

Abstract
We present a case of reverse Z-effect phenomenon in a basicervical femoral fracture using a cephalomedullary nail together with two superior antirotation screws and evaluate the procedure. An 86-year-old woman fell in her home and could not stand due to right hip joint pain. X-ray and CT imaging showed a right basicervical femoral fracture (AO/OTA classification; 31B3), and open reduction and internal fixation (OR/IF) was performed with a cephalomedullary nail and two superior antirotation screws (TES Nail, HOMS, Tokyo, Japan). Two months later, X-ray showed penetration of the femoral head by the inferior lag screw with lateral migration of the two superior antirotation screws; the so-called “reverse Z-effect”; without any trauma. We performed the exchange of a shorter inferior lag screw for the longer one, and replaced the sliding type end cap with one of rocking type. The reverse Z-effect has been reported in cases with two lag screws, i.e. one inferior and one superior, in the past; however, to our knowledge, there has been no case reported in the literature using two superior antirotation screws together with one inferior lag screw.
Keywords: Reverse Z-effect, Basicervical femoral fracture, OR/IF, Cephalomedullary nail, Antirotation screw
Introduction
Hip fracture is one of the most common injuries in the elderly. The estimated number of hip fracture patients in Japan in 2007 was about 148,100 [1]. Surgical treatment is generally the first choice to regain walking ability, and open reduction and internal fixation is performed in most cases, as blood flow in the fractured bone fragment is usually relatively good, and synostosis can be expected in trochanteric femoral fractures. Recently, cephalomedullary nail has been a popular method of stabilization for such cases because of its less invasiveness compared to sliding hip screws [2]. Among trochanteric femoral fractures, basicervical femoral fractures are defined as fractures which occur medially from the intertrochanteric line above the lesser trochanter [3]. Deneca et al. reported that basicervical femoral fractures have larger rotational instability than most other types [4]. Therefore, an improved cephalomedullary nail was introduced with two proximal screws including an antirotation screw with the purpose of increasing the rotational stability of the fracture, and excellent post-operative results with it were reported [5,6]. Recently, we encountered one basicervical femoral fracture case that caused a rare phenomenon; “reverse Z-effect”; after the surgery using a cephalomedullary nail with two superior antirotation screws. This report describes the course, results of imaging studies, and surgical findings of that case.
Case report
An 86-year-old woman fell in her home and could not stand due to right hip joint pain, and she was carried to our hospital by ambulance. X-ray and CT scan showed a right basicervical femoral fracture (Fig. 1) (AO/OTA classification; 31B3), and she was admitted to our hospital for an emergency. Open reduction and internal fixation (OR/IF) (TES Nail, HOMS, Japan) was performed two days after the trauma using a cephalomedullary nail with a sliding type end cap, two superior antirotation screws, and one inferior lag screw. The two superior antirotation screws were 25 mm shorter than the inferior lag screw (Fig. 2). The patient was allowed full weight bearing from the day after surgery, and she was discharged from our hospital walking on her own with only a cane one month later. At two months after surgery, she felt sudden right hip joint pain without any trauma and visited our hospital again. X-ray showed penetration of the femoral head by the inferior lag screw with lateral migration of the two superior antirotation screws (Fig. 3). CT scan showed partial synostosis of the fractured bone fragment, and bone defect in the acetabulum was mild and restricted to a narrow region (Fig. 3). The inferior lag screw was replaced with a shorter one, and the sliding type end cap was replaced with one of the rocking type the day after admission (Fig. 4). She was allowed full weight bearing from the day after that surgery and discharged without pain two weeks later. At the last follow-up, 1 year thereafter, bone union had completed and the patient was able to walk alone, unaided, without any pain (Fig. 5).
Fig. 1.

Right basicervical femoral fracture.
Fig. 2.

