

Abstract
Despite the fact that street-connected children and youth (SCY) in low- and middle-income countries experience numerous social and health inequities, few evidence-based policies and interventions have been implemented to improve their circumstances. Our study analyzed strategies to advance health equity through action on the social determinants of health (SDH) for SCY in Kenya based on General Comment 21 of the United Nations Committee on the Rights of the Child. To identify policies and interventions, we analyzed archival newspaper articles and policy documents and elicited ideas from a diversity of social actors across Kenya. Our results identified three types of policies and interventions: repressive, welfare oriented, and child rights based. We then situated these strategies within the World Health Organization’s conceptual framework on SDH inequities to understand their mechanism of impact on health equity. Our results demonstrate that a child rights approach provides a strong avenue for advancing health equity through action on the SDH for SCY in Kenya. As a result of these findings, we developed a checklist for policy makers and other stakeholders to assess how their policies and interventions are upholding human rights, addressing needs, and working to advance health equity for SCY.
Introduction
Street-connected children and youth (SCY) in Kenya, for whom the streets play a central role in their everyday lives and social identities, experience premature and preventable mortality as well as numerous avoidable morbidities, including growth and developmental disparities, mental health issues, the consequences of violence, a high prevalence of HIV and sexually transmitted infections, and poor reproductive health outcomes.1 We postulate that these adverse health outcomes are the result of significant health, social, and economic inequities, including stigma and discrimination.2
Despite SCY experiencing these inequities, few policies or health interventions have been implemented to reduce them in Kenya or in other low- and middle-income countries.3 Multiple reviews suggest that there is insufficient evidence regarding appropriate and effective policies and interventions to reduce the harms associated with street involvement and rehabilitation for SCY and conclude that more research is needed.4
Kenya’s Constitution (article 53) recognizes the need for all children to be protected from abuse, neglect, harmful cultural practices, all forms of violence, inhumane treatment and punishment, and hazardous or exploitative labor. The Constitution also affirms that children have basic rights, including the right to education, nutrition, shelter, health care, and parental care.5 In Kenya, SCY under 18 years of age are protected by the Children’s Act, which outlines children’s rights and welfare in accordance with the Convention on the Rights of the Child (CRC), to which Kenya is a signatory.6 Moreover, in 2003, the Kenyan government established the Street Families Rehabilitation Trust Fund, which seeks to address the needs of SCY and street families and safeguard their rights. However, the program’s reach and impact have not been evaluated, and there is no national policy on SCY.7 Additionally, evidence demonstrates that SCY in Kenya experience significant human rights violations and are not adequately protected in accordance with the Children’s Act and the CRC.8 We postulate that the substantial health inequities experienced by SCY are the result of structural and social determinants of health (SDH) and human rights violations that are a product of policies and practices rooted in the country’s socioeconomic and political context.
Health inequities are systematic differences that are socially produced and unfair, arising as a result of the SDH.9 In the World Health Organization’s conceptual framework on the SDH, a country’s social, economic, and political conditions influence an individual’s social position in society and their exposure and vulnerability to health-compromising conditions. According to this conceptual framework, policies and interventions to advance health equity require context-specific action on structural and intermediary determinants to reduce social stratification, differential exposures and vulnerabilities, and unequal consequences of ill health (Figure 1).10 Strategies to advance health equity may use universal or targeted public policies and interventions at various entry points (including the national context, public policy, and community and individual levels). Universal policies are those that affect the whole population in the national environment (macro level), while targeted policies are those that focus on a disadvantaged group or target health gaps at the community or individual levels. Action on SDH to reduce health inequities is a political process and requires governments to take responsibility to address structural and social inequities to ensure that citizens can exercise their right to the highest attainable standard of health.11
Figure 1.
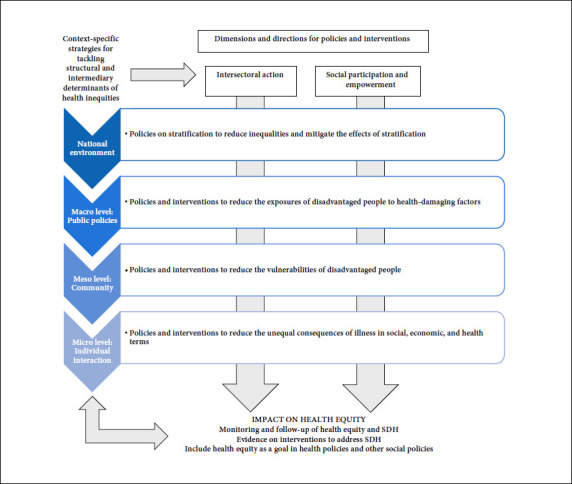
Framework for tackling structural and intermediary determinants of health inequities
The World Health Organization states that “the international human rights framework is the appropriate conceptual structure within which to advance towards health equity through action on SDH.” Therefore, to reduce SDH inequities experienced by disadvantaged populations, such as SCY, international human rights instruments, such as the CRC, provide a legal framework for states to construct policies that work toward achieving equity, while providing a mechanism for civil society to hold states accountable.12 General Comment 21 on children and street situations was released in 2017 by the Committee on the Rights of the Child to provide authoritative guidance, in line with the CRC, to states seeking to respond to injustices experienced by SCY and to improve this population’s circumstances using a child rights approach.13 A child rights approach is one whereby the child is consulted in decisions affecting their health and well-being and is respected as a rights holder. This contrasts with welfare strategies, whereby the child is seen as a victim to be rescued, and repressive approaches that consider SCY to be delinquents and that often criminalize them. It is essential to use a child rights approach when seeking to improve health equity. SCY-related policies and interventions that apply General Comment 21 will intersect with the conceptual framework for tackling SDH inequities at various entry points to influence health equity (Figure 2). For example, when SCY’s right to accessible, free, safe, relevant, and quality education (CRC article 28) is upheld, this will help alter social stratification by reducing inequalities that lead to different socioeconomic positions, which affect health equity. Education can prevent children and youth from ending up in street situations and—for children and youth already on the street—can offer a pathway to transition from the streets and alter their future socioeconomic position.14
Figure 2.
