

Abstract
Background:
The clinical applicability of the minipterional (MPT) craniotomy is still limited to small and superficial anterior circulation aneurysms. We discuss the technical nuances of a modified MPT approach, the extradural MPT approach (eMPTa), for the treatment of a giant intracranial aneurysm (GIA) arising from the paraclinoid carotid artery.
Case Description:
A 44-year-old female presented with facial hypoesthesia and third cranial nerve palsy. Further investigations revealed the presence of a 27 mm aneurysm arising from the communicating segment of the internal carotid artery. The patient underwent surgical clipping through an extradural MPT craniotomy and combined anterior clinoidectomy. Postoperative angio-computed tomography demonstrated complete aneurysm occlusion and patency of the parent vessels. The patient recovered fully from her previous deficits.
Conclusion:
The skull base drilling, interdural dissection, and anterior clinoidectomy are key steps during the eMPTa that optimizes the use of the extradural corridor. Such adaptations are enough to improve the surgical maneuverability along the paraclinoid region and adapt the MPT suitability for the treatment of complex GIA.
Keywords: Keyhole, Microsurgical, Oculomotor, Pterional, Skull base

BACKGROUND
In spite of many advantages of the minipterional (MPT) craniotomy, its clinical applicability is still regarded to be limited to small and superficial aneurysms located in the anterior circulation.[1,11] Reports of large aneurysms treated through these small craniotomies are simply scarce.[6,7,9] In this manuscript, we present the technical nuances of a variation of the MPT approach, the extradural MPT approach (extMPTa) in the setting of a giant paraclinoid internal carotid artery (ICA) aneurysm.
METHODS: CASE REPORT
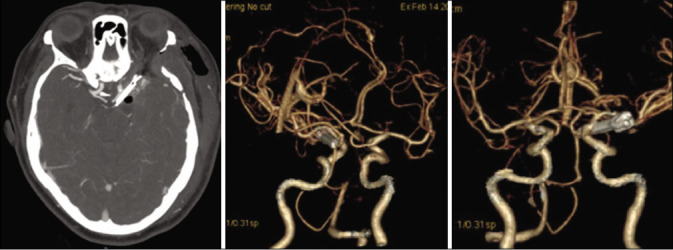
A 44-year-old male with a medical history of arterial hypertension and chronic headaches presented with sudden-onset left third cranial nerve palsy and ipsilateral facial hypoesthesia. Computed tomography (CT) revealed a nonruptured left parasellar giant intracranial aneurysm (GIA) [Figure 1].
Figure 1:
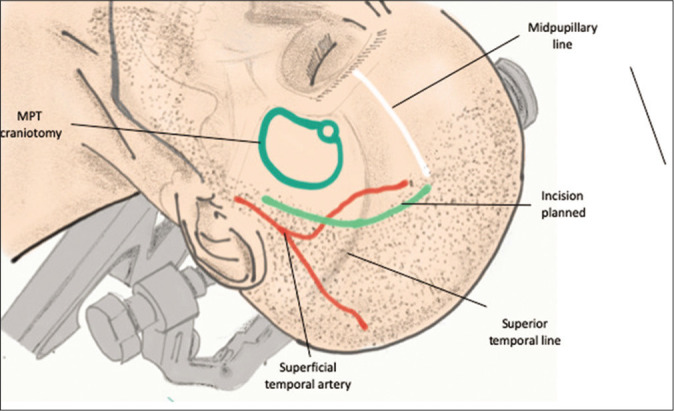
Positioning: the patient is positioned supine, with the neck slightly extended and the head laterally rotated, approximately 30 degrees. The head rotation may be modified by tilting the table, as needed (e.g., a more lateral inclination is needed during partial orbitotomy or anterior clinoidectomy). A curvilinear scalp incision is started