

Key Points
Question
What key biological characteristics of maternal severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and placental function and pathology have implications for vertical transmission and neonatal protection?
Findings
In this prospective cohort study including 127 pregnancies, there was no maternal viremia, placental infection, or vertical transmission of SARS-CoV-2. Compromised transplacental transfer of anti–SARS-CoV-2 antibodies with robust transfer of influenza-specific immunity and nonoverlapping placental expression of SARS-CoV-2 receptors angiotensin-converting enzyme 2 and transmembrane serine protease 2 were noted.
Meaning
These findings suggest that, although low rates of maternal viremia and patterns of placental SARS-CoV-2 receptor distribution may underlie the rarity of vertical transmission, reduced transplacental transfer of anti–SARS-CoV-2 antibodies may leave neonates at risk for infection.
This cohort study examines maternal and neonatal severe acute respiratory syndrome coronavirus 2 viral load, transplacental antibody transfer, and placental pathology among pregnant women.
Abstract
Importance
Biological data are lacking with respect to risk of vertical transmission and mechanisms of fetoplacental protection in maternal severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.
Objective
To quantify SARS-CoV-2 viral load in maternal and neonatal biofluids, transplacental passage of anti–SARS-CoV-2 antibody, and incidence of fetoplacental infection.
Design, Setting, and Participants
This cohort study was conducted among pregnant women presenting for care at 3 tertiary care centers in Boston, Massachusetts. Women with reverse transcription–polymerase chain reaction (RT-PCR) results positive for SARS-CoV-2 were recruited from April 2 to June 13, 2020, and follow-up occurred through July 10, 2020. Contemporaneous participants without SARS-CoV-2 infection were enrolled as a convenience sample from pregnant women with RT-PCR results negative for SARS-CoV-2.
Exposures
SARS-CoV-2 infection in pregnancy, defined by nasopharyngeal swab RT-PCR.
Main Outcomes and Measures
The main outcomes were SARS-CoV-2 viral load in maternal plasma or respiratory fluids and umbilical cord plasma, quantification of anti–SARS-CoV-2 antibodies in maternal and cord plasma, and presence of SARS-CoV-2 RNA in the placenta.
Results
Among 127 pregnant women enrolled, 64 with RT-PCR results positive for SARS-CoV-2 (mean [SD] age, 31.6 [5.6] years) and 63 with RT-PCR results negative for SARS-CoV-2 (mean [SD] age, 33.9 [5.4] years) provided samples for analysis. Of women with SARS-CoV-2 infection, 23 (36%) were asymptomatic, 22 (34%) had mild disease, 7 (11%) had moderate disease, 10 (16%) had severe disease, and 2 (3%) had critical disease. In viral load analyses among 107 women, there was no detectable viremia in maternal or cord blood and no evidence of vertical transmission. Among 77 neonates tested in whom SARS-CoV-2 antibodies were quantified in cord blood, 1 had detectable immunoglobuilin M to nucleocapsid. Among 88 placentas tested, SARS-CoV-2 RNA was not detected in any. In antibody analyses among 37 women with SARS-CoV-2 infection, anti–receptor binding domain immunoglobin G was detected in 24 women (65%) and anti-nucleocapsid was detected in 26 women (70%). Mother-to-neonate transfer of anti–SARS-CoV-2 antibodies was significantly lower than transfer of anti-influenza hemagglutinin A antibodies (mean [SD] cord-to-maternal ratio: anti–receptor binding domain immunoglobin G, 0.72 [0.57]; anti-nucleocapsid, 0.74 [0.44]; anti-influenza, 1.44 [0.80]; P < .001). Nonoverlapping placental expression of SARS-CoV-2 receptors angiotensin-converting enzyme 2 and transmembrane serine protease 2 was noted.
Conclusions and Relevance
In this cohort study, there was no evidence of placental infection or definitive vertical transmission of SARS-CoV-2. Transplacental transfer of anti-SARS-CoV-2 antibodies was inefficient. Lack of viremia and reduced coexpression and colocalization of placental angiotensin-converting enzyme 2 and transmembrane serine protease 2 may serve as protective mechanisms against vertical transmission.
Introduction
Recent data from the Centers for Disease Control and Prevention (CDC)1 suggest that pregnant women with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection are more likely to require intensive care unit stay or mechanical ventilation than nonpregnant women of reproductive age. New data suggest that there is an increased risk of fetal2 and maternal3 death in the setting of maternal SARS-CoV-2 infection. While pregnancy-specific immunological and physiological changes may predispose women to increased morbidity in the setting of respiratory viruses,4 data are lacking regarding biological correlates of maternal disease severity in SARS-CoV-2 and have largely been extrapolated from nonpregnant populations or from pregnant women with SARS-CoV-1 or Middle East respiratory syndrome infection.5,6,7 Data regarding the maternal immune response, vertical transmission, and placental infection have been limited largely to case reports, small case series, and systematic reviews.8,9,10,11,12,13,14,15,16,17,18,19,20 Here, we report key biological data from a large prospective cohort study of SARS-CoV-2 infection in pregnancy regarding viral load, antibody response, transplacental antibody transfer, and placental pathology.
Methods
This study was approved by institutional review boards at all participating centers. All participants provided written informed consent. This study is reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Study Design
Pregnant women at 3 tertiary care centers in Boston, Massachusetts (Massachusetts General, Brigham and Women’s Hospital, and Beth Israel Deaconess Medical Center), were approached for enrollment in a coronavirus disease 2019 (COVID-19) pregnancy biorepository study starting April 2, 2020. Pregnant women were eligible for inclusion if they were aged 18 years or older, able to provide informed consent or had a health care proxy to do so, and diagnosed with, or at risk for, SARS-CoV-2 infection. Owing to wide community spread in Massachusetts during the study,21 all pregnant women presenting for hospital care were deemed at risk. Maternal confirmed SARS-CoV-2 infection was defined as nasopharyngeal swab reverse transcription–polymerase chain reaction (RT-PCR) test results positive for SARS-CoV-2. Neonates born to women with confirmed SARS-CoV-2 infection were tested by nasopharyngeal swab at age 24 hours.
Participants and Procedures
Identification of eligible participants with SARS-CoV-2 infection and enrollment of controls is detailed in the eAppendix in the Supplement. Universal screening for SARS-CoV-2 among all pregnant women on admission to labor and delivery units (initiated on April 16, 2020 at Massachusetts General Hospital and Brigham and Women’s Hospital and on April 27, 2020 at Beth Israel Deaconess Medical Center) permitted the enrollment of a robust control population. The National Institutes of Health and Society for Maternal-Fetal Medicine criteria were used to define COVID-19 disease severity (eAppendix in the Supplement).21,22 Severe maternal morbidity was defined per CDC criteria,23 and severe neonatal morbidity was defined per Maternal-Fetal Medicine Units Network criteria24,25 (eAppendix in the Supplement). Nonpregnant women of reproductive age (18-45 years) hospitalized with confirmed SARS-CoV-2 infection and enrolled contemporaneously as part of a general adult cohort described previously26 were used as an additional comparison group.
Sample Collection and Processing, SARS-CoV-2 Viral Load, and Antibody Quantification
Details on collection and processing of plasma, nasal and oropharyngeal swabs, saliva, sputum, and placenta, and comprehensive descriptions of methods for viral load quantification, enzyme-linked immunosorbent assay, and placental pathology are available in the eAppendix in the Supplement. SARS-CoV-2 viral load was quantified using the CDC 2019-nCoV_N1 primers and probe set.27 RNA was extracted from maternal and cord blood plasma and maternal respiratory specimens collected for research purposes; the clinical nasopharyngeal swab was not used for viral load quantification. Maternal blood and respiratory specimens collected in closest proximity to acute illness were used for viral load analyses. SARS-CoV-2 viral loads less than 40 RNA copies/mL were categorized as undetectable and set at 1.0 log10 RNA copies/mL.
