

Abstract
The aim of this report was to investigate coronary artery occlusion related to De Winter‐like electrocardiogram (ECG) pattern. A patient admitted to Zhongshan Hospital who was diagnosed with acute coronary syndrome with De Winter‐like ECG pattern was reviewed in our case report. In this case, we found that a De Winter‐like ECG change in the inferior and lateral leads was associated with left circumflex coronary artery occlusion. After a timely reperfusion therapy, the symptom was obviously alleviated with a normalization of upsloping ST‐segment. Doctors should be aware that De Winter‐like ECG changes can also predict acute occlusion in any coronary artery, not only in the left anterior descending artery and right coronary artery but also in the left circumflex coronary artery.
Keywords: De Winter syndrome, Coronary artery occlusion
History of presentation
A 60‐year‐old man was admitted to the emergency department with persistent substernal chest and throat tightness and associated diaphoresis of 4 h duration. Electrocardiogram (ECG) performed at admission showed ST‐segment depression in inferior leads. The troponin T level was 0.055 ng/mL (normal value, <0.03 ng/mL) and rose to 0.085 ng/mL 2 h after admission.
Medical history
The patient had a medical history of hypertension and no family history of cardiac diseases. He was a current smoker with a smoking history of 30 package‐years.
Differential diagnosis
Differential diagnoses included ST‐segment elevation myocardial infarction (STEMI), non‐STEMI (NSTEMI), dissection of the aorta, and myocarditis.
Investigations
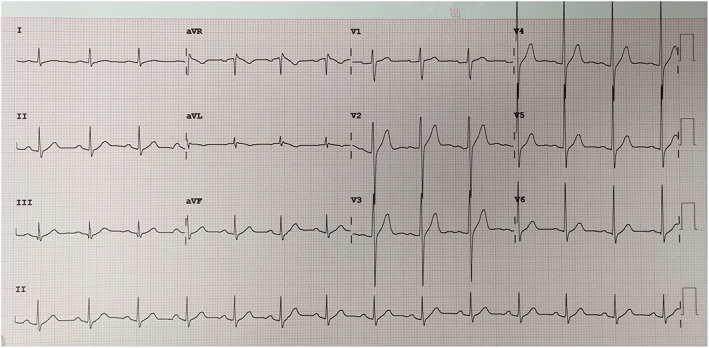
ECG (Figure 1 ) revealed upsloping ST‐segment depression at J point and positive T waves in leads II, III, aVF, and V5 through V6. Duration of QRS did not broaden, with a minimal ST‐elevation in lead aVR.
FIGURE 1.
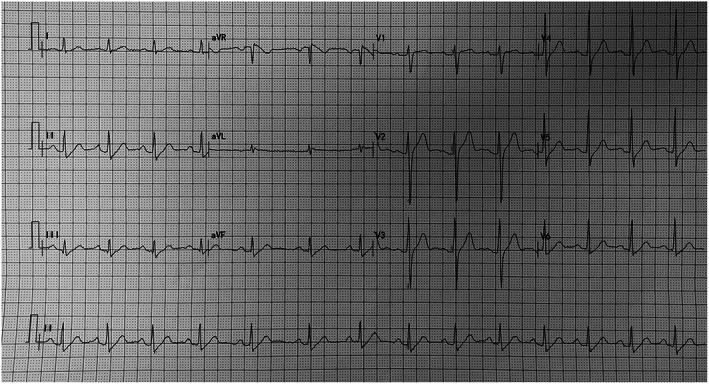
An electrocardiogram showing upsloping ST‐segment depression and normal T waves in leads II, III, aVF, and V5 through V6.
Management
The patient underwent immediate coronary angiography, and the procedure revealed a total occlusion of the proximal site of left circumflex coronary artery (LCX) (Figure 2 ), myocardial bridge leading to 20–30% stenosis of mid‐distal left anterior descending (LAD) artery, and no significant stenosis of right coronary artery (RCA) (Figure 3 ). The occlusion was treated successfully by percutaneous coronary intervention (PCI) with stent placement (Figure 4 ). After the procedure, the symptom of patient was obviously alleviated with normalization of ST‐segment in leads II, III, aVF, and V5 through V6 (Figure 5 ). An echocardiography after PCI identified reduced contraction in basal inferoposterior wall of the left ventricle.
FIGURE 2.
