

Abstract
Background:
Despite increasing the number of women and ethnic minority groups in surgery, the academic advancement of such individuals within surgical fields lags behind Caucasian men. We sought to identify gender and ethnic inequalities in the receipt of surgical society research grants for young faculty investigators and compare the scholarly productivity of these groups.
Materials and methods:
In this cross-sectional and retrospective study, the gender and race of surgical society grant recipients were determined from surgical society Web sites. Surgical society grants aimed at providing research grants for junior faculty investigators were analyzed. Using the Scopus database, each recipient’s scholarly productivity was determined by means of h-index, a standardized measure of the quantity and impact of an individual’s published articles. We generated descriptive statistics to compare the gender, race, and h-index of grant recipients in the years 2006-2008 and 2016-2018.
Results:
Between 2006 and 2008, there were 68 research grant recipients. Of these recipients, 79% were men and 21% were women. The racial breakdown was 54% Caucasian men, 22% Asian men, 1.4% African American men, 1.4% Hispanic men, 12% Caucasian women, 7% Asian Women, and 1.4% African American women. The average h-index of the male and female recipients is 25 (±14) and 24 (±14), respectively (P = 0.81). Between 2016 and 2018, there were 113 research grant recipients. Of these recipients, 66% were men and 34% were women. The racial breakdown was 47% Caucasian men, 16% Asian men, 3.5% African American men, 1% Hispanic men, 26% Caucasian women, 3.5% Asian women, and 3.5% African American women. The average h-index of the male and female recipients is 12 (±8) and 9 (±6), respectively (P = 0.046). Caucasian women had the only statistically significant change in the proportion of grant recipients from 2006-2008 to 2016-2018, with an increase from 12% to 26% (P = 0.02).
Conclusions:
Most surgical society research grants for young investigators continue to be awarded to Caucasian men, with Caucasian women earning a distant second in the 2016-2018 cohort. Ethnic minorities continue to be awarded less research grants than Caucasian recipients. Overall, the average h-index of women was less than men. This study highlights the persistent need for surgical societies to consider gender and ethnic disparities when awarding junior investigator grants, including barriers minority groups may face in achieving the same h-index as Caucasian men.
Keywords: Diversity, Inclusion, Gender equity, Surgical society, Academic surgery
Introduction
Over the past 50 y, there has been a dramatic change in the demographics of medical students, physicians, and the surgical workforce. The percentage of female medical students is now equal to that of male medical students in the United States.1 Despite this advancement, it is projected that gender equity will not be achieved in surgical residency until 2028 and full professorship in 2096.2 The lack of racial diversity within academic surgery is also well described within the literature.3–5
There have been many efforts to combat the lack of diversity in the surgical workforce, ranging from calls to find barriers that minorities face in careers in academic surgery to pilot programs addressing the issue.6–8 Although there has been an increase in the number of women and minorities in general surgery, these underrepresented groups remain less likely to choose careers in academic surgery.2,8,9 For those who pursue a career in academic surgery, the path to promotion and leadership is longer than their nonminority counterparts.2,10
The aim of junior surgical society research grants is to jumpstart careers in academic surgery. Surgical societies have a unique opportunity with junior surgical society research grants to improve diversity within the field. Yet, little is known about how these grants are allocated in terms of recipient demographic. It is also unclear how the demographics of recipients have changed with the changing demographics of the surgical workforce. We sought to investigate the demographics of junior surgical society grants recipients and how they have changed over a 10-y period. We also aimed to evaluate the scholarly productivity of these recipients and how the 2006-2008 recipients developed over 10 y.
Materials and methods
We performed a cross-sectional and retrospective study of junior surgical society research grant recipients from 2006-2008 and 2016-2018. General surgery and general surgery subspecialty surgical society Web sites were examined. We included all grants with funding for research designated for junior surgeon investigators. Most grants required applicants to be within 5-8 y post-training, where training was defined as residency or fellowship. We included some grants who stated a preference for young investigators, but no cutoff period (Table 1). The race and gender of each recipient were determined from the academic profile on the respective institutions’ Web site. For recipients without profiles on institutional Web sites, the race and gender of the recipient were determined from another site such as LinkedIn or ResearchGate. Recipients were classified as men or women based on their first name and appearance. Recipients were grouped as Caucasian, Asian, African American, or Hispanic based on their appearance. Two authors determined the gender and race of each recipient and had 100% agreement on gender and 97% agreement on race.