Antibodies against SARS-CoV-2 receptor binding domain (RBD) on the S1 subunit of the spike protein and SARS-CoV-2 nucleocapsid (N) antigen were quantified using enzyme-linked immunosorbent assay. Quantification of antibody against the common influenza antigen hemagglutinin A (HA) was performed as a positive control. For transplacental antibody transfer analyses, paired maternal-cord blood samples from the delivery hospitalization were used.
Placental Pathology
An experienced placental pathologist (D.J.R.) reviewed the slides and gross findings from all cases and controls, rendering diagnoses per the Amsterdam guidelines (eTable 1 in the Supplement).28 Placentas from participants with SARS-CoV-2 infection were tested for placental infection using RNA in situ hybridization, as previously described.29,30 A SARS-CoV-2 –positive lung section and known SARS-CoV-2–positive placental section31 were used as positive controls (eFigure 1 in the Supplement). A subset of 7 cases from patients who were mildly or severely ill were additionally examined for expression of the SARS-CoV-2 receptor angiotensin-converting enzyme 2 (ACE2) and the spike transmembrane serine protease 2 (TMPRSS2), which is required for viral cell entry,32 by immunohistochemistry.
Outcomes
Primary outcomes in this study were quantification of SARS-CoV-2 viral load in maternal plasma, maternal respiratory fluids, and umbilical cord plasma; quantification of anti-SARS-CoV-2 immunoglobin (Ig) G and IgM antibodies in maternal and cord plasma; and presence of SARS-CoV-2 RNA in the placenta and evaluation of placental histopathology in cases and controls. The main secondary outcome was placental ACE2 and TMPRSS2 receptor expression.
Statistical Analyses
Differences between participants with confirmed SARS-CoV-2 infection and those with RT-PCR results negative for SARS-CoV-2 with respect to demographic variables, viral load, antibody response, placental gene expression, and placental pathology were evaluated using appropriate tests (ie, parametric or nonparametric) with 2-sided P values. Continuous outcome measures were summarized as either mean (SD) or median (interquartile range [IQR]), as appropriate for the normality of the data. Associations between disease severity and factors of interest were analyzed in either dichotomized or ordinal fashion, using Pearson χ2 (or Fisher exact) test, or Spearman rank-based testing. Correlation analyses between maximum maternal viral load, antibody response, and COVID-19 severity were performed using Spearman rank-based testing. Differences between paired maternal and cord sera IgG and IgM were evaluated with Wilcoxon signed rank testing. Statistical significance was defined as P < .05; Bonferroni P value corrections were used for placental pathology analyses. Analyses were performed using Prism version 8 (GraphPad) and Stata/IC version 14.2 (StataCorp). The eAppendix in the Supplement contains additional description of statistical methods.
Results
From April 2 through June 13, 2020, samples were obtained from 127 enrolled participants, 64 with RT-PCR results positive for SARS-CoV-2 and 63 with RT-PCR results negative for SARS-CoV-2. These included 88 completed mother-neonate dyads (47 with SARS-CoV-2 infection and 41 without SARS-CoV-2 infection), 4 women who delivered but did not have neonatal samples for analysis, 9 women who were still pregnant when the study ended, and 26 neonatal samples (placenta or umbilical cord blood) without matched maternal samples (eFigure 2 in the Supplement).
Participant Characteristics
Maternal and neonatal demographic characteristics and outcomes for cases and controls are reported in the Table. Participant demographic characteristics for the nonpregnant cohort are reported in eTable 2 in the Supplement. Among 64 participants with SARS-CoV-2 infection, 23 (36%) were asymptomatic, 22 (34%) had mild disease, 7 (11%) had moderate disease, 10 (16%) had severe disease, and 2 (3%) had critical disease.21,22 A total of 9 patients (14%) were diagnosed in the second trimester, and 54 patients (86%) were diagnosed in the third trimester. There were 2 fetal or neonatal deaths in the SARS-CoV-2 positive group: one 35-week intrauterine fetal demise in an asymptomatic woman diagnosed with SARS-CoV-2 on presentation for management of intrauterine fetal demise, and one 22-week neonatal demise secondary to extreme prematurity in the setting of abruption and preterm labor in a symptomatic patient. No neonates born to women with confirmed SARS-CoV-2 infection had positive test results for SARS-CoV-2. Assay results for each participant are detailed in eTable 3 in the Supplement. Detailed information on severe maternal and neonatal morbidity is provided in eTable 4 and eTable 5 in the Supplement.
Table. Cohort Demographic Characteristics and Delivery Outcomes.
| Characteristic | SARS-CoV-2 status, No. (%) | P value | |
|---|---|---|---|
| Negative (n = 63) | Positive (n = 64) | ||
| Maternal age, mean (SD), y | 33.9 (5.4) | 31.6 (5.6) | .02 |
| Race | |||
| Asian | 6 (10) | 0 | <.001 |
| Black | 5 (8) | 3 (5) | |
| White | 44 (70) | 26 (41) | |
| Othera | 5 (8) | 16 (25) | |
| >1 Race | 0 | 7 (11) | |
| Unknown or not reported | 3 (5) | 12 (19) | |
| Ethnicity | |||
| Hispanic or Latino | 13 (20) | 42 (66) | <.001 |
| Not Hispanic or Latino | 46 (73) | 21 (33) | |
| Unknown or not reported | 5 (8) | 2 (3) | |
| Type of insurance | |||
| Private | 48 (76) | 20 (32) | <.001 |
| Public | 15 (24) | 43 (68) | |
| Unknown | 0 | 1 (2) | |
| Pregravid BMI | |||
| <18.5 | 1 (2) | 0 | .04 |
| 18.5-24.9 | 29 (46) | 15 (23) | |
| 25.0-29.9 | 15 (24) | 23 (36) | |
| ≥30.0 | 18 (29) | 26 (41) | |
| Gestational weight gain, median (IQR), lb | 28 (20-35) | 21 (12-29) | .007 |
| Gravidity, median (IQR), No. | 2 (1-3) | 3 (2-4) | .06 |
| Parity, median (IQR), No. | 1 (0-1) | 1 (0-2) | .11 |
| History of preterm birth | 3 (5) | 6 (9) | .36 |
| Maternal comorbidities | |||
| Chronic hypertension | 1 (2) | 3 (5) | .32 |
| Diabetes or gestational diabetes | 12 (19) | 11 (17) | .79 |
| BMI >30 | 18 (29) | 26 (41) | .15 |
| Asthma | 8 (13) | 7 (11) | .76 |
| Other preexisting pulmonary condition | 0 | 2 (3) | .16 |
| Chronic kidney disease | 0 | 0 | NA |
| HIV | 0 | 0 | NA |
| IBD | 0 | 0 | NA |
| Thyroid disease | 4 (6) | 13 (21) | .02 |
| Cancer | 2 (3) | 2 (3) | .99 |
| Substance use within past year | |||
| Alcohol | 1 (1) | 0 | .53 |
| Cigarettes or tobacco | 5 (8) | 0 | .02 |
| Marijuana | 2 (3) | 1 (2) | .55 |
| Other vape | 0 | 0 | NA |
| Opioids | 0 | 0 | NA |
| Opioid replacement therapy | 0 | 0 | NA |
| Other | 0 | 1 (2) | .32 |
| Gestational age at delivery, median, (IQR), wkb | 39.1 (38.3-39.7) | 39 (37.4-40.1) | .14 |
| Preterm deliveryc | 5 (8) | 10 (18) | .11 |
| Spontaneous | 2 (40) | 3 (30) | NA |
| Detectable SARS-CoV-2 antibodies (RBD or N)d | |||
| IgG | 1 (2.5) | 26 (70) | <.001 |
| IgM | 1 (2.5) | 16 (43) | |
| Laborb | 38 (60) | 47 (82) | .008 |
| Mode of deliveryb | .006 | ||
| Vaginal | 24 (38) | 36 (63) | NA |
| Cesarean | 39 (62) | 21 (37) | |
| Preeclampsia/gestational hypertensionb | 13 (21) | 15 (26) | .46 |
| Infant sexb | |||
| Male | 34 (54) | 26 (45) | .31 |
| Female | 29 (46) | 31 (54) | |
| Birthweight, mean (SD), gb | 3429.21 (597.34) | 3072.28 (669.8) | .003 |
| Fetal growth restriction | 1 (2) | 4 (6) | .06 |
| Neonate SARS-CoV-2 screening resulte | |||
| Negative | NA | 48(75) | NA |
| Not tested | NA | 9 (14) | NA |
| Not delivered at time of analysis/pending test/unknown | NA | 7 (11) | NA |
| Composite morbidity | |||
| Maternal | 2 (3) | 9 (14) | .03 |
| Neonatalb | 5 (8) | 14 (25) | .01 |
| Neonatal deathf | 0 | 2 (4) | .16 |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); IBD, inflammatory bowel disease; Ig, immunoglobin; IQR, interquartile range; N, nucleocapsid; NA, not applicable; RBD, receptor binding domain; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Among participants with SARS-CoV-2, other race included Asian Indian (1 participant), Cape Verdean (2 participants), Dominican (4 participants), Dominican Hispanic (1 participant), Guatemalan (2 participants), Honduran (1 participant), not listed (1 participant), other (3 participants), and Salvadoran (3 participants). Among participants without SARS-CoV-2, other race included Salvadoran (2 participants) and other (3 participants).