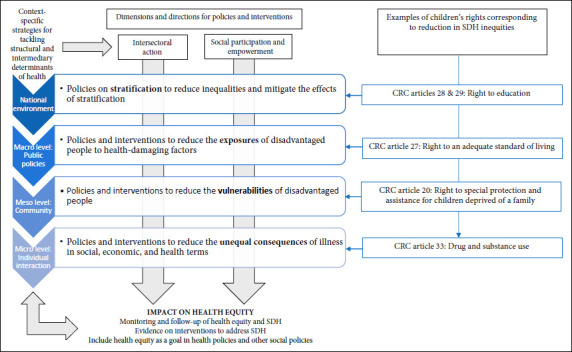
Examples of how child rights policies for SCY can increase health equity at various entry points in the conceptual framework for tackling structural and intermediary determinants of health inequities
Given the lack of effective evidence-based policies and interventions for this population, substantial health inequities, and under-realization of SCY’s rights, we sought to identify existing and proposed policies and interventions for SCY in Kenya through interviews with policy makers, health care providers, community and government stakeholders (for example, SCY opinion leaders, county children’s officers, and the police), and SCY. In our analysis, we categorize these existing and proposed policies and interventions into child rights, welfare, or repressive approaches, and analyze how they intersect with the World Health Organization’s conceptual framework for tackling SDH inequities to increase or decrease health equity. Given the resource constraints typically experienced by low- and middle-income countries, we further present how the use of Abraham Maslow’s hierarchy of needs can help governments and other stakeholders prioritize interventions and policies for implementation.15 This study is vital for informing effective policymaking that respects SCY’s rights and for providing evidence for the design and implementation of responsive and contextually relevant policies and interventions that reduce health inequities.
Methods
Study design
This multi-method qualitative study was conducted from May 2017 to September 2018. We conducted focus group discussions and in-depth interviews with a broad range of social actors, analyzed archival newspaper articles, and analyzed a government policy document to explore and describe proposed and existing policies and interventions that seek to respond to the needs of SCY in Kenya.
Study setting
We purposively selected five counties in western Kenya as study sites (Trans-Nzoia, Bungoma, Kisumu, Uasin Gishu, and Nakuru) where large numbers of SCY are known to reside. Our primary study site was the town of Eldoret, the administrative capital of Uasin Gishu, home to Moi University, Moi Teaching and Referral Hospital, and the Academic Model Providing Access to Healthcare (AMPATH), a long-standing partnership between Moi University, Moi Teaching and Referral Hospital, and a consortium of universities from North America.16
Study participants
Participants included a diverse range of social actors, such as community leaders (chiefs and elders), the county children’s coordinator, children’s officers, police officers, vendors, general community members, stakeholders such as SCY opinion leaders and directors of relevant nongovernmental organizations, parents of street children, former and current SCY, peer navigators, and health care providers at Moi Teaching and Referral Hospital and AMPATH in Uasin Gishu County given our established relations with the local community. In all other counties, we engaged children’s officers, police officers, and SCY.
Ethical considerations
This study received ethical approval from Moi Teaching and Referral Hospital’s Institutional Research Ethics Committee and the University of Toronto’s Research Ethics Board. The study received a waiver of parental consent for minors. Written informed consent was obtained from all participants. Participants were made aware that their interviews would be audio recorded; nine participants declined to be audio recorded but agreed to be interviewed and gave the interviewer permission to take notes. Community participants and SCY were compensated for their time with 200 Ksh (US$2), and government officials were compensated with 1,000 Ksh (US$10).
Recruitment and enrollment
We conducted street outreach and study sensitization in street venues in each county to establish a relationship with SCY and explain the purpose of the study. SCY aged 15–24 were purposively sampled and invited to participate voluntarily in the study from these locations. We contacted community members (leaders, vendors, police officers, and parents of SCY) by phone or in person to explain the purpose of the study and invite them to voluntarily participate. For government officials, we initially contacted them with a formal letter and then followed up in person. At Moi Teaching and Referral Hospital and AMPATH, we purposively selected health care providers through our established networks and contacts.
Data generation
The study’s data sources consisted of the following: 10 randomly selected newspaper articles focused on SCY in Kenya that were published between 2015 and 2018; one purposively selected international newspaper article; a government policy document; and 41 in-depth interviews and seven focus group discussions with a total of 100 participants (48 women and 52 men). The median age was 16 years for SCY participants and 42 years for community members. A team of eight trained interviewers conducted focus group discussions and in-depth interviews in either English or Swahili. In total, 22 interviews were conducted in English and 26 were conducted in either Swahili or a mix of Swahili and English. Focus group discussions and in-depth interviews used an interview guide that asked participants about their general perceptions of the population, their experiences interacting with SCY, their perceptions of SCY’s needs, and areas for potential intervention. A separate interview guide was developed for SCY, which asked about their experiences and interactions with the community, their perceived needs, their ability to access health care and other social services, and their interest in specific interventions. Focus group discussions lasted an average of 1.5 hours, and in-depth interviews lasted an average of 40 minutes.
Qualitative data analysis
After conducting an in-depth reading of our data, we held multiple collaborative analytic working group meetings. We developed a codebook in an iterative manner drawing on the Committee on the Rights of the Child’s General Comment 21 and the World Health Organization’s conceptual framework on the SDH.17 We developed a series of codes based on each article of the CRC to capture how existing and proposed policies and interventions respond to the needs and rights of SCY. We then analyzed how each policy or intervention relates to a specific article of the CRC and whether it could be categorized as a child rights, welfare, or repressive strategy. We used the World Health Organization’s conceptual framework on SDH inequities in our analysis to demonstrate how these proposed and existing policies and interventions intersect with the conceptual framework to determine their potential influence on health equity for SCY. We developed the final codebook by repeatedly testing its validity and comprehensiveness through test-coding transcripts. Four of the authors coded the transcripts and compared them for consistency. Analytic notes and annotations were documented and used in a series of interpretive meetings to define and refine themes.
Findings
Our analysis explores existing and proposed policies and interventions that seek to respond to the needs of SCY in Kenya. We categorize these strategies according to three major themes: repressive, welfare, and child rights-based approaches in line with the CRC.18 We explore how each type of strategy may affect socioeconomic stratification, exposures to hazards and risks, social and economic vulnerabilities, and unequal consequences for SCY in the context of the conceptual framework for tackling SDH inequities (Figure 1). In Tables 1, 2, and 3, we identify each policy or intervention, provide a supporting quotation by a study participant, categorize whether the policy or intervention is existing or proposed by study participants, identify the CRC article(s) it relates to, and outline how the policy or intervention intersects with the World Health Organization’s conceptual framework for tackling SDH inequities to reduce or increase health equity.
