

Abstract
Objective:
The purpose of this randomised clinical trial study was to compare the incidence and intensity of post-operative pain following the use of single-file and multi-file rotary instruments with continuous rotational motion for root canal preparation in asymptomatic permanent human teeth.
Methods:
A total of 105 healthy consenting patients who fulfilled specific inclusion criteria and had premolar or molar teeth diagnosed with asymptomatic irreversible pulpitis without periapical pathosis requiring endodontic treatment participated in this study. The patients were randomly allocated by stratification into five groups of 21 according to the instruments and systems used for root canal preparation: (a) Neoniti A1 (#25) single file, (b) RaCe #25/.06 single file, (c) Mtwo #25/.06 single file, (d) Easy RaCe, (e) and Mtwo multifile. Endodontic treatment was carried out in a single appointment. The severity of post-operative pain was assessed by numerical rating scale scores until complete pain relief was achieved. Analgesic consumption and the incidence of pain were also evaluated. Data were analysed by one-way ANOVA and Tukey HSD tests.
Results:
When comparing different instruments and systems for canal preparation, the analgesic consumption, incidence and intensity of post-operative pain did not differ (p>0.05). The highest levels of post-operative pain were experienced after 6 h in all groups.
Conclusion:
The post-operative pain did not differ between the single and multi-file root canal preparation techniques evaluated in this study.
Keywords: Analgesic, instrumentation, Nickel-titanium, post-operative pain, root canal treatment, Rotary
HIGHLIGHTS.
The greatest intensity and incidence of post-operative pain was seen after 6 h in all experimental groups.
No significant difference was seen between the intensity of post-operative pain when comparing different instrumentation types.
Patients in the Neoniti group had the lowest and the Easy RaCe group had the highest analgesic consumption, although these differences were not statistically significant.
INTRODUCTION
Post-operative pain after endodontic treatments is a major concern for patients and can be a deterrent for seeking treatment. Endodontic treatment reduces the pain experienced by patients before treatment; however, many studies have reported a high incidence of post-operative pain after these treatments (1-3). Several mechanical, chemical, and microbial factors influence post-operative pain and flare-ups experienced by patients (4). The instrumentation process has been claimed to have significant relevance for post-operative pain and flare-ups, for instance, by influencing debris and bacterial extrusion (5-7). Controversy exists regarding the apical extrusion of debris induced by different instrumentation techniques such as single-file instrumentation systems, which are becoming popular among endodontists and general practitioners performing endodontic therapy (5-7). De-Deus et al. demonstrated that ProTaper Universal multi-file rotary instrumentation extruded significantly more debris than the Wave-One reciprocating single-file instrumentation technique (8). Küçükyilmaz et al. showed that the OneShape continuous rotational single-file instru-mentation system produced the least extruded debris while the Reciproc single-file reciprocating instrumentation system produced the greatest amounts (9). Bürklein et al. also showed more debris extrusion from Reciproc, a reciprocating single-file instrumentation system, while no significant difference was noted between F360 and OneShape single-file rotary systems and the Mtwo multi-file rotary system (10). However, Mittal et al. evaluated the apical bacterial extrusion and concluded that ProTaper multi-file rotary systems exhibited significantly more bacterial extrusion than OneShape single-file rotary systems (11).
Neoniti (Neolix, Châtres-la-Forêt, France) is a nickel-titanium (NiTi) rotary system manufactured by a wirecut electrical discharge machining process. The manufacturer claims that it has controlled memory and a rough surface, resulting in abrasive properties, satisfactory shaping and no screwing effect. This system is used in continuous rotation and consists of the following files:
A1: provided in three tip sizes (#20, #25 and #40).
C1: with a tip size of #25 and 0.12 taper used as an optional orifice shaper.
Because the use of the C1 file is optional, this system can be used as a single-file technique.
Studies have suggested that routine rotary instrumentation systems such as Mtwo or RaCe be used in a single-file continuous rotational technique because they have found no difference in the efficacy of root canal preparation of Mtwo and RaCe rotary files when used as a single-file technique versus multiple-file technique (12, 13).
