

Abstract
OBJECTIVE:
To analyze the demographic data, etiologies and risk factors of 106 children and adolescents with low back pain (LBP) who applied to our clinic.
METHODS:
The medical records of patients with low back pain under 18 presenting to our clinic in 2014–2018 were examined retrospectively. Patients’ demographic data, physical examination findings, laboratory and imaging results, and risk factors for low back pain were evaluated; diagnosis and treatment modalities were recorded.
RESULTS:
In this study, 106 children and adolescents 8–17 (mean 14.24±2.33) years, 55 girls (51.8%) and 51 boys (48.1%) were included. Sixty-two patients (58.4%) were diagnosed with non-specific low back pain, 24 (22.6%) with lumbar disc herniation, six (5.6%) with inflammatory low back pain, five (4.7%) with spondylolysis (with accompanying listhesis in two), five (4.7%) with scoliosis, and four (3.7%) with Scheuermann Disease. Three patients were operated and another patient underwent an algological intervention for persistent pain. Six patients diagnosed as spondyloarthropathy were referred to the pediatric rheumatology department. Pain in the remaining cases was brought under control using conservative methods in a combination of medical treatment, rest and physiotherapy.
CONCLUSION:
Low back pain is a frequent complaint in the child-adolescent age group. The causes of low back pain are as diverse as adults in this age group. The contrary common belief that severe problems, such as malignancy are common, mechanical reasons as the most common cause of low back pain.
Keywords: Adolescent, child, low back pain
Low back pain (LBP) is defined as pain beginning from beneath the 12th rib and ending above the gluteal region. LBP in adulthood is one of the major public health problems in the world. It is also common among children and adolescents [1], and a high prevalence in this age group has been reported in various epidemiological studies [2, 3]. The lifetime prevalence of LBP in children and adolescents in previous studies ranges from 9% to 69% and increases significantly between 12 and 18 years [4]. Until the age of 17 years, significant gender differences occur; it is more common in girls [5]. Causes of LBP in children and adolescents are as diverse as in adults, but there is considerably less information regarding LBP in this age group compared to adults. Self-limiting non-specific LBP is described as the most common form of the condition in children and adolescents. Several factors, such as gender, anthropometry, tightness of hamstring muscles, hypermobility, rapid growth, physical inactivity or a high level of sports activities, TV watching, sitting position and psychological and social impacts, have been associated with non-specific LBP [6–8].
We screened child-adolescent patients who presented to our clinic with LBP during a four year period. The present study aims to describe the etiologies of LBP and pain-associated risk factors and emphasize that the problem is one commonly seen in this age group.
MATERIALS AND METHODS
Patients aged under 18 presenting to our clinic due to LBP between May 2014 and May 2018 were included in this research. Our study was designed retrospectively, and ethical committee approval was obtained before commencement. Organic (referred pain), infectious, malign and psychogenic etiologies were excluded from this study. Patients’ demographic data, the severity of pain measured using a visual analog scale, positive examination findings, laboratory tests, roentgenogram and magnetic resonance imaging (MRI) findings were recorded. Imaging comprised plain standing AP and lateral roentgenogram and lumbosacral MRI. Sacroiliac MRI was performed only in patients with inflammatory LBP. Patients were asked about suspected risk factors for LBP, such as family history, remaining in a fixed (seated) position for more than two hours per day, and sporting activity (participating in active sporting activity at least three days per week). Hypermobility, another possible risk factor for LBP, was tested using Beighton et al.’s [9] method. Scores of six out of nine are regarded as indicating general joint hypermobility [10]. Hamstring flexibility was measured in a lying position with the hip flexed 90° and using an active knee extension test with a simple goniometer. Hamstring tightness above 40° was accepted as a possible risk factor. Patients’ diagnoses and treatments applied were recorded.
Statistical Analysis
Statistical analysis of the data obtained was performed on IBM SPSS Statistics 22 (IBM SPSS, Turkey) software. Descriptive statistical methods (mean, standard deviation and frequency) were used.