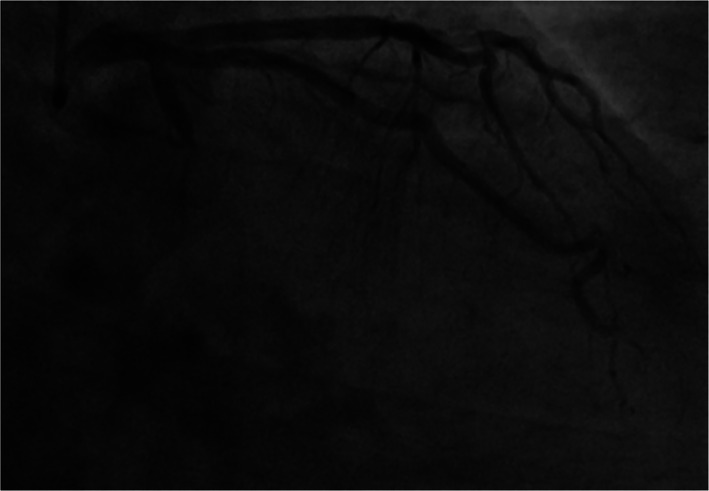
Coronary angiography revealed occlusion of left circumflex coronary artery.
FIGURE 3.
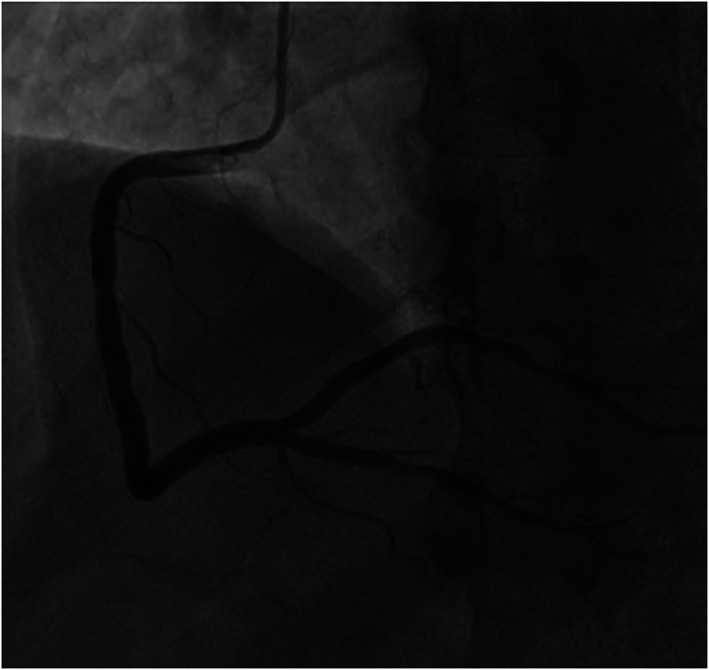
Coronary angiography revealed no significant stenosis of right coronary artery.
FIGURE 4.
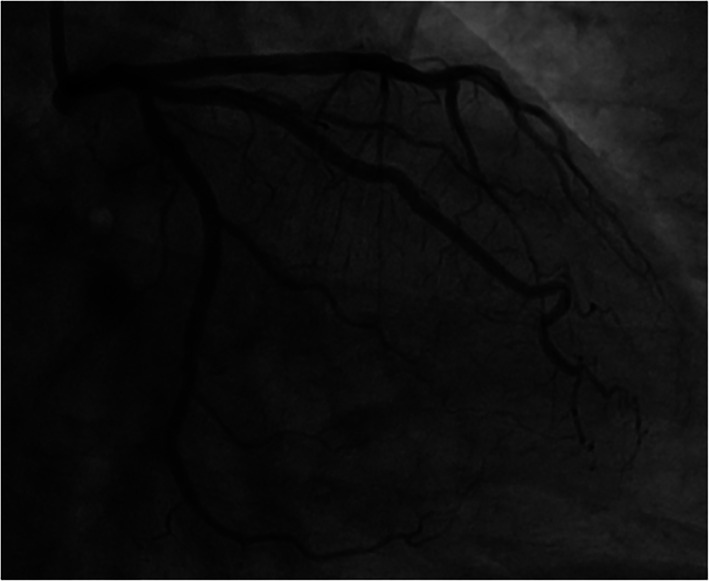
The occlusion was treated successfully by means of percutaneous coronary intervention with stent placement.
FIGURE 5.
Postprocedure electrocardiogram showed that evolution of ST‐segment in leads II, III, aVF, and V5 through V6 was normal.
Follow‐up
At the 1 year follow‐up, the patient followed guideline‐directed medical therapy. And he also received smoking‐cessation counselling and was referred to a cardiac rehabilitation programme. Until now, he no longer experiences chest tightness or pain.