At analysis, 57 participants with SARS-CoV-2 had delivered.
Preterm birth was defined as less than 37 weeks’ gestation and classified as spontaneous (eg, spontaneous labor, preterm premature rupture of the membranes) or indicated (eg, hypertensive disorders of pregnancy).
Forty mothers without SARS-CoV-2 and 37 mothers with SARS-CoV-2 had antibodies quantified for antibody transfer experiments. All participants with positive results for IgM to RBD also had positive IgG to RBD results. Of 12 participants with positive IgM to N results, 9 participants also had positive IgG to N results.
Forty-eight neonates (84% of neonates born to mothers with SARS-CoV-2 infection) were tested. Seven mothers with SARS-CoV-2 infection had not yet delivered. Thirteen neonates born to mothers diagnosed with SARS-CoV-2 earlier in pregnancy, but who tested negative for SARS-CoV-2 at the time of delivery were not clinically tested for SARS-CoV-2, per hospital infection control policies. Four of these neonates underwent a research assessment with quantification of viral load, which was negative.
Neonatal deaths detailed in severe neonatal morbidity eTable 5 in the Supplement.
Maternal Disease Severity
Maternal disease severity was significantly associated with detectable respiratory viral load (5 of 45 women [11%] with mild disease; 6 of 19 women [32%] with severe disease; P = .04) (eTable 6 in the Supplement). Maternal disease severity was positively correlated with serum concentration of C-reactive protein (Spearman ρ = 0.56; P = .003) and alanine aminotransferase (ρ = 0.42; P = .004). Disease severity was negatively correlated with white blood cell count (ρ = −0.57; P < .001).
Viral Load
SARS-CoV-2 viral load was quantified in 107 pregnant women (62 with SARS-CoV-2 infection and 45 without SARS-CoV-2 infection) and their neonates. Median (IQR) time from symptom onset to blood draw for viral load analysis was 13 (2-32) days. Median (IQR) time from symptom onset to collection of respiratory specimens for viral load analyses was 13 (1.75-31.75) days. There was no detectable viremia in any maternal or umbilical cord blood from 62 dyads with SARS-CoV-2 infection and 45 dyads without SARS-CoV-2 (Figure 1). Respiratory viral loads were quantified in 78 participants (44 with SARS-CoV-2 infection and 34 without SARS-CoV-2 infection). Among these, 11 women had detectable viral load in respiratory specimens (ie, nasal swab, oropharyngeal swab, saliva, or sputum). Among participants with RT-PCR confirmed SARS-CoV-2 infection, detectable viral load in maternal respiratory fluids was significantly associated with higher mean (SD) maternal anti-RBD IgG titers compared with 51 participants with undetectable viral load (0.79 [0.91] titers vs 0.29 [0.36] titers; P = .02) (eTable 7 in the Supplement). Among pregnant women with detectable viral load, sputum had the highest viral loads, followed by saliva, oral swab, and nasal swab. Viral load was not significantly correlated with any placental pathology among women with SARS-CoV-2 infection. Maternal viral load by time elapsed from SARS-CoV-2 diagnosis is depicted in eFigure 3 in the Supplement.
Figure 1. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Viral Load in Maternal and Neonatal Biofluids and Tissues by Maternal Disease Severity.

The dot plot shows viral loads across samples by reverse transcription–polymerase chain reaction test results. Samples were analyzed in triplicate. No significant differences in viral load between any respiratory fluid were detected by Wilcoxon signed rank test.
Compared with 11 nonpregnant women of reproductive age in the general adult cohort (age range, 22-42 years), there was no significant difference between mean (SD) respiratory viral load in pregnant and nonpregnant women (mean [SD], 3.8 [1.5] log10 copies/mL vs 4.8 [2.4] log10 copies/mL; P = .31). There was 1 case of viremia among women of reproductive age in the hospitalized nonpregnant cohort (plasma viral load of 2.4 log10 copies/mL detected 13 days after symptom onset).
Transplacental Antibody Transfer
Antibody quantification was performed for 77 mother-neonate dyads, including 37 mothers with RT-PCR–confirmed SARS-CoV-2 infection and 40 mothers with RT-PCR results negative for SARS-CoV-2. Maternal and neonatal blood for transplacental antibody transfer analyses was drawn at the time of delivery admission. Median (IQR) time from symptom onset to blood draw for antibody quantification was 28.5 (9-44) days. Among mothers with SARS-CoV-2 infection, 24 (65%) had detectable anti-RBD IgG and 26 (70%) had detectable anti-N IgG (ρ = 0.71, P < .001). Among umbilical cords from mothers with SARS-CoV-2 infection, 23 (62%) had detectable anti-RBD IgG and 22 (59%) had detectable anti-N IgG.
High transfer of influenza HA–specific antibody was observed regardless of maternal SARS-CoV-2 status (mean [SD] IgG HA transfer ratio: overall, 1.64 [1.37]; confirmed SARS-CoV-2, 1.44 [0.80]; P = .42). Compared with influenza, mean (SD) antibody transfer ratios were significantly reduced for anti–SARS-CoV-2 IgG against RBD (0.72 [0.57]; P < .001) and N (0.74 [0.44]; P < .001) (Figure 2A-C and Figure 3A). Maternal viral load was significantly negatively correlated with transplacental antibody transfer ratio of anti-RBD and anti-N IgG and negatively associated with cord blood anti-RBD and anti-N IgG titers (eTable 8 in the Supplement). Efficiency of antibody transfer (assessed by antibody transfer ratio) did not differ significantly between N and RBD, but mean (SD) antibody titers against N were significantly higher in the umbilical cord than those against RBD (0.77 [0.9] vs 0.24 [0.34]; P < .001). Cord blood titer of anti-RBD IgG was highly correlated with anti-N IgG (Spearman ρ = 0.86; P < .001) and with titers against HA (ρ = 0.48, P = .007, Figure 3B). Mean transfer ratios for IgG against RBD, N, and HA in preterm vs term neonates are depicted in eTable 9 in the Supplement.