Osteosynthesis with the cephalomedullary nail with two superior antirotation screws (Although the AR screws look like one because of their overlap, they are actually two).
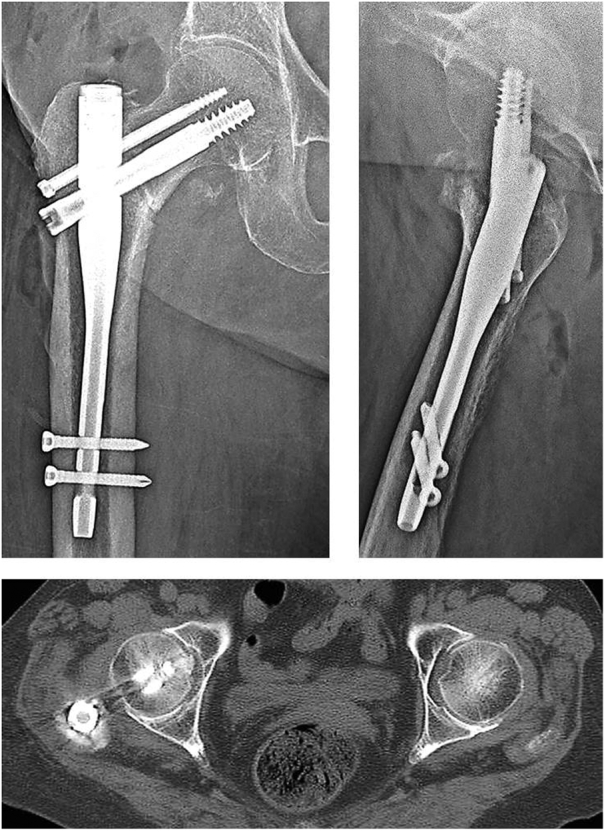
Fig. 3.

Reverse Z-effect phenomenon treated with cephalomedullary nail with two superior antirotation screws. The inferior lag screw has penetrated the femoral head into the acetabulum, and the superior antirotation screws have migrated laterally.
Fig. 4.
Second operation with replacement by shorter inferior lag screw and rocking type end cap.
Fig. 5.

Bone union in the right basicervical femoral fracture.
Discussion
Recently, in addition to the system of multiple lag screws, the telescoping lag screw system in the cephalomedullary nail has been developed to minimize the complication of lag screw cutout from the femoral head which leads to reoperation in trochanteric femoral fractures. However, cases involving Z-effect, wherein the superior lag screw penetrates the femoral head with lateral migration of the inferior lag screw, have been reported with this system. This is considered to be caused by adding power, like when bending, to a superior antirotation screw due to too great length of the superior antirotation screw [[7], [8], [9]]. Kubiak et al. described that using two lag screws sometimes caused Z-effect, which does not occur when using only one lag screw, while both methods showed equivalent rigidity and stability in elastic and cyclical tests [10]. Therefore, using antirotation screws that are 20–25 mm shorter than the inferior lag screw is currently recommended to prevent the Z-effect. In the present case, two superior antirotation screws, 25 mm shorter than the inferior lag screw were used. As a result, the inferior lag screw penetrated the femoral head, and the “reverse Z-effect” occurred with a lateral migration of the two superior antirotation screws and a medial penetration of the inferior lag screw.
In the past, reverse Z-effect has been reported in cases using a two lag screw operation [[7], [8], [9]]. Tyllianakis et al. described that five cases of Z-effect and one case of reverse Z-effect were noted in 46 unstable pertrochanteric fractures for which OR/IF was performed using proximal femoral nail with two lag screws in 20 months mean follow-up period [9]. However, to our knowledge, there has been no report regarding using two superior antirotation screws and one inferior lag screw in the literature. It has been theorized that the Z-effect is caused by comminution of the femoral medial cortex and varus positioning of the fixation. Strauss et al. reported that they were able to reproduce the Z-effect phenomenon by repetition of compressive loading to bone model using solid polyurethane foam, however, the reverse Z-effect was not observed after cyclic compressive loading at all [11]. Although medial vector force that is caused by weight bearing to inferior lag screw is supposed to be involved in the mechanism of reverse Z-effect, the exact etiology has not been completely explained yet.
It should be expected that the presence of two shorter superior antirotation screws would dynamically increase the sliding force over that of a single superior antirotation screw. Based on this assumption, a relative shortness of superior antirotation screw length, compared to the inferior lag screw, might lead to the lateral migration of those two superior antirotation screws and medial penetration of the femoral head by the inferior lag screw as an opposite reaction due to weight bearing (Fig. 6). Zirngibl et al. described that if the antirotation screw is too long or too short for the inferior lag screw, it would lead to fixation failure including cut-out, Z-effect and reverse Z-effect [12]. In summary, it must always be noted that the antirotation screw is in the optimum position with respect to the inferior lag screw in order to prevent reverse Z-effect.
Fig. 6.