RESULTS
One hundred-six children and adolescents aged between eight and 17 (mean 14.24±2.33), 55 (51.8%) girls and 51 (48.1%) boys were included in this study. Patients’ mean VAS pain value was 5.26±1.55, and their mean body mass index (BMI) was 22.11±4.24. Patients’ general characteristics are shown in Table 1, distribution of age and gender is shown in Figure 1, findings accompanying non-specific LBP and risk factors are shown in Table 2, and etiologies of LBP are shown in Table 3.
TABLE 1.
Patients’ general characteristics
| % | Mean±SD | |
|---|---|---|
| Age | 14.24±2.33 | |
| BMI | 22.11±4.24 | |
| VAS | 5.26±1.55 | |
| Sex | ||
| Girls | 51.8 | |
| Boys | 48.1 | |
| Body weight | ||
| Normal weight | 64.1 | |
| Overweight | 9.4 | |
| Obese | 9.4 | |
| Underweight | 16.9 |
SD: Standard deviation; BMI: Body mass index; VAS: Visual Analogue Scale.
FIGURE 1.
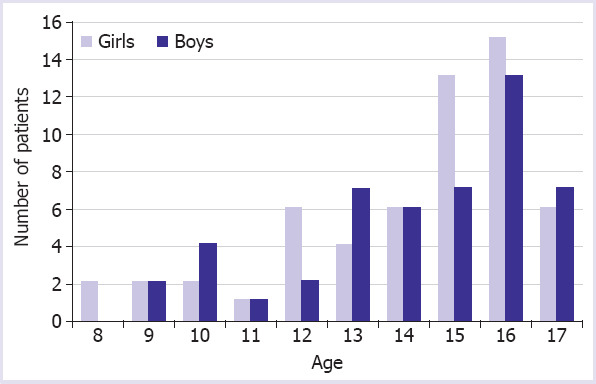
Age and gender distribution of the low back pain in children and adolescents.
TABLE 2.
Distribution of the findings accompanying non-specific low back pain and risk factors
| % | |
|---|---|
| Posture disorder | |
| No | 74.1 |
| Yes | 25.8 |
| Tight hamstrings | |
| No | 58.0 |
| Yes | 41.9 |
| Hypermobility | |
| No | 70.9 |
| Yes | 29.0 |
| Family history | |
| No | 72.5 |
| Yes | 27.4 |
| Obesity | |
| No | 85.5 |
| Yes | 14.5 |
| Active sporting life | |
| No | 75.8 |
| Yes | 24.1 |
| Spending time in an immobile position per day (>3 h) | |
| No | 62.9 |
| Yes | 37.0 |
TABLE 3.
Distribution of etiologies of the low back pain
| % | |
|---|---|
| Diagnosis | |
| Non-specific LBP | 58.4 |
| Lumbar disk herniation | 22.6 |
| Protrusion | 19.8 |
| Extrusion | 2.8 |
| Inflammatory LBP | 5.6 |
| Spondylolysis | 2.8 |
| Spondylolysis+Listhesis | 1.8 |
| Scoliosis | 4.7 |
| Scheuermann disease | 3.7 |
LBP: Low back pain.
Non-specific LBP
Sixty-two patients (58.7%) had non-specific LBP. The mean age of these patients, 33 girls and 29 boys, was 14.19±2.40. The risk factors of non-specific LBP were as follows. Nine patients (14.5%) were obese, four (6.4%) patients were overweight. Poor posture was present in 16 (25.8%) patients. Twenty-six patients (41.9%) had tight hamstring muscles. A positive family history was present in 17 (27.4%) patients. Hypermobility was present in 18 (29.0%). Fifteen (24.1%) patients took part in sporting activities at least three times a week. Five (5) patients played basketball, four (4) patients played football, two (2) patients did tae-kwon-do, two (2) patients did gymnastics, one (1) patient played volleyball and one (1) patient took part in dancing. Twenty-three of our patients (37.0%) remained in an immobile position for three h a day due to TV, tablet or mobile phone use. Symptoms were resolved either spontaneously or by short-term rest and analgesic drug use. All patients were given a home exercise programme.