Table 1.
Repressive strategies to mitigate child and youth street involvement, human rights concerns, and impacts on health equity
| Policy or intervention | Quotation from study participant | Existing | Proposed | Relevant provision(s) from the Convention on the Rights of the Child | Context | Impacts on health equity |
|---|---|---|---|---|---|---|
| Forced migration | “The county government of Uasin Gishu tried, they took all of them and took them elsewhere in Western, but they came back. The governor of Busia is the one who returned them, he said that they came from that direction [laughs].” (nurse/ counselor/social worker) | X |
|
Macro level: Public policy | ↑ Exposure ↑ Vulnerabilities |
|
| Targeted violence by county askaris and law enforcement | “We have the local chief who is very brutal to us. Anytime we go for his help, he beats us up and we are often locked up by his AP officers after thorough beating.” (street-connected young person) | X |
|
Macro level: Public policy Meso level: Community Micro level: Individual |
↑ Exposure ↑ Vulnerabilities ↑ Unequal consequences |
|
| Street sweeps and roundups | “There is a time we did a sweep in town, we got over 247, we tried to take them to institutions for temporary placement and planning on how we can try and trace maybe their homes, families, relatives, so it became a challenge because some of them will run away.” (children’s officer) | X |
|
Macro level: Public policy | ↑ Exposure ↑ Vulnerabilities |
|
| Criminalization of street involvement | “Being on the street should be made an offense by the bylaws of the county government. It is a crime to be seen on the street according to the Children’s Act. If there is a bylaw, they will not be taken to prison. Children should be taken to institutions under the bylaw. The law should be that you pick a street child and take them to an institution. They are in the street because of bad associations, but actually it is illegal.” (police officer) | X | X |
|
Macro level: Public policy | ↑ Stratification ↑ Exposure ↑ Vulnerabilities |
| Remand homes, juvenile detention, and prison | “We also have a remand hall in [location redacted] and there was a time that street children and youths engaged themselves in crimes and the public was very hostile to them because two polytechnic students were murdered, and it was alleged that the street people did it, so in order to save them we had to round them up at the remand hall for sometime because it turned out very ugly.” (county children’s officer) | X |
|
Macro level: Public policy | ↑ Exposure ↑ Vulnerabilities |
|
| Separation of children from families | “I feel bad when I meet ladies with children, I usually feel like taking them home. If you take the mother, she will come back [to the street] so you just take the child.” (community member) | X |
|
Macro level: Public policy | ↑ Exposure ↑ Vulnerabilities |
|
| Forced sterilization and one-child policy | “For their population to be limited, the government should start a home for them and maybe force them and to stop more reproduction on the streets ... We should develop a policy like China, one family one child [laughs] because I have not read anywhere that there are street children in China, when you want another kid you must have a very good reason ... If you have one kid, there is a slim possibility that this child will run to the streets.” (clinical officer) | X |
|
Macro level: Public policy | ↑ Vulnerabilities ↑ Unequal Consequences |
|
| Extrajudicial killing | “Activists are convinced that the county government has embarked on a policy of trying to rid Eldoret of its street children population by killing them or killing enough of them to force the others to flee.” (Guardian, October 10, 2016) | X |
|
Macro level: Public policy Meso level: Community |
↑ Exposure ↑ Vulnerabilities |
|
Table 2.
Welfare strategies to mitigate child and youth street involvement, human rights concerns, and impacts on health equity
| Policy or intervention | Quotation from study participant | Existing | Proposed | Relevant provision(s) from the Convention on the Rights of the Child | Context | Impacts on health equity |
|---|---|---|---|---|---|---|
| Family reunification and repatriation | “Some said they had homes, but a small percentage had nowhere to go, and I remember working with the police and the civil society to remove them from the streets. We took them home and barely two weeks later they were back on the streets.” (children’s officer) | X | Article 20 on the right to special protection and assistance for children deprived of a family environment | Macro level: Public policy Meso level: Community |
↑↓ Exposure ↑↓ Vulnerabilities |
|
| Rescue centers and rehabilitation facilities | “Yes, because I feel these children are really suffering and they sniff glue. They should be well taken care of, even if they are locked up somewhere and given security and leave only when they have been rehabilitated. They should also be educated.” (police officer) | X | Article 20 on the right to special protection and assistance for children deprived of a family environment Article 3(3) on standards of care and protection institutions, services, and facilities Article 25 on periodic review of placements |
Macro level: Public policy Meso level: Community |
↑↓ Exposure ↑↓ Vulnerabilities |
|
| Children’s home | “For the small ones, there should be a children’s home that is funded partially by the community and partially by government, it would really help them. They are bright and they can learn.” (vendor) | X | Article 20 on the right to special protection and assistance for children deprived of a family environment Article 3(3) on standards of care and protection institutions, services, and facilities Article 25 on periodic review of placements |
Macro level: Public policy Meso level: Community |
↑↓ Exposure ↑↓ Vulnerabilities |
|
| Education | “Find ways of handling those who are already here by forcing them to go to school, of course talk to them first and they may do what you are telling them. Some may want to go to vocational trainings. Give them a period and those who would still refuse after this period, take actions on them because sometimes force is good.” (religious leader) | X | Article 28 on education Article 29 on the aims of education |
Macro level: Public policy | ↑ Stratification ↑ Exposure |
Table 3.