Table 1 –
Junior surgical society research grants.
| Surgical society | Grant name |
|---|---|
| American Association of Endocrine Surgeons (AAES) | Paul Logerfo Research Award |
| American Association of Plastic Surgeons (AAPS) | Faculty Research Scholarship |
| Association for Academic Surgery (AAS) | Joel J. Roslyn Faculty Research Award |
| American Foundation for Surgery of the Hand (AFSH) | American Foundation of Surgery of the Hand Basic Science Grant |
| American Surgical Association (ASA) | Fellowship Research Award |
| American Society of Transplant Surgeons (ASTS) | Faculty Developing Grant |
| Central Surgical Association (CSA) | Enrichment Award |
| Central Surgical Association (CSA) | Turcotte Award |
| Eastern Association for the Surgery of Trauma (EAST) | Trauma Research Scholarship |
| Eastern Association for the Surgery of Trauma (EAST) | Templeton Injury Prevention Research Scholarship |
| Eastern Association for the Surgery of Trauma (EAST) | Multicenter Junior Investigator Award |
| International Society for Heart and Lung Transplantation (ISHLT) | Norman E. Shumway Career Development/Joel D. Cooper Career Development Award |
| Surgical Infection Society | Junior Faculty Basic or Translational Research Fellowship |
| Surgical Infection Society | Junior Faculty Clinical Research Fellowship |
| Society for Surgery of the Alimentary Tract (SSAT) | Career Development Award for Clinical/Outcomes/Education Research |
| Society for Surgery of the Alimentary Tract (SSAT) | Healthcare Disparities Research Award |
| Society for Surgery of the Alimentary Tract (SSAT) | Career Development Award |
| Society of Surgical Oncology (SSO) | Clinical Investigator Award |
| Society of Surgical Oncology (SSO) | Young Investigator Award |
| Society of University Surgeons (SUS) | Junior Faculty Award |
| Thoracic Surgery Foundation (TSF) and Southern Thoracic Surgical Association (STSA) | TSF/STSA Research Award |
| Thoracic Surgery Foundation (TSF) and Society of Thoracic Surgeons (STS) | STS Research Award |
| Thoracic Surgery Foundation (TSF) | TSF Research Award |
| Thoracic Surgery Foundation (TSF) | Nina Starr Braunwald Research Fellowship Award |
The scholarly productivity of each recipient in the 2006-2008 cohort was measured using h-index and articles published on PubMed since the date of the research grant award. The h-index is a number calculated using the authors’ number of publications and the impact of these publications. The impact of publications is measured using the impact factor of the journals and the number of times the article has been referenced. The h-index of each recipient was found through the SCOPUS database. The number of publications and author order on publications for each recipient was determined using the PubMed database. The current academic position held by each recipient was determined from institutional profiles. For the 2016-2018 cohort, the scholarly productivity of the grant recipients was measured using the h-index. For each grant recipient, the h-index was the recipients’ current h-index. Statistical significance was defined as P < 0.05. P values were calculated using an unpaired t-test for continuous variables. A Fisher exact test or χ2 test for categorical variables with a sample size less than 5 or greater than or equal to 5, respectively. This research was exempt from human subjects.
Results
2006-2008 cohort
The recipients of 36 young investigator designated surgical society research grants were analyzed. In the 2006-2008 cohort, there were 68 grant recipients. The 2006-2008 cohort was 79% men (n = 54; Table 2). The racial breakdown was 66.2% Caucasian (n = 45), 29.4% Asian (n = 20), 3% African American (n = 2), and 1.5% Hispanic (n = 1). In 2006-2008, the Caucasian men received most research grants at 54% (n = 37), with Asian men a distant second at 22% (n = 15). Non-Caucasian recipients received 33% (n = 23) of the research grants. The current average h-index of each recipient is 25 (±14).