Lumbar Disc Herniation
Lumbar disc herniation was determined in 24 (22.6%) patients. The mean age of our patients with disc herniation was 14.04±2.27. Thirteen of them were girls (56.5%) and eleven were boys (43.4%). Anterior flexion was limited in 18 of the 24 patients, and the straight leg raising test was positive in seven patients. Lumbar muscle spasm was positive in twelve (12) patients. A positive trauma history was in eight) and family history was in ten patients. No patients had any motor deficit but three of patients had reduced achilles reflex. Distribution of the single-level lumbar disc herniation was as follows: 4 at L4-5, 12 at L5-S1. In the two-level herniation group, there were four patients with a L4-5 and L5-S1herniation, one (1) patient with a L3-4 and L4-5 herniation. Extruded hernia at the L5-S1 level was determined in three patients. Only three patients were operated electively during our follow-up for persistent pain. Transforaminal steroid injection was administered by the algology department to one patient with extruded disc herniation. Symptoms requiring a repeat injection occurred approximately six months after the pain were brought under control. The other patients’ symptoms were brought under control with symptomatic therapy (rest, analgesic drug use and physiotherapy).
Inflammatory LBP
Six patients in the adolescent age group, four boys and two girls, described inflammatory LBP. At physical examination, lower back movements were painful, and only one (1) patient had limited anterior flexion. Two patients had high acute phase reactants. These tests were not requested in two cases, but the other patients’ HLA B27 values were positive. An appearance compatible with early inflammatory findings was observed at sacroiliac joint MRI. Non-steroidal anti-inflammatory drugs and exercise programme (including core stabilization, posture and breathing exercises) were given to these patients and they referred to the pediatric rheumatology department.
Spondylolysis-listhesis
Spondylolysis was determined in five patients, and accompanying listhesis (grade 1 anterior listhesis at the L5-S1 level and L4-5 level) was observed in two (2). Lysis was at the L5-S1 level in two patients, at the L4-5 level in two and L3-4 in one (1). Diagnosis was made with X-ray in three patients and with MRI in two (2). One of the patients played on the school basketball team, and one had a long history of playing tae kwon do. Pain was brought under control with activity restriction, brace use, analgesic drugs. Exercise programme were also given to the patients (stretching of the hamstring muscles, core stabilization and strengthening of the trunk muscles).
Scoliosis
We determined scoliosis in five of our patients. Pain was in lumbar region. Roentgenogram of scoliosis was performed on patients who had positive Adam’s forward test. There were single lumber curve in three patients, predominantly lumbar double curve in one -patient. Cobb angle was less than 20 degrees and Risser grade 4–5 in these four patients. Pain was brought under control with physiotherapy. In a patient with double curvature, we determined scoliosis more than 30 degrees in thoracal and between 20–30 degrees in the lumbar region. However, the patient was presented with only the LBP complaint. MRI of the dorsal and lumbar spine was reported a syrinx cavity which was detected at level D4-10 and she was operated.
Scheuermann Disease
We determined Scheuermann disease with thoracolumbar involvement in four (three boys and one girl) of our patients. Pain was in the upper lumbar region and taken under control using a brace and physiotherapy.
DISCUSSION
In our series of 106 patients, LBP was more common in the adolescent age group. There was no significant difference in gender, and the most common cause of etiology was non-specific LBP.
Determining the etiology in LBP is important to predict the clinical course. Because LBP in childhood is a significant risk factor for the adulthood. If it is not diagnosed correctly, it may become chronic and cause disability in adulthood [1]. There is a commonly held opinion that there is a high probability of back pain-LBP in childhood resulting from major causes, such as malignity or infection. However, mechanical and physical factors represent the majority of causative mechanisms for LBP among boys and girls of school age [1]. Consistent with previous studies, the etiology of LBP was non-specific (mechanical) in 58.7% of our cases.
Non-specific LBP in this age group has been linked to a range of diverse factors, including sex, anthropometry, incorrect posture, tight hamstrings, hypermobility, taking part in sporting activities and use of devices, such as TV, tablets and smartphones, rapid growth, family history and psychological and social agents [1, 5].
de Sá Pinto et al. [11] compared obese children aged 7–14 with normal weight controls and determined a positive correlation between BMI and LBP. However, a systematic review published in 2014 included 40 studies reported poor evidence for a positive correlation between LBP and overweight [12].
