

Abstract
Continuous glucose monitoring is poised to radically change the treatment of diabetes and patient engagement of those afflicted with this disease. This article will provide an overview of CGM and equip health care providers to begin integrating this technology into their clinical practice.
Continuous glucose monitoring (CGM) systems are more than just glucose monitors. Recent CGM systems have moved beyond mere blood glucose monitoring (BGM) by providing both real-time and predictive glycemic data. The robust data garnered from CGM can also be used for detection of trends, identification of asymptomatic events, and review of glycemic variability over a range of time.
Increased frequency of glucose monitoring is associated with decreased hypoglycemia and increased glycemic time in range (TIR), which correlates with improved A1C (1). Moreover, glucose patterns captured via CGM data analysis can highlight areas in need of treatment intervention (e.g., to prevent hypoglycemia, improve glycemic control at specific times of day, and increase overall TIR). As is well known, the A1C test provides an indication of average glycemic control over the previous 2–3 months. However, it does not capture glycemic variability; thus, individuals who have the same A1C may have vastly different glucose ranges (2,3). CGM can be a good option for patients with inconsistent or confounding glycemic control, who desire engagement in their own disease management, or whose treatment plan puts them in danger of hypoglycemia.
Health care providers (HCPs) can implement two different modalities of CGM. They may prescribe a personal CGM device, which a patient can use either continuously or intermittently, or they may purchase for their practices professional CGM systems that can be sent home with a patient for a brief period of time for diagnostic purposes. The Medtronic iPro2 and the FreeStyle Libre Pro are professional CGM systems for which data are blinded to the patient. The data are uploaded in the HCP’s office for retrospective review with the patient. The Dexcom G6 professional CGM system can be prescribed in blinded and unblinded modes. HCPs may use the unblinded option to help patients increase their awareness of their own glucose levels and make real-time treatment decisions.
The data collected by these devices and either downloaded in the clinic or transmitted remotely allow for visualization of a patient’s true glycemic picture and the effects of current interventional treatments. CGM data also give HCPs insight into patients’ behaviors and glycemic patterns and may reveal previously undetected issues such as hypoglycemia (2,3). Retrospective review of CGM data can reveal therapeutic impacts on glucose management, aid in making treatment decisions, and provide opportunities for education.
Professional CGM systems have been used clinically to measure the effects of variables over an intermittent or specific time interval, such as 3 days or 2 weeks. More specifically, such CGM has been used to evaluate the effects of various interventions, behaviors, and therapies, including the effects of foods or various types of exercise and medication titration (4–7).
The abundance of data gathered via CGM can be reviewed and interpreted through the ambulatory glucose profile (AGP) report, a standardized CGM report that provides a graphical and quantitative display of glycemic activity. The AGP visually displays the dynamics of glycemic activity, including periods of hypoglycemia, glycemic excursions (both high and low), TIR, and recurring glucose patterns, all of which are meaningful metrics for guiding comprehensive diabetes management.
From the patient perspective, CGM offers the benefit of real-time glycemic monitoring with glucose trend information indicated by directional arrows. These trend arrows are a visual display of the direction of glycemic activity (i.e., whether the current glucose level is rising, stable, or decreasing) (8). The visual display of CGM data allows patients to view their glycemic activity and monitor the effects of different types of food, timing of meals, activity levels, stress, and illness. This opportunity facilitates increased patient engagement with diabetes management. Having glucose data readily available is also relevant for loved ones and caregivers of people with diabetes, allowing them to better assist in care and offering them peace of mind with regard to hypoglycemia and hyperglycemia.
Integrating CGM into clinical practice can be challenging for several reasons. Common issues reported include data overload, increased clinic staff time, and the need for HCP education on data interpretation (9,10). Orienting practice staff to the use of CGM technology and downloading reports to a standalone computer and printer that are separate from restrictive administrative firewalls can streamline analysis of CGM data.
Although there can be some barriers to CGM use, there is also strong evidence for its utility in patients with either type 1 or type 2 diabetes and with either personal or professional CGM systems (11). Patient benefits include improvement in A1C, reductions in hypoglycemia and glycemic variability, and greater treatment satisfaction and improved sense of mental well-being (12–15).
One solution to overcoming barriers is intermittent use, of personal or professional CGM, from every other week to perhaps every 6 months, followed by office review of the AGP report (16). This option permits an overview of the glycemic picture at important intervals, such as during lifestyle intervention or after medication changes. In addition, reviewing the AGP report with a patient offers an HCP the opportunity for patient education and a means of encouraging communication and shared decision-making.
This article is intended to equip HCPs to effectively incorporate CGM into clinical practice by reviewing the overwhelming benefits of this technology and the strategies available to overcome therapeutic inertia with regard to its use. Practical tips and tools for streamlining the use of CGM are provided to maximize patients’ office visits through concise, proficient interpretation of CGM data. Topics include how to efficiently review and share the information displayed on the AGP report, how to interpret and act on that information, and how to bill for CGM use and data interpretation services.
