

Editor—Current evidence on coronavirus disease 2019 (COVID-19) shows that the most severely affected patients tend to have higher cytokine concentrations. The so-called cytokine storm was proposed as a rationale to test therapies based on cytokine antagonists and more specifically to interleukin-6 (IL-6). However, further investigations revealed that cytokine levels in COVID-19 are not higher than in other virus-related infections.1 In addition, some data support a potential role for endothelial injury in the pulmonary vascular shunts, extra-pulmonary manifestations, and thrombosis pathogenesis.2 We analysed inflammation and endothelial injury biomarkers with regard to disease severity of critically ill patients with COVID-19 to investigate the potential mechanism of disease progression.
We conducted a single-centre prospective study at Amiens Hospital University (Amiens, France) as an ancillary study of a prospective database of critically ill patients with COVID-19 (registered on ClinicalTrials.gov NCT04354558 and Commission Nationale de l’Informatique et des Libertés number PI2020_843_0026). The population study comprised adult patients admitted to our ICU with a confirmed diagnosis of COVID-19 (RT–PCR diagnosed from nasopharyngeal swab). Severity was defined according to the WHO case definition.3 The severe group included patients with respiratory distress syndrome (rate ≥30 bpm) or oxygen saturation ≤93% at rest or ratio of arterial partial pressure of oxygen to fractional concentration of oxygen in inspired air <300 mm Hg (X kPa), or >50% lesion progression over 24–48 h by pulmonary imaging. The critical group included patients with respiratory failure and requiring mechanical ventilation, or with shock or organ failure that requires ICU care.
Peripheral blood samples were collected on ICU admission in ethylenediamine tetra-acetic acid-containing tubes and centrifuged within 30 min of sampling for 10 min at 1000 × g. Plasma samples were collected and stored at –80°C until use. Cytokine levels were analysed in two-fold diluted plasma samples using ProteinSimple® (San Jose, CA, USA) microfluidic enzyme-linked immunosorbent assay (ELISA) technology, according to the manufacturer's instructions. The inter-assay and intra-assay coefficients of variation for tumour necrosis factor-α (TNF-α) and IL-6 were all <9%. Levels of angiopoietin (Ang)-1 and Ang-2 were determined in five-fold diluted plasma samples using commercially available ELISA kits according to the manufacturer's instructions (ELH-Angiopoietin1 and ELH-Angiopoietin2; RayBiotech, Norcross, GA, USA). Assay sensitivity was 30 pg ml−1 for Ang-1 and 10 pg ml−1 for Ang-2. The inter-assay and intra-assay coefficients of variation for Ang-1 and Ang-2 were all <12%.
From March to May 2020, 65 patients were included in the study: 17 patients in the severe group (26%) and 48 in the critical group (74%). Patient data are reported in Table 1 .
Table 1.
Patient and biological characteristics of COVID-19 patients according to the level of the severity. Ang, angiopoietin; COPD, chronic obstructive pulmonary disease; DVT, deep venous thrombosis; ECMO, extracorporeal membrane oxygenation; IL-6, interleukin-6; MV, mechanical ventilation; PE, pulmonary embolus; RRT, renal replacement therapy; SOFA, sequential organ failure assessment; TNF-α, tumour necrosis factor-alpha; WBC, white blood cell count.