Figure 2. Maternal-Cord Transplacental Antibody Transfer of Anti-Influenza Hemagglutinin A (HA) and Anti–Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Antibodies .
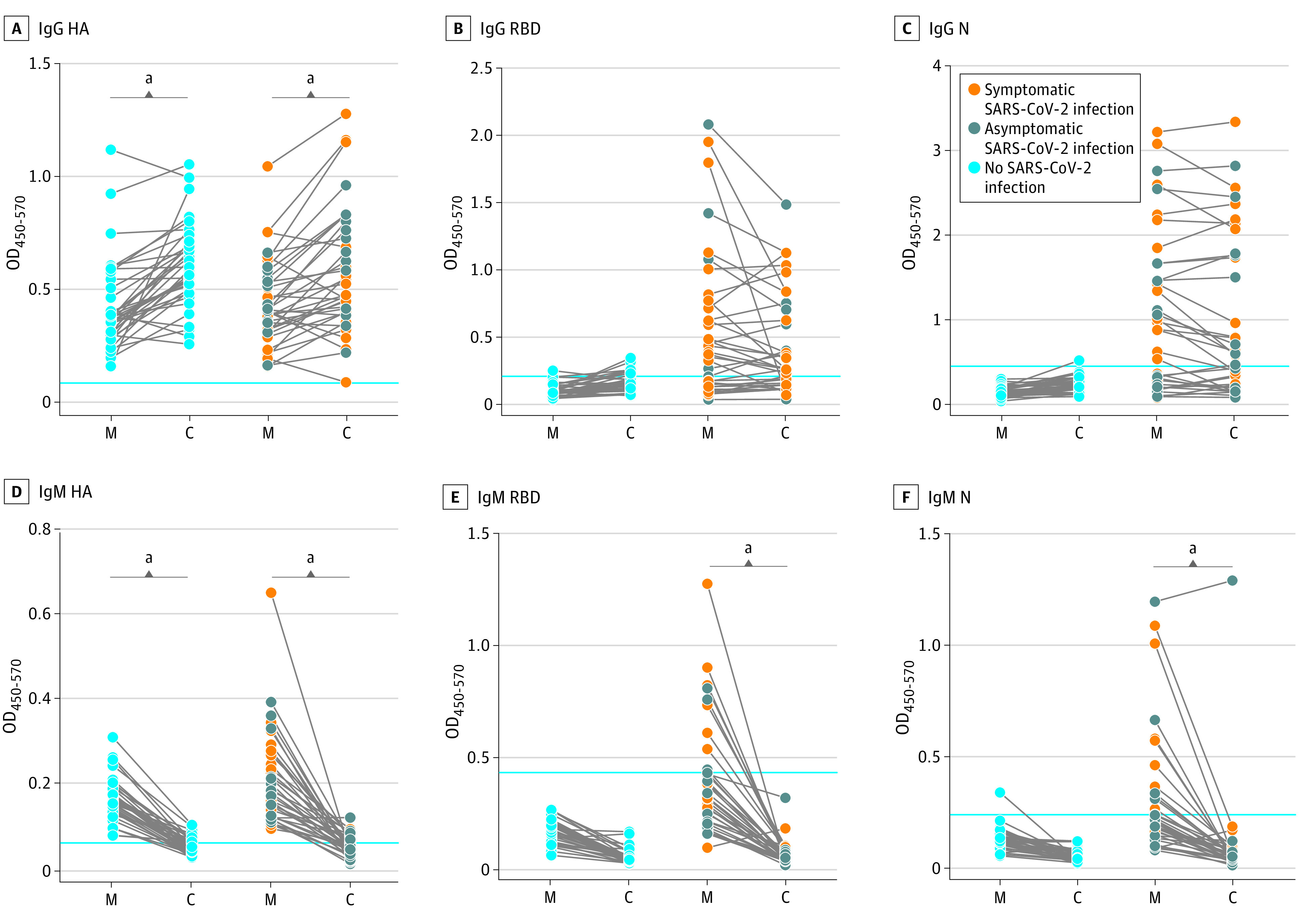
The dot plots depict relative immunoglobuin (Ig) G or IgM titer against influenza HA, SARS-CoV-2 receptor binding domain (RBD), and SARS-CoV-2 nucleocapsid (N) present in maternal plasma (M) or matched umbilical cord blood (C). Data are represented as the optical density (OD) 450 value after background correction and are shown as the mean of 2 replicates. The blue lines represent the sum of the mean value of SARS-CoV-2 negative samples and 3 × the SD of those samples. Significance was determined by a Wilcoxon matched-pairs signed rank test.
aP < .001.
Figure 3. Cord-to-Maternal Transplacental Antibody Transfer Ratios for Influenza and Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2).

A, Cord-to-maternal transfer ratio, calculated as (optical density [OD]450-570 cord)/(OD450-570 maternal) for antibodies against influenza hemagglutinin A (HA), and SARS-CoV-2 receptor binding domain (RBD) and nucleocapsid (N). Significance was assessed with a 1-way analysis of variance followed by Tukey post hoc testing to determine the source of significant differences in antibody transfer ratios among HA, RBD, and N. Ig indicates immunoglobin; black lines, means. B, Correlation between cord-to-maternal antibody transfer ratios for the indicated antibodies. Significance and ρ were determined by Spearman’s rank correlation.
aP < .001.
As expected, IgM transfer across the placenta was rare (Figure 2D-F). N-specific IgM was observed in a single SARS-CoV-2 umbilical cord sample. The mother was asymptomatic, tests for IgM to RBD were negative in both maternal blood and cord plasma, and IgM to HA was detectable at equivalent levels in maternal and cord blood. The neonate had nasopharyngeal swab RT-PCR results negative for SARS-CoV-2, and was clinically well-appearing. This participant had high levels of anti-N IgM in maternal blood and placental pathology was notable for maternal vascular malperfusion lesions, plasma cell deciduitis, and villitis of unknown etiology, suggesting a compromised syncytiotrophoblast barrier, increasing potential placental leakiness. In addition, placental intervillous thrombi were noted, consistent with fetomaternal hemorrhage.
Maternal transplacental antibody transfer did not differ significantly by maternal disease severity or maternal medical comorbidities (ie, obesity, hypertension, or diabetes). Maternal and cord anti-SARS-CoV-2 antibody titers were significantly correlated with number of days from symptom onset (eFigure 4 and eFigure 5 in the Supplement). Compared with nonpregnant hospitalized women of reproductive age, there was no significant difference in mean (SD) antibody titers between pregnant and nonpregnant women (IgG RBD: 0.39 [0.52] vs 0.35 [0.40]; P = .63; IgG N: 0.88 [0.86] vs 0.51 [0.48]; P = .29). However, the mean (SD) time from symptom onset to antibody draw among nonpregnant women was shorter than in pregnant women (11 [5.1] days vs 28 [20.6] days).
