

Key Points
Question
What is the extent to which uveal melanoma treatment is curative?
Findings
In this integrative analysis, excess absolute risks of uveal melanoma deaths in SEER data showed 2 waves, 1 peaking at approximately 3 years and the other peaking at approximately 15 years. Institutional data suggest that the first wave represents BAP1 mutant cases and the second wave SF3B1 mutant cases, and a third group with a flat excess absolute risks of death of approximately 0 dominates cohorts beyond 15 years.
Meaning
This analysis raises questions about the survival benefits of ocular therapy.
Abstract
Importance
The extent to which uveal melanoma is cured by ocular therapy is not known.
Objective
To estimate cured fractions (CF) of uveal melanoma using combination of institutional and Surveillance, Epidemiology, and End Results (SEER) data.
Design, Setting, and Participants
Integrative analysis of 42 years of SEER data (1975-2016) with 25 years (1993-2018) of complementary institutional data. The analysis included SEER US patients and molecularly prognosticated patients in the United States and Europe. Three SEER databases (SEER-9, SEER-13, and SEER-18) were merged. A total of 10 678 SEER cases of uveal melanoma diagnosed from 1975 to 2016 using International Classification of Disease for Oncology morphology codes 8720-8790 (for melanoma) and site codes C69.2-4 (for choroid, ciliary body, and iris) were downloaded April 16, 2019. The institutional data included 5 institutional cohorts of 788 molecularly prognosticated patients (diagnosed prior to July 2019) with 3115 person-years at risk of death and 262 observed deaths.
Main Outcomes and Measures
Excess absolute risks of death (EAR) and cured fraction (CF) indicates lifetime area under the EAR curve. These are applied to populations and subpopulations.
Results
The SEER EAR, with sexes and races pooled, can be modeled as a sum of 2 waves. The first wave peaks at approximately 3 years and is negligible by 15 years, at which time the second wave peaks. Institutional data suggest that the first wave is owing to BAP1 mutant cases (204 of 355 [57.5%]; 95% CI, 52%-63%) and that the second wave is owing to BAP1 wild-type SF3B1 mutant cases (60 of 355 [17%]; 95% CI, 13%-21%). There is also a third group with a low flat EAR time course (91 of 355 [25.5%]; 95% CI, 21%-30%). The overall statistical CF of 60% is reached by approximately 25 years.
Conclusions and Relevance
These findings suggest that the benefits of ocular therapy for curing uveal melanoma may be questionable because statistical cures reflect deaths of poor prognosis cases and survival of good prognosis cases. Changes in uveal melanoma patient management may be needed to improve survival.
This study estimates cured fractions (CF) of uveal melanoma using a combination of institutional and epidemiologic data.
Introduction
An early rise in uveal melanoma mortality after enucleation was first observed by Zimmerman et al,1 who attributed it to metastatic cells being released by the surgery. Since then, such early increases in mortality after ocular therapy have been observed in patients treated not only with enucleation but also with episcleral plaque radiation therapy2 and proton beam radiation therapy.2,3 The mortality peak thus reflects the natural evolution of the disease. After the peak, mortality rates return toward baseline, rapidly at first and then more slowly, becoming negligible approximately 25 years after ocular therapy.4
National population-based cancer registries, such as the Surveillance, Epidemiology, and End Results (SEER) Program, are rich resources of unselected data collected over decades. Such data are amenable to specialized forms of survival analysis wherein a statistical (ie, population-level) cure is achieved when relative survival plateaus, or equivalently, when excess absolute risks of death (EAR) return to a normal zero value. Complementing such data are institutional data that characterize the genetic landscape (mutational status) of uveal melanoma. In this study, such data provide a basis for biologic interpretation of waveforms underlying the SEER EAR time course.
The goal of this study was to integrate uveal melanoma SEER data and molecularly prognosticated patient data to assess the fraction of patients who survive through times of excess mortality. Conditional on parametric models of EAR, we estimated subtype and total times to cure and fraction of patients alive at time to cure, ie, cured fractions (CF).
Methods
For SEER data that are deidentified and publicly available, institutional review board approval was not needed. For inclusion of the institutional deidentified data set, institutional review board approval was obtained from the Cleveland Clinic, Cleveland, Ohio.
SEER Data
The SEER data were processed and analyzed using the R package SEERaBomb (the R Foundation).5 This software merges all 3 SEER databases (SEER-9, SEER-13, and SEER-18) to provide more cases than can be retrieved conventionally using SEER*stat. It also accesses background US mortality rates in the Human Mortality Database (https://www.mortality.org/). Uveal melanoma cases were identified using International Classification of Disease for Oncology (ICD-O-3) morphology (melanoma: 8720-8790) and site (C69.3 [choroid], C69.4 [ciliary body and iris], and C69.2 [retina]) codes.6 Diagnoses occurred between January 1, 1975, and December 31, 2016.
Institutional Data
Published data sets of molecularly prognosticated patients were pooled.7,8,9,10 These patients had undergone tumor sample analysis using 1 or more of the following molecular techniques: fluorescent in situ hybridization (FISH), gene expression profiling (GEP), and mutation analysis using whole-exome sequencing followed by validation with Sanger sequencing (SS) or targeted next-generation sequencing (NGS). Diagnoses of these patients occurred over the last 25 years (between 1993 and 2018). Good-prognosis patients were those with tumors having disomy chromosome 3 (FISH),7 class 1 (GEP),8 and absence of BAP1 or SF3B1 gene mutation (SS and NGS).9,10 Bad-prognosis patients had monosomy 3 by FISH,7 class 2 GEP,8 or presence of a BAP1 or SF3B1 gene mutation by NGS.9,10 Tumor size was classified as small (stage 1, defined by the American Joint Committee on Cancer, 7th edition) vs large (American Joint Committee on Cancer stage 3 or 4) (Table).11
Table. Institutional Dataa.
| Variable | No. | Source/comment |
|---|---|---|
| Age, median (range), y | 62 (16-92) | NA |
| Sex | ||
| Male | 405 | NA |
| Female | 383 | |
| Tumor size | ||
| Small | 105 | Classified as small (stage 1), medium (stage 2), large (stage 3 or 4) as defined by the American Joint Committee on Cancer, 7th edition11 |
| Medium | 210 | |
| Large | 161 | |
| Prognostic method | ||
| FISH | 148 | Singh et al, 20167 |
| GEP | 215 | Brinkley et al, 20208 |
| Whole-exome sequencing and SS | 312 | Yavuzyigitoglu et al, 201610 |
| NGS | 113 | Thornton et al, 20209 |
| Prognosis group | ||
| Good prognosis | 237 | Tumors having disomy chromosome 3 (FISH), class 1 (GEP), absence of BAP1 or SF3B1 gene mutation (SS, NGS) |
| Bad prognosis | 353 | Tumors having monosomy chromosome 3 (FISH), Class 2 (GEP), presence of BAP1 or SF3B1 gene mutation (SS, NGS) |
| Mutation status | ||
| BAP1 mutant | 204 | In only those tested (n = 355) |
| SF3B1 mutant | 60 | |
| Wild type | 91 | |
| Systemic status | ||
| Alive | ||
| With metastasis | 11 | NA |
| Without metastasis | 506 | NA |
| Dead | ||
| With metastasis | 162 | NA |
| Without metastasis | 109 | NA |
Abbreviations: FISH, fluorescent in situ hybridization; GEP, gene expression profiling; NA, not applicable; NGS, next-generation sequencing; SS, Sanger sequencing.