Discussion
The De Winter syndrome is an uncommon ECG pattern in patients with ischaemic chest pain. De Winter et al. 1 first reported the STEMI equivalent ECG without ST‐elevation in 2008. The diagnostic characteristics include (i) 1–3 mm upsloping ST‐segment depression at the J point in the precordial leads; (ii) tall, prominent, symmetric T waves in the precordial leads; (iii) minimal ST‐elevation (0.5–1 mm) in aVR lead; and (iv) classical STEMI morphology may precede or follow the De Winter pattern. Verouden et al. 2 found in a large scale of retrospective study that 2% of patients who need PCI to LAD had De Winter ECG pattern. A systematic review 3 recommended De Winter ECG pattern as a test to identify acute coronary occlusion for its positive predictive values of 95% to 100%. After 2008, many case reports were published, but mostly limited to precordial leads and associated with LAD occlusion. To the best of our knowledge, rare cases have been reported so far showing ECG changes in inferior leads equivalent to De Winter LAD pattern associated with RCA occlusion. 4 Nevertheless, there has been no report about De Winter ECG pattern related with LCX total occlusion. However, in our present case, the De Winter pattern ECG in the inferolateral leads is associated with acute total occlusion of LCX artery. Acute ischaemia of basal inferoposterior wall of the left ventricle was indicated by echocardiography. The electrophysiological mechanisms of the ECG pattern remains elusive, and the potential reasons may include 5 (i) an anatomical variant of the Purkinje fibres, with endocardial conduction delay; (ii) the lack of activation of sarcolemmal ATP‐sensitive potassium (KATP) channels caused by ischaemic ATP depletion; (iii) collateral blood supply might protect the myocardium from transmural ischaemia; and (iv) the area of transmural ischaemia was so large that no injury currents were generated toward the precordial leads but only directed upward to an AVR lead. Our case suggested that the De Winter pattern ECG would present in any lead and be associated with acute occlusion of any artery. Therefore, cardiologists and physicians should be able to recognize that such unique pattern of ECG changes is not limited to anterior leads but can occur in inferior and sidewall leads as well and should be aware that acute occlusion can occur in any coronary artery, not only in the LAD and RCA but also in the LCX.
This case showed that the occurrence of De Winter ECG sign with ST‐segment depression at the J point with upsloping ST‐segments and positive T‐wave in the inferior wall and sidewall leads was associated with acute total LCX artery occlusion. Recognition of this ECG pattern is of vital importance to an immediate reperfusion therapy.
Conflict of interest
Qingxing Chen, Tian Zou, Yang Pang, Yunlong Ling, and Wenqing Zhu declare that they have no conflict of interest.
Funding
None.
Chen, Q. , Zou, T. , Pang, Y. , Ling, Y. , and Zhu, W. (2020) The De Winter‐like electrocardiogram pattern in inferior and lateral leads associated with left circumflex coronary artery occlusion. ESC Heart Failure, 7: 4301–4304. 10.1002/ehf2.12946.
Qingxing Chen and Tian Zou contributed equally to this work.
References
- 1. De Winter RJ, Verouden NJ, Wellens HJ, Wilde AA, Interventional Cardiology Group of the Academic Medical Center . A new ECG sign of proximal LAD occlusion. N Engl J Med 2008; 359: 2071–2073. [DOI] [PubMed] [Google Scholar]
- 2. Verouden NJ, Koch KT, Peters RJ, Henriques JP, Baan J, van der Schaaf R, Vis MM, Tijssen JG, Piek JJ, Wellens HJ, Wilde AA, De Winter RJ. Persistent precordial “hyperacute” T‐waves signify proximal left anterior descending artery occlusion. Heart 2009; 95: 1701–1706. [DOI] [PubMed] [Google Scholar]
- 3. Morris NP, Body R. The De Winter ECG pattern. Eur J Emerg Med 2017; 24: 236–242. [DOI] [PubMed] [Google Scholar]
- 4. Tsutsumi K, Tsukahara K. Is the diagnosis ST‐segment elevation or non‐ST‐segment elevation myocardial infarction? Circulation 2018; 138: 2715–2717. [DOI] [PubMed] [Google Scholar]
- 5. Li RA, Leppo M, Miki T, Seino S, Marbán E. Molecular basis of electrocardiographic ST‐segment elevation. Circ Res 2000; 87: 837–839. [DOI] [PubMed] [Google Scholar]