There is a common belief that postural problems are a cause of LBP. However, the relationship between LBP and posture is not clear. A recent study of 966 Portuguese children aged between 10 and 16 reported that incorrect postural habits were linked to LBP [13].
Harreby et al.’s study of 1389 schoolchildren aged 13–16 and Salminen et al.’s study of 370 schoolchildren aged 11–17 reported that tightness of hamstring muscles was common among adolescents but was not correlated with LBP [6, 7].
A study of 7542 schoolchildren aged 13–15 reported a significant relation between non-specific LBP and positive family history [14].
In a large cohort of 14-year-olds, no relationship between joint hypermobility and chronic musculoskeletal pain (including LBP) was found [15], while few studies reported a positive correlation between hypermobility and LBP in young people [16].
A high incidence of LBP occurs in young people engaging in sports requiring flexion/extension/rotation of the spine [17]. Sjolie reported a high incidence of LBP among 88 teenagers in those who took part in aerobics [18]. In their study of schoolchildren, Balaque et al. reported an association between LBP and aerobics, bodybuilding, volleyball, tennis and cycling [8]. The same study reported that watching TV for more than two h daily increased the incidence of LBP [8], while another reported a positive correlation between time spent watching TV and position and LBP [19].
Muscle growth is slower than bone growth at puberty. Rapid growth may also be associated with changes in posture. In this period, tightness of thoracolumbar fascia, increase in lordosis and decrease in muscle flexibility result in pain. Rapid growth may be one of the causes non-specific LBP in adolescence [20].
Unlike general literature, the second most common etiology in our patients with LBP was lumbar disc herniation. The reported incidence of lumbar disc herniation in the pediatric and adolescent population is low (3.5%) [21], but we determined disc herniation in 24 (22.6%) of our patients with LBP. Conservative methods are the first choice of treatment. However, in cases whose no respond to conservative treatments, the progression of neurological deficit or cauda equina syndrome should be treated with surgery. A recent study of 70 patients aged between 10–19 reported that disc herniation was most common at the L4-5 and L5-S1 levels. All patients in that study were treated using conservative methods, and only six were operated on due to progressive neurological deficit and persistent pain [22].
Inflammatory LBP was the third most frequent etiology in our case series. Children and adolescents present with the insidious onset of low back and buttock pain. On clinical examination, there may be a pain to palpation over the sacroiliac joint and mobility of the lumbar region may be reduced. HLAB27 is often positive in this age group. Roentgenogram of the pelvis is usually normal. MRI shows the presence of bone marrow oedema [23].
Spondylolysis was the fourth most frequent etiology in our case series. The prevalence of spondylolysis/spondylolisthesis in adolescents is approximately 6% [24]. It is frequently seen among adolescents who take part in active sports, particularly adolescents requiring repetitive hyperextension and flexion movements [25]. In a study, spondylolysis was determined in 47% of 100 adolescent athletes with LBP [26]. Conservative management of spondylolysis/spondylolisthesis results in successful outcomes for the majority of patients [24].
Idiopathic scoliosis was the fifth most frequent etiology in our case series. It is observed in 1–3% of children and adolescents [27]. Although it is widely believed that scoliosis is capable of causing LBP, no definite relationship between scoliosis and LBP has been proved yet. A recent systematic review reported that the prevalence of LBP in those adolescents with scoliosis is similar to those without [28].
The sixth most frequent etiology was Scheuermann Disease in our case series. The incidence of Scheuermann Disease is 1–8% of the general population [29]. It may involve both the thoracic and lumbar spine. Lumbar spine involvement is characteristically associated with more pain than thoracic involvement [30]. Before bone maturation, using brace and physiotherapy is effective in reducing pain and stopping progress.
In conclusion, LBP is common seen in the child-adolescent age group. It is frequently non-specific and self-limiting, but most of the causes appearing in adulthood may also be seen. In the literature, the risk factors for LBP are controversial. The etiology of LBP should be identified and treated in this age group due to the possibility of it to persist into adulthood.
Footnotes
Ethics Committee Approval: The Fatih Sultan Mehmet Training and Research Hospital Ethics Committee granted approval for this study (date: 18.05.2017, number: 10028).