Pooled data sets of molecularly prognosticated patients. Sources and profile (n = 788). Tumor samples were analyzed by FISH, GEP, or, to detect mutations, whole-exome sequencing validated by SS or targeted NGS.
Two-way Analysis of Variance–Like EAR Analyses
Values of EAR = (O−E)/PY were computed from O, E, and PY, generated by the SEERaBomb R function mortality since diagnosis (msd). Here O is the number of observed deaths, E is the number of expected deaths, and PY is the number of person-years at risk of death. The EAR time courses were analyzed for differences between age groups by Poisson regression, assuming O is Poisson distributed with mean ec × PY+E, letting c depend on group and time interval additively, as in a 2-way analysis of variance model. Throughout, no adjustments were made for multiple testing.
Waveform EAR Analyses
The excess hazard he(t) was modeled as sum of a triangle wave and a γ function wave that was fitted to EAR. The γ wave is k2 × (t/2) × e(c-kt) for t > 0 and the triangle wave is m1t for 0 < t < t1, m1 × t1 − ([m1 × t1] / [t2 − t1])(t2 − t1) for t1 < t < t2, and 0 for t > t2. In the γ wave, k is a time-scale parameter and c is an amplitude parameter (c = 0 yields an area under the curve [AUC] of 1). In the triangle wave, t1 is the time of the peak, m1 is the slope up to it, and t2 is the time to cure. We fitted he(t) to EAR = (O−E)/PY by fitting Oti distributed as Pois (he (ti) × Yti + Eti) using Poisson regression (using the R function mle2 in the R package bbmle). Here ti are PY-weighted centroids of user-defined time intervals since diagnosis. For SF3B1 mutant cases, only the rising edge of the triangle wave was fitted.
Cured Fraction
The AUC is the lifetime excess expected number of deaths per person diagnosed. The Poisson probability of zero excess deaths (ie, of not being killed by the uveal melanoma) is then exp(−AUC). This is the CF. Where molecularly prognosticated data were too sparse to apply EAR methods (owing to time intervals with 0 deaths), we used Kaplan-Meier estimates12 of metastasis-free survival.13,14 The log-rank test was used to determine statistical significances of survival curve differences. All P values were 2-sided, and a P value less than .05 was considered significant.
Results
SEER Data
In the 10 678 uveal melanoma cases diagnosed between 1975 and 2016, EAR peaked at 0.056 (an additional 5.6% chance of death per year) in the interval of 2 to 3 years, rapidly fell to 0.022 in the interval of 8 to 10 years, and slowly tapered to approximately 0 by approximately 25 years (Figure 1A; eTable 1 in the Supplement). Using a 2-way ANOVA-like model, EAR amplitudes differed by age (Figure 1B and eTable 2 in the Supplement; P < .001) in favor of patients 60 years or younger as compared with patients older than 60 years, but not by sex (P = .46; t = 0.72). The EAR AUC of Figure 1A was 0.512, so the CF is e−.512 = 0.60 (Figure 1C). The EARs are well approximated by a sum of γ and triangle waves (Figure 1D); wave AUCs of 0.212 (triangle) and 0.34 (γ) yield a CF of e−(0.212 + 0.34) = 0.57.