Table 2 –
Recipient demographics.
| n (%) | 2006-2008 (n = 68) | 2016-2018 (n = 113) | P value |
|---|---|---|---|
| Male | 54 (79%) | 76 (67%) | 0.08 |
| Caucasian men | 37 (54%) | 53 (47%) | 0.33 |
| Asian men | 15 (22%) | 18 (16%) | 0.3 |
| African American men | 1 (1.4%) | 4 (3.5%) | 0.65 |
| Hispanic men | 1 (1.4%) | 1 (1%) | 1 |
| Caucasian women | 8 (12%) | 29 (26%) | 0.02 |
| Asian women | 5 (7%) | 4 (3.5%) | 0.3 |
| African American women | 1 (1.4%) | 4 (3.5%) | 0.65 |
| Hispanic women | 0 | 0 |
Bold indicates P values that are significant.
2016-2018 cohort
In the 2016-2018 cohort, there were 113 grant recipients, 67% (n = 76) of the recipients were men (Table 2). The racial breakdown of recipients was 72.5% Caucasian (n = 82), 19.5% Asian (n = 22), 7.1% African American (n = 8), and 0.88% Hispanic (n = 1). Caucasian men received the largest proportion of research grants at 47% (n = 53), with Caucasian women a distant second at 26% (n = 29). Non-Caucasian recipients received 27% (n = 31) of the research grants. The current average h-index of the recipients is 12 (±8). Caucasian women had the only statistically significant change in proportion of grant recipients from 2006-2008 to 2016-2018, with an increase from 12% (n = 8) to 26% (n = 29) (P = 0.02).
Academic productivity over time by gender
In the 2016-2018 cohort, the average h-index of male recipients (13 ± 8) was significantly greater than the average h-index of female recipients (10 ± 6) (P = 0.04; Fig. 1). In the 2006-2008 cohort, the average male h-index was 25 (±14) and the average female h-index was 24 (±14) (P = 0.81). The average number of publications since the award was 79 (±75) and 50 (±37), for men and women, respectively (P = 0.17) (Fig. 2). The average number of first and last author publications since the award was 37 (±38) and 24 (±20), for men and women, respectively (P = 0.22).
Fig. 1 –
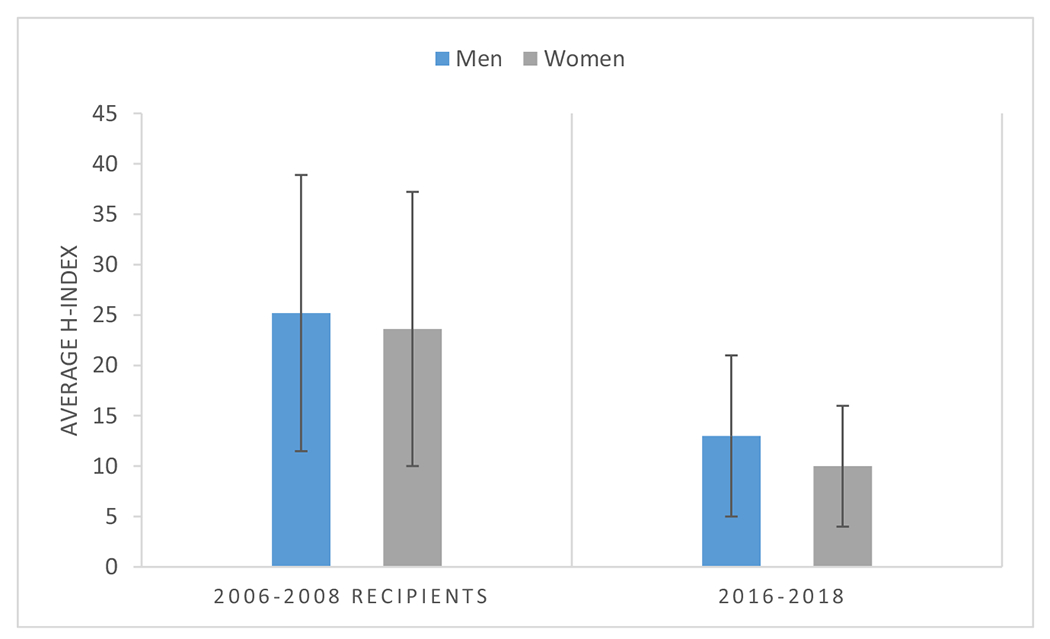
Current average h-index of recipients by gender.