CGM Options
Several options exist for both professional and personal CGM (Table 1). Differences among the available systems include varying need for calibration with fingerstick BGM, differing software and phone applications (apps) for data showing and interpretation, and differing sensor warm-up periods and wear times. In addition, the FreeStyle Libre system requires the user to “swipe,” or scan, the receiver or a smartphone over the sensor to obtain a reading. This type of system is sometimes referred to as “flash CGM.” All the systems shown in Table 1 provide software that allows results to be accessed by HCPs and patients, which can be useful for both educational and treatment purposes. For patients using a dedicated reader that comes with their device, data can be downloaded in the clinic or at home by patients using a cable that connects the reader to a computer. For patients using the system’s app on a mobile device, data are automatically uploaded to the Cloud, allowing HCPs to view data at any time by logging into an HCP portal.
TABLE 1.
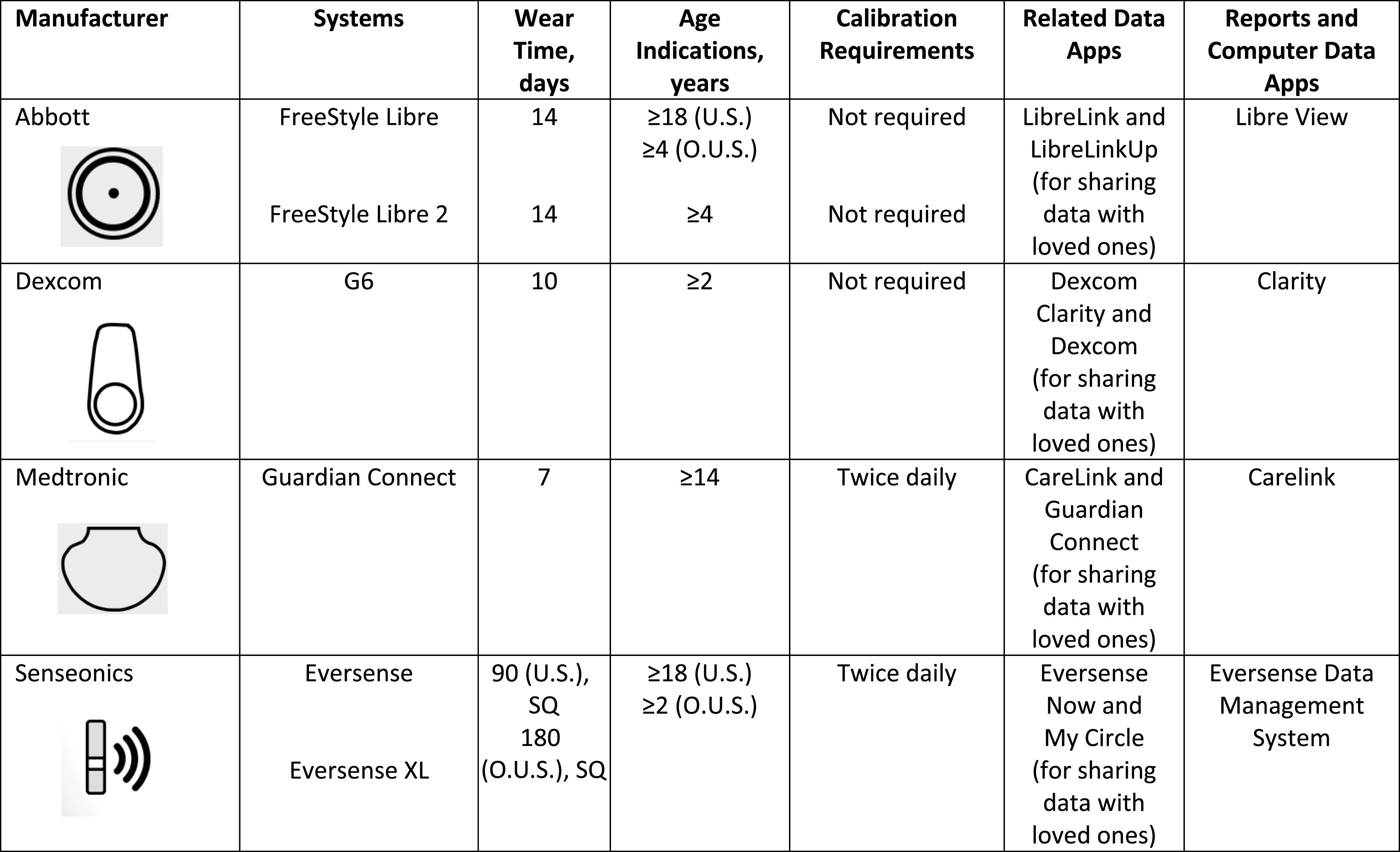 |
Indications vary by country. O.U.S., outside of the United States; SQ, subcutaneously; U.S., in the United States.
Latest-generation models of CGM systems also have features that allow them to work with smart devices. For example, the Dexcom G6 sends glucose readings to a smart mobile device or to the Dexcom receiver every 5 minutes (17). The FreeStyle Libre can also be used with a smart mobile device. The Medtronic Guardian Connect system can connect with the Sugar.IQ app, which can give users insights into their data (18,19). The FreeStyle Libre 2 provides glucose values every minute, with optional real-time high and low alarms.