Figure 1. Surveillance, Epidemiology, and End Results (SEER) Data.
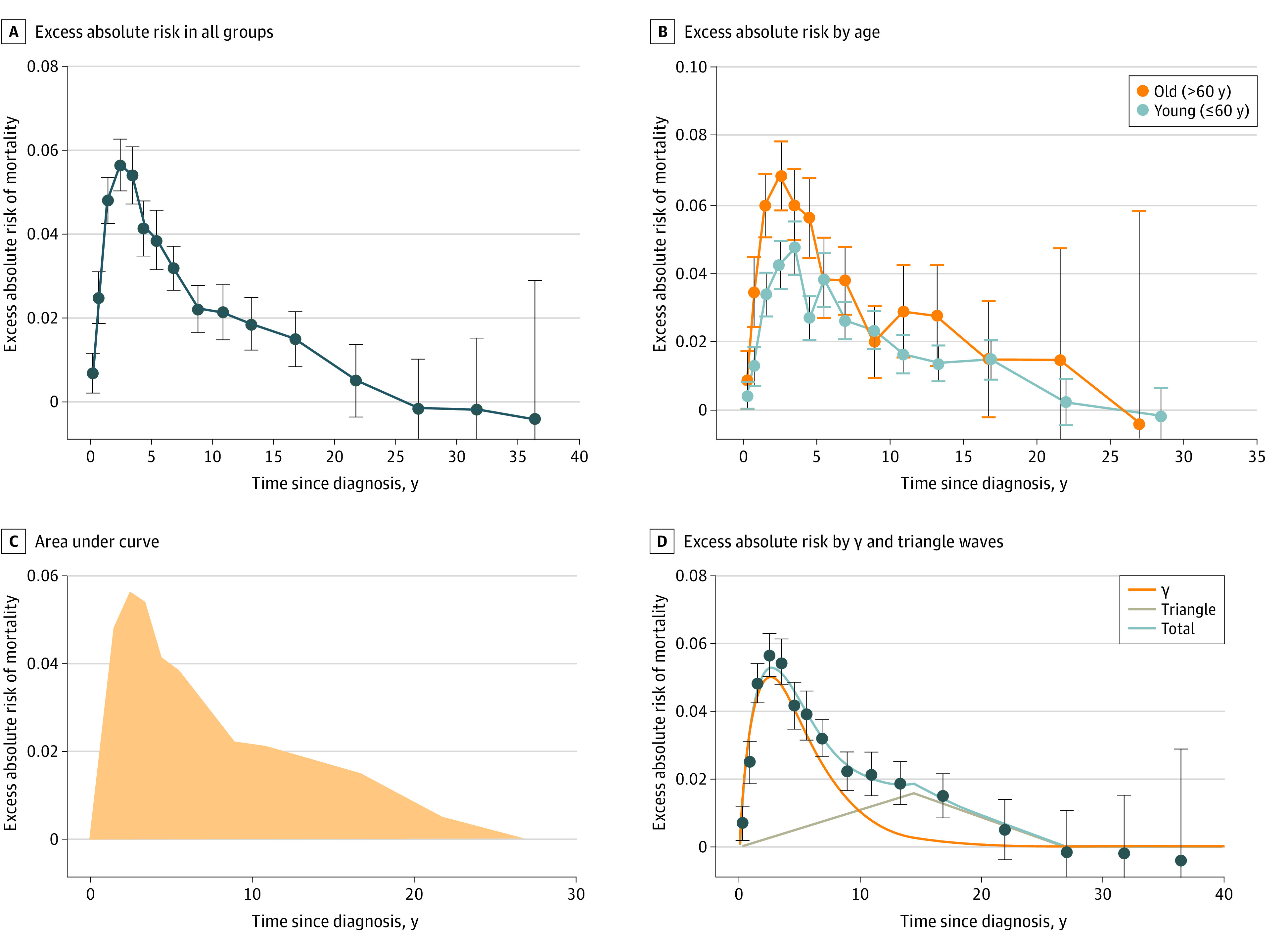
With all groups pooled (A), excess absolute risks of death (EAR) peaks to 0.056 in times greater than 2 years and 3 years or less, rapidly falls to 0.022 between 8 and 10 years, and slowly tapers thereafter to approximately 0 by year 25 (time to cure). Negative EAR estimates and 95% confidence interval values imply better-than-average survival in that interval. Person-years at risk and numbers of observed deaths in each interval are given in eTable 1 in the Supplement. The EAR amplitude depends on age (B; P < .001). The age cutoff of 60 years was chosen as an approximation of the median age of 63 years. Error bars are 95% confidence intervals. The person-years and number of observed death values are provided in eTable 2 in the Supplement. The area under the curve in (A) is 0.512 (C); therefore, cured fraction (CF) = e−0.512 = 0.60. The sum of the γ function wave and triangle wave yield a reasonable fit to pooled EAR values (D). The areas under the curve of 0.212 for the triangle wave and 0.34 for the γ wave yield a CF of e−(0.212 + 0.34) = 0.57, which is similar to the model-free estimate of 0.60 in (C).
Institutional Data
A total of 788 molecularly prognosticated cases with the median follow-up among survivors of 4 years (range, 0-25) were available for analysis. A total of 271 patients died from any cause and of these deaths, 173 were owing to metastasis. Kaplan-Meier survival probabilities differed between small and large tumors (Figure 2A) and good-prognosis and bad-prognosis tumors (Figure 2B). These factors cancel each other prognostically because there was no difference between small bad-prognosis and large good-prognosis tumors (Figure 2C). No patients with small good-prognosis tumors died of metastasis (Figure 2D). Pooling cases across tumor sizes, EARs differed between good-prognosis and bad-prognosis groups (Figure 3A; χ2 = 88.9; P < .001). Shapes of the EAR time courses of the BAP1 and SF3B1 mutant subpopulations (Figure 3B; eTables 3 and 4 in the Supplement) resembled the γ and triangle wave subcomponents of the EAR time course of the full SEER population (Figure 2D), suggesting that the SEER γ wave may be owing to BAP1 mutant cases (or equivalents based on GEP) and that the SEER triangle wave may be owing to SF3B1 mutant cases.
Figure 2. Kaplan-Meier Plots of Survival Probabilities of Patients in Prognostic Subsets.
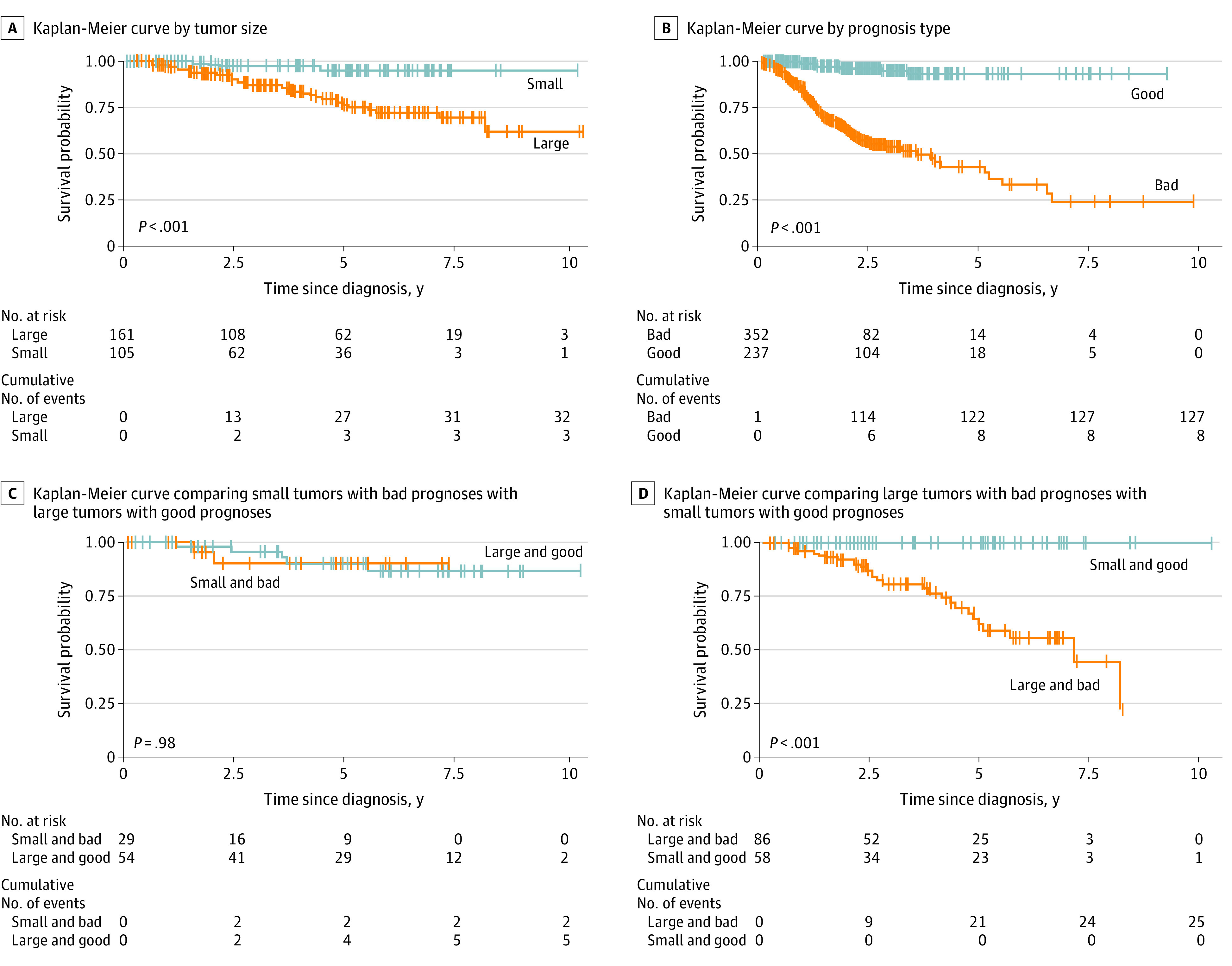
Statistically significant differences in survival are evident when small tumors are compared with large tumors (A) and when good prognostic tumors are compared with bad prognostic tumors (B). No difference in survival was observed when small bad prognostic tumors were compared with large good prognostic tumors (C). None of the patients with small good prognostic tumors died of metastasis (D).