Child rights strategies to mitigate child and youth street involvement, human rights concerns, and health equity impacts
| Policy or intervention | Quotation from study participant | Existing | Proposed | Relevant provision(s) from the Convention on the Rights of the Child | Context | Impacts on health equity |
|---|---|---|---|---|---|---|
| Political representation | “We should bring a bill where we treat them as a special group of people, like we treat the disabled [and] then we elect someone to represent their interests in parliament because they are many—the data shows there are about 100,000 street children in Kenya.” (clinical officer) | X | Article 12 on the right to be heard Article 15 on the right to freedom of association and peaceful assembly Article 13 on freedom of expression Article 17 on access to information | Global level Macro level: Public policy |
↓ Stratification | |
| Education | “Those willing to go back to school, they go back to school.” (clinical officer) | X | Article 28 on education Article 29 on the aims of education Article 27 on an adequate standard of living |
Macro level: Public policy | ↓ Stratification ↓ Exposure |
|
| Vocational training | “In terms of investment as a country we are losing a lot, these are people with energy who can do much for this country because they need to participate in country building and we have to think on how to empower them through education and informal education for some like vocational training.” (community stakeholder) | X | Article 28 on education Article 29 on the aims of education Article 27 on an adequate standard of living |
Macro level: Public policy | ↓ Stratification ↓ Exposure |
|
| Life skills and empowerment | “Girls need to be made to believe in themselves, that even if they are found on the streets there is something good in them and they can work towards that and be better people later in life. Like giving them insight so that they can identify what they can do in life. We can start variety of things so that they know what to pursue, maybe they won't want to go back to school but they can do vocational training like beadwork, sewing and even gardening.” (nurse/counselor/social workers) | X | Article 28 on education Article 29 on the aims of education Article 6 on the right to life, survival, and development Article 27 on an adequate standard of living |
Macro level: Public policy Meso level: Community |
↓ Stratification ↓ Exposure ↓ Vulnerabilities |
|
| Economic and livelihood strategies | “If it's mostly youths, we will have to set up economic programs that will empower them so that they can have their own families and provide. You will find that in town they have started engaging in some economic activities, they are directing traffic and parking lots, they are doing car wash so I will go for that economic program to empower them.” (clinical officer) | X | Article 28 on education Article 29 on the aims of education Article 27 on an adequate standard of living |
Macro level: Public policy Meso level: Community |
↓ Stratification ↓ Exposure |
|
| Social protection | “I know the national government has programs targeting orphans and vulnerable children, but there should be a special program for the street families.” (community stakeholder) | X | Article 18 on parental responsibility | Macro level: Public policy | ↓ Stratification | |
| Empowerment of parents and families | “We should make the parents able. Most are from a poor family and unable to receive basic needs. We should empower parents by creating businesses and chamas [savings groups]. We can offer them rehabilitation from alcoholism.” (police officer) | X | Article 18 on parental responsibility | Macro level: Public policy Meso level: Community |
↓ Stratification ↓ Exposure |
|
| Issuing identification and documents | “What the government can do is to provide ID cards for those above 18 years and any other social support.” (clinician) | X | X | Article 7 on birth registration Article 8 on identity | Macro level: Public policy | ↓ Stratification |
| Comprehensive rehabilitation centers | “And the only way is having that facility where rehabilitation can be done, where they can access medical care, they can be able to access education, clothing and food.” (children’s officer) | x | Article 28 on education Article 20 on the right to special protection and assistance to children deprived of a family environment Article 27 on the right to an adequate standard of living Article 24 on health |
Macro level: Public policy Meso level: Community |
↓ Stratification ↓ Exposure ↓ Vulnerabilities ↓ Unequal Consequences |
|
| Medical insurance | “There is the government initiative of NHIF [National Hospital Insurance Fund], we should create a small package of taking care of their health needs that they can be able to access. It should be a social responsibility for NHIF, I am sure they are making profit.” (clinician) | X | Article 24 on health Article 33 on drug and substance use Article 27 on an adequate standard of living |
Macro level: Public policy | ↓ Stratification Vulnerabilities | |
| Access to health services | “According to our Constitution, it's a basic and fundamental right of every citizen of our country to be provided for health care by the government. If we say we are providing a special kind of medical cover for these people, you know we like free things—people will enlist themselves as street youths and children. It's better we make health universal to everyone.” (clinicians) | X | Article 24 on health Article 33 on drug and substance use Article 27 on the right to an adequate standard of living |
Macro level: Public policy | ↓ Stratification ↓ Vulnerabilities |
|
| Medical outreach | “I think there should be more medical camps for them, because when you get a street child coming to the hospital, trust me they are very sick. Most of them don't seek medical attention until it's maybe too late. So, you see the way we go to the communities to do the health camps, we could also take them to the streets for the purpose of preventions of some of these conditions.” (nurse) | X | Article 2 on non-discrimination Article 17 on access to information Article 24 on health Article 33 on drug and substance use |
Meso level: Community Micro level: Individual |
↓ Vulnerabilities ↓ Unequal Consequences |
|
| Trauma-informed primary care | “Specialized programs should be there for them because we have said that it's the responsibility of each individual. When they come to the hospitals, we should enroll them in different programs and involve the social worker and psychological counselor and try to talk to them in order to get them off the streets and find them a place to go to. Don't just see them and leave them to go back to where they were.” (nurse) | X | Article 24 on health Article 33 on drug and substance use |
Micro level: Individual | ↓ Unequal Consequences | |
| Housing and shelter | “Shelter. We should be rented for houses or taken to a safe place.” (street- connected young person) | X | Article 20 on the right to special protection and assistance to children deprived of a family environment Article 27 on the right to an adequate standard of living |
Macro level: Public policy Meso level: Community |
↓ Exposure ↓ Vulnerabilities |
|
| Feeding programs | “Find a way of giving them food, even just one meal a day. If possible, those who want to live outside the streets, a place should be found for them to live in, but the most important one is food.” (community stakeholder) | X | X | Article 27 on the right to an adequate standard of living Article 6 on the right to life |
Meso level: Community Micro level: Individual |
↓ Vulnerabilities ↓ Unequal Consequences |
| Clothing | “As long as they get food, shelter, and clothing, these children will change.” (former street-connected young woman) | X | X | Article 27 on the right to an adequate standard of living | Macro level | ↓ Exposure |
| Drop-in services | “Dropping centers will help them because they will come and shower, get food but at long last they will go back to the base.” (peer navigator) | X | Article 20 on the right to special protection and assistance to children deprived of a family environment Article 27 on the right to an adequate standard of living |
Meso level: Community Micro level: Individual |
↓ Vulnerabilities ↓ Unequal Consequences |
|
| Counseling, social work, and emotional support | “They also need love. If you rehabilitate me yet you hate me, it won’t add any value.” (clinician) “These children usually feel like they are not needed, and when you want to come up with a rehabilitation center or any program that deal with them, you will have to focus on psychological and emotional issues and you must therefore invest a lot in counseling.” (community stakeholder) |
X | Article 24 on health Article 33 on drug and substance use |
Micro level: Individual | ↓ Unequal Consequences | |