For those seeking an option with extended monitoring time, the Eversense system provides real-time glucose monitoring every 5 minutes for up to 90 days (180 days outside of the United States) (20). A noteworthy feature of this system is the small, implantable fluorescence-based sensor, which is placed just below a patient’s skin by a specially trained physician (20). The sensor is powered by a removable transmitter that sits on the upper arm (20). The transmitter receives a light signal that is converted into a glucose reading and sent wirelessly every 5 minutes to a mobile app (20).
It is worth clarifying the differences among the three FreeStyle Libre CGM products. The FreeStyle Libre is a flash CGM that requires users to scan the sensor with a reader or smartphone to view data (21). The FreeStyle Libre Pro is a professional system that may be prescribed for short-term professional use. The FreeStyle Libre 2 was recently approved for use in the United States. Its sensor transmits glucose data every minute to the reader, which will alarm if the glucose crosses a user's preset threshold. However, swiping is required to visualize the glucose data (22).
Patient Selection
Personal CGM
Ideal candidates for personal CGM use would be individuals who need or want more engagement with their diabetes management. For those at risk for hypoglycemia such as patients using sulfonylureas, basal insulin, mealtime insulin, or insulin pumps, CGM systems that have alarms such as the Dexcom G6, Medtronic Guardian Connect, Eversense, or FreeStyle Libre 2 would be preferred because they all offer real-time glucose alerts. Other candidates for CGM would be patients with advanced age or complex patients with comorbid and additional chronic diseases who may be at increased risk for hypoglycemia and hospitalization for complications related to glucose control. In addition, individuals with poorly managed diabetes would benefit from real-time monitoring combined with education about the effects of diet, activity, and medications on glycemic management. Outside of the United States, the FreeStyle Libre, Dexcom G6, and Medtronic Guardian systems are approved for use in pregnant women; however, at this time no personal CGM devices are approved for such use in the United States.
CGM would not be suitable for individuals who are dehydrated, hypotensive, in shock, or in a hyperglycemic-hyperosmolar state with or without ketosis; for neonates; or for diagnosis or screening of diabetes (21). In many of these circumstances, interstitial fluid glucose measurements may not be reliable because of body fluid shifts. Table 1 includes information on age-group indications for each available system. The FreeStyle Libre 14-day system is not recommended for patients with hypoglycemia unawareness because it does not have real-time high or low glucose alarms (21,22).
Professional CGM
In a professional capacity, CGM can be reviewed retrospectively to gather information about glycemic activity in multiple scenarios. Ideal patients for this method are those whose A1C is not in the target range, those with increased risk for hypoglycemia, and those not ready to use a CGM system full time but who may still benefit from periodically collected CGM data. This information would be also valuable when considering insulin dosing and meal composition and for calculating a patient’s insulin-to-carbohydrate (I:C) ratio (the number of grams of consumed carbohydrate that 1 unit of insulin will cover).
Scanning and Viewing Practices With CGM Systems
Interacting with a CGM sensor by scanning a flash device or viewing data on a real-time system is crucial for data retrieval and optimal patient benefit. With the Dexcom, Senseonics, and Medtronic systems, as well as the FreeStyle Libre 2, the sensor has a transmitter that sends data to a reader or smartphone app at regular intervals (every 5 minutes with the Dexcom, Senseonics, and Medtronic systems and every 1 minute with the FreeStyle Libre 2). With the first-generation FreeStyle Libre, there is no transmitter, so scanning is always required; therefore, there are no alerts for high or low glucose readings. With the newer FreeStyle Libre 2, the transmitter sends alerts to the reader or app for critical values, but scanning is still required for routinely viewing glucose levels.
The Freestyle Libre requires users to scan it a minimum of once every 8 hours to capture all of the data because the on-body sensor only stores 8 hours of glucose data at a time. Frequent scanning provides favorable benefits such as improved overall TIR and decreased hypoglycemia and A1C (23–25). In an international study of patients who averaged 16 scans per day, higher frequency scanning yielded significantly better glycemic outcomes compared with low-frequency scanning, a result that was consistent across the various countries in the study (23). Moreover, reductions in A1C occur early with use of the FreeStyle Libre system and are sustained over time (26). Effects on hypoglycemia occur as early as within the first 48 hours of sensor use, with further hypoglycemia reduction in the ensuing week (23). Patients can also benefit economically because there is no additional cost for frequent scanning or viewing sensor glucose information compared with fingerstick BGM, which requires a new test strip for each reading. Table 2 describes various scanning and viewing strategies for CGM users (8).
TABLE 2.