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
Authorship Contributions: Concept – OGI; Design – OGI, PA, FEBU; Supervision – FUO; Materials – OGI, PA; Data collection and/or processing – OGI, FEBU; Analysis and/or interpretation – OGI, PA, FEBU; Literature review – OGI; Writing – OGI; Critical review – IA, FUO.
REFERENCES
- 1.Kordi R, Rostami M. Low back pain in children and adolescents:an algorithmic clinical approach. Iran J Pediatr. 2011;21:259–70. [PMC free article] [PubMed] [Google Scholar]
- 2.Cakmak A, Yücel B, Ozyalçn SN, Bayraktar B, Ural HI, Duruöz MT, et al. The frequency and associated factors of low back pain among a younger population in Turkey. Spine (Phila Pa 1976) 2004;29:1567–72. doi: 10.1097/01.brs.0000131432.72531.96. [DOI] [PubMed] [Google Scholar]
- 3.Jones MA, Stratton G, Reilly T, Unnithan VB. A school-based survey of recurrent non-specific low-back pain prevalence and consequences in children. Health Educ Res. 2004;19:284–9. doi: 10.1093/her/cyg025. [DOI] [PubMed] [Google Scholar]
- 4.Calvo-Muñoz I, Gómez-Conesa A, Sánchez-Meca J. Physical therapy treatments for low back pain in children and adolescents:a meta-analysis. BMC Musculoskelet Disord. 2013;14:55. doi: 10.1186/1471-2474-14-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.O'Sullivan PB, Beales DJ, Smith AJ, Straker LM. Low back pain in 17 year olds has substantial impact and represents an important public health disorder:a cross-sectional study. BMC Public Health. 2012;12:100. doi: 10.1186/1471-2458-12-100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Harreby M, Nygaard B, Jessen T, Larsen E, Storr-Paulsen A, Lindahl A, et al. Risk factors for low back pain in a cohort of 1389 Danish school children:an epidemiologic study. Eur Spine J. 1999;8:444–50. doi: 10.1007/s005860050203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Salminen JJ. The adolescent back. A field survey of 370 Finnish schoolchildren. Acta Paediatr Scand Suppl. 1984;315:1–122. [PubMed] [Google Scholar]
- 8.Balagué F, Dutoit G, Waldburger M. Low back pain in schoolchildren. An epidemiological study. Scand J Rehabil Med. 1988;20:175–9. [PubMed] [Google Scholar]
- 9.Beighton P, Grahame R. Hypermobility of joints. 2nd ed. Springer Berlin Heidelberg New York. 1989 [Google Scholar]
- 10.Clinch J, Deere K, Sayers A, Palmer S, Riddoch C, Tobias JH, et al. Epidemiology of generalized joint laxity (hypermobility) in fourteen-year-old children from the UK:a population-based evaluation. Arthritis Rheum. 2011;63:2819–27. doi: 10.1002/art.30435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.de SáPinto AL, de Barros Holanda PM, Radu AS, Villares SM, Lima FR. Musculoskeletal findings in obese children. J Paediatr Child Health. 2006;42:341–4. doi: 10.1111/j.1440-1754.2006.00869.x. [DOI] [PubMed] [Google Scholar]
- 12.Paulis WD, Silva S, Koes BW, van Middelkoop M. Overweight and obesity are associated with musculoskeletal complaints as early as childhood:a systematic review. Obes Rev. 2014;15:52–67. doi: 10.1111/obr.12067. [DOI] [PubMed] [Google Scholar]
- 13.Minghelli B, Oliveira R, Nunes C. Postural habits and weight of backpacks of Portuguese adolescents:Are they associated with scoliosis and low back pain? Work. 2016;54:197–208. doi: 10.3233/WOR-162284. [DOI] [PubMed] [Google Scholar]
- 14.Masiero S, Carraro E, Celia A, Sarto D, Ermani M. Prevalence of nonspecific low back pain in schoolchildren aged between 13 and 15 years. Acta Paediatr. 2008;97:212–6. doi: 10.1111/j.1651-2227.2007.00603.x. [DOI] [PubMed] [Google Scholar]