Figure 3. Excess Absolute Risks for Patients With Good Prognoses, Bad Prognoses, Both Combined (All), and Surveillance, Epidemiology, and End Results (SEER) Patients as a Reference.
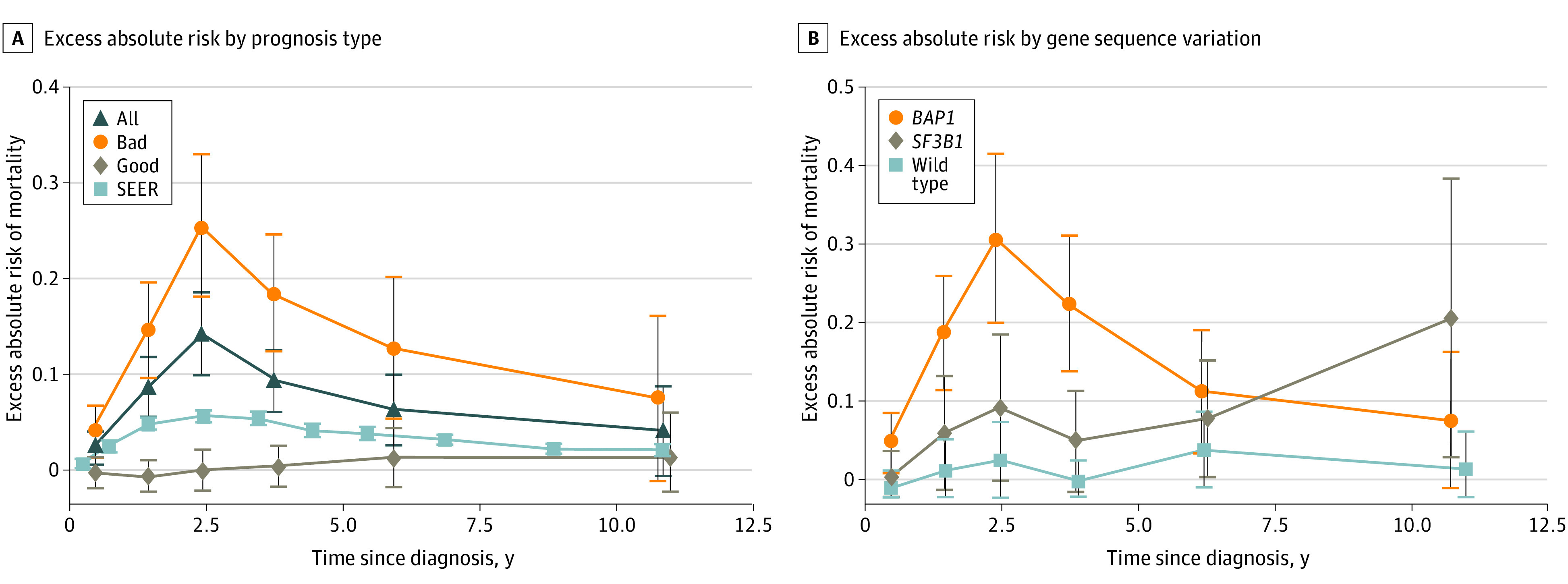
The amplitude difference between the good and bad prognosis groups is significant at P < .001. The excess absolute risk time courses of BAP1 and SF3B1 mutant cases (B) are similar to the γ and triangle waveforms in Figure 1D. For observed deaths and person-years (PY) at risk in each interval, see eTables 3 and 4 in the Supplement.
Cured Fraction Estimates
To estimate subpopulation-specific CF, we fitted the γ wave to EAR of BAP1 mutated patients (Figure 4A) and a straight line to EAR for SF3B1 mutant cases (Figure 4B). This yielded CFs of 18% and 0%, respectively. To associate these estimates with SEER data, we note that of 355 Rotterdam10 and Liverpool9 study patients with mutational analysis, 204 (57.5%; 95% CI, 52%-63%) were BAP1 mutated, 60 (17%; 95% CI, 13%-21%) were SF3B1 mutated (7 mutated in both genes were scored as BAP1 mutants), and 91 (25.5%; 95% CI, 21%-30%) were wild type at both loci. Assuming in SEER data then that 58% were BAP1 mutated, 17% SF3B1 mutated, 25% have an EAR of 0, and that the γ wave and linear model fits in Figures 3A and B also apply to SEER data, by 25 years, 80% of patients with BAP1 mutant cases have died and 20% are alive (ie, 12% of the total cohort are alive), and all patients with SF3B1 mutant cases have died; therefore, the apparent cure rate is 37%. We note that owing to SF3B1 mutant subpopulation deaths, linearity extended beyond the data in Figure 3B is compatible with a falling triangle wave slope over 15 to 25 years in the overall population average that is measured epidemiologically using SEER data in Figure 1D.
Figure 4. Subpopulation Excess Absolute Risk (EAR) Fits.