Recommendations for Personal Scanning or Viewing of CGM Data (8)
| Scenario | Recommended Timing | Rationale |
|---|---|---|
| Morning | On waking | Facilitates completed stream of readings and retrospective review of previous night’s glucose trends. For FreeStyle Libre users, a gap in data may be present if sleeping >8 hours. |
| Premeal | Before each meal | Current readings and trend arrows inform mealtime insulin dose calculations and timing of insulin injections around meals. |
| Postmeal | 2 hours after each meal | Enables evaluation of mealtime treatment and determination of the need for corrective action. |
| Bedtime | Before sleep | Enables evaluation of current glucose reading and trend arrow to determine whether corrective action is needed to prevent nocturnal hypoglycemia or hyperglycemia. |
| Sick day | Every 4 hours | Allows for monitor of the effects of illness on glucose levels. Note that vitamin C and salicylic acid (aspirin) may affect the accuracy of readings with the FreeStyle Libre and Medtronic systems. |
| Exercise | Every 15–30 minutes | Can prevent hypoglycemia during and after exercise. |
How to Use CGM Data
Trend arrows displayed on CGM systems provide predictive cues about glycemic activity and the direction in which the glucose level is trending. There are several ways to use these trend arrows to monitor and manage treatment. Patients view their data at predetermined times of the day, such as first thing in the morning, before and after meals, and at bedtime. This strategy is similar to a fingerstick BGM approach. When viewing data after meals, users can evaluate their treatment decisions and their rate of glycemic change after a meal. These results would be helpful for stimulating discussions with patients about the content and timing of meals.
To benefit from trend arrows, patients must be instructed on how to correctly read and act on these cues. Education should include actively showing patients the trend arrow icons on their CGM reader and discussing what each one indicates. Next, patients should be instructed on how to react to the trend arrows, such as through medication adjustment, change in activity level, or actions to prevent hypoglycemia. Table 3 provides a guide of understanding trend arrows (27–29).
TABLE 3.
| Medtronic Arrow | Dexcom Arrow | FreeStyle Libre Arrow | Trend Meaning | Glucose Value in 30 Minutes* |
|---|---|---|---|---|
| ↑↑↑ | ↑↑ | NA | Glucose is rising very quickly, >3 mg/dL/min | >90 mg/dL higher |
| ↑↑ | ↑ | ↑ | Glucose is rising quickly, 2–3 mg/dL/min (>2 mg/dL/min with FreeStyle Libre) | 60–90 mg/dL higher (>60 mg/dL for FreeStyle Libre) |
| ↑ | ↗ | ↗ | Glucose is rising 1–2 mg/dL/min | 30–60 mg/dL higher |
| No arrow | → | → | Glucose is changing slowly, <1 mg/dL/min | <30 mg/dL |
| ↓ | ↘ | ↘ | Glucose is falling 1–2 mg/dL/min | 30–60 mg/dL lower |
| ↓↓ | ↓ | ↓ | Glucose is falling quickly, 2–3 mg/dL/min (>2 mg/dL/min with FreeStyle Libre) | 60–90 mg/dL lower (>60 mg/dL for FreeStyle Libre) |
| ↓↓↓ | ↓↓ | NA | Glucose is falling very quickly, >3 mg/dL/min | >90 mg/dL lower |
Predicted 30-minute change in glucose is illustrative. NA, not applicable.
Trend arrows may be used to make insulin dose adjustments for CGM users who are prescribed bolus insulin (8,30). Many people with diabetes dose their mealtime insulin based on two factors: the carbohydrates in the food they are about to eat (using their I:C ratio) and their need for correctional insulin to bring their current premeal glucose level into the target range (based on an individualized insulin sensitivity factor [ISF], which is the blood glucose lowering in mg/dL to be expected per unit of rapid-acting insulin delivered when glucose is above target). Suppose a person who is about to consume 60 g carbohydrates has an I:C ratio of 1:15; that person would need 4 units of insulin to cover the carbohydrate content of the meal. However, if that person’s premeal glucose is 200 mg/dL (target 150 mg/dL) and the person’s ISF is 50 (i.e., 1 unit of insulin will lower above-target glucose by 50 mg/dL), that person would need an additional unit of correctional insulin. Thus, the total calculated bolus insulin dose before the meal would be 5 units.
With CGM, bolus insulin doses can be more carefully fine-tuned. Table 4 shows how trend arrows can better inform mealtime and correctional insulin dosing for FreeStyle Libre and Dexcom CGM users. For example, in the case of a FreeStyle Libre user with the same parameters described above, the trend arrow adjustment for a downward arrow would be −1.5 units. Therefore, the total calculated dose would be 5 units − 1.5 units = 3.5 units. The user should then round down to the nearest whole number and deliver a total of 3 units. In contrast, the adjustment for an upward trend arrow would be +1.5 units. Thus, the calculated dose would be 1.5 + 5 = 6.5, and the person should then round down to the nearest whole number and delivery a total of 6 units.
TABLE 4.
Insulin Dose Adjustments Using FreeStyle Libre and Dexcom CGM Systems in Adults: Before and ≥4 Hours After Meals (8,30)
| CGM System | User’s Personalized ISF, mg/dL | ||||
|---|---|---|---|---|---|
| FreeStyle Libre Arrow | Dexcom Arrow | <25 | 25 to <50 | 50 to <75 | ≥75 |
| NA | ↑↑ | +4.5 units | +3.5 units | +2.5 units | +1.5 units |
| ↑ | ↑ | +3.5 units | +2.5 units | +1.5 units | +1.0 units |
| ↗ | ↗ | +2.5 units | +1.5 units | +1.0 units | +0.5 units |
| → | → | No adjustment | No adjustment | No adjustment | No adjustment |
| ↘ | ↘ | −2.5 units | −1.5 units | −1.0 units | −0.5 units |
| ↓ | ↓ | −3.5 units | −2.5 units | −1.5 units | −1.0 units |
| NA | ↓↓ | −4.5 units | −3.5 units | −2.5 units | −1.5 units |
NA, not applicable.