Fig. 2 –
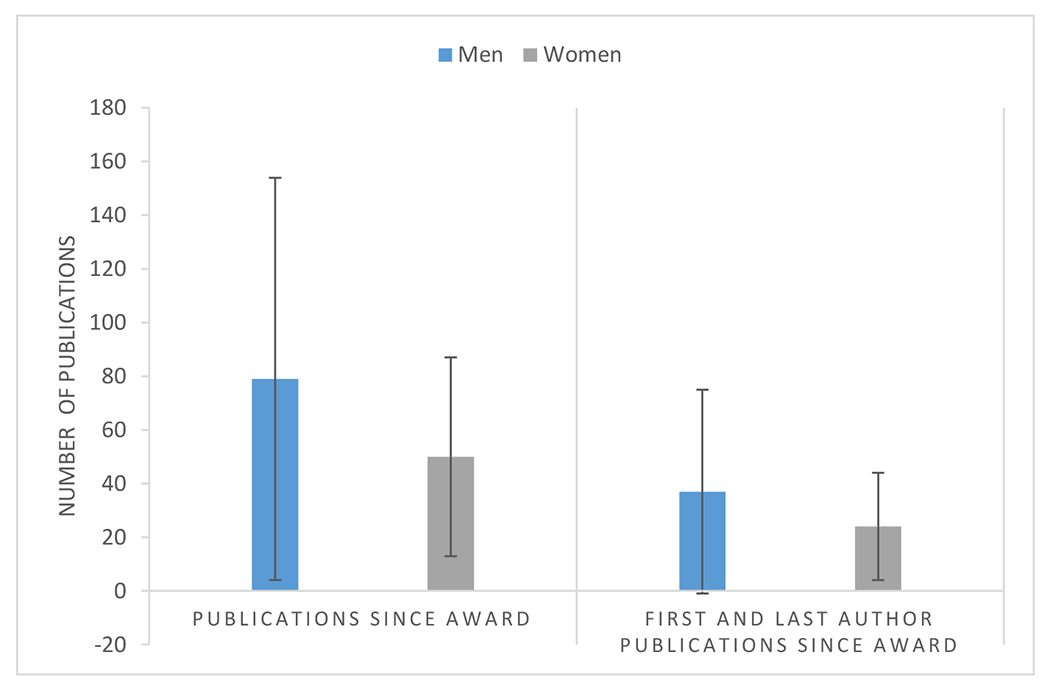
2006-2008 grant recipients: publications since award.
Current academic positions of recipients
In the 2006-2008 cohort, 54 recipients were men and 14 recipients were women (Table 3). The percentage of recipients who are currently professors in this cohort is 63% (n = 34) and 50% (n = 7), of male and female recipients, respectively (P = 0.38). The percentage of associate professors is 22% (n = 12) and 36% (n = 5), of male and female recipients, respectively (P = 0.08). The percentage of assistant professors is 7% (n = 4) and 7% (n = 1), of male and female recipients, respectively (P = 1). Three recipients are current chairs of departments of surgery and two of the three are men (P = 0.51). Eighteen, or 33%, of the male recipients are division chairs, chiefs, or directors. Six, or 43%, of the female recipients are division chairs, chiefs, or directors (P = 0.5).
Table 3 –
Academic appointment by gender in the 2006-2008 cohort.