| Variable | Overall population (n=65) | Severe group (n=17) | Critical group (n=48) | P-value |
|---|---|---|---|---|
| Age (yr) | 63 [56–69] | 61 [50–70] | 64 [58–69] | 0.207 |
| Male gender, n (%) | 45 (70) | 11 (65) | 34 (71) | 0.638 |
| BMI (kg m−2) | 29.7 [26.8–33.5] | 28.5 [26.7–34.5] | 29.9 [27.0–33.1] | 0.726 |
| Comorbidities, n (%) | ||||
| Hypertension | 34 (52) | 9 (53) | 25 (52) | 0.951 |
| Dyslipidaemia | 19 (29) | 6 (35) | 13 (27) | 0.547 |
| Severe obesity | 12 (19) | 3 (18) | 9 (19) | 1.000 |
| Smoking | 7 (11) | 1 (6) | 6 (13) | 0.664 |
| Diabetes mellitus | 17 (26) | 3 (18) | 14 (29) | 0.523 |
| Coronary artery disease | 7 (11) | 0 (0) | 7 (15) | 0.176 |
| COPD | 3 (5) | 0 (3) | 3 (6) | 0.559 |
| Days from symptoms onset to hospital admission (days) | 6 [3–8] | 7 [2–8] | 6 [4–8] | 0.938 |
| WBC (mm−3) | 6800 [4700–8900] | 7650 [5350–9390] | 7300 [5200–9870] | 0.874 |
| Lymphocytes (mm−3) | 700 [600–1200] | 710 [600–1100] | 700 [598–1107] | 0.409 |
| C-reactive protein (mg L−1) | 109 [58–241] | 71 [51–137] | 145 [94–234] | 0.013 |
| Creatinine (μmol L−1) | 70 [51–175] | 68 [52–77] | 85 [61–183] | 0.085 |
| D-dimers (ng ml−1) | 1110 [770–2100] | 1065 [790–5915] | 1550 [770–5060] | 0.702 |
| Paco2 (kPa) | 4.53 [4.26–5.33] | 4.93 [4.53–5.20] | 5.07 [4.40–5.87] | 0.410 |
| Pao2 (kPa) | 10.13 [9.20–12.93] | 12.00 [10.00–15.87] | 10.67 [9.20–13.73] | 0.528 |
| Arterial lactate (mmol L−1) | 1.7 [1.3–2.4] | 1.8 [1.2–2.4] | 1.8 [1.6–2.2] | 1.000 |
| SOFA score | 5 [2–9] | 2 [1–4] | 7 [4–12] | <0.0001 |
| Cytokines (pg ml−1) | ||||
| TNF-α | 20.0 [16.2–33.9] | 16.5 [15.6–19.8] | 26.7 [16.7–35.5] | 0.006 |
| IL-6 | 87.3 [31.1–173.0] | 36.4 [27.2–112.0] | 88.9 [42.1–293.0] | 0.038 |
| Angiopoietins (pg ml−1) | ||||
| Ang-1 | 9408 [6583–11783] | 9642 [7650–12243] | 9018 [6461–11598] | 0.221 |
| Ang-2 | 3992 [2188–6731] | 3015 [2054–3473] | 4484 [2408–7169] | 0.025 |