One can easily see how the trend arrow can considerably alter insulin dosing. Trend arrow adjustments should not be made when the trend arrow is not stable, which is often the case in the first 4 hours after a meal.
Reviewing and Interpreting the AGP Report
The AGP report can also be reviewed with patients in the office or through telemedicine platforms to further their understanding of glycemic patterns. For patients who use a mobile device as their CGM reader, the data are automatically uploaded to the Cloud, and automatic sharing with the HCP can be set up. For patients who use the dedicated CGM reader that comes with their CGM system, the reader must be plugged into a remote computer connected to the Internet or to a computer in the HCP office for data downloading.
Extracting the insights from an AGP report and using those insights to improve the care of a person with diabetes can be very rewarding. An article elsewhere in this special-topic issue of Clinical Diabetes (p. 439) further explores the effective use of CGM data.
Briefly, the most useful data elements for clinical decision-making are summarized in Table 5 (31). First, it is a good idea to see how often a patient is wearing and using the CGM device. If sensor usage is low, the HCP can address any barriers. Next, the HCP can look at the glucose management indicator (GMI), which is a new term for estimated A1C based on CGM data. The coefficient of variation (calculated from the blood glucose mean and SD and expressed as %CV) gives a measure of glucose variability and, if high, suggests an increased risk of hypoglycemia.
TABLE 5.
Recommended Clinical Targets for CGM Parameters and Potential Interventions (31)
| Metric | Target for Most People With Diabetes | Target for Older and Higher-Risk Individuals | Actions If Out of Target |
|---|---|---|---|
| CGM usage | 14 of the past 14 days; active 70% of the time | 14 of the past 14 days; active 70% of the time | Explore patient barriers to CGM use |
| Average glucose | GMI <7% | GMI <8% | Review glucose range bar graph |
| Glucose variability | %CV ≤36% | %CV ≤36% | Review glucose range bar graph |
| Glucose ranges | TIR (70–180 mg/dL) >70% or 17 hours/day | TIR (70–180 mg/dL) >50% or 12 hours/day | Is there hyperglycemia or hypoglycemia? Address hypoglycemia first. |
| TBR (<70 mg/dL) <4% or 1 hours/day; TBR (<54 mg/dL) <1% or 15 minutes/day | TBR (<70 mg/dL) <1% or 15 minutes/day | Identify and adjust contributing medications such as sulfonylureas, basal insulin, and bolus insulin. Explore self-management issues such as exercise, missed meals, and insulin dosing. | |
| TAR (>180 mg/dL) <25% or 6 hours/day; TAR (>250 mg/dL) <5% or 1 hour/day | TAR (>250 mg/dL) <10% or 2.5 hours/day | Is the hyperglycemia fasting or post-meal? Consider medication adjustments. Explore self-management issues such as food choices and insulin dosing. |
TAR, time above range; TBR, time below range.
The targets for the various glucose ranges are listed in Table 5. For most people with diabetes, being in the range of 70–180 mg/dL for >70% of the time is desirable. For elderly or frail patients at higher risk of hypoglycemia, the TIR target may be reduced to >50%. If there is significant hypoglycemia or hyperglycemia, reviewing the individual daily patterns may help in discerning the need for changes to the treatment regimen versus optimization of self-management behaviors.
The AGP can serve as a powerful tool for education about diabetes self-management. A practical approach that has worked in our office is to save the AGP report as a jpg or pdf file, which can be viewed on screen in color if a color printer is not available. This file can be printed for the patient, embedded into the chart, or shared via e-mail with patient permission. Clinicians can highlight areas of focus, develop a personalized diabetes action plan, and provide a copy for the patient to take home after the visit as a tangible takeaway for action. Engaging patients in discussion by asking what they see in their AGP report and seeking their input on potential solutions and action plans is helpful. The same AGP report can be used for medical record purposes and to document Current Procedural Terminology (CPT) billing codes and modifiers when interpretation is involved (Table 6).
TABLE 6.
Common Billing Codes for Personal and Professional CGM Visits and Services (32)
| CPT Code | Type of Service | Provider | Frequency | Encounter Type |
|---|---|---|---|---|
| 95249 | Personal CGM (initial startup and training) | RN, PharmD, RD, CDCES, or MA (if within scope) under the supervision of a physician, advanced practitioner, or hospital outpatient department | Once during the time the patient owns the device or if transiting to a new device | Face-to-face visit |
| 95250 | Professional CGM (startup, training, application, removal, and printout) | RN, PharmD, RD, CDCES, or MA (if within scope) under the supervision of a physician, advanced practitioner, or hospital outpatient department | Maximum once per month | Face-to-face visit |
| 95251 | CGM data interpretation | Physician, NP, PA, or CNS | Monthly* | Non–face-to-face visit |
| −25 modifier | Separate identifiable service | Physician, NP, PA, or CNS | With office visits | Face-to-face visit |
Time intervals for data analysis reimbursement may vary by payer organization.