There is a lack of evidence regarding the direct correlation between post-operative pain and apical bacterial and/or debris extrusion subsequent to the use of different instrument systems. Therefore, conducting clinical research regarding the relation between single rotary file instrumentation systems and post-operative pain and comparing these with multi-file rotary instrumentation systems is of high clinical significance. The purpose of this study was to compare the incidence and intensity of post-operative pain following the use of single-file (Neoniti A1 #25, #25/.06 RaCe and Mtwo) and multi-file (Mtwo and Easy RaCe) rotary instruments for root canal preparation in asymptomatic permanent human teeth (12). The null hypothesis was that there is no significant difference between the incidence and intensity of post-operative pain following root canal preparation with single-file and multi-file rotary instruments in asymptomatic permanent human teeth.
MATERIALS AND METHODS
This randomised clinical trial was approved by the Ethics Committee of AJA University of Medical Sciences (Reg. No. IR.AJAUMS.REC.1394.12) and registered at www.irct.ir (IRCT201506167963N2).
The sample size calculation, which was based on an error of alpha=0.05 and a power of 0.8, indicated that ideally a sample size of 21 in each group would be required.
One hundred and five healthy consenting patients between the ages of 15 and 55 years who were referred to the Department of Endodontic of AJA University of Medical Sciences participated in this study. All of these patients required endodontic treatment for maxillary or mandibular premolars or molars diagnosed with asymptomatic irreversible pulpitis without periapical pathosis. The patients experienced no symptoms prior to treatment initiation.
The exclusion criteria were consumption of any type of medication before treatment, presence of root resorption, apical pathosis, sinus tracts, pulpal obliteration, periodontal scoring index less than 3, systemic disease, history of trauma, pregnancy, traumatic occlusion, TMJ problems, bruxism or clenching, history of intolerance of NSAIDs and previous endodontic treatment.
The patients were randomly allocated by stratification into five groups of 21 according to gender, the type of tooth and jaw (Table 1). Allocation was done by a person other than the operator performing the root canal procedure. After evaluations, the information of each patient and the instrumentation technique assigned to the patient was written and sealed in an envelope and given to the operator.
TABLE 1.
Baseline demographic and clinical characteristics of patients in each group
| Instrumentation | Gender | Jaw | Tooth type | |||
|---|---|---|---|---|---|---|
| Male | Female | Maxilla | Mandible | Premolar | Molar | |
| Neoniti single file (n=21) | 9 | 12 | 8 | 13 | 10 | 11 |
| RaCe single file (n=21) | 10 | 11 | 8 | 13 | 8 | 13 |
| Mtwo single file (n=21) | 10 | 11 | 8 | 13 | 8 | 13 |
| Easy RaCe (n=21) | 8 | 13 | 8 | 13 | 9 | 12 |
| Mtwo multi-file (n=21) | 12 | 9 | 9 | 12 | 7 | 14 |
All teeth were treated in one appointment by the same operator. A 2% lidocaine solution with 1/80000 epinephrine (Persocaine-E®, Daroupakhsh Co., Tehran, Iran) was applied to achieve profound local anaesthesia. Afterwards, the access cavity was prepared and the tooth was isolated using a rubber dam. The initial working length was determined with an electronic root canal measurement device (Root ZX, J Morita, Tokyo, Japan) and then confirmed by radiographic imaging. Subsequently, root canal preparation was accomplished by using a limited-torque electric motor (Endo e class, Marathon Saeyang Microtech, Daegu, Korea) and one of the following instruments and systems:
Neoniti A1#25 (Neolix, Châtres-la-Forêt, France) single file
RaCe #25/.06 (FKG Dentaire, La-Chaux-de-Fonds, Switzerland) single file
Mtwo #25/.06 (Sweden and Martina, Padua, Italy) single file
Easy RaCe up to #25/.06
Mtwo multi-file up to #25/.06
The protocol used for single-file systems was as follows. After preparation by #10 and #15 stainless steel K-files, the root canals were prepared using the respective file with active lateral force in an anti-curvature in-and-out brushing motion until the file reached the working length. After every three in-andout motions, irrigation and patency was achieved (12). Easy RaCe preparation was carried out with a crown-down technique starting with the #40/.10 instrument and followed by the #35/.08 and #25.06 files. Mtwo multi-file preparation was carried out with a single-length technique using the following sequence: 10/.04, 15/.05, 20/.06 and 25/.06 with each used until reaching the working length (12). For adequate preparation in root canals with wider dimensions, files were applied with active lateral force with respect to anti-curvature for a longer time until glassy smooth dentinal walls were attained.