| Ang-2/Ang-1 | 0.49 [0.23–1.11] | 0.22 [0.18–0.57] | 0.57 [0.29–1.14] | 0.028 |
| Duration of MV (days) | NA | NA | 22 [16–32] | NA |
| ICU stay (days) | 18 [8–31] | 5 [3–7] | 25 [14–34] | <0.0001 |
| Hospital stay (days) | 27 [14–38] | 14 [11–21] | 32 [18–43] | <0.0001 |
| RRT, n (%) | 19 (29) | 0 (0) | 19 (40) | 0.001 |
| Vasopressor use, n (%) | 19 (29) | 0 (0) | 19 (40) | 0.003 |
| ECMO, n (%) | 4 (6) | 0 (0) | 4 (8) | 0.03 |
| DVT or PE | 5 (8) | 0 (0) | 5 (10) | 0.023 |
| Discharge from ICU | 53 (82) | 17 (100) | 36 (75) | <0.0001 |
| Discharge from hospital | 52 (80) | 17 (100) | 35 (73) | <0.0001 |
| ICU mortality (%) | 12 (18) | 1 (6) | 11 (23) | 0.088 |
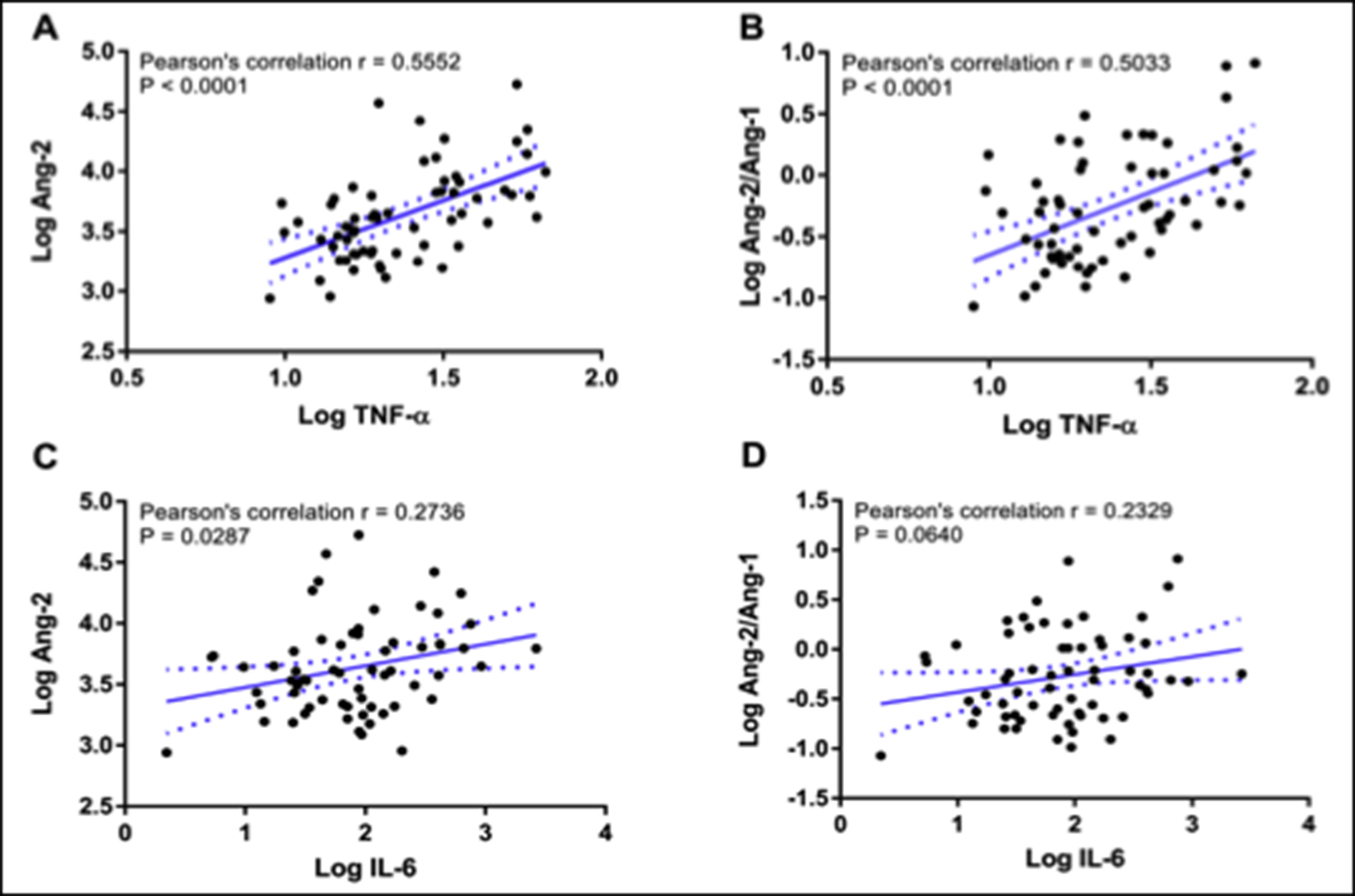
At ICU admission, TNF-α and IL-6 were significantly higher in the critical group in comparison with the severe group (P=0.006 and P=0.038, respectively). Ang-1 did not significantly differ between groups (P=0.221), whereas Ang-2 and Ang-2/Ang-1 were significantly higher in the critical group (P=0.025 and P=0.028, respectively). Ang-2 was positively correlated to IL-6 and TNF-α (P=0.029 and P<0.0001); Ang-2/Ang-1 was correlated to TNF-α (P<0.0001) (Supplementary figure).
In univariate logistic regression analysis, TNF-α, IL-6, Ang-2, and Ang-2/Ang-1 were associated with vasopressor use (P<0.0001, P=0.038, P=0.013, and P=0.041, respectively). The TNF-α and Ang-2 levels were associated with renal replacement therapy (RRT) requirement (P=0.001 and P=0.046, respectively), but not IL-6 or Ang-2/Ang-1. Tumour necrosis factor-α was the only plasma marker associated with in-ICU death (P=0.025) (Supplementary table). After adjustment for clinical severity, only TNF-α was an independent factor associated with vasopressor use (odds ratio [OR]: 54.03; 95% confidence interval [CI]: 1.12–2611), RRT requirement (OR: 142.7; 95% CI: 4.3–4716.1), and in-ICU death (OR: 22.5; 95% CI: 1.1–440.6).