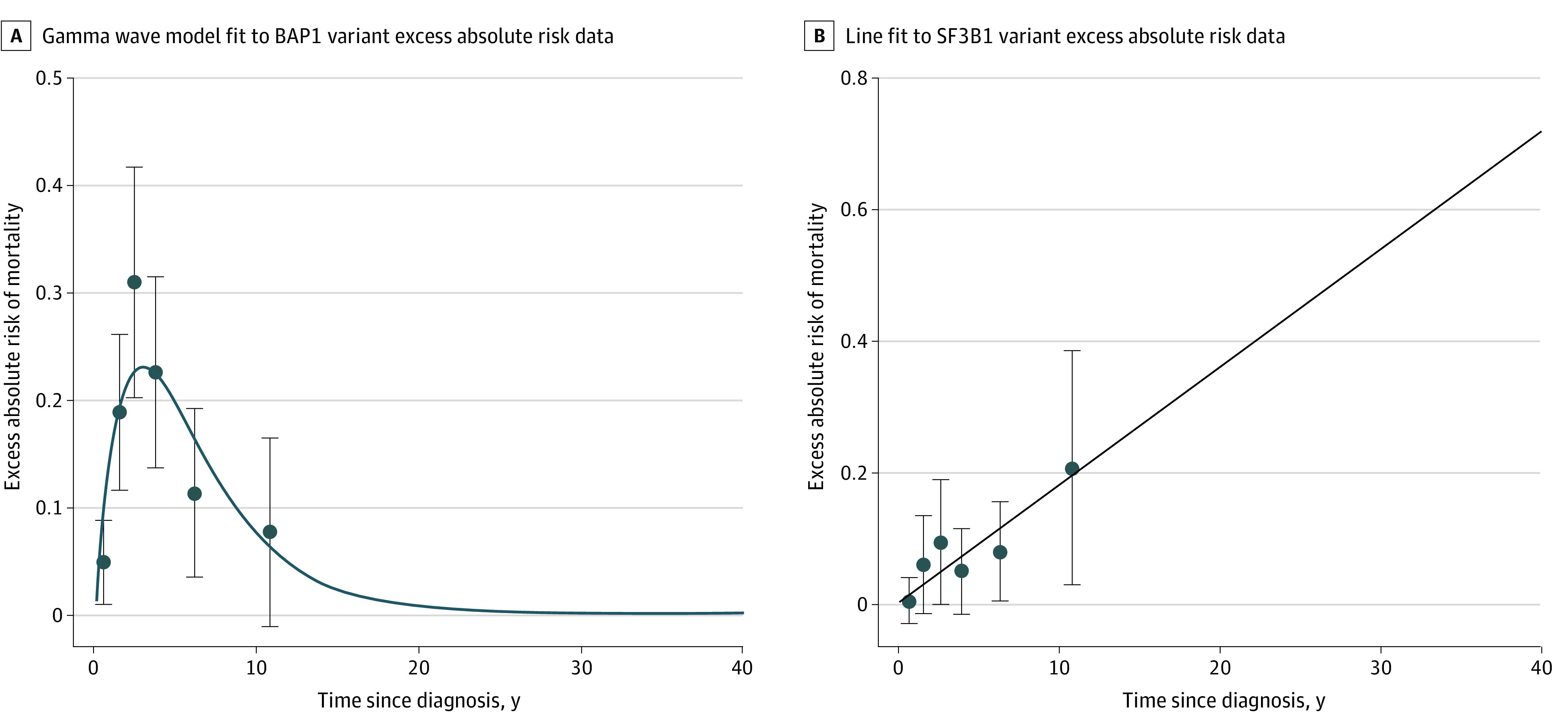
Fitting the γ wave model to BAP1 mutant EAR data yields the curve in (A) and estimates (SE) of the γ wave amplitude (c) and shape (k) parameters: c = 1.31 (0.18) and k = 0.335 (0.049). Fitting a line (though the origin) to SF3B1 mutant EAR data yields a slope of 0.018 (0.0044) (B). Data are as in Figure 3B (observed deaths and person-years at risk in each interval are provided in eTable 4 in the Supplement).
Competing Risks
The analysis of the previous section predicts that no SF3B1 mutant cases will ever be cured. However, the indolent nature of the SF3B1 mutant EAR time course suggests that a substantial proportion of these patients will die of other causes. Similarly, some patients with BAP1 mutant cases will also die of competing causes of death. Competing risks might thus explain a major portion of the difference between the apparent cure rate of 37% predicted in previous sections and a statistical cure rate of 60% estimated from SEER data in Figure 1A and 1C.
Discussion
When does the long-term survivorship translate into cure from uveal melanoma? The SEER data alone yield a statistical CF of approximately 60% at 25 years (Figure 1A and 1C). It also yields 2 EAR waves of death, a γ wave responsible for the initial peak at 2 to 4 years, and a triangle wave responsible for the slow taper between 9 and 25 years (Figure 1D). Although expressed differently, our observations are consistent with what has been reported previously. Lane et al3 reported annual rates of death decreasing gradually after year 6 and dropping to less than 1% at 14 years after treatment. This is consistent with a Finnish study reporting that 90% (95% CI, 84%-95%) of the uveal melanoma deaths occur within 15 years4 and a Swedish study, also using EAR methods, reporting that excess mortality vanished by about 15 years.15
Our SEER-based CF estimate of 60% is similar to the proportion of patients with good prognoses in published studies16,17,18,19,20,21 and in independent data sets.7,8,9,10 Augsburger et al22 noted a relationship between the fraction of metastatic deaths and the proportion of patients with bad prognostic status, but their observations22 lacked statistical support provided here. There are only a few references to uveal melanoma CF.4,23 Gamel et al16 in 1992 calculated CF as the asymptote of the log normal cause-specific survival function to report that large tumor sizes (>16.0 mm in basal diameter) and pleomorphic nucleoli (features that correlate with bad prognosis by molecular classification)16 were associated with low CF.16,23 Their observed CF in 2892 patients treated with enucleation was 52% at 15 years, which is similar to our estimate. To our knowledge, the only other CF estimate was 62% by Kujala et al,4 who, in their analysis of 289 patients, referred to it as an overall immune fraction.4 They suspected this implied a CF of 62% but could be confident only among those with tumors involving the ciliary body or those who had extrascleral extensions.4 Our SEER-based CF of 60% is thus well supported by other reports.
When we associate EAR curves of molecularly defined patients with SEER EAR curves, it becomes evident that the mortality is predominantly driven by the bad-prognosis group (Figure 3A). Based on mathematical modeling, 3 subpopulations are proposed to exist, a BAP1-mutated population that underlies the SEER EAR γ wave, a SF3B1-mutated population that underlies the triangle wave, and a subpopulation wild type at both of these loci with approximately normal life expectancies (Figure 2D). The BAP1-mutated subpopulation has an EAR that may return to zero. In contrast, the EAR of the SF3B1 subpopulation continues to rise (Figure 3B). We are able to replicate observations by Grossniklaus et al,24 who elegantly showed that the early rise in yearly metastatic rate (peaks at 1.0-3.5 years with return to baseline at 5 years) and the later peak at 7 years were associated with with somatic tumor mutations in BAP1 and SF3B1, respectively.24 Because metastasis is not an inevitable event with the presence of BAP1 mutation, we need to understand the biologic/cellular mechanisms that trigger cell death or prevent cell death (such as ferroptosis)25 in the presence of mutations and the role of host factors.26
The third subgroup, representing perhaps 30% to 40% of the initial total, has approximately a normal life expectancy that leads to its dominance of cohorts by approximately 25 years. Kaplan-Meier analysis by size and prognostication status showed that both tumor size and prognostication group are associated with survival probability (Figure 2A and B)19 and that small tumors with good prognostic status were free of metastatic death in these data and therefore most likely to be cured.17 Those with large tumors and bad prognostic status had the highest probability of metastatic death and were therefore least likely to be cured (Figure 2D). Because molecular prognostic tests have been incorporated into clinical use for only about 10 years, we are unable to analyze the effect of prognostic categories on the EAR beyond that period. We estimate that perhaps 20% of high-risk individuals (bad prognostic status or large tumors) and most low-risk patients (good prognostic status or small tumors) survive the main peak of metastatic mortality.