Placental Pathology
Pathologic examinations were performed on 88 placentas, including 44 from women with SARS-CoV-2 and 44 from women without SARS-CoV-2. RNA in situ hybridization revealed no cases of SARS-CoV-2 RNA in the placenta. A known SARS-CoV-2–infected placenta was used as a positive control, and in situ hybridization did detect SARS-CoV-2 RNA in this placenta (Figure 4A and B). Expression of the SARS-CoV-2 entry receptors ACE2 and TMPRSS2 was examined via immunohistochemistry on placental tissue sections, and we identified membranous syncytiotrophoblastic ACE2 expression, with a strong bias of expression to the stromal side of the cell (Figure 4C). TMPRSS2 was weakly expressed primarily in the villous endothelium, not the syncytiotrophoblastic membrane (Figure 4D). There was no characteristic placental pathology in our SARS-CoV-2–exposed placentas (eTable 10 in the Supplement). However, maternal vascular malperfusion was noted in 16 of 44 (36%) SARS-CoV-2 exposed placentas and 8 of 44 (18%) unexposed placentas (P = .06) (Figure 4E and F). Among participants with confirmed SARS-CoV-2 infection, the odds of maternal vascular malperfusion lesions increased significantly with disease severity (odds ratio, 2.09 [95% CI, 1.11-3.97]; P = .02) (eTable 11 in the Supplement).
Figure 4. Placental Findings in Maternal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection.

A and B: RNA in situ hybridization results at 20× original. Magenta red signal is visualized in the syncytiotrophoblast, with a complete lack of positivity in any stromal cells (including but not limited to Hofbauer cells) (A). C and D: SARS-CoV-2 receptor expression by immunohistochemistry at 40× original. C, Expression is restricted to the villous trophoblast with a polarity such that the highest expression is stromal side of the syncytiotrophoblast (gray arrow) with minimal to absent expression on the maternal vascular side (blue arrow). D, Weak expression limited to the villous endothelial cells (black arrow). Resident placental macrophages (Hofbauer cells) expressed neither angiotensin-converting enzyme 2 (ACE2) nor transmembrane serine protease 2 (TMPRSS2). E and F: Maternal vascular malperfusion (MVM) pathology. E, Hematoxylin and eosin stain at 4× original. F, Hematoxylin and eosin stain at 10× original.
Discussion
In this prospective cohort study of 127 pregnancies from a single city during the COVID-19 pandemic, we report zero cases of vertical transmission and no placental infection. We also report the absence of viremia in pregnant participants infected with SARS-CoV-2, relatively low frequency of detectable viral load in respiratory fluids, and a new finding of reduced efficiency of transplacental transfer of anti-SARS-CoV-2 antibodies. These data fill a substantial knowledge gap, point to the rarity of vertical transmission, and establish compromised SARS-CoV-2–specific immunity in the neonate. With only a handful of reported cases of vertical transmission,10,13,17,18,19,20 and the initial report from a prospectively-enrolled US registry demonstrating a vertical transmission rate of 1.1% (2 of 179 neonates),33 mechanisms of fetoplacental protection from SARS-CoV-2, and how these might impact neonatal immunity represent a critical area of investigation. Our study suggests low incidence of maternal viremia and nonoverlapping placental ACE2 and TMPRSS2 expression as potential mechanisms associated with protection against placental infection and vertical transmission in maternal COVID-19.
Viral Load as a Potential Factor in Maternal Disease Severity and Neonatal Immunity
No women with confirmed SARS-CoV-2 infection had detectable viremia in our cohort. The reported incidence of SARS-CoV-2 viremia in the literature was 10% to 15% in 2 series of nonpregnant patients, including men and women.34,35 Rates of viremia as high as 27% were reported in a cohort of nonpregnant patients hospitalized during the same time period at the institutions included in this study, with the same median days from symptom onset to study blood draw and evaluated in the same laboratory, with the same assay.26 This highlights the sensitivity of the viral load assay, acuity of disease presentation at our hospitals during the study enrollment period, and ability of the assay to detect virus when present in plasma at the same median interval from symptom onset to blood draw. Thus, the absence of viremia in our cohort points to the potential for enhanced maternal viral control. The lack of maternal viremia is plausible given the low prevalence of placental infection reported in SARS-CoV-2 to date and points to low likelihood of viral placental seeding. Future investigations may provide insights into the mechanisms underlying the lower incidence of viremia observed here in the setting of pregnancy. Importantly, enhanced natural killer–cell and T-cell responses to influenza A virus have been noted during pregnancy,36 and are enriched within the placenta.37 These data suggest that cytotoxic cells may be poised to control viruses during pregnancy, providing a robust front line defense against pathogens.
Recent studies have reported reduced sensitivity of oropharyngeal swab,38 saliva,39 and anterior or lower nasal swab40,41 compared with nasopharyngeal swab for the detection of SARS-CoV-2. Among participants with symptomatic illness, the detection of viral load on research respiratory specimens was significantly more likely when specimens were collected closer to the clinical nasopharyngeal swab positive for SARS-CoV-2. Similar to studies in nonpregnant patients, viral load was associated with increased disease severity.26,42
Transplacental Antibody Transfer and Positive Umbilical Cord IgM
Anti-RBD IgG and anti-N IgG transfer was significantly lower than for anti-HA IgG, and significantly lower than the expected cord-to-maternal antibody ratio of approximately 1.5 typically observed for pathogens including pertussis, influenza, and measles.43,44,45 Conversely, robust transfer of influenza-specific antibodies was noted, highlighting normal placental antibody transfer function. To our knowledge, this is the first report of reduced transplacental transfer of antibodies to SARS-CoV-2. These data point to a potential alteration in SARS-CoV-2–specific antibodies, which may result in compromised transfer. Whether altered transfer is related to infection-associated differences in SARS-CoV-2 antibody glycosylation or to differences in vaccine-elicited (HA) vs natural infection (SARS-CoV-2)–generated antibodies remains unclear. Recently reported findings that neonatal transferred antibodies may be short-lived46 raise further concern not only for poor initial transfer efficacy, but also for shorter durability of vertically transmitted immunity. Given data that demonstrate increased neonatal risk in the setting of reduced transplacental transfer secondary to native dengue virus infection,47,48,49 and maternal HIV (ie, reduced transfer of antibodies against tetanus, varicella-zoster virus, Epstein-Barr virus, measles, polio, and pertussis),50,51,52 it is certainly possible that reduced transplacental transfer of anti-SARS-CoV-2 antibodies increases risk of SARS-CoV-2 infection for neonates and infants. Recent data from the CDC indicate that infants aged 0 to 2 months comprise nearly 20% of all hospitalizations for SARS-CoV-2 infection among children aged 0 to 18 years.53
A single umbilical cord of a neonate born to a mother with confirmed SARS-CoV-2 infection had detectable IgM to SARS-CoV-2 N antigen. Given that placental pathology was suggestive of a damaged syncytiotrophoblast barrier and that we also observed high maternal levels of anti-N IgM and detectable anti-HA IgM in the cord at the same level as in maternal plasma, these findings likely represent aberrant transplacental transfer of IgM in the setting of placental compromise,54 rather than a specific elevation of IgM due to in utero infection. Although the finding of positive IgM has been interpreted as evidence of vertical transmission in prior reports,10,11,46 these findings raise the question of whether a more robust definition of vertical transmission is needed.