This study has three main findings. First, IL-6, TNF-α, and Ang-2 were increased in the critical group. Second, TNF-α was associated with organ failure and mortality. Third, TNF-α levels correlated with Ang-2. The first finding supports the so-called cytokine storm pathogenesis. Nevertheless, our findings on IL-6 are not in accordance with previous reports. It was suggested that IL-6 is a key factor in COVID-19-associated cytokine response, allowing therapies with IL-6 antagonists, such as tocilizumab. However, the first clinical trials with IL-6 antagonists were disappointing with negative results regarding mortality or disease progression.4 Moreover, a recent meta-analysis confirmed that IL-6 elevation in COVID-19 is actually lower than in other respiratory virus-related diseases.5
In our report, TNF-α was a better correlate of initial severity and progression of ICU stay. Observations from large registries of patients with COVID-19 and with chronic rheumatism or inflammatory bowel diseases suggested that anti-TNF-α therapies may have prevented COVID-19 progression during the outbreak.6 These results confirm the pro-inflammatory state associated with COVID-19 and emphasise the confirmed benefit of corticosteroid therapy on disease progression and mortality in critically ill patients.7
We also assessed endothelial injury with Ang-2 elevation. This result reinforces our previous hypothesis that COVID-19 is, at least partially, a vascular disease with endothelial damage, angiogenesis, and thrombosis.8 Angiopoietin-2 expression can be promoted by different stimuli, including inflammation and hypoxaemia. We confirmed a positive correlation between Ang-2 and TNF-α levels, suggesting endothelial activation induced by inflammation, although an additive effect of tissue hypoxia on Ang-2 release was not excluded.9 Critical patients had higher Ang-2 elevation than less severe patients. Angiopoietin-2, by promoting endothelial permeability, may increase pulmonary oedema, and hence disease severity. In accordance with our results, Smadja and colleagues10 showed that Ang-2 level at hospital admission predicted COVID-19 severity.
The lack of a non-COVID-19 comparative group is a major limitation of this study. For example, Ang-2 levels in patients with COVID-19 might be similar to those of patients with other causes of acute respiratory distress syndrome. Nevertheless, we compared Ang-2 according to COVID-19 severity, showing that the most severe patients had higher markers of endothelial injury. Another major limitation is the single-time-point measurement.
Our main mechanistic hypothesis is that after the initial phase of viral infection, a pro-inflammatory state occurs, aggravated by local hypoxaemia, leading to progression of pulmonary vascular injuries.
Declarations of interest
The authors declare that they have no conflicts of interest.
Funding
Amiens Hospital University.
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.bja.2020.12.017.
Appendix A. Supplementary data
The following is the Supplementary data to this article:
{kind=link}
References
- 1.Sinha P., Matthay M.A., Calfee C.S. Is a “cytokine storm” relevant to COVID-19? JAMA Intern Med. 2020;180:1152–1154. doi: 10.1001/jamainternmed.2020.3313. [DOI] [PubMed] [Google Scholar]
- 2.Varga Z., Flammer A.J., Steiger P. Endothelial cell infection and endotheliitis in COVID-19. Lancet. 2020;395:1417–1418. doi: 10.1016/S0140-6736(20)30937-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wu Z., McGoogan J.M. Characteristics of and important lessons from the Coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for disease control and prevention. JAMA. 2020;323:1239. doi: 10.1001/jama.2020.2648. [DOI] [PubMed] [Google Scholar]
- 4.Salvarani C., Dolci G., Massari M. Effect of tocilizumab vs standard care on clinical worsening in patients hospitalized with COVID-19 pneumonia: a randomized clinical trial. JAMA Intern Med Adv. 2020 doi: 10.1001/jamainternmed.2020.6615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Leisman D.E., Ronner L., Pinotti R. Cytokine elevation in severe and critical COVID-19: a rapid systematic review, meta-analysis, and comparison with other inflammatory syndromes. Lancet Respir Med. 2020;8:1233–1244. doi: 10.1016/S2213-2600(20)30404-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Robinson P.C., Richards D., Tanner H.L., Feldmann M. Accumulating evidence suggests anti-TNF therapy needs to be given trial priority in COVID-19 treatment. Lancet Rheumatol. 2020;2:e653–e655. doi: 10.1016/S2665-9913(20)30309-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. Sterne J.A.C., Murthy S. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. JAMA. 2020;324:1330–1341. doi: 10.1001/jama.2020.17023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mahjoub Y., Rodenstein D.O., Jounieaux V. Severe Covid-19 disease: rather AVDS than ARDS? Crit Care. 2020;24:327. doi: 10.1186/s13054-020-02972-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kümpers P., Lukasz A., David S. Excess circulating angiopoietin-2 is a strong predictor of mortality in critically ill medical patients. Crit Care. 2008;12:R147. doi: 10.1186/cc7130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Smadja D.M., Guerin C.L., Chocron R. Angiopoietin-2 as a marker of endothelial activation is a good predictor factor for intensive care unit admission of COVID-19 patients. Angiogenesis. 2020;23:1–10. doi: 10.1007/s10456-020-09730-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.