Schema of reverse Z-effect phenomenon.
Conclusion
Postoperative complications in intramedullary proximal femoral nail include implant breakage, lateral migration of lag screws, cutout through the femoral head, fracture of the lateral trochanteric wall, and Z or reverse Z-effect. Reverse Z-effect is a rare complication, and its onset mechanism has been not yet been completely elucidated. The optimal length of the two superior antirotation screws compared to the inferior lag screw length must be clarified in future research.
Funding
No funds have been received in support of this work. No benefits in any form have been or will be received from a commercial party related to, directly or indirectly, the subject of this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent was obtained from the patient in this article.
Declaration of competing interest
The authors declare that they have no conflicts of interest.
References
- 1.Orimo H. Hip fracture incidence in Japan: estimates of new patients in 2007 and 20-year trends. Arch. Osteoporos. 2009;4:71–77. doi: 10.1007/s11657-009-0031-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Warren J.A. Cephalomedullary nailing versus sliding hip screws for intertrochanteric and basicervical hip fractures: a propensity-matched study of short-term outcomes in over 17,000 patients. European Journal of Orthopaedic Surgery & Traumatology: orthopedie traumatology. 2020;30:243–250. doi: 10.1007/s00590-019-02543-y. [DOI] [PubMed] [Google Scholar]
- 3.Blair B., Koval K.J., Kummer F., Zuckerman J.D. Basicervical fractures of the proximal femur. A biomechanical study of 3 internal fixation techniques. Clin. Orthop. Relat. Res. 1994:256–263. [PubMed] [Google Scholar]
- 4.Deneka D.A. Biomechanical comparison of internal fixation techniques for the treatment of unstable basicervical femoral neck fractures. J. Orthop. Trauma. 1997;11:337–343. doi: 10.1097/00005131-199707000-00007. [DOI] [PubMed] [Google Scholar]
- 5.Zelle B.A. Safety and efficacy of a two-screw cephalomedullary nail for intertrochanteric femur fracture fixation: a retrospective case series in 264 patients. Patient Saf. Surg. 2018;12:31. doi: 10.1186/s13037-018-0177-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang Q. Management of low-energy basicervical proximal femoral fractures by proximal femoral nail anti-rotation. Orthop. Surg. 2019;11:1173–1179. doi: 10.1111/os.12579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Werner-Tutschku W. Intra- and perioperative complications in the stabilization of per- and subtrochanteric femoral fractures by means of PFN. Unfallchirurg. 2002;105:881–885. doi: 10.1007/s00113-002-0416-5. (in German) [DOI] [PubMed] [Google Scholar]
- 8.Boldin C. The proximal femoral nail (PFN)—a minimal invasive treatment of unstable proximal femoral fractures: a prospective study of 55 patients with a follow-up of 15 months. Acta Orthop. Scand. 2003;74:53–58. doi: 10.1080/00016470310013662. [DOI] [PubMed] [Google Scholar]
- 9.Tyllianakis M., Panagopoulos A., Papadopoulos A., Papasimos S., Mousafiris K. Treatment of extracapsular hip fractures with the proximal femoral nail (PFN): long term results in 45 patients. Acta Orthop. Belg. 2004;70:444–454. [PubMed] [Google Scholar]
- 10.Kubiak E.N. Intramedullary fixation of unstable intertrochanteric hip fractures: one or two lag screws. J. Orthop. Trauma. 2004;18:12–17. doi: 10.1097/00005131-200401000-00003. [DOI] [PubMed] [Google Scholar]
- 11.Strauss E.J., Kummer F.J., Koval K.J., Egol K.A. The “Z-effect” phenomenon defined: a laboratory study. Journal of Orthopaedic Research: official publication of the Orthopaedic Research Society. 2007;25:1568–1573. doi: 10.1002/jor.20457. [DOI] [PubMed] [Google Scholar]
- 12.Zirngibl B., Biber R., Bail H.J. How to prevent cut-out and cut-through in biaxial proximal femoral nails: is there anything beyond lag screw positioning and tip-apex distance? International Orthopaedics (SICOT) 2013;37:1363–1368. doi: 10.1007/s00264-013-1898-1. [DOI] [PMC free article] [PubMed] [Google Scholar]