During instrumentation, 5.25% sodium hypochlorite was used for irrigation. After the completion of instrumentation, 1 mL of 17% EDTA (Calasept, Nordiska Dental AB, Angelhilm, Sweden) was administered for 1 min to remove the smear layer, and 2% chlorhexidine (Calasept, Nordiska Dental AB, Angelhilm, Sweden) was used as the final irrigant. Subsequently, the root canals were obturated with gutta-percha (Meta biomed, Cheongju, Korea) and AH26 (Dentsply DeTrey, Konstanz, Germany) sealer using a lateral compaction technique. Teeth were temporarily restored with reinforced zinc oxide eugenol cement (Zoliran, Golchai, Tehran, Iran).
At the end of the appointment, patients were provided with 10 capsules of 400 mg Ibuprofen (Gelofen®, Jabberebne Hayyan, Tehran, Iran) and advised to take one analgesic every 6 h if experiencing pain (after recording their level of pain). Levels of pain were recorded by the nurse who was unaware of the instrumentation technique appointed to the patients (14, 15). A numerical rating scale (NRS) was used for recording pain levels. For the first 24 h after treatment, patients were contacted by phone every 6 hours. If necessary, depending on the intensity of pain, the patients were allowed to take a dose of analgesic. Afterwards, further NRS scores were recorded every 24 h until complete pain relief was achieved (16). The number of analgesics taken by each patient was also recorded.
In cases associated with very severe pain, after recording the amount of pain the patient would be advised to use the alternative method of pain control consisting of 400 mg Ibuprofen and 325 mg Paracetamol alternatively every 2 h. Those experiencing side effects of NSAIDs would be excluded from further analysis.
Data were analysed with Statistical Package for the Social Sciences software version 22 (IBM Corp.; Armonk, NY, USA) using one-way ANOVA and Tukey HSD tests. Differences were considered statistically significant at P<0.05 when a 95% confidence interval level was obtained.
RESULTS
Table 2 shows the number of analgesics taken by the patients in each group. The Neoniti group had the lowest and the Easy RaCe group had the highest analgesic consumption, although these differences were not statistically significant (P=1.00). None of the patients participating in this study experienced severe enough pain to use the alternative method of pain control.
TABLE 2.
Mean±SD and minimum and maximum analgesic consumption in each experimental group
| Instrumentation type | Mean±SD | Minimum | Maximum |
|---|---|---|---|
| Neoniti single file | 1.9±1.1 | 0 | 5 |
| RaCe single file | 1.9±1.1 | 1 | 4 |
| Mtwo single file | 1.8±1.3 | 1 | 5 |
| Easy RaCe | 2.3±1.1 | 1 | 4 |
| Mtwo multi-file | 1.9±1.1 | 1 | 4 |
Figure 1 shows the mean post-operative pain (NRS scores) experienced by patients in each instrumentation group after the evaluated time intervals. The highest NRS scores were recorded at 6 h post-operation in all experimental groups. Only patients in the Neoniti and Mtwo single-file groups exhibited pain at 24 h post-operation, and in the case of patients in the Mtwo single-file group the pain continued up to 48 h post-operation. It should be noted that the pain experienced was mild.