| Parenting skills | “We should also educate the parents to treat their children like humans and not abandon them because there are parents who send their children to the streets to fend for themselves.” (community leader) | X | Article 18 on parental responsibility | Meso level: Community Micro level: Individual |
↓ Vulnerabilities ↓ Unequal Consequences |
|
| Sports and recreation | “Open up a football academy in town and they form a team that has support groups so that every day after training they leave with something in their pockets and can pay rent. After that they can even play for AFC or Gor and we will say we helped them.” (peer navigator) | X | Article 31 on rest, play, and leisure | Micro level: Individual | ↓ Unequal Consequences |
Repressive strategies
Table 1 shows a number of repressive strategies that exist in Kenya or were proposed by participants to respond to the issue of child and youth street involvement. Existing strategies include forced displacement and migration, targeted violence, “street sweeps,” the criminalization of street involvement, juvenile detention, the separation of children from street families, and extrajudicial killing, all of which contravene the CRC and result in decreases in health equity. Situated within the framework for tackling SDH inequities, the majority of these strategies can be seen as public policies that result in increasing SCY’s exposures and vulnerability to specific health-compromising conditions. One exception is the criminalization of street involvement, which may increase social stratification by further affecting SCY’s socioeconomic position (for example, by leaving them with a criminal record). Nonetheless, some participants recommended the criminalization of street involvement as a policy to reduce and prevent street involvement:
We need laws in Kenya to govern the street children, a law prohibiting any child from going to the streets so that we can control that movement. (clinician)
Despite the fact that the criminalization of street involvement was abolished when the Vagrancy Act was repealed in 1997, numerous laws continue to contain provisions allowing for the arrest and detention of SCY, including the power to arrest without warrant and offenses related to idle and disorderly conduct.19 As explained by a children’s officer, SCY are frequently arrested through street sweeps, detained in prison, and eventually released back to the streets, suggesting that street involvement remains criminalized:
So the only thing they will do is sweeping them off the street, arresting them, throwing them in prison, and the prisons will reach a point where it is overwhelming because you can’t just get over 300 youths and children, bring them at the prisons, and then dump them there. What was their capacity, what plans did you have? Because even at that time, we felt bad that this is what the county government can do, doing raids at 2 a.m. in the night, gathering the children and then bringing them here. We start assessing. From the assessment, there is no aftercare plan. What do you do? Take them to prison or remand and then tomorrow again you will meet them in the street? (children’s officer)
As the children’s officer suggests, this process of criminalization does nothing to rehabilitate children and youth or reduce the harms associated with street involvement. Instead, it leaves children and youth further oppressed and provides a legal avenue to enact related repressive strategies, such as street sweeps, juvenile detention, and imprisonment.
Welfare strategies
The existing and proposed welfare strategies that we documented include family reunification and repatriation, rehabilitation and rescue centers, children’s homes (orphanages), and education (Table 2). The majority of these welfare strategies are situated at the public policy and community levels, require targeted public policies and investments, and seek to uphold article 20 of the CRC on the right to special protection and assistance for children deprived of a family environment. The impacts of these welfare strategies on health equity are variable, and many may increase or decrease health equity depending on how the policy or intervention is implemented, the quality and standards of care, and the extent to which the child’s right to be heard and involved in decision-making is considered.
Family reunification and repatriation. Immediate and extended families are the first line of care for orphaned and vulnerable children when they are able to provide a safe and appropriate care environment.20 Family reunification and repatriation represents one welfare strategy for SCY who have a home, as explained by a county children’s coordinator:
Ideally, those who have homes have to be integrated back to the community where they come from and in an organized manner. (county children’s coordinator)
However, SCY who are repatriated frequently return to the streets, as stated by a children’s officer:
Even if you are able to trace their homes and re-integrate them, after two weeks they will be back on the streets. Sometimes it is annoying, and you end up being harsh on them. When they are apprehended, some of them are remorseful and they say that they will never come to the streets again and they want to go to school. (children’s officer)
SCY report that abject poverty, family conflict, neglect, abuse, and alcoholism in the home precipitate their migration to the streets.21 As a result, it is likely that a large proportion of SCY being repatriated home subsequently return to the street due to unsafe home environments and the inability of parents or guardians to provide an adequate standard of living, including education, thereby increasing exposures and vulnerabilities and decreasing health equity. As stated by a children’s officer, many children report that “they want to go to school,” suggesting that their families were unable to send them to school and hence they returned to the streets. SCY may be repatriated without careful consideration of their best interests (CRC article 3) and without being consulted in the decision-making process (CRC article 12). When SCY willingly agree to be repatriated home, impoverished households should be supported through the provision of social protection programs (CRC article 18) and support to parents and caregivers (article 27).22 In cases where a family is unable to care for the child, temporary or permanent alternative care in institutions such as rescue centers or children’s homes may be an option.
Rescue centers and rehabilitation facilities. When children and youth connected to the streets are without parents or guardians, the state is the de facto guardian and is obliged to ensure safe alternative care to any child temporarily or permanently deprived of his or her family environment; this does not include detention cells or closed centers where children and youth are deprived of liberty.23 Safe alternative temporary care may reduce exposures and vulnerabilities, thus increasing health equity. The use of rescue centers is an existing welfare strategy promoted by children’s officers across counties as an alternative care environment that should be expanded:
Number one, street children do not belong to remand homes because these are just children in need of care and protection, and the same applies to adults living on the streets. What should be the number one priority? Because these people need rehabilitation, not just picking and taking them back home. We need a place of safe custody and what we call rescue centers. (children’s officer)
When appropriate and quality rescue centers exist, SCY may be hesitant to access them due to fear and distrust of the government as a result of the frequent use of repressive strategies. As explained by a children’s officer, SCY are reluctant to use a government child protection center that is run in partnership with a nongovernmental organization:
Like I told you before, they fear accessing this place. So, you can stay even for months without seeing a single street child being brought here at the center because of the perspective they have knowing this is the juvenile, so they imagine, “I am taking myself to be arrested.” But we try our best to tell them you can come here, access counseling. (children’s officer)
SCY’s participation in the design, implementation, and day-to-day service provision at rescue centers may build trust and therefore ensure that interventions are responsive, appropriate, and used. SCY have a right to be heard (CRC article 12) and to participate in the decision-making process regarding their placements and care environment (CRC article 20).24 Failure to consider the child’s views and their willingness to enter a specific care environment may result in them returning to the streets or being unnecessarily exposed to inequitable health outcomes.