Placental Pathology
No cases of suspected vertical transmission were observed, and no placental infections were diagnosed in our series of placentas exposed to SARS-CoV-2, suggesting the presence of intrinsic defenses against vertical transmission. The poorly overlapping expression of ACE2 and TMPRSS2 within the placenta may represent an unanticipated defense mechanism. Placental infection leading to fetal infection requires either infection of the villous syncytiotrophoblast or the villous stroma, followed by viral traversal of the villous endothelial cells to make contact with fetal blood. We report nonoverlapping expression of ACE2 and TMPRSS2 within the placenta, with polarized villous ACE2 expression restricted to the stromal side of the syncytiotrophoblast, and weak expression of TMPRSS2 in the villous endothelial cells. Hofbauer cells in the villous stroma express neither. This expression pattern suggests that the villi are somewhat protected from infection and may help explain why placental SARS-CoV-2 infection and vertical transmission is so rare. The nonoverlapping expression of ACE2 and TMPRSS2 and weaker expression of TMPRSS2 compared with ACE2 are consistent with recent single-cell RNA-Seq data reporting lack of coordinated cotranscription of ACE2 and TMPRSS2 in placentas predating the COVID-19 pandemic.55
Limitations
This study has some limitations. The recruitment of controls as a convenience sample resulted in some demographic differences between cases and controls. Disproportionate COVID-19 disease burden in the Latinx community in the greater Boston area has been noted by our group,56 reflected in the demographic characteristics of our cases and controls. There was a higher rate of cesarean delivery among our controls, given that cesareans are often scheduled daytime procedures. It is both a strength and a limitation that our study necessarily examines transplacental antibody transfer in the setting of third trimester maternal infection with SARS-CoV-2, owing to the timing of the pandemic in Boston. The third trimester is typically regarded as the time when highest placental antibody transfer occurs,57,58,59 with most of these data from vaccinatable pathogens.60,61,62,63 While it is possible that antibody transfer may be lower in third trimester natural or native infection compared with second trimester infection, data are lacking in this regard. Comparing efficiency of antibody transfer in first, second, and third trimester native infection with SARS-CoV-2 will be an important area for future study, as women infected in the first and second trimester begin to deliver.
The timing of our study with the height of the first wave of the pandemic in Boston affords a unique opportunity to examine transfer of SARS-CoV-2 antibodies due to third-trimester native infection. The limited data available for Zika and Dengue virus infection in pregnancy demonstrate lower placental transfer ratios than have been described for influenza, pertussis, and measles vaccination43,44,45 but still higher ratios than we observed, ranging from 0.9 to approximately 1.2.64,65,66,67 Unlike our study, many studies on Zika and Dengue virus are unable to pinpoint the timing of maternal infection to a particular trimester, owing to their enrollment in endemic areas and use of antibody testing to determine infection. The large size of our cohort and the presence of robust contemporaneous controls with RT-PCR results negative for SARS-CoV-2 permit dissection of the impact of SARS-CoV-2 from other pandemic-related exposures that could influence maternal-fetal immune response68,69,70 is a strength of this study.
Conclusions
This report of maternal viral load, transplacental antibody transmission, and placental pathology in 127 pregnancies during the SARS-CoV-2 pandemic provides needed data about maternal viral control, reduced transplacental transfer of anti–SARS-CoV-2 antibodies, and lack of vertical transmission in mother-neonate dyads. These findings can immediately inform clinical care and vaccine development and deployment strategies to maximize benefit for pregnant women and their neonates.
eAppendix. Supplementary Methods
eTable 1. Placental Pathology Categories
eFigure 1. SARS-CoV-2 RNA in Situ Hybridization
eFigure 2. Participant Enrollment
eTable 2. Participant Demographics for Nonpregnant Adult Cohort
eTable 3. Experimental Assays Performed per Participant
eTable 4. Severe Maternal Morbidity
eTable 5. Severe Neonatal Morbidity
eTable 6. Participant Characteristics, Viral Loads, Antibody Quantification, and Placental Pathology Stratified by Maternal Disease Severity
eFigure 3. Maternal Viral Load by Time Elapsed From SARS-CoV-2 Diagnosis
eTable 7. Detectable Viral Load and Maternal and Neonatal Antibody
eTable 8. Correlations Between Maternal and Neonatal Antibody Titers, Transplacental Antibody Transfer, and Maximum Maternal Viral Load
eTable 9. Antibody Transfer Ratio in Full-Term vs Preterm Gestations
eFigure 4. Maternal Antibody Titers by Days From Symptom Onset
eFigure 5. Cord Antibody Titers by Days from Maternal Symptom Onset
eTable 10. Placental Pathology by Maternal SARS-CoV-2 Status
eTable 11. Placental Pathology by Maternal SARS-CoV-2 Severity
eReferences
References
- 1.Ellington S, Strid P, Tong VT, et al. Characteristics of women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status—United States, January 22-June 7, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(25):769-775. doi: 10.15585/mmwr.mm6925a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Khalil A, von Dadelszen P, Draycott T, Ugwumadu A, O’Brien P, Magee L. Change in the incidence of stillbirth and preterm delivery during the COVID-19 pandemic. JAMA. 2020;324(7):705-706. doi: 10.1001/jama.2020.12746 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Takemoto MLS, Menezes MO, Andreucci CB, et al. The tragedy of COVID-19 in Brazil: 124 maternal deaths and counting. Int J Gynaecol Obstet. 2020. doi: 10.1002/ijgo.13300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Liu H, Wang LL, Zhao SJ, Kwak-Kim J, Mor G, Liao AH. Why are pregnant women susceptible to COVID-19? an immunological viewpoint. J Reprod Immunol. 2020;139:103122. doi: 10.1016/j.jri.2020.103122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dashraath P, Wong JLJ, Lim MXK, et al. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am J Obstet Gynecol. 2020;222(6):521-531. doi: 10.1016/j.ajog.2020.03.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Alberca RW, Pereira NZ, Oliveira LMDS, Gozzi-Silva SC, Sato MN. Pregnancy, viral infection, and COVID-19. Front Immunol. 2020;11:1672. doi: 10.3389/fimmu.2020.01672 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schwartz DA, Graham AL. Potential maternal and infant outcomes from (Wuhan) coronavirus 2019-nCoV infecting pregnant women: lessons from SARS, MERS, and other human coronavirus infections. Viruses. 2020;12(2):12. doi: 10.3390/v12020194 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Baergen RN, Heller DS. Placental pathology in Covid-19 positive mothers: preliminary findings. Pediatr Dev Pathol. 2020;23(3):177-180. doi: 10.1177/1093526620925569 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395(10226):809-815. doi: 10.1016/S0140-6736(20)30360-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dong L, Tian J, He S, et al. Possible vertical transmission of SARS-CoV-2 from an infected mother to her newborn. JAMA. 2020;323(18):1846-1848. doi: 10.1001/jama.2020.4621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fenizia C, Biasin M, Cetin I. In utero mother-to-child SARS-CoV-2 transmission: viral detection and fetal immune response. medRxiv. Preprint posted online July 10, 2020. doi: 10.1101/2020.07.09.2014959 [DOI]
- 12.Hosier H, Farhadian S, Morotti R, et al. SARS-CoV-2 infection of the placenta. medRxiv. Preprint posted online May 12, 2020. doi: 10.1172/JCI139569 [DOI]