Time to cure is the time at which the overall EAR reaches 0 (approximately 25 years) (Figure 1A).27,28 We would be cautious and use the term of statistical cure because these population average estimates are not applicable to individual patients.27 It is important to stress that EAR estimates are stable, having not changed in the past few decades (eFigure in the Supplement).6 This simplifies and indeed enables the analysis presented here because old data are then directly relevant to the future. Given the low risks of metastatic events beyond 15 years,3,4,29,30 discontinuation of the systemic surveillance31 may be reasonable to consider for those with good prognoses.
Time to cure of approximately 25 years implies that they occur late in life and are unlikely to be related to ocular therapy.27 It may be more appropriately thought of as the time since ocular therapy, by which most risk of metastatic death has been manifested. In other words, a CF of approximately 25 years largely reflects deaths among patients with a poor prognosis. This raises questions about the survival benefits of ocular therapy. Currently prescribed ocular therapy, at least for high-risk patients (bad prognostic status and/or large tumor size), seems to be palliative rather than curative.32,33,34 Damato34 and Afshar and Damato35 have explored hypothetical scenarios with varying assumptions regarding natural history and possible survival benefit of ocular therapy.34,35 Augsburger et al22 postulated that the ocular therapy had no effect on risk of metastasis in bad prognostic cases because metastasis had already happened and was not going to happen in those with good prognosis. Our analysis supports the position that high-risk patients are being undertreated and suggests consideration of adjuvant therapy in such patients.36,37
Conversely, the question of whether low-risk patients (good prognostic status and/or small tumor size) are being overtreated exists. In the absence of randomized clinical trials (which may be unethical),34,38 we can only be guided by indirect evidence regarding the efficacy of ocular therapy. For small tumors with good prognoses, initial observation may be an option, particularly in patients who are asymptomatic or those who are likely to lose vision from therapeutic intervention because none of the patients with such tumors died of metastatic uveal melanoma (Figure 2D).17
Several inferences regarding molecular prognostication can be drawn from the long-term mortality patterns reported here. First, prognostic biopsies should be considered in all cases, including small choroidal melanoma, because they can guide the timing and type of local therapeutic intervention. Second, current practice of classifying patients broadly into good and bad prognostic groups is not only test dependent39,40 but also insufficient because the mortality pattern within the bad prognosis group is at least of 2 subtypes (early vs late) and seems to be driven by genetic profile (mutations).9,10,41,42 Hence, mutational subtyping of uveal melanoma might be the preferred method for prognostication. Finally, eligibility criteria for adjuvant trials should be based on mutational subtyping because the targets and effects of investigational targeted therapy are likely to be mutation specific and the expected effect on mortality (early vs late) would have to be considered when designing study protocols. Although searches for additional genes continue,43,44 it appears the major genes implicated in uveal melanoma mortality have already been identified, accounting for most of early mortality and perhaps all of delayed mortality. Current prognostication into 3 mutation groups is thus expected to continue to cover most cases.
Our observations are supported by various lines of existing evidence: micrometastases are early events in uveal melanoma,45,46 patients with small tumors and good prognostic status do not manifest metastasis,17 commonly performed therapies of primary uveal melanoma (episcleral brachytherapy and enucleation) have equivalent survival benefits,47 and the survival of patients has remained unchanged for the last 40 years despite incremental improvements in local therapy.6 Additionally, we believe survival outcomes partitioned into the molecularly characterized subpopulations reported herein are an extension of predicted metastatic behavior of 2 distinct evolutionary pathways of uveal melanoma metastasis.48,49,50,51
Limitations
Although SEER cancer registry data52 are the source of summary statistics that are published annually as the national cancer report in the United States,53 and although it meets long-term analyses prerequisites of large numbers of patients6 and long follow-up,54 the cause of death as determined from death certificates may be erroneous. By using the Human Mortality Database to form EARs, we avoid this cause of death limitation of SEER data. A limitation of the institutional data used is that, despite long follow-up for some patients prognosticated with mutational analysis, insufficient numbers of such patients remained in the at-risk set beyond 10 years to confidently estimate survival past this point and truly assess long-term survival. As such, our results need to be verified using other data sets.
Conclusions
In conclusion, SEER and institutional data combined suggest that a statistical cure rate of 60% at approximately 25 years largely reflects deaths among patients with a poor prognosis. This raises questions about the survival benefits of ocular therapy and suggests that changes to current uveal melanoma patient management are needed to increase survival.
