BELIEVE. Int. J. Urol. 2020; 27: 188. [DOI] [PubMed] [Google Scholar]
- 11. Nomiya M, Yamaguchi O, Andersson KE et al The effect of atherosclerosis‐induced chronic bladder ischemia on bladder function in the rat. Neurourol. Urodyn. 2012; 31: 195–200. [DOI] [PubMed] [Google Scholar]
- 12. Sagawa K, Aikawa K, Nomiya M et al Impaired detrusor contractility in a rat model of chronic bladder ischemia. Urology 2013; 81: 1379.e9–1379.e14. [DOI] [PubMed] [Google Scholar]
- 13. Madhu C, Enki D, Drake MJ, Hashim H. The functional effects of cigarette smoking in women on the lower urinary tract. Urol. Int. 2015; 95: 478–82. [DOI] [PubMed] [Google Scholar]
- 14. Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet. Gynecol. 1997; 89: 501–6. [DOI] [PubMed] [Google Scholar]
- 15. Bump RC, McClish DK. Cigarette smoking and urinary incontinence in women. Am. J. Obstet. Gynecol. 1992; 167: 1213–8. [DOI] [PubMed] [Google Scholar]
- 16. Danforth KN, Townsend MK, Lifford K, Curhan GC, Resnick NM, Grodstein F. Risk factors for urinary incontinence among middle‐aged women. Am. J. Obstet. Gynecol. 2006; 194: 339–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Dallosso HM, McGrother CW, Matthews RJ, Donaldson MM, Leicestershire MRCISG. The association of diet and other lifestyle factors with overactive bladder and stress incontinence: a longitudinal study in women. BJU Int. 2003; 92: 69–77. [DOI] [PubMed] [Google Scholar]
- 18. Statistics Bureau of Japan . Population Census. 2019. [Cited 1 Oct 2019.] Available from URL: https://www.stat.go.jp/data/jinsui/2017np/index.html.
- 19. Homma Y, Yoshida M, Seki N et al Symptom assessment tool for overactive bladder syndrome–overactive bladder symptom score. Urology 2006; 68: 318–23. [DOI] [PubMed] [Google Scholar]
- 20. Avery K, Donovan J, Peters TJ, Shaw C, Gotoh M, Abrams P. ICIQ: a brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourol. Urodyn. 2004; 23: 322–30. [DOI] [PubMed] [Google Scholar]
- 21. Gotoh M, Homma Y, Yokoyama O, Nishizawa O. Responsiveness and minimal clinically important change in overactive bladder symptom score. Urology 2011; 78: 768–73. [DOI] [PubMed] [Google Scholar]
- 22. Wein AJ, Rovner ES. Definition and epidemiology of overactive bladder. Urology 2002; 60: 7–12. [DOI] [PubMed] [Google Scholar]
- 23. Chen GD, Lin TL, Hu SW, Chen YC, Lin LY. Prevalence and correlation of urinary incontinence and overactive bladder in Taiwanese women. Neurourol. Urodyn. 2003; 22: 109–17. [DOI] [PubMed] [Google Scholar]
- 24. Hannestad YS, Rortveit G, Daltveit AK, Hunskaar S. Are smoking and other lifestyle factors associated with female urinary incontinence? The Norwegian EPINCONT Study. BJOG 2003; 110: 247–54. [PubMed] [Google Scholar]
- 25. Brown JS, Seeley DG, Fong J, Black DM, Ensrud KE, Grady D. Urinary incontinence in older women: Who is at risk? Study of Osteoporotic Fractures Research Group. Obstet. Gynecol. 1996; 87: 715–21. [DOI] [PubMed] [Google Scholar]
- 26. Hirayama A, Torimoto K, Mastusita C et al Risk factors for new‐onset overactive bladder in older subjects: results of the Fujiwara‐kyo study. Urology 2012; 80: 71–6. [DOI] [PubMed] [Google Scholar]
- 27. Komesu YM, Schrader RM, Ketai LH, Rogers RG, Dunivan GC. Epidemiology of mixed, stress, and urgency urinary incontinence in middle‐aged/older women: the importance of incontinence history. Int. Urogynecol. J. 2016; 27: 763–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Ponholzer A, Temml C, Wehrberger C, Marszalek M, Madersbacher S. The association between vascular risk factors and lower urinary tract symptoms in both sexes. Eur. Urol. 2006; 50: 581–6. [DOI] [PubMed] [Google Scholar]
- 29. Andersson KE, Nomiya M, Sawada N, Yamaguchi O. Pharmacological treatment of chronic pelvic ischemia. Ther. Adv. Urol. 2014; 6: 105–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Pinggera GM, Mitterberger M, Steiner E et al Association of lower urinary tract symptoms and chronic ischaemia of the lower urinary tract in elderly women and men: assessment using colour Doppler ultrasonography. BJU Int. 2008; 102: 470–4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Regional distribution of participants.
Figure S2. The correlation between the OABSS score and ICIQ‐SF score.
Figure S3. The prevalence of (a) daytime frequency and (b) nocturia in each smoking habit group. (c) The prevalence of daytime frequency and nocturia in ex‐smokers with different durations of smoking cessation. (d) The prevalence of OAB and UUI among current smokers of aged 20–39 years, according to the Brinkman index.
Table S1. Prefecture of residence of participants by smoking habit.
Table S2. Raw data.