Figure 1.
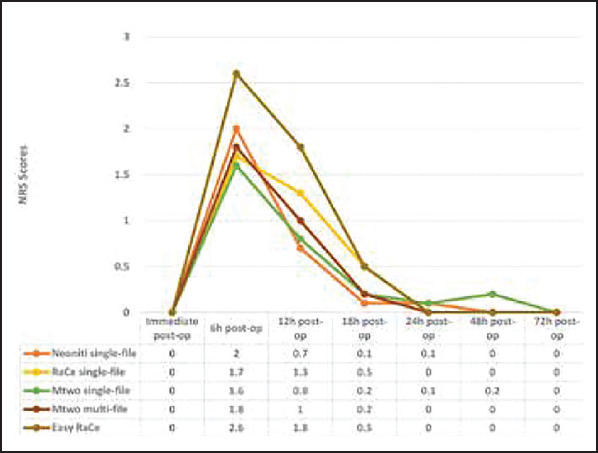
Numerical rating scale (NRS) scores of different experimental groups
No significant difference was seen between the intensity of post-operative pain when comparing different instrumentation types (P=0.56) (Table 3).
TABLE 3.
Incidence of post-operative pain in different experimental groups
| Instrument (n=21 each) | Incidence of post-operative pain Number (per cent) | ||||
|---|---|---|---|---|---|
| 6 h | 12 h | 18 h | 24 h | 48 h | |
| Neoniti single file | 12 (57.1%) | 7 (33.3%) | 1 (4.7%) | 1 (4.7%) | 0 |
| RaCe single file | 9 (42.8%) | 7 (33.3%) | 4 (19%) | 0 | 0 |
| Mtwo single file | 7 (33.3%) | 6 (28.6%) | 3 (14.3%) | 1 (4.8%) | 1 (4.8%) |
| Mtwo multi-file | 11 (52.4%) | 6 (28.6%) | 3 (14.3%) | 0 | 0 |
| Easy RaCe | 15 (71.4%) | 1 (52.4%) | 4 (19%) | 0 | 0 |
DISCUSSION
Endodontic treatment is performed to manage pain, but post-operative pain after this treatment has been reported to occur in 1.9%-48% of cases (1-3). Post-operative pain can cause anxiety in patients and is a deterrent factor for patients that might prohibit them from seeking treatment. Therefore, finding techniques leading to less post-operative pain is of clinical significance. Practitioners have a tendency to utilise easier instrumentation techniques requiring less chair time. Aminsobhani et al. found no significant difference in the canal-centring ability, apical transportation, or amount of cleaned root canal walls between specimens prepared with Mtwo and RaCe rotary files when used in single-file versus multi-file techniques (12, 13). Currently, no study has evaluated the post-operative pain experienced by patients subsequent to root canal instrumentation with Neoniti, RaCe and Mtwo rotary files used in a single-file technique. Therefore, the aim of the current study was to compare post-operative pain experienced by patients after root canal reparation with Neoniti and RaCe and Mtwo rotary files used in a single or multiple-file technique in a continuous rotational motion.
To limit the effect of confounding variables, factors such as the presence of pre-operative pain, symptomatic cases and apical pathosis, which have been clearly shown to significantly affect the intensity and incidence of post-operative pain were excluded in this study (1, 17, 18). Considering the limitations in sample collection, allocation by stratification was done according to gender, the type of tooth and jaw because these factors have been shown to be significantly associated with higher post-operative pain (19, 20). The operator was not blinded in this trial but was not aware of the instrumentation system until the moment of cleaning and shaping (allocation concealment). This step helped to reduce operator-dependent variations.