Insurance Coverage and Reimbursement for CGM
Coverage for Patients
Insurance coverage for personal CGM varies by type of insurance (commercial, Medicare, or Medicaid). For Medicare, CGM must meet certain requirements to be eligible for durable medical equipment (DME) coverage, and prescriptions generally must be filled through Medicare DME–approved distributors. Reimbursement criteria require CGM to be therapeutic, meaning that no confirmatory fingerstick BGM will be required for therapeutic decision-making; the three CGM systems that meet this criterion are the Dexcom G6, FreeStyle Libre 14-day, and FreeStyle Libre 2 systems. Additionally, covered CGM systems must have a DME component (i.e., a separate durable medical device) and supplies covered as part of DME. Medicare will provide reimbursement for a device “bundle” depending on the CGM model selected. For example, the FreeStyle Libre reader and a 1-month supply of sensors would be a covered bundle.
Currently, Medicare will cover CGM for therapeutic monitoring of blood glucose in cases meeting the following criteria: 1) the patient has diabetes (type 1 or type 2), 2) the patient has an insulin regimen that requires frequent adjustment on the basis of BGM or CGM, 3) the patient’s insulin regimen involves at least three injections per day or the use of an insulin pump, 4) the patient is checking blood glucose at least four times daily, and 5) the clinician has in-person visits with the patient every 6 months after initial prescription of CGM to assess adherence to the CGM regimen and diabetes treatment plan. For Medicaid, most plans currently cover CGM for people with type 1 diabetes and will occasionally cover it for patients with type 2 diabetes who are using an insulin pump or a multiple daily injection (MDI) insulin regimen. CGM prescriptions for Medicaid must be sent directly to either a Medicaid participating pharmacy or DME supplier. Private commercial insurance companies frequently cover CGM for people with either type 1 or type 2 diabetes, and these prescriptions often can be submitted directly to pharmacies.
Documentation to support coverage for patients can vary according to payer. Some may require a certificate of medical necessity, whereas others may need documentation of uncontrolled diabetes while using an MDI insulin regimen, insulin-dependent diabetes, participation in a diabetes education program, recurrent hypoglycemia or hypoglycemia unawareness, pregnancy with uncontrolled type 1 diabetes, or blood glucose logs showing results of BGM testing at least four times daily. To streamline the approval process, embedding all such information in the clinical chart notes at the time of the visit will enable a summary of the necessary documentation to be produced most easily. To maintain CGM coverage, documentation should note a patient’s use of CGM continuously to adjust insulin dosing on a daily or weekly basis, make medication adjustments, and prevent hypoglycemia.
Reimbursement for Providers
Billing for CGM services is dependent on two key factors: equipment ownership and data interpretation. Different billing codes apply depending on whether the CGM equipment is owned by the patient (personal CGM) or the physician (professional CGM) (Table 6) (32). A face-to-face encounter may be billed for personal CGM startup and training (CPT code 95249) or for professional CGM startup and training (code 95250) with download of the receiver at the provider’s office. Training and downloading services can be provided by a trained registered nurse (RN), pharmacist (PharmD), registered dietitian (RD), certified diabetes care and education specialist (CDCES), or medical assistant (MA) (if within scope) under the supervision of a physician, advanced practitioner, or hospital outpatient department. These codes may only be used once during the time a patient owns the device or if the patient is transitioned to a new device.
Subsequent CGM data interpretation may be billed only by a physician, nurse practitioner (NP), physician assistant (PA), or clinical nurse specialist (CNS) on a monthly basis (code 95251) and does not require a face-to-face encounter (Table 6). All of these codes require review of a minimum of 72 hours of CGM data to bill for services. Lastly, the −25 modifier may be used if billing for CGM services that are performed on the same day as a problem visit (codes 99212–99215) if a significant and separately identifiable service took place (e.g., if during a regular follow-up visit you perform pre-CGM evaluation in advance of the patient starting a period of professional CGM use, you could use 95250–25).
Telehealth and virtual visits have been rapidly expanding in 2020, and reimbursement requirements and codes are evolving in response. The Centers for Medicare & Medicaid Services (CMS) has defined criteria for reimbursement of telehealth services (33). These criteria include the type of services provided, geographic location, type of institution delivering the services, and type of HCP. The types of telehealth services eligible for reimbursement are divided into four categories: 1) remote patient face-to-face services seen via live video conferencing, 2) non–face-to-face services that can be conducted either through live video conferencing or via store-and-forward telecommunication services, 3) home telehealth services, and 4) remote patient face-to-face, interactive services. In addition to meeting the above criteria, telehealth services must be furnished via an interactive telecommunications system by a physician or authorized HCP to an individual eligible for telehealth services, and the individual receiving the service must be located in a telehealth-originating site (e.g., a remote visit with an eligible patient at a rural health care clinic). List of Medicare telehealth services by CPT or Healthcare Common Procedure Coding System codes are available on the CMS website (33).