- 15.Morris SL, O'Sullivan PB, Murray KJ, Bear N, Hands B, Smith AJ. Hypermobility and Musculoskeletal Pain in Adolescents. J Pediatr. 2017;181:213–21. e1. doi: 10.1016/j.jpeds.2016.09.060. [DOI] [PubMed] [Google Scholar]
- 16.Fairbank JC, Pynsent PB, Van Poortvliet JA, Phillips H. Influence of anthropometric factors and joint laxity in the incidence of adolescent back pain. Spine (Phila Pa 1976) 1984;9:461–4. doi: 10.1097/00007632-198407000-00007. [DOI] [PubMed] [Google Scholar]
- 17.Bono CM. Low-back pain in athletes. J Bone Joint Surg Am. 2004;86:382–96. doi: 10.2106/00004623-200402000-00027. [DOI] [PubMed] [Google Scholar]
- 18.Sjolie AN. Associations between activities and low back pain in adolescents. Scand J Med Sci Sports. 2004;14:352–9. doi: 10.1111/j.1600-0838.2004.377.x. [DOI] [PubMed] [Google Scholar]
- 19.Mohseni-Bandpei MA, Bagheri-Nesami M, Shayesteh-Azar M. Nonspecific low back pain in 5000 Iranian school-age children. J Pediatr Orthop. 2007;27:126–9. doi: 10.1097/BPO.0b013e3180317a35. [DOI] [PubMed] [Google Scholar]
- 20.Gennari JM, Themar-Noel C, Panuel M, Bensamoun B, Deslandre C, Linglart A, et al. French Society of Spine Surgery (SFCR). Adolescent spinal pain:The pediatric orthopedist's point of view. Orthop Traumatol Surg Res. 2015;101:S247–50. doi: 10.1016/j.otsr.2015.06.012. [DOI] [PubMed] [Google Scholar]
- 21.Kumar R, Kumar V, Das NK, Behari S, Mahapatra AK. Adolescent lumbar disc disease:findings and outcome. Childs Nerv Syst. 2007;23:1295–9. doi: 10.1007/s00381-007-0370-1. [DOI] [PubMed] [Google Scholar]
- 22.Karademir M, Eser O, Karavelioglu E. Adolescent lumbar disc herniation:Impact diagnosis, and treatment. J Back Musculoskelet Rehabil. 2017;30:347–52. doi: 10.3233/BMR-160572. [DOI] [PubMed] [Google Scholar]
- 23.Houghton KM. Review for the generalist:evaluation of low back pain in children and adolescents. Pediatr Rheumatol Online J. 2010;8:28. doi: 10.1186/1546-0096-8-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Klein G, Mehlman CT, McCarty M. Nonoperative treatment of spondylolysis and grade I spondylolisthesis in children and young adults:a meta-analysis of observational studies. J Pediatr Orthop. 2009;29:146–56. doi: 10.1097/BPO.0b013e3181977fc5. [DOI] [PubMed] [Google Scholar]
- 25.Herman MJ, Pizzutillo PD, Cavalier R. Spondylolysis and spondylolisthesis in the child and adolescent athlete. Orthop Clin North Am. 2003;34:461–7. doi: 10.1016/s0030-5898(03)00034-8. [DOI] [PubMed] [Google Scholar]
- 26.Micheli LJ, Wood R. Back pain in young athletes. Significant differences from adults in causes and patterns. Arch Pediatr Adolesc Med. 1995;149:15–8. doi: 10.1001/archpedi.1995.02170130017004. [DOI] [PubMed] [Google Scholar]
- 27.Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA. Adolescent idiopathic scoliosis. Lancet. 2008;371:1527–37. doi: 10.1016/S0140-6736(08)60658-3. [DOI] [PubMed] [Google Scholar]
- 28.Balagué F, Pellisé F. Adolescent idiopathic scoliosis and back pain. Scoliosis Spinal Disord. 2016;11:27. doi: 10.1186/s13013-016-0086-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lowe TG. Scheuermann's kyphosis. Neurosurg Clin N Am. 2007;18:305–15. doi: 10.1016/j.nec.2007.02.011. [DOI] [PubMed] [Google Scholar]
- 30.Afshani E, Kuhn JP. Common causes of low back pain in children. Radiographics. 1991;11:269–91. doi: 10.1148/radiographics.11.2.1827529. [DOI] [PubMed] [Google Scholar]