When using single rotary file systems, root canal preparation will be achieved through a crown-down technique and using a crown-down technique for preparation has been shown to be associated with less debris extrusion compared with other instrumentation techniques (21). On the other hand, when using single-file systems, a piston effect may be created when the instrument reaches the apical portion of the root canal thus leading to debris extrusion through a patent apical foramen (22). The amount of apical bacterial and debris and neuropeptides released from C-type nerve fibres present in the periodontal ligament (PDL) have been suggested to be the main reasons for post-operative pain experienced by patients (5-7, 23). Differences between the amount of apical bacterial and debris extrusion between instrumentation techniques have been evaluated by several researchers (5, 8, 11,24). Bürklein et al. (5) demonstrated that continuous rotation of files may improve coronal transportation of dentin chips and debris by acting like a screw conveyor, thus resulting in reduced apical debris extrusion. Another factor influencing apical debris extrusion is the design of the files. For instance, files with effective cutting ability, such as Neoniti and Mtwo, remove a greater amount of dentin in a relatively shorter period of time and are incapable of coronally displacing debris (10). Mittal et al. (11) compared apical bacterial extrusion subsequent to rotary instrumentation with ProTaper multi-file and OneShape single-file systems and concluded that apical bacterial extrusion was significantly greater in multi-file compared to single-file rotary systems. Therefore, differences were expected in the post-operative pain experienced subsequent to instrumentation with multi-file and single-file rotary systems. Interestingly, the results of the current study revealed that the instrumentation type had no significant influence on post-operative pain. In addition, the intensity of pain experienced by patients did not affect their choice of analgesics because none of the patients required the use of alternative pain control methods. Thus, the various aforementioned factors influencing debris extrusion in different techniques evaluated in this study may tend to counteract each other resulting in no significant difference. Another explanation for these results can be that periapical tissues might serve as a natural barrier providing a physical backpressure thus limiting the apical extrusion of debris and irrigants as shown in in vivo studies (25).
The greatest intensity and incidence of post-operative pain was seen after 6 h in all experimental groups. This trend was seen in previous studies (16, 26) and might be attributed to the expression of pro-inflammatory mediators and neuropeptides such as substance P and calcitonin gene-related peptide in the periodontal ligament subsequent to root canal preparation (16, 23, 26,27).
CONCLUSION
Under the limitations of this study, it can be concluded that root canal preparation using a single file with continuous rotation did not influence the incidence or intensity of post-operative pain experienced by asymptomatic patients with no apical pathosis.
Footnotes
Conflict of Interest: No conflict of interest was declared by the authors.
Ethical Approval: Ethics committee approval was received for this study from Ethics Committee of AJA University of Medical Sciences (Reg. No. IR.AJAUMS.REC.1394.12).
Informed Consent: Written informed consent was obtained from patients who participated in this study.
Peer-review: Externally peer-reviewed.
Financial Disclosure: The authors declared that this study has received no financial support.
Authorship Contributions: Concept – M.A., N.M.; Design – M.A.; Supervision – N.M.; Funding - M.A.; Materials - M.A.; Data collection &/or processing – N.M.; Analysis and/or interpretation – A.K.; Literature search – A.G.; Writing – N.M.; Critical Reviews - N.M., A.G.