Before 6 March 2020, Medicare could only pay clinicians for telehealth services such as routine visits in certain circumstances (e.g., for beneficiaries living in a rural area who had to travel to a local medical facility to get tele-health services from a doctor in a remote location rather than receive telehealth services in their home) (34). However, because of the coronavirus 2019 (COVID-19) outbreak, telehealth services were expanded to permit telehealth visits from any health care facility, including a physician’s office, hospital, nursing home, or rural health clinic, as well as from patient homes and regardless of the diagnosis. This was an important change that allowed patients to maintain social distancing guidelines to reduce the risk of COVID-19 transmission. It will be of interest to see how the availability of telemedicine and the ability to remotely access CGM continue to shape the future of health care delivery and diabetes management.
Conclusion: Opportunities for Improving Outcomes
CGM systems go beyond A1C and fingerstick BGM by bringing glycemic monitoring out of the past, into the present, and looking toward the future. Patients who use CGM have the opportunity to increase their awareness of their own glycemic responses and engagement in the management of their own disease. They can monitor the effects of different foods, times of day, activity levels, and illness on their blood glucose levels. CGM is also beneficial for patients’ caregivers and loved ones who participate in diabetes management. HCPs who incorporate these systems into their clinical practice will gain a valuable tool that provides a comprehensive view of glycemic events, trends, and patterns, enabling them to effectively intervene to improve their patients’ diabetes management and outcomes.
Article Information
Acknowledgments
The author acknowledges the editorial assistance of Suzie Webster of ConsignMed, Inc.
Funding
The articles in this special-topic issue of Clinical Diabetes were supported by unrestricted educational grants to the American Diabetes Association from Abbott Diabetes Care and Dexcom.
Duality of Interest
No potential conflicts of interest relevant to this article were reported.
Footnotes
The publication of this special-topic issue of Clinical Diabetes was supported by unrestricted educational grants to the American Diabetes Association from Abbott Diabetes Care and Dexcom.
References
- 1.Lang J, Jangam S, Dunn T, Hayter G. Expanded real-world use confirms strong association between frequency of flash glucose monitoring and glucose control [Abstract ATTD19-0299] Diabetes Technol Ther 2019;21(Suppl. 1):A40 [Google Scholar]
- 2.Wright EE Jr, Gavin JR 3rd. Clinical use of professional continuous glucose monitoring. Diabetes Technol Ther 2017;19(Suppl. 2):S12–S15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Distiller LA, Cranston I, Mazze R. First clinical experience with retrospective flash glucose monitoring (FGM) analysis in South Africa: characterizing glycemic control with ambulatory glucose profile. J Diabetes Sci Technol 2016;10:1294–1302 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Powers MA, Cuddihy RM, Wesley D, Morgan B. Continuous glucose monitoring reveals different glycemic responses of moderate- vs high-carbohydrate lunch meals in people with type 2 diabetes. J Am Diet Assoc 2010;110:1912–1915 [DOI] [PubMed] [Google Scholar]
- 5.Bashir M, Elhadd T, Ali H, et al. A pilot study using flash continuous glucose monitoring in patients with type-2 diabetes on multiple anti-diabetic agents during Ramadan. Diabetes Metab Syndr 2018;12:965–968 [DOI] [PubMed] [Google Scholar]
- 6.Yardley JE, Kenny GP, Perkins BA, et al. Resistance versus aerobic exercise: acute effects on glycemia in type 1 diabetes. Diabetes Care 2013;36:537–542 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Myette-Côté É, Terada T, Boulé NG. The effect of exercise with or without metformin on glucose profiles in type 2 diabetes: a pilot study. Can J Diabetes 2016;40:173–177 [DOI] [PubMed] [Google Scholar]
- 8.Kudva YC, Ahmann AJ, Bergenstal RM, et al. Approach to using trend arrows in the FreeStyle Libre flash glucose monitoring systems in adults. J Endocr Soc 2018;2:1320–1337 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Heinemann L. Continuous glucose monitoring and clinical trials. J Diabetes Sci Technol 2009;3:981–985 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rodbard D. Continuous glucose monitoring: a review of successes, challenges, and opportunities. Diabetes Technol Ther 2016;18(Suppl. 2):S3–S13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Vigersky R, Shrivastav M. Role of continuous glucose monitoring for type 2 in diabetes management and research. J Diabetes Complications 2017;31:280–287 [DOI] [PubMed] [Google Scholar]