Child rights strategies
Table 3 shows child rights strategies proposed by participants to respond to the issue of child and youth street involvement. The proposed strategies are both universal and targeted. They intersect at multiple levels with the conceptual framework for tackling SDH inequities, and so decrease social stratification, exposures, vulnerability, and unequal consequences of ill health. Despite the fact that our findings indicate that the majority of existing policies and interventions implemented in Kenya use repressive and welfare strategies, children’s officers across counties recognized that SCY are rights holders and that the CRC should guide policies and interventions for this vulnerable population. For example, one officer stated:
Here the situation is so pathetic, I remember even the UN Convention on the Rights of the Child states that a nation is supposed to create programs for such children—therefore, we must actually address the problems and give them their rights, like shelter, where something beneficial to them should be ongoing like vocational training. There should be something for each one of them, especially to prepare for their future. (children’s officer)
While the child rights strategies in this section do not exist in practice, they represent an array of contextually relevant child rights strategies that policy makers and other stakeholders could employ to address SDH inequities and improve health equity for SCY. Below, we explore the following subthemes that emerged from these proposed strategies: political representation; education, vocational training, and life skills; and housing and basic needs for an adequate standard of living.
Political representation. National governments are responsible for protecting and advancing the health equity and human rights of SCY. SCY’s participation in shaping social and health policies and interventions upholds their right to be heard (CRC article 12), right to freedom of association in civil and political space (CRC article 15), right to freedom of expression (CRC article 13), and right to access information (CRC article 17).25 One former street-connected young woman recommended that the government elicit the opinions of SCY in order to inform policy:
The government should summon them so that they can air their views so that the government knows how to help them because you cannot just push them to a place. (former street-connected young woman)
The suggestion to involve SCY in policymaking extended to the election of a representative to advocate on their behalf, as proposed by a clinician:
We should bring a bill where we treat them as a special group of people, like we treat the disabled [and] then we elect someone to represent their interests in Parliament because they are many—the data shows there are about 100,000 street children in Kenya. (clinician)
The social participation and empowerment of disadvantaged groups to shape social and health policies is an essential component of promoting health equity.26 Political representation and inclusion in dialogue and decision-making regarding social and health policies and interventions upholds SCY’s rights while also increasing the likelihood that strategies are responsive and relevant to their circumstances and needs.
Education, vocational training, and life skills. Access to free, safe, appropriate, and quality education (CRC article 28) is vital not only for preventing street involvement but also for supporting children and youth already on the streets and who are interested in returning to school. The education system should have a range options from which SCY can choose with proper guidance.27 This may include formal and informal education, vocational training, and life skills training, all of which may reduce social stratification and thereby positively affect SCY’s health equity. As suggested by one community leader, free educational facilities could be established specifically for SCY:
A school should be built to educate street children, but there should be order so that you know who the street children are, these children know each other so you just can’t bring in someone new ... It has to be free because they can’t afford, but if they have to pay, they can get sponsors when they advance with education. (community leader)
Another community leader explicitly suggested that children and youth be included in the decision-making process on education: “Ask them what they want to do and give them options to the available courses.” In addition, a peer navigator explained that entry into any education system requires consideration of SCY’s age, length of street involvement, gender, and readiness for change:
I would enroll all of them according to their ages so that you know where to fix whom, because the young ones may not be thinking about life. For those below 13 years, they can go back to school or adult learning, like at the drop-in centers there can be teachers there to help them and be taught about behavioral changes like quitting gum [glue sniffing]. If they change, if they want to learn, take them to school and do a follow-up. Some may become mechanics; take them to someone to train them. For girls, you can train them sewing and open up a place for them. That is, if they want to change. (peer navigator)
SCY across counties expressed that those who wished to return to school should be supported in doing so. The type of education they are offered should be dependent on their ages, as explained by one street-connected young man:
We think the young ones should go to school and if someone can volunteer to be their guardian so that their lives can change ... The young ones should be taken to school, for some of us we can provide for ourselves so if one has a talent, help us to nurture the talent to help ourselves. (street-connected young man)
Nurturing talents may be done through vocational and other life skills training. Older SCY generally suggested they be trained and supported in finding jobs and starting income-generating activities in lieu of returning to formal education. Safe, quality, appropriate, and free education in all of its forms may improve SCY’s socioeconomic position, lead to changes in occupation and income, and in turn help reduce social stratification and increase health equity.
Housing and basic needs for an adequate standard of living. SCY have a right to an adequate standard of living, adequate nutrition, clothing, safe housing, and free and accessible medical care and education (CRC article 27). Additionally, children deprived of a family environment have a right to special protection and assistance (CRC article 20). Housing, a care environment, and access to basic services all affect an individual’s material, social, environmental, and psychosocial circumstances, which influence their exposure and vulnerability to health-compromising conditions.28
A large proportion of participants recommended that shelter and essential basic needs be a priority in responding to the crisis of SCY in Kenya. As suggested by a clinician, “We should first consider human basic needs; they need a house, clothing, and food.” Participants proposed different strategies with respect to shelter, from the general provision of housing to that of night shelters, as stated by a vendor:
I would have a place built for them where they can come to sleep even if they loiter the whole day. Shelter is very important because they are really dying from pneumonia due to cold. On the streets you can’t tell a sick one, but if they live somewhere you can be able to tell, some even die, and you won’t know. (vendor)
Beyond housing and shelter, SCY have a right to adequate nutrition under CRC articles 6 (right to life) and 27 (adequate standard of living). Nutrition is fundamental to a child’s survival and development and can reduce the unequal consequences of ill health. One religious leader suggested implementing a feeding program:
Maybe feeding because most of them suffer from malnutrition, sometimes they don’t eat. Or they eat things from the dustbin. A good feeding program is important. (religious leader)
However, the use of feeding programs was opposed by children’s officers in some counties, due to fears of “pull factors” (that is, drawing children to the street):
We also need to do away with these feeding program which people think is the best even within the business community not knowing that this is a pull factor. (children’s officer)
To avoid this risk, some suggested that feeding programs be connected to broader long-term services:
I am not for the idea of a feeding program that is not connected to a long-term solution, so feeding them and allowing them to go back to the streets is not right. If you feed them, even those in estates will always come for lunch, even if they are in schools. (county children’s officer)
The fact that children and youth not connected to the streets might leave school at lunchtime to access a feeding program may point to a broader community issue of household food insecurity among vulnerable children and youth living in informal settlements. Therefore, a feeding program intervention may require a universal rather than targeted policy—such as a universal school lunch program in addition to feeding programs for SCY—to address vulnerable children’s right to adequate nutrition regardless of their street involvement.