eFigure. Mortality in the US has not changed much in 40 years
eTable 1. Full results underlying Figure 1A
eTable 2. Full results underlying Figure 1B
eTable 3. Full results underlying Figure 3A
eTable 4. Full results underlying Figure
References
- 1.Zimmerman LE, McLean IW, Foster WD. Does enucleation of the eye containing a malignant melanoma prevent or accelerate the dissemination of tumour cells. Br J Ophthalmol. 1978;62(6):420-425. doi: 10.1136/bjo.62.6.420 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Singh AD, Rennie IG, Kivela T, Seregard S, Grossniklaus H. The Zimmerman-McLean-Foster hypothesis: 25 years later. Br J Ophthalmol. 2004;88(7):962-967. doi: 10.1136/bjo.2003.029058 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lane AM, Kim IK, Gragoudas ES. Long-term risk of melanoma-related mortality for patients with uveal melanoma treated with proton beam therapy. JAMA Ophthalmol. 2015;133(7):792-796. doi: 10.1001/jamaophthalmol.2015.0887 [DOI] [PubMed] [Google Scholar]
- 4.Kujala E, Mäkitie T, Kivelä T. Very long-term prognosis of patients with malignant uveal melanoma. Invest Ophthalmol Vis Sci. 2003;44(11):4651-4659. doi: 10.1167/iovs.03-0538 [DOI] [PubMed] [Google Scholar]
- 5.Radivoyevitch T, Sachs RK, Gale RP, et al. . Defining AML and MDS second cancer risk dynamics after diagnoses of first cancers treated or not with radiation. Leukemia. 2016;30(2):285-294. doi: 10.1038/leu.2015.258 [DOI] [PubMed] [Google Scholar]
- 6.Aronow ME, Topham AK, Singh AD. Uveal melanoma: 5-year update on incidence, treatment, and survival (SEER 1973-2013). Ocul Oncol Pathol. 2018;4(3):145-151. doi: 10.1159/000480640 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Singh AD, Medina CA, Singh N, Aronow ME, Biscotti CV, Triozzi PL. Fine-needle aspiration biopsy of uveal melanoma: outcomes and complications. Br J Ophthalmol. 2016;100(4):456-462. doi: 10.1136/bjophthalmol-2015-306921 [DOI] [PubMed] [Google Scholar]
- 8.Binkley EM, Bena JF, Davanzo JM, Hinz C, Boldt HC, Singh AD. Gene expression profiling prognostication of posterior uveal melanoma: does size matter? Ophthalmol Retina. 2020;4(6):620-629. [DOI] [PubMed] [Google Scholar]
- 9.Thornton S, Coupland SE, Olohan L, et al. . Targeted next-generation sequencing of 117 routine clinical samples provides further insights into the molecular landscape of uveal melanoma. Cancers (Basel). 2020;12(4):E1039. doi: 10.3390/cancers12041039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yavuzyigitoglu S, Koopmans AE, Verdijk RM, et al. ; Rotterdam Ocular Melanoma Study Group . Uveal melanomas with SF3B1 mutations: a distinct subclass associated with late-onset metastases. Ophthalmology. 2016;123(5):1118-1128. doi: 10.1016/j.ophtha.2016.01.023 [DOI] [PubMed] [Google Scholar]
- 11.Riemens A, Bromberg J, Touitou V, et al. . Treatment strategies in primary vitreoretinal lymphoma: a 17-center European collaborative study. JAMA Ophthalmol. 2015;133(2):191-197. doi: 10.1001/jamaophthalmol.2014.4755 [DOI] [PubMed] [Google Scholar]
- 12.Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. Journal of the American Statistical Association. 1958;53(282):457-481. doi: 10.1080/01621459.1958.10501452 [DOI] [Google Scholar]
- 13.Therneau T. A Package for Survival Analysis in R. R package version 3.1-12. Accessed November 13, 2020. https://CRAN.R-project.org/package=survival.
- 14.Therneau TM, Grambsch PM. Modeling Survival Data: Extending the Cox Model New York: Springer; 2000. doi: 10.1007/978-1-4757-3294-8 [DOI] [Google Scholar]
- 15.Bergman L, Seregard S, Nilsson B, Lundell G, Ringborg U, Ragnarsson-Olding B. Uveal melanoma survival in Sweden from 1960 to 1998. Invest Ophthalmol Vis Sci. 2003;44(8):3282-3287. doi: 10.1167/iovs.03-0081 [DOI] [PubMed] [Google Scholar]
- 16.Dogrusöz M, Jager MJ. Genetic prognostication in uveal melanoma. Acta Ophthalmol. 2018;96(4):331-347. doi: 10.1111/aos.13580 [DOI] [PubMed] [Google Scholar]
- 17.Dogrusöz M, Bagger M, van Duinen SG, et al. . The Prognostic value of AJCC staging in uveal melanoma is enhanced by adding chromosome 3 and 8q status. Invest Ophthalmol Vis Sci. 2017;58(2):833-842. doi: 10.1167/iovs.16-20212 [DOI] [PubMed] [Google Scholar]
- 18.Damato B, Eleuteri A, Taktak AF, Coupland SE. Estimating prognosis for survival after treatment of choroidal melanoma. Prog Retin Eye Res. 2011;30(5):285-295. doi: 10.1016/j.preteyeres.2011.05.003 [DOI] [PubMed] [Google Scholar]
- 19.Vaquero-Garcia J, Lalonde E, Ewens KG, et al. . PRiMeUM: a model for predicting risk of metastasis in uveal melanoma. Invest Ophthalmol Vis Sci. 2017;58(10):4096-4105. doi: 10.1167/iovs.17-22255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Shields CL, Ganguly A, Bianciotto CG, Turaka K, Tavallali A, Shields JA. Prognosis of uveal melanoma in 500 cases using genetic testing of fine-needle aspiration biopsy specimens. Ophthalmology. 2011;118(2):396-401. doi: 10.1016/j.ophtha.2010.05.023 [DOI] [PubMed] [Google Scholar]
- 21.Onken MD, Worley LA, Char DH, et al. . Collaborative Ocular Oncology Group report number 1: prospective validation of a multi-gene prognostic assay in uveal melanoma. Ophthalmology. 2012;119(8):1596-1603. doi: 10.1016/j.ophtha.2012.02.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Augsburger JJ, Corrêa ZM, Trichopoulos N. An alternative hypothesis for observed mortality rates due to metastasis after treatment of choroidal melanomas of different sizes. Trans Am Ophthalmol Soc. 2007;105:54-59. [PMC free article] [PubMed] [Google Scholar]
- 23.Gamel JW, McLean IW, McCurdy JB. Biologic distinctions between cure and time to death in 2892 patients with intraocular melanoma. Cancer. 1993;71(7):2299-2305. doi: [DOI] [PubMed] [Google Scholar]
- 24.Szalai E, Jiang Y, van Poppelen NM, et al. . Association of uveal melanoma metastatic rate with stochastic mutation rate and type of mutation. JAMA Ophthalmol. 2018;136(10):1115-1120. doi: 10.1001/jamaophthalmol.2018.2986 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zhang Y, Shi J, Liu X, et al. . BAP1 links metabolic regulation of ferroptosis to tumour suppression. Nat Cell Biol. 2018;20(10):1181-1192. doi: 10.1038/s41556-018-0178-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Grossniklaus HE Understanding uveal melanoma metastasis to the liver: the Zimmerman Effect and the Zimmerman hypothesis. Ophthalmology. 2019;126(4):483-487. doi: 10.1016/j.ophtha.2018.09.031 [DOI] [PubMed] [Google Scholar]