REFERENCES
- 1.Ng YL, Glennon J, Setchell D, Gulabivala K. Prevalence of and factors affecting post?obturation pain in patients undergoing root canal treatment. Int Endod J. 2004;37(6):381–91. doi: 10.1111/j.1365-2591.2004.00820.x. [DOI] [PubMed] [Google Scholar]
- 2.Morse DR, Furst ML, Belott RM, Lefkowitz RD, Spritzer IB, Sideman BH. Infectious flare-ups and serious sequelae following endodontic treatment:a prospective randomized trial on efficacy of antibiotic prophylaxis in cases of asymptomatic pulpal-periapical lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1987;64(1):96–109. doi: 10.1016/0030-4220(87)90123-x. [DOI] [PubMed] [Google Scholar]
- 3.Pak JG, White SN. Pain prevalence and severity before, during, and after root canal treatment:a systematic review. J Endod. 2011;37(4):429–38. doi: 10.1016/j.joen.2010.12.016. [DOI] [PubMed] [Google Scholar]
- 4.Alves Vde O. Endodontic flare-ups:a prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(5):e68–e72. doi: 10.1016/j.tripleo.2010.05.014. [DOI] [PubMed] [Google Scholar]
- 5.Bürklein S, Schäfer E. Apically extruded debris with reciprocating single- file and full-sequence rotary instrumentation systems. J Endod. 2012;38(6):850–2. doi: 10.1016/j.joen.2012.02.017. [DOI] [PubMed] [Google Scholar]
- 6.Ferraz CC, Gomes NV, Gomes BP, Zaia AA, Teixeira FB, Souza-Filho FJ. Apical extrusion of debris and irrigants using two hand and three engine-driven instrumentation techniques. Int Endod J. 2001;34(5):354–8. doi: 10.1046/j.1365-2591.2001.00394.x. [DOI] [PubMed] [Google Scholar]
- 7.Nair PN, Henry S, Cano V, Vera J. Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after “one-visit”endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99(2):231–52. doi: 10.1016/j.tripleo.2004.10.005. [DOI] [PubMed] [Google Scholar]
- 8.De-Deus G, Neves A, Silva EJ, Mendonça TA, Lourenço C, Calixto C, et al. Apically extruded dentin debris by reciprocating single-file and multifile rotary system. Clin Oral Investig. 2015;19(2):357–61. doi: 10.1007/s00784-014-1267-5. [DOI] [PubMed] [Google Scholar]
- 9.Kucukyilmaz E, Savas S, Saygili G, Uysal B. Assessment of apically extruded debris and irrigant produced by different nickel-titanium instrument systems. Braz Oral Res. 2015;29:1–6. doi: 10.1590/1807-3107bor-2015.vol29.0002. [DOI] [PubMed] [Google Scholar]
- 10.Bürklein S, Benten S, Schäfer E. Quantitative evaluation of apically extruded debris with different single?file systems:Reciproc, F360 and OneShape versus Mtwo. Int Endod J. 2014;47(5):405–9. doi: 10.1111/iej.12161. [DOI] [PubMed] [Google Scholar]
- 11.Mittal R, Singla MG, Garg A, Dhawan A. A Comparison of Apical Bacterial Extrusion in Manual, ProTaper Rotary, and One Shape Rotary Instrumentation Techniques. J Endod. 2015;41(12):2040–4. doi: 10.1016/j.joen.2015.09.002. [DOI] [PubMed] [Google Scholar]
- 12.Aminsobhani M, Ghorbanzadeh A, Dehghan S, Niasar AN, Kharazifard MJ. A comparison of canal preparations by Mtwo and RaCe rotary files using full sequence versus one rotary file techniques;a cone-beam computed tomography analysis. Saudi Endodontic Journal. 2014;4(2):70–6. [Google Scholar]
- 13.Aminsobhani M, Razmi H, Nozari S. Ex Vivo Comparison of Mtwo and RaCe Rotary File Systems in Root Canal Deviation:One File Only versus the Conventional Method. Journal of dentistry (Tehran, Iran) 2015;12(7):469–77. [PMC free article] [PubMed] [Google Scholar]
- 14.Silva EJ, Menaged K, Ajuz N, Monteiro MR, Coutinho-Filho Tde S. Postoperative pain after foraminal enlargement in anterior teeth with necrosis and apical periodontitis:a prospective and randomized clinical trial. Journal of endodontics. 2013;39(2):173–6. doi: 10.1016/j.joen.2012.11.013. [DOI] [PubMed] [Google Scholar]