- 12.Jensen MH, Mahmoudi Z, Christensen TF, et al. Evaluation of an algorithm for retrospective hypoglycemia detection using professional continuous glucose monitoring data. J Diabetes Sci Technol 2014;8:117–122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Reddy M, Jugnee N, El Laboudi A, Spanudakis E, Anantharaja S, Oliver N. A randomized controlled pilot study of continuous glucose monitoring and flash glucose monitoring in people with type 1 diabetes and impaired awareness of hypoglycaemia. Diabet Med 2018;35:483–490 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wood A, O’Neal D, Furler J, Ekinci EI. Continuous glucose monitoring: a review of the evidence, opportunities for future use and ongoing challenges. Intern Med J 2018;48:499–508 [DOI] [PubMed] [Google Scholar]
- 15.Al Hayek AA, Al Dawish MA. The potential impact of the FreeStyle Libre flash glucose monitoring system on mental well-being and treatment satisfaction in patients with type 1 diabetes: a prospective study. Diabetes Ther 2019;10:1239–1248 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hirsch IB, Verderese CA. Professional flash continuous flash glucose monitoring with ambulatory glucose profile reporting to supplement A1C: rationale and practical implementation. Endocr Pract 2017;23:1333–1344 [DOI] [PubMed] [Google Scholar]
- 17.Dexcom Dexcom G6 continuous glucose monitoring system. Available from https://www.dexcom.com/safety-information?utm_source=adwords&utm_campaign=b&sfc=701f3000000athzAAA&msclkid=f1d6ab93940d12cf6b8af49b38a7746f&utm_source=bing&utm_medium=cpc&utm_campaign=SCH_B_US_G6&utm_term=dexcom%206%20blood%20glucose%20monitor&utm_content=G6_Blood-Glucose_PH&dclid=CNai7-uhw-oCFQi8wAodXdoP4A#dexcom-g6-brief. Accessed 20 July 2020
- 18.Medtronic Guardian Sensor 3 continuous glucose monitoring system. Available from https://www.medtronic.com/us-en/healthcare-professionals/products/diabetes/continuous-glucose-monitoring-systems/guardian-sensor-3.html. Accessed 10 July 2020
- 19.Medtronic iPRO2 professional CGM (continuous glucose monitoring). Available from https://www.medtronic.com/us-en/healthcare-professionals/products/diabetes/continuous-glucose-monitoring-systems/ipro2-professional.html. Accessed 1 August 2020
- 20.Senseonics The Eversense CGM system. Available from https://www.eversensediabetes.com/eversense-cgm-system. Accessed 1 August 2020
- 21.Abbott Diabetes Care FreeStyle Libre 14-Day Flash Glucose Monitoring System: User Manual. Alameda, CA, Abbott Diabetes Care, 2018 [Google Scholar]
- 22.Abbott Diabetes Care FreeStyle home page. Available from https://provider.myfreestyle.com/index.html. Accessed 10 July 2020
- 23.Dunn TC, Xu Y, Hayter G, Ajjan RA. Real-world flash glucose monitoring patterns and associations between self-monitoring frequency and glycaemic measures: a European analysis of over 60 million glucose tests. Diabetes Res Clin Pract 2018;137:37–46 [DOI] [PubMed] [Google Scholar]
- 24.Jangum S, Dunn T, Xu Y, Ajjan R. Sustained improvement in glycaemic control following flash glucose monitoring: a worldwide observational analysis [Abstract] Diabetes Technol Ther 2018;20(Suppl. 1):A25 [Google Scholar]
- 25.Haak T, Hanaire H, Ajjan R, Hermanns N, Riveline JP, Rayman G. Flash glucose-sensing technology as a replacement for blood glucose monitoring for the management of insulin-treated type 2 diabetes: a multicenter, open-label randomized controlled trial. Diabetes Ther 2017;8:55–73 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Evans M, Welsh Z, Ells S, Seibold A. The impact of flash glucose monitoring on glycaemic control as measured by HbA1c: a meta-analysis of clinical trials and real-world observational studies. Diabetes Ther 2020;11:83–95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Abbott Diabetes Care FreeStyle Libre 14-day system: getting started guide. Available from https://provider.myfreestyle.com/pdf/Brochure-FSL14D-Patient-Getting-Started%20Guide-HCP-Marketing.pdf. Accessed 1 August 2020
- 28.Dexcom Dexcom G6: using your G6. Available from https://s3-us-west-2.amazonaws.com/dexcompdf/Using-Your-G6.pdf. Access 1 August 2020
- 29.Medtronic Medtronic Guardian Connect system support: glucose trends. Available from https://www.medtronicdiabetes.com/customer-support/guardian-connect-system-support/glucose-trends. Accessed 1 August 2020
- 30.Aleppo G, Laffel LM, Ahmann AJ, et al. A practical approach to using trend arrows on the Dexcom G5 CGM system for the management of adults with diabetes. J Endocr Soc 2017;1:1445–1460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Battelino T, Danne T, Bergenstal RM, et al. Clinical targets for continuous glucose monitoring data interpretation: recommendations from the International Consensus on Time in Range. Diabetes Care 2019;42:1593–1603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Novitas Solutions Medicare jurisdiction H (JH) website. Available from https://www.novitas-solutions.com/webcenter/portal/MedicareJH. Accessed 24 April 2020
- 33.Centers for Medicare & Medicaid Services List of telehealth services. Available from https://www.cms.gov/Medicare/Medicare-General-Information/Telehealth/Telehealth-Codes. Accessed 24 April 2020
- 34.Centers for Medicare & Medicaid Services Telehealth services. Available from https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/TelehealthSrvcsfctsht.pdf. Accessed 24 April 2020