| n (%) | Male (n = 54) | Female (n = 14) | P value |
|---|---|---|---|
| Professor | 34 (63%) | 7 (50%) | 0.38 |
| Associate Professor | 12 (22%) | 5 (36%) | 0.08 |
| Assistant Professor | 4 (7%) | 1 (7%) | 1 |
| Other | 4 (7%) | 1 (7%) | 1 |
| Chair of Department | 2 (4%) | 1 (7%) | .51 |
| Division Chair/Chief/Director | 18 (33%) | 6 (43%) | 0.5 |
Discussion
The lack of diversity in academic surgery has been well described and the field continues to struggle to match the demographics of the general population and physician population.3–5 Obtaining research funding with grants is often considered essential to the establishment of an early research presence for those who desire a career in academic surgery. Once a surgeon has received funding, they are more likely to successfully achieve further funding.11 Therefore, junior surgical society research grants provide a unique opportunity for the field of academic surgery to increase diversity and inclusion by intentionally funding traditionally underrepresented groups. Despite this opportunity to increase the diversity of academic surgery, the results of this study indicate that most grant recipients in both the 2006-2008 and 2016-2018 cohorts were men at 79% and 67%, respectively (Table 2). According to the AAMC report on diversity, however, 79% of surgeons in 2004 were men and 64% of surgeons in 2018 were women, indicating that these awards are proportionate.12,13 According to the AAMC report on faculty diversity in 2017 and 2018, the demographics of assistant professors was 46% Caucasian men, 14% Asian men, 2% African American men, 3% Hispanic men, 18% Caucasian women, 6% Asian women, 2% African American women, and 1% Hispanic women.14,15
The proportionate awarding of research awards to the current population, however, only serves to further propagate the advantage of groups already in the majority, and does not account for the certain change in these proportions in the younger surgeon population. For example, although 79% of all surgeons were men in 2006, it is likely that a lower percentage of "young surgeons” were men, therefore, there is a relative overrepresentation of men recipients of these awards. It is nearly impossible to externally determine how many surgeons applied for these junior investigator awards from each gender or race in this period. Previous research has shown that blinding the publication process has increased the diversity of authors.16 Blinding the process of how junior surgical society award recipients are chosen may help increase the diversity of recipients.
The proportion of female recipients increased over the 10-y period, paralleling an increase in women in academic surgery, but the percentage of minorities did not. In the 2006-2008 cohort, most recipients were Caucasian men, with Asian men a distant second (Table 2). The percentage of Caucasian female recipients increased from 12% in 2006-2008 to 26% in 2016-2018, which was the only statistically significant change. The increased proportion of Caucasian female recipients lead to lower proportion of Caucasian male recipients, in addition to a lower proportion of minority recipients. The data from the AAMC report on diversity in 2004 demonstrated that 26% of surgeons at that time were a racial minority. In 2019, 40% of the surgical force were racial minorities. The results indicate that there has been appropriate progress toward gender equity within grant recipients. However, despite progress with diversity in the surgical workforce, there has been a decrease in minority representation among surgical society grant recipients over the 10-y period.
Comparing the scholarly productivity of minority recipients was not possible secondary to low numbers of minority recipients. Drawing any conclusion from the data is inappropriate. When comparing the scholarly productivity of recipients by gender, we found that in the 2016-2018 cohort, the current h-index of women was significantly less than the h-index of the men in the cohort. These results are consistent with the publication gender gap in academic surgery that is well described in the literature.17–19 The h-indexes, number of publications since award, and number of first and last author publications since award of men and women in the 2006-2008 cohort were not significantly different. However, the women in this cohort had a lower average h-index, number of publications, and number of first and last author publications. In addition, the men were more likely to currently be full professors than the women in this cohort.
These results align with the literature that demonstrates that the career trajectory of women in academic surgery is far slower than men in scholarly productivity, promotion, and leadership positions.2,20 There is a well described publication bias in surgery that favors white, cisgender males in publication, which may account for the disparity in h-index.21,22 Furthermore, we must address the barriers women face in publication. As this study demonstrates that those women who are considered promising enough as “junior investigators” to warrant investment from surgical society awards, are unable to match their male peers in publication impact.23
The benefit of having minorities and women in surgery are expansive, and should be sought after. Diversity in surgical faculty increases the recruitment of underrepresented minorities into academic surgery.3 Minority surgeons are far more likely than nonminorities to work with underserved populations.7,24 In addition, minority patients are more likely to seek care and feel more comfortable with a minority surgeon.8 Wallis et al.25 demonstrated that female surgeons have lower 30-d mortality rates than male surgeons. Despite the clear benefits of increasing diversity in academic surgery, there are many barriers that exist for women and minorities. Mentorship is one of the key factors necessary for promotion and success in academic surgery and a barrier for non-Caucasian males.8,26,27 The male and female perspectives, regarding surgery and success, differ greatly. Women are more likely to feel as though they are not included in the culture of a department.28–30
There have been multiple proposed solutions for increasing diversity in academic surgery. One successful example is a diversity surgeon’s initiative, which entailed a minimally invasive surgery techniques program. The program was created to connect minority surgeons with minority residents in the field, promote minority surgical resident success, and help promote careers in academic surgery.8 Butler et al. also suggested introducing the “Rooney Rule” in leadership positions. The rule was born out of the national football league, who noted that although their player population was extremely diverse, they had a very low percentage of diverse head coaches. The national football league made a rule that for every head coach position that opened up, a minority candidate must be interviewed and considered. The “Rooney Rule” could be considered to improve diversity within junior surgical society grants and in turn diversity in academic surgery. In addition, blinding the reviewer from the name of the applicant could reduce inherent selection bias. The advent of minority and gender-specific young investigator research grants could help increase diversity. One example of this type of grant is the Nina Starr Braunwald Research Award, which has been awarded to women in thoracic surgery since 1993. Minority and gender-focused surgical societies should consider creating similar young investigator research awards to continue to promote diversity in medicine.