- 15.Arias A, de la Macorra JC, Azabal M, Hidalgo JJ, Peters OA. Prospective case controlled clinical study of post-endodontic pain after rotary root canal preparation performed by a single operator. Journal of dentistry. 2015;43(3):389–95. doi: 10.1016/j.jdent.2014.07.008. [DOI] [PubMed] [Google Scholar]
- 16.Nekoofar MH, Sheykhrezae MS, Meraji N, Jamee A, Shirvani A, Jamee J, et al. Comparison of the effect of root canal preparation by using WaveOne and ProTaper on postoperative pain:a randomized clinical trial. J Endod. 2015;41(5):575–8. doi: 10.1016/j.joen.2014.12.026. [DOI] [PubMed] [Google Scholar]
- 17.Sadaf D, Ahmad MZ. Factors Associated with Postoperative Pain in Endodontic Therapy. Int J Biomed Sci. 2014;10(4):243–7. [PMC free article] [PubMed] [Google Scholar]
- 18.De Andrade Risso P, Da Cunha AJLA, De Araujo MCP, Luiz RR. Postoperative pain and associated factors in adolescent patients undergoing two?visit root canal therapy. Aust Endod J. 2009;35(2):89–92. doi: 10.1111/j.1747-4477.2008.00134.x. [DOI] [PubMed] [Google Scholar]
- 19.Ali A, Olivieri JG, Duran-Sindreu F, Abella F, Roiq M, Garcia-Font M. Influence of preoperative pain intensity on postoperative pain after root canal treatment:A prospective clinical study. J Dent. 2016;45:39–42. doi: 10.1016/j.jdent.2015.12.002. [DOI] [PubMed] [Google Scholar]
- 20.Ali SG, Mulay S, Palekar A, Seipal D, Joshi A, Gufran H. Prevalence of and factors affecting post-obturation pain following single visit root canal treatment in Indian population:A prospective, randomized clinical trial. Contemp Clin Dent. 2012;3(4):459–63. doi: 10.4103/0976-237X.107440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.al-Omari MA, Dummer PM. Canal blockage and debris extrusion with eight preparation techniques. J Endod. 1995;21(3):154–8. doi: 10.1016/s0099-2399(06)80443-7. [DOI] [PubMed] [Google Scholar]
- 22.Gambarini G, Testarelli L, De Luca M, Milana V, Plotino G, Grande NM, et al. The influence of three different instrumentation techniques on the incidence of postoperative pain after endodontic treatment. Ann Stomatol (Roma) 2013;4(1):152–5. doi: 10.11138/ads.0152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Caviedes-Bucheli J, Moreno JO, Carreno CP, et al. The effect of single-file reciprocating systems on Substance P and Calcitonin gene-related peptide expression in human periodontal ligament. Int Endod J. 2013;46(5):419–26. doi: 10.1111/iej.12005. [DOI] [PubMed] [Google Scholar]
- 24.Caviedes-Bucheli J, Castellanos F, Vasquez N, Ulate E, Munoz HR. The influence of two reciprocating single-file and two rotary-file systems on the apical extrusion of debris and its biological relationship with symptomatic apical periodontitis. A systematic review and meta-analysis. Int Endod J. 2016;49(3):255–70. doi: 10.1111/iej.12452. [DOI] [PubMed] [Google Scholar]
- 25.Bonaccorso A, Cantatore G, Condorelli GG, Schäfer E, Tripi TR. Shaping ability of four nickel-titanium rotary instruments in simulated S-shaped canals. J Endod. 2009;35(6):883–6. doi: 10.1016/j.joen.2009.03.007. [DOI] [PubMed] [Google Scholar]
- 26.Krithikadatta J, Sekar V, Sudharsan P, Velumurugan N. Influence of three Ni-Ti cleaning and shaping files on postinstrumentation endodontic pain:A triple-blinded, randomized, controlled trial. Journal of conservative dentistry:JCD. 2016;19(4):311–6. doi: 10.4103/0972-0707.186442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Caviedes-Bucheli J, Azuero-Holguin MM, Gutierrez-Sanchez L, Higuerey- Bermudez F, Pereira-Nava V, Lombana N, et al. The effect of three different rotary instrumentation systems on substance P and calcitonin gene-related peptide expression in human periodontal ligament. J Endod. 2010;36(12):1938–42. doi: 10.1016/j.joen.2010.08.043. [DOI] [PubMed] [Google Scholar]