A model to advance health equity for street-connected children and youth
Our findings suggest that existing repressive and welfare-based strategies may contribute to health inequities for SCY in Kenya by increasing socioeconomic stratification, exposures to hazards and health risks, vulnerabilities, and unequal health consequences. As a result, we have developed a checklist for policy makers and other stakeholders to help them assess how their policies, programs, and services are upholding SCY’s human rights, addressing their needs, and working to advance health equity (Figure 3). This checklist can also guide local and national governments and other stakeholders in prioritizing their responses to the many needs of SCY. Using a child rights approach and drawing on Maslow’s hierarchy of needs, we propose that at the foundation of any response be an immediate obligation to meet SCY’s physiological needs.29 The overall goal of this checklist is to assist stakeholders in ensuring that SCY are able to enjoy minimum essential levels of their social, economic, and cultural rights, while doing so in a manner that meets SCY’s most pressing needs in a hierarchy of influence. While all of the rights outlined in the CRC are essential, implementing policies and interventions to respond to the issue of child and youth street involvement and reduce the harms associated with street life requires careful consideration of which basic needs must be met before an individual is able to modify their behavior and shift their motivation to the next emerging need in the hierarchy.30 For example, a child will not be able to actively participate and learn in school (safety), or in sports and other recreational activities (self-actualization), if their basic physiological need for food is unmet. Therefore, we suggest using the checklist to work from implementing policies and interventions that support SCY’s physiological needs first and foremost, followed by safety, love and belonging, self-esteem, and self-actualization.
Figure 3.
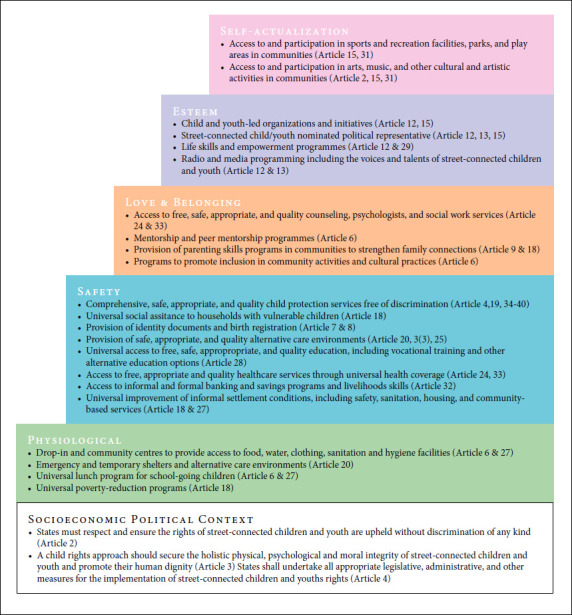
Checklist for assessing whether policies and interventions are upholding SCY’s human rights and addressing their needs
Discussion
Our findings indicate that the majority of policies and interventions that have been implemented to respond to the issue of SCY in Kenya are repressive and welfare strategies that contravene the CRC.31 It is important to note that policies and interventions that we classified as welfare strategies (such as family reunification and repatriation, as well as rescue centers and rehabilitation) may be rights-based when children and youth are involved in the decision-making process regarding their care. Notably, our results suggest that a diverse range of actors, including government officials, across Kenya recognize the importance of children’s rights and have recommended numerous contextually relevant child rights strategies that can be implemented and evaluated for their effectiveness and impact on health equity for SCY.
It is clear that a range of policies and interventions are required to tackle structural and intermediary determinants by reducing social stratification, differential exposures and vulnerabilities, and the unequal consequences of ill health; no one intervention will meet all of SCY’s rights and needs. The social, economic, and health inequities experienced by SCY are multiple and require a coordinated intersectoral government and civil society response.32 Our checklist outlined above can be used to support policy makers and civil society in doing so within a framework that upholds SCY’s human rights. Given the lack of existing evidence-based policies and interventions for SCY in low- and middle-income countries, governments, stakeholders, and researchers should collaborate to design, implement, and evaluate strategies that may be situated within this checklist.33
Existing child rights and evidence-based poverty reduction strategies, such as Kenya’s cash-transfer program for orphaned and vulnerable children, could, for example, be extended to all impoverished households caring for the most vulnerable children and youth.34 Given that household poverty is a primary structural determinant of children and young people’s street involvement, alleviating poverty and improving households’ ability to adequately care for children will likely reduce the number of children and youth who migrate to the streets.35 Critically, there is a need to develop and implement social welfare programs for children and youth who are already connected to the streets. Direct assistance to children and youth through the provision of food, safe places to live, and free and accessible medical care and education is fundamental to their rights to special protection, assistance, and an adequate standard of living.
This study has both strengths and limitations. Our investigation solicited the ideas of a diverse range of actors across Kenya. We also upheld SCY’s right to be heard by actively involving former and current SCY in identifying policies to advance health equity—a crucial component of an effective plan for action on SDH equity. Moreover, our analysis was situated in the World Health Organization’s widely used and well-regarded conceptual framework on SDH inequities in conjunction with the CRC, making it appropriate for and applicable to addressing health equity through legal and political reform. Despite these strengths, the geographic limitations of our study mean that our findings may not be generalizable to all counties in Kenya or to other low- or middle-income countries. Nonetheless, we believe that our recommendations can be adapted to other low- and middle-income countries, given their foundation in the CRC and the World Health Organization’s framework on SDH inequities. While our checklist is meant to provide guidance, we recognize that it is not exhaustive and that other child rights policies and intervention options may exist. We encourage those using this tool to situate their child rights policies and interventions within the hierarchy and carefully consider the context for implementation and their mechanisms of action and impact on health equity.
Conclusion
Child rights strategies and intersectoral collaboration are required to respond to the epidemic of child and youth street involvement and to reduce the harms associated with street life. Although repressive and welfare strategies are the ones most employed in Kenya, utilizing a child rights approach would provide a strong framework for advancing health equity through action on the SDH for SCY in Kenya. Our findings point to several policies and interventions that can be evaluated for their effectiveness in reducing street involvement and ameliorating the health and well-being of SCY.