- 13.Patanè L, Morotti D, Giunta MR, et al. Vertical transmission of COVID-19: SARS-CoV-2 RNA on the fetal side of the placenta in pregnancies with COVID-19 positive mothers and neonates at birth. Am J Obstet Gynecol MFM. 2020;100145. doi: 10.1016/j.ajogmf.2020.100145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Penfield CA, Brubaker SG, Limaye MA, et al. Detection of SARS-COV-2 in placental and fetal membrane samples. Am J Obstet Gynecol MFM. 2020;100133. doi: 10.1016/j.ajogmf.2020.100133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shanes ED, Mithal LB, Otero S, Azad HA, Miller ES, Goldstein JA. Placental pathology in COVID-19. Am J Clin Pathol. 2020;154(1):23-32. doi: 10.1093/ajcp/aqaa089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chen S, Huang B, Luo DJ, et al. Pregnancy with new coronavirus infection: clinical characteristics and placental pathological analysis of three cases [Article in Chinese]. Zhonghua Bing Li Xue Za Zhi. 2020;49(5):418-423. doi: 10.3760/cma.j.cn112151-20200225-00138 [DOI] [PubMed] [Google Scholar]
- 17.Lamouroux A, Attie-Bitach T, Martinovic J, Leruez-Ville M, Ville Y. Evidence for and against vertical transmission for severe acute respiratory syndrome coronavirus 2. Am J Obstet Gynecol. 2020;223(1):91.e1-91.e4. doi: 10.1016/j.ajog.2020.04.039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Alzamora MC, Paredes T, Caceres D, Webb CM, Valdez LM, La Rosa M. Severe COVID-19 during pregnancy and possible vertical transmission. Am J Perinatol. 2020;37(8):861-865. doi: 10.1055/s-0040-1710050 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zeng H, Xu C, Fan J, et al. Antibodies in infants born to mothers with COVID-19 pneumonia. JAMA. 2020;323(18):1848-1849. doi: 10.1001/jama.2020.4861 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Vivanti AJ, Vauloup-Fellous C, Prevot S, et al. Transplacental transmission of SARS-CoV-2 infection. Nat Commun. 2020;11(1):3572. doi: 10.1038/s41467-020-17436-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mass.gov COVID-19 Daily Dashboard. Accessed June 20, 2020.https://www.mass.gov/info-details/covid-19-response-reporting#covid-19-daily-dashboard-
- 22.Society for Maternal-Fetal Medicine Management considerations for pregnant patients with COVID-19. Updated July 2, 2020. Accessed July 3, 2020, 2020. https://s3.amazonaws.com/cdn.smfm.org/media/2415/SMFM_COVID_Management_of_COVID_pos_preg_patients_7-2-20.PDF_.pdf
- 23.Centers for Disease Control and Prevention Severe maternal morbidity in the United States. Accessed July 7, 2020. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html
- 24.Kilpatrick SK, Ecker JL; American College of Obstetricians and Gynecologists and the Society for Maternal–Fetal Medicine . Severe maternal morbidity: screening and review. Am J Obstet Gynecol. 2016;215(3):B17-B22. doi: 10.1016/j.ajog.2016.07.050 [DOI] [PubMed] [Google Scholar]
- 25.Chauhan SP, Rice MM, Grobman WA, et al. ; MSCE, for the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units (MFMU) Network . Neonatal morbidity of small- and large-for-gestational-age neonates born at term in uncomplicated pregnancies. Obstet Gynecol. 2017;130(3):511-519. doi: 10.1097/AOG.0000000000002199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Fajnzylber JM, Regan J, Coxen K, et al. SARS-CoV-2 viral load is associated with increased disease severity and mortality. medRxiv. Preprint posted online July 17, 2020. doi: 10.1101/2020.07.15.20131789 [DOI] [PMC free article] [PubMed]
- 27.Centers for Disease Control and Prevention Research use only 2019-Novel Coronavirus (2019-nCoV) real-time RT-PCR primers and probes. Accessed April 2, 2020. https://www.cdc.gov/coronavirus/2019-ncov/lab/rt-pcr-panel-primer-probes.html
- 28.Khong TY, Mooney EE, Ariel I, et al. Sampling and definitions of placental lesions: Amsterdam Placental Workshop Group consensus statement. Arch Pathol Lab Med. 2016;140(7):698-713. doi: 10.5858/arpa.2015-0225-CC [DOI] [PubMed] [Google Scholar]
- 29.Saatcioglu HD, Kano M, Horn H, et al. Single-cell sequencing of neonatal uterus reveals an Misr2+ endometrial progenitor indispensable for fertility. Elife. 2019;8:8. doi: 10.7554/eLife.46349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wang F, Flanagan J, Su N, et al. RNAscope: a novel in situ RNA analysis platform for formalin-fixed, paraffin-embedded tissues. J Mol Diagn. 2012;14(1):22-29. doi: 10.1016/j.jmoldx.2011.08.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hecht JL, Quade B, Deshpande V, et al. SARS-CoV-2 can infect the placenta and is not associated with specific placental histopathology: a series of 19 placentas from COVID-19-positive mothers. Mod Pathol. 2020;33(11):2092-2103. doi: 10.1038/s41379-020-0639-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181(2):271-280.e8. doi: 10.1016/j.cell.2020.02.052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Flaherman VJ, Afshar Y, Boscardin J, et al. Infant outcomes following maternal infection with SARS-CoV-2: first report from the PRIORITY Study. Clin Infect Dis. 2020;ciaa1411. doi: 10.1093/cid/ciaa1411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Chen X, Zhao B, Qu Y, et al. Detectable serum SARS-CoV-2 viral load (RNAaemia) is closely correlated with drastically elevated interleukin 6 (IL-6) level in critically ill COVID-19 patients. Clin Infect Dis. 2020;ciaa449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506. doi: 10.1016/S0140-6736(20)30183-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kay AW, Fukuyama J, Aziz N, et al. Enhanced natural killer-cell and T-cell responses to influenza A virus during pregnancy. Proc Natl Acad Sci U S A. 2014;111(40):14506-14511. doi: 10.1073/pnas.1416569111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wells AI, Coyne CB. Type III interferons in antiviral defenses at barrier surfaces. Trends Immunol. 2018;39(10):848-858. doi: 10.1016/j.it.2018.08.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wölfel R, Corman VM, Guggemos W, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020;581(7809):465-469. doi: 10.1038/s41586-020-2196-x [DOI] [PubMed] [Google Scholar]
- 39.Jamal AJ, Mozafarihashjin M, Coomes E, et al. ; Toronto Invasive Bacterial Diseases Network COVID-19 Investigators . Sensitivity of nasopharyngeal swabs and saliva for the detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Clin Infect Dis. 2020;ciaa848. doi: 10.1093/cid/ciaa848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Péré H, Podglajen I, Wack M, et al. Nasal swab sampling for SARS-CoV-2: a convenient alternative in times of nasopharyngeal swab shortage. J Clin Microbiol. 2020;58(6):58. doi: 10.1128/JCM.00721-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Tu YP, Jennings R, Hart B, et al. Swabs collected by patients or health care workers for SARS-CoV-2 testing. N Engl J Med. 2020;383(5):494-496. doi: 10.1056/NEJMc2016321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Wang W, Xu Y, Gao R, et al. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA. 2020;323(18):1843-1844. doi: 10.1001/jama.2020.3786 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Gonçalves G, Cutts FT, Hills M, Rebelo-Andrade H, Trigo FA, Barros H. Transplacental transfer of measles and total IgG. Epidemiol Infect. 1999;122(2):273-279. doi: 10.1017/S0950268899002046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Heininger U, Riffelmann M, Leineweber B, Wirsing von Koenig CH. Maternally derived antibodies against Bordetella pertussis antigens pertussis toxin and filamentous hemagglutinin in preterm and full term newborns. Pediatr Infect Dis J. 2009;28(5):443-445. doi: 10.1097/INF.0b013e318193ead7 [DOI] [PubMed] [Google Scholar]