Our study did not investigate the process that the surgical societies used to select surgical society grant recipients. In addition, we did not have information on applicant demographics or qualifications for the grants. Further limitations of our study include the method of identifying the racial background of the recipient. A survey of the recipients helping identify gender and racial background could have provided more accurate results. However, to the best of our knowledge, this is the first study of surgical society research grant recipients and the results provide important context into who is receiving these awards and what their scholarly productivity is.
Conclusion
Junior surgical society grants provide surgical societies with a unique opportunity to increase diversity in academic surgery. This study highlights the persistent need for surgical societies to consider gender and ethnic disparities when awarding junior investigator grants, including barriers minority groups may face in achieving the same h-index as Caucasian men. Future studies to identify perceived causes of decreased scholarly productivity, slower promotion, and less leadership roles are necessary.
Acknowledgment
This publication was made possible by the Clinical and Translational Science Collaborative of Cleveland, KL2TR002547 from the National Center for Advancing Translational Sciences (NCATS) component of the National Institutes of Health and NIH roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Footnotes
Financial disclosures: None.
Conflicts of interest: None.
Disclosure
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
REFERENCES
- 1.Bates C, Gordon L, Travis E, Chatterjee A, et al. Striving for gender equity in academic medicine careers: a call to action. Acad Med. 2016;91:1050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhuge Y, Kaufman J, Simeone DM, Chen H, Velazquez OC. Is there still a glass ceiling for women in academic surgery? Ann Surg. 2011;253:637–643. [DOI] [PubMed] [Google Scholar]
- 3.Abelson JS, Symer MM, Yeo HL, et al. Surgical time out: our counts are still short on racial diversity in academic surgery. Am J Surg. 2018;215:542–548. [DOI] [PubMed] [Google Scholar]
- 4.Butler PD, Longaker MT, Britt LD. Major deficit in the number of underrepresented minority academic surgeons persists. Ann Surg. 2008;248:704–709. [DOI] [PubMed] [Google Scholar]
- 5.Reede JY. A recurring theme: the need for minority physicians. Health Aff 2003;22:91–93. [DOI] [PubMed] [Google Scholar]
- 6.West MA, Hwang S, Maier RV, et al. Ensuring equity, diversity, and inclusion in academic surgery: an American Surgical Association White Paper. Ann Surg. 2018;268:403–407. [DOI] [PubMed] [Google Scholar]
- 7.Butler PD, Longaker MT, Britt L. Addressing the paucity of underrepresented minorities in academic surgery: can the “Rooney Rule” be applied to academic surgery? Am J Surg. 2010;199:255–262. [DOI] [PubMed] [Google Scholar]
- 8.Butler PD, Britt L, Green ML, et al. The diverse surgeons initiative: an effective method for increasing the number of under-represented minorities in academic surgery. J Am Coll Surg. 2010;211:561–566. [DOI] [PubMed] [Google Scholar]
- 9.Flannery AM. Success, women, and academic surgery. Surgery. 2002;131:670–671. [DOI] [PubMed] [Google Scholar]
- 10.Abelson JS, Wong NZ, Symer M, et al. Racial and ethnic disparities in promotion and retention of academic surgeons. Am J Surg. 2018;216:678–682. [DOI] [PubMed] [Google Scholar]
- 11.Chan JK, Shalhoub J, Gardiner MD, Suleman-Verjee L. Nanchahal J Strategies to secure surgical research funding: fellowships and grants. JRSM Open. 2014;5, 2042533313505512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Diversity in Medicine: Facts and Figures 2019. Association of American Medical Colleges; 2019. Available at: https://www.aamc.org/system/files/2019-12/19-222-Executive%20Summary-FINAL-120919.pdf. Accessed August 11, 2020.
- 13.Diversity in the Physician Workforce: Facts and Figures 2006. Association of American Medical Colleges; 2006. Available at: https://www.aamc.org/system/files/reports/1/diversityinthephysicianworkforce-factsandfigures2006.pdf. Accessed August 11, 2020.
- 14.2017 US Medical School Faculty. Association of American Medical Colleges; 2017. Available at: https://www.aamc.org/data-reports/faculty-institutions/interactive-data/2017-us-medical-school-faculty. Accessed August 11, 2020.
- 15.2018 US Medical School Faculty. Association of American medical Colleges; 2018. Available at: https://www.aamc.org/data-reports/faculty-institutions/interactive-data/2018-us-medical-school-faculty. Accessed August 11, 2020.
- 16.Budden AE, Tregenza T, Aarssen LW, Koricheva J, Leimu R, Lortie CJ. Double-blind review favours increased representation of female authors. Trends Ecol Evol. 2008;23:4–6. [DOI] [PubMed] [Google Scholar]
- 17.Housri N, Cheung MC, Koniaris LG, Zimmers TA. Scientific impact of women in academic surgery. J Surg Res. 2008;148:13–16. [DOI] [PubMed] [Google Scholar]
- 18.Mueller C, Wright R, Girod S. The publication gender gap in US academic surgery. BMC Surg. 2017;17:16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kurichi JE, Kelz RR, Sonnad SS. Women authors of surgical research. Arch Surg. 2005;140:1074–1077. [DOI] [PubMed] [Google Scholar]
- 20.Sexton KW, Hocking KM, Wise E, et al. Women in academic surgery: the pipeline is busted. J Surg Educ. 2012;69:84–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Engqvist L, Frommen JG. Double-blind peer review and gender publication bias. Anim Behav. 2008:76. [Google Scholar]
- 22.Tregenza T Gender bias in the refereeing process? Trends Ecol Evol. 2002;17:349–350. [Google Scholar]
- 23.Boitano LT, Hart KL, Tanious A, et al. Gender Bias in Surgical Publication: Improvement but Still Progress to be Made. Academic Surgical Congress; 2019. [Google Scholar]
- 24.Steinbrook R Diversity in Medicine. Mass Medical Soc; 1996. [DOI] [PubMed] [Google Scholar]
- 25.Wallis CJ, Ravi B, Coburn N, Nam RK, Detsky AS, Satkunasivam R. Comparison of postoperative outcomes among patients treated by male and female surgeons: a population based matched cohort study. BMJ. 2017;359:j4366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Seemann NM, Webster F, Holden HA, et al. Women in academic surgery: why is the playing field still not level? Am J Surg. 2016;211:343–349. [DOI] [PubMed] [Google Scholar]
- 27.Colletti LM, Mulholland MW, Sonnad SS. Perceived obstacles to career success for women in academic surgery. Arch Surg. 2000;135:972–977. [DOI] [PubMed] [Google Scholar]
- 28.Zutshi M, Hammel J, Hull T. Colorectal surgeons: gender differences in perceptions of a career. J Gastrointest Surg. 2010;14:830–843. [DOI] [PubMed] [Google Scholar]
- 29.Sonnad SS, Colletti LM. Issues in the recruitment and success of women in academic surgery. Surgery. 2002;132:415–419. [DOI] [PubMed] [Google Scholar]
- 30.Cochran A, Hauschild T, Elder WB, Neumayer LA, Brasel KJ, Crandall ML. Perceived gender-based barriers to careers in academic surgery. Am J Surg. 2013;206:263–268. [DOI] [PubMed] [Google Scholar]