References
- 1.Committee on the Rights of the Child. 2017. General Comment No. 21, Children in Street Situations, UN Doc. CRC/C/GC/21.; Winston S. E., Chirchir A. K., Muthoni L. N. et al. “Prevalence of sexually transmitted infections including HIV in street involved adolescents in western Kenya,”. Sexually Transmitted Infections. 2015;91(5):305. doi: 10.1136/sextrans-2014-051797. [DOI] [PMC free article] [PubMed] [Google Scholar]; Embleton L., Ayuku D., Atwoli L. et al. “Knowledge, attitudes, and substance use practices among street children in western Kenya,”. Substance Use and Misuse. 2012;47(11):1234–1247. doi: 10.3109/10826084.2012.700678. [DOI] [PMC free article] [PubMed] [Google Scholar]; Goldblatt A., Kwena Z., Lahiff M. et al. “Prevalence and correlates of HIV infection among street boys in Kisumu, Kenya,”. PLoS ONE. 2015;10(10) doi: 10.1371/journal.pone.0140005. [DOI] [PMC free article] [PubMed] [Google Scholar]; Braitstein P., Ayaya S., Nyandiko W. M. et al. “Nutritional status of orphaned and separated children and adolescents living in community and institutional environments in Uasin Gishu County, Kenya,”. PLoS One. 2013;8(7):e70054. doi: 10.1371/journal.pone.0070054. [DOI] [PMC free article] [PubMed] [Google Scholar]; Atwoli L., Ayuku D., Hogan J. et al. “Impact of domestic care environment on trauma and posttraumatic stress disorder among orphans in western Kenya,”. PLoS One. 2014;9(3):e89937. doi: 10.1371/journal.pone.0089937. [DOI] [PMC free article] [PubMed] [Google Scholar]; Embleton L., Ayuku D., Makori D. et al. “Causes of death among street-connected children and youth in Eldoret, Kenya,”. BMC International Health and Human Rights. 2018;18(1) doi: 10.1186/s12914-018-0160-8. [DOI] [PMC free article] [PubMed] [Google Scholar]; Save the Children. The chronic urban emergency in Rift Valley Kenya: Report from profiling children connected to the streets in Rift Valley Province. Save the Children and UNICEF; 2012. [Google Scholar]
- 2.Embleton L., Shah P., Gayapersad-Amin A. “Characterizing street-connected young people’s social and health inequities in Kenya using the conceptual framework on social determinants of health and convention on the rights of the child: A qualitative investigation,”. 2020. under review.; Gayapersad A., Embleton L., Shah P. “Using a sociological conceptualization of stigma to explore the social process of stigmatization and discrimination of street-connected children and youth in Kenya,”. 2020. under review.
- 3.Coren E., Hossain R., Pardo Pardo J. et al. “Interventions for promoting re-integration and reducing harmful behaviour and lifestyles in street-connected children and young people,”. Cochrane Database of Systematic Reviews. 2016;1 doi: 10.1002/14651858.CD009823.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Berckmans I., Velasco M. L., Tapia B. P. et al. “A systematic review: A quest for effective interventions for children and adolescents in street situation,”. Children and Youth Services Review. 2012;34(7):1259–1272. Ibid. [Google Scholar]; Dybicz P. “Interventions for street children: Analysis of current best practices,”. International Social Work. 2005;48(6):763–771. [Google Scholar]
- 5. Constitution of Kenya (2010).
- 6.1989. Convention on the Rights of the Child, G.A. Res. 44/25.; United Nations. Signatures and ratifications of the Convention on the Rights of the Child. Available at https://treaties.un.org/Pages/ViewDetails.aspx?src=IND&mtdsg_no=IV-11&chapter=4&lang=en.; Republic of Kenya. Children Act. 2012.
- 7.Republic of Kenya. Twelfth Parliament (No. 033) – (Third Session) The Senate Order Paper. Republic of Kenya; 2019. [Google Scholar]
- 8. Save the Children (see note 1).
- 9.Solar O., Irwin A. A conceptual framework for action on the social determinants of health. 2010. Social Determinants of Health Discussion Paper 2 (Policy and Practice)
- 10. Ibid.
- 11. Ibid.
- 12.1989. Ibid.; Convention on the Rights of the Child, G.A. Res. 44/25.
- 13. Committee on the Rights of the Child (see note 1).
- 14. Ibid.
- 15.Maslow A. “A theory of human motivation,”. Psychological Review. 1943.
- 16.Einterz R. M., Kimaiyo S., Mengech H. N. K. et al. “Responding to the HIV pandemic: The power of an academic medical partnership,”. Academic Medicine: Journal of the Association of American Medical Colleges. 2007;82:812–818. doi: 10.1097/ACM.0b013e3180cc29f1. [DOI] [PubMed] [Google Scholar]
- 17. Committee on the Rights of the Child (see note 1); Solar and Irwin (see note 9).
- 18. Committee on the Rights of the Child (see note 1), para. 5.
- 19.Republic of Kenya. National Police Service Act. 2016. ; Republic of Kenya. The Penal Code Chapter 63. 2009. ; South African Litigation Centre. Vagrancy-related provisions in various criminal laws and criminal procedure laws in Africa. 2018. pp. 1–26.
- 20. Committee on the Rights of the Child (see note 1), para. 35.
- 21.Sorber R., Winston S., Koech J. et al. “Social and economic characteristics of street youth by gender and level of street involvement in Eldoret, Kenya,”. PLoS One. 2014;9(5):e97587. doi: 10.1371/journal.pone.0097587. Save the Children (see note 1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Committee on the Rights of the Child (see note 1), paras. 48, 49.
- 23. Ibid., para. 44.
- 24. Ibid., paras. 33, 45.
- 25. Ibid., paras. 33, 37, 42.
- 26. Solar and Irwin (see note 9).
- 27. Committee on the Rights of the Child (see note 1), paras. 48–49.
- 28. Ibid.
- 29. Maslow (see note 15).
- 30. Ibid.
- 31. Committee on the Rights of the Child (see note 1), para. 5.
- 32. Solar and Irwin (see note 9).
- 33. Berckmans et al. (see note 4); Coren et al. (see note 3).
- 34.Bryant J. H. “Kenya’s cash transfer program: Protecting the health and human rights of orphans and vulnerable children,”. Health and Human Rights Journal. 2009;11(2):65–76. [PubMed] [Google Scholar]
- 35.Embleton L., Lee H., Gunn J. et al. “Causes of child and youth homelessness in developed and developing countries: A systematic review and meta-analysis,”. JAMA Pediatrics. 2016;170(5) doi: 10.1001/jamapediatrics.2016.0156. Sorber et al. (see note 21). [DOI] [PMC free article] [PubMed] [Google Scholar]