- 45.Munoz FM, Bond NH, Maccato M, et al. Safety and immunogenicity of tetanus diphtheria and acellular pertussis (Tdap) immunization during pregnancy in mothers and infants: a randomized clinical trial. JAMA. 2014;311(17):1760-1769. doi: 10.1001/jama.2014.3633 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Gao J, Li W, Hu X, et al. Disappearance of SARS-CoV-2 antibodies in infants born to women with COVID-19, Wuhan, China. Emerg Infect Dis. 2020;26(10):2491-2494. doi: 10.3201/eid2610.202328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hammond SN, Balmaseda A, Pérez L, et al. Differences in dengue severity in infants, children, and adults in a 3-year hospital-based study in Nicaragua. Am J Trop Med Hyg. 2005;73(6):1063-1070. doi: 10.4269/ajtmh.2005.73.1063 [DOI] [PubMed] [Google Scholar]
- 48.Pengsaa K, Luxemburger C, Sabchareon A, et al. Dengue virus infections in the first 2 years of life and the kinetics of transplacentally transferred dengue neutralizing antibodies in Thai children. J Infect Dis. 2006;194(11):1570-1576. doi: 10.1086/508492 [DOI] [PubMed] [Google Scholar]
- 49.Simmons CP, Chau TN, Thuy TT, et al. Maternal antibody and viral factors in the pathogenesis of dengue virus in infants. J Infect Dis. 2007;196(3):416-424. doi: 10.1086/519170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Cumberland P, Shulman CE, Maple PA, et al. Maternal HIV infection and placental malaria reduce transplacental antibody transfer and tetanus antibody levels in newborns in Kenya. J Infect Dis. 2007;196(4):550-557. doi: 10.1086/519845 [DOI] [PubMed] [Google Scholar]
- 51.Ogolla S, Daud II, Asito AS, et al. Reduced transplacental transfer of a subset of Epstein-Barr virus-specific antibodies to neonates of mothers infected with Plasmodium falciparum malaria during pregnancy. Clin Vaccine Immunol. 2015;22(11):1197-1205. doi: 10.1128/CVI.00270-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ray JE, Dobbs KR, Ogolla SO, et al. Reduced transplacental transfer of antimalarial antibodies in Kenyan HIV-exposed uninfected infants. Open Forum Infect Dis. 2019;6(6):ofz237. doi: 10.1093/ofid/ofz237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kim L, Whitaker M, O’Halloran A, et al. ; COVID-NET Surveillance Team . Hospitalization rates and characteristics of children aged <18 years hospitalized with laboratory-confirmed COVID-19—COVID-NET, 14 states, March 1-July 25, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1081-1088. doi: 10.15585/mmwr.mm6932e3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Ben-Hur H, Gurevich P, Elhayany A, Avinoach I, Schneider DF, Zusman I. Transport of maternal immunoglobulins through the human placental barrier in normal pregnancy and during inflammation. Int J Mol Med. 2005;16(3):401-407. doi: 10.3892/ijmm.16.3.401 [DOI] [PubMed] [Google Scholar]
- 55.Pique-Regi R, Romero R, Tarca AL, et al. Does the human placenta express the canonical cell entry mediators for SARS-CoV-2? Elife. 2020;9:e58716. doi: 10.7554/eLife.58716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Goldfarb IT, Clapp MA, Soffer MD, et al. Prevalence and severity of coronavirus disease 2019 (COVID-19) illness in symptomatic pregnant and postpartum women stratified by Hispanic ethnicity. Obstet Gynecol. 2020;136(2):300-302. doi: 10.1097/AOG.0000000000004005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Pentsuk N, van der Laan JW. An interspecies comparison of placental antibody transfer: new insights into developmental toxicity testing of monoclonal antibodies. Birth Defects Res B Dev Reprod Toxicol. 2009;86(4):328-344. doi: 10.1002/bdrb.20201 [DOI] [PubMed] [Google Scholar]
- 58.Garty BZ, Ludomirsky A, Danon YL, Peter JB, Douglas SD. Placental transfer of immunoglobulin G subclasses. Clin Diagn Lab Immunol. 1994;1(6):667-669. doi: 10.1128/CDLI.1.6.667-669.1994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Ciobanu AM, Dumitru AE, Gica N, Botezatu R, Peltecu G, Panaitescu AM. Benefits and risks of IgG transplacental transfer. Diagnostics (Basel). 2020;10(8):10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Zhong Z, Haltalli M, Holder B, et al. The impact of timing of maternal influenza immunization on infant antibody levels at birth. Clin Exp Immunol. 2019;195(2):139-152. doi: 10.1111/cei.13234 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Abu Raya B, Srugo I, Kessel A, et al. The effect of timing of maternal tetanus, diphtheria, and acellular pertussis (Tdap) immunization during pregnancy on newborn pertussis antibody levels: a prospective study. Vaccine. 2014;32(44):5787-5793. doi: 10.1016/j.vaccine.2014.08.038 [DOI] [PubMed] [Google Scholar]
- 62.Eberhardt CS, Blanchard-Rohner G, Lemaître B, et al. Maternal immunization earlier in pregnancy maximizes antibody transfer and expected infant seropositivity against pertussis. Clin Infect Dis. 2016;62(7):829-836. doi: 10.1093/cid/ciw027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Healy CM, Munoz FM, Rench MA, Halasa NB, Edwards KM, Baker CJ. Prevalence of pertussis antibodies in maternal delivery, cord, and infant serum. J Infect Dis. 2004;190(2):335-340. doi: 10.1086/421033 [DOI] [PubMed] [Google Scholar]
- 64.Castanha PMS, Souza WV, Braga C, et al. ; Microcephaly Epidemic Research Group . Perinatal analyses of Zika- and dengue virus–specific neutralizing antibodies: a microcephaly case-control study in an area of high dengue endemicity in Brazil. PLoS Negl Trop Dis. 2019;13(3):e0007246. doi: 10.1371/journal.pntd.0007246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Collier AY, Borducchi EN, Chandrashekar A, et al. Sustained maternal antibody and cellular immune responses in pregnant women infected with Zika virus and mother to infant transfer of Zika-specific antibodies. Am J Reprod Immunol. 2020;e13288. doi: 10.1111/aji.13288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Singh T, Lopez CA, Giuberti C, et al. Efficient transplacental IgG transfer in women infected with Zika virus during pregnancy. PLoS Negl Trop Dis. 2019;13(8):e0007648. doi: 10.1371/journal.pntd.0007648 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Castanha PM, Braga C, Cordeiro MT, et al. Placental transfer of dengue virus (DENV)-specific antibodies and kinetics of DENV infection-enhancing activity in Brazilian infants. J Infect Dis. 2016;214(2):265-272. doi: 10.1093/infdis/jiw143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Boulanger-Bertolus J, Pancaro C, Mashour GA. Increasing role of maternal immune activation in neurodevelopmental disorders. Front Behav Neurosci. 2018;12:230. doi: 10.3389/fnbeh.2018.00230 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Estes ML, McAllister AK. Maternal immune activation: implications for neuropsychiatric disorders. Science. 2016;353(6301):772-777. doi: 10.1126/science.aag3194 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Schepanski S, Buss C, Hanganu-Opatz IL, Arck PC. Prenatal immune and endocrine modulators of offspring’s brain development and cognitive functions later in life. Front Immunol. 2018;9:2186. doi: 10.3389/fimmu.2018.02186 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix. Supplementary Methods
eTable 1. Placental Pathology Categories
eFigure 1. SARS-CoV-2 RNA in Situ Hybridization
eFigure 2. Participant Enrollment
eTable 2. Participant Demographics for Nonpregnant Adult Cohort
eTable 3. Experimental Assays Performed per Participant
eTable 4. Severe Maternal Morbidity
eTable 5. Severe Neonatal Morbidity
eTable 6. Participant Characteristics, Viral Loads, Antibody Quantification, and Placental Pathology Stratified by Maternal Disease Severity
eFigure 3. Maternal Viral Load by Time Elapsed From SARS-CoV-2 Diagnosis
eTable 7. Detectable Viral Load and Maternal and Neonatal Antibody
eTable 8. Correlations Between Maternal and Neonatal Antibody Titers, Transplacental Antibody Transfer, and Maximum Maternal Viral Load
eTable 9. Antibody Transfer Ratio in Full-Term vs Preterm Gestations
eFigure 4. Maternal Antibody Titers by Days From Symptom Onset
eFigure 5. Cord Antibody Titers by Days from Maternal Symptom Onset
eTable 10. Placental Pathology by Maternal SARS-CoV-2 Status
eTable 11. Placental Pathology by Maternal SARS-CoV-2 Severity
eReferences