- 27.Tralongo P, Surbone A, Serraino D, Dal Maso L. Major patterns of cancer cure: clinical implications. Eur J Cancer Care (Engl). 2019;28(6):e13139. doi: 10.1111/ecc.13139 [DOI] [PubMed] [Google Scholar]
- 28.Jakobsen LH, Andersson TM, Biccler JL, et al. . On estimating the time to statistical cure. BMC Med Res Methodol. 2020;20(1):71. doi: 10.1186/s12874-020-00946-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Jensen OA Malignant melanomas of the human uvea: 25-year follow-up of cases in Denmark, 1943--1952. Acta Ophthalmol (Copenh). 1982;60(2):161-182. doi: 10.1111/j.1755-3768.1982.tb08371.x [DOI] [PubMed] [Google Scholar]
- 30.Bagger M, Smidt-Nielsen I, Andersen MK, et al. . Long-term metastatic risk after biopsy of posterior uveal melanoma. Ophthalmology. 2018;125(12):1969-1976. doi: 10.1016/j.ophtha.2018.03.047 [DOI] [PubMed] [Google Scholar]
- 31.Choudhary MM, Gupta A, Bena J, Emch T, Singh AD. Hepatic ultrasonography for surveillance in patients with uveal melanoma. JAMA Ophthalmol. 2016;134(2):174-180. doi: 10.1001/jamaophthalmol.2015.4810 [DOI] [PubMed] [Google Scholar]
- 32.Singh AD, Triozzi PL. Endoresection for choroidal melanoma: palliative or curative intent? Br J Ophthalmol. 2008;92(8):1015-1016. doi: 10.1136/bjo.2008.145805 [DOI] [PubMed] [Google Scholar]
- 33.García-Arumí J, Zapata MA, Balaguer O, Fonollosa A, Boixadera A, Martinez-Castillo V. Endoresection in high posterior choroidal melanomas: long-term outcome. Br J Ophthalmol. 2008;92(8):1040-1045. doi: 10.1136/bjo.2008.137562 [DOI] [PubMed] [Google Scholar]
- 34.Damato B Does ocular treatment of uveal melanoma influence survival? Br J Cancer. 2010;103(3):285-290. doi: 10.1038/sj.bjc.6605765 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Afshar AR, Damato BE. Uveal melanoma: evidence for efficacy of therapy. Int Ophthalmol Clin. 2015;55(1):23-43. doi: 10.1097/IIO.0000000000000053 [DOI] [PubMed] [Google Scholar]
- 36.Yang J, Manson DK, Marr BP, Carvajal RD. Treatment of uveal melanoma: where are we now? Ther Adv Med Oncol. 2018;10:1758834018757175. doi: 10.1177/1758834018757175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Triozzi PL, Singh AD. Adjuvant therapy of uveal melanoma: current status. Ocul Oncol Pathol. 2014;1(1):54-62. doi: 10.1159/000367715 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Augsburger JJ Is observation really appropriate for small choroidal melanomas. Trans Am Ophthalmol Soc. 1993;91:147-168. [PMC free article] [PubMed] [Google Scholar]
- 39.Bellerive C, Grossniklaus HE, Singh AD. Prognostication for uveal melanoma: are two tests better than one? Ocul Oncol Pathol. 2017;3(4):301-303. doi: 10.1159/000472153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Shao YF, Echegaray JJ, Singh N, Singh AD. Variability of bad prognosis in uveal melanoma. Ophthalmol Retina. 2019;3(2):186-193. doi: 10.1016/j.oret.2018.09.007 [DOI] [PubMed] [Google Scholar]
- 41.Robertson AG, Shih J, Yau C, et al. . Integrative analysis identifies four molecular and clinical subsets in uveal melanoma. Cancer Cell. 2017;32(2):204-220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Reiman A, Kikuchi H, Scocchia D, et al. . Validation of an NGS mutation detection panel for melanoma. BMC Cancer. 2017;17(1):150. doi: 10.1186/s12885-017-3149-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Abdel-Rahman MH, Sample KM, Pilarski R, et al. . Whole exome sequencing identifies candidate genes associated with hereditary predisposition to uveal melanoma. Ophthalmology. 2020;127(5):668-678. doi: 10.1016/j.ophtha.2019.11.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Bowcock AM, Anbunathan H, Verstraten R, Singh AD, Harbour JW. Integrative copy number analysis of uveal melanoma reveals novel candidate genes involved in tumorigenesis including a tumor suppressor role for PHF10/BAF45a. Clin Cancer Res. 2019;25(16):5156-5166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Eskelin S, Pyrhönen S, Summanen P, Hahka-Kemppinen M, Kivelä T. Tumor doubling times in metastatic malignant melanoma of the uvea: tumor progression before and after treatment. Ophthalmology. 2000;107(8):1443-1449. doi: 10.1016/S0161-6420(00)00182-2 [DOI] [PubMed] [Google Scholar]
- 46.Singh AD Uveal melanoma: implications of tumor doubling time. Ophthalmology. 2001;108(5):829-831. doi: 10.1016/S0161-6420(00)00607-2 [DOI] [PubMed] [Google Scholar]
- 47.Collaborative Ocular Melanoma Study Group The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma: V: twelve-year mortality rates and prognostic factors: COMS report No. 28. Arch Ophthalmol. 2006;124(12):1684-1693. doi: 10.1001/archopht.124.12.1684 [DOI] [PubMed] [Google Scholar]
- 48.Parrella P, Sidransky D, Merbs SL. Allelotype of posterior uveal melanoma: implications for a bifurcated tumor progression pathway. Cancer Res. 1999;59(13):3032-3037. [PubMed] [Google Scholar]
- 49.Tschentscher F, Hüsing J, Hölter T, et al. . Tumor classification based on gene expression profiling shows that uveal melanomas with and without monosomy 3 represent two distinct entities. Cancer Res. 2003;63(10):2578-2584. [PubMed] [Google Scholar]
- 50.Singh N, Singh AD, Hide W. Inferring an evolutionary tree of uveal melanoma from genomic copy number aberrations. Invest Ophthalmol Vis Sci. 2015;56(11):6801-6809. doi: 10.1167/iovs.15-16822 [DOI] [PubMed] [Google Scholar]
- 51.Field MG, Durante MA, Anbunathan H, et al. . Punctuated evolution of canonical genomic aberrations in uveal melanoma. Nat Commun. 2018;9(1):116. doi: 10.1038/s41467-017-02428-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.SEER_brochure.pdf. Accessed November 16, 2020. https://seer.cancer.gov/about/factsheets/
- 53.Henley SJ, Ward EM, Scott S, et al. . Annual report to the nation on the status of cancer, part I: National cancer statistics. Cancer. 2020;126(10):2225-2249. doi: 10.1002/cncr.32802 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2017, National Cancer Institute. Bethesda, MD. Published April 15, 2020. Accessed November 16, 2020. https://seer.cancer.gov/csr/1975_2017/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure. Mortality in the US has not changed much in 40 years
eTable 1. Full results underlying Figure 1A
eTable 2. Full results underlying Figure 1B
eTable 3. Full results underlying Figure 3A
eTable 4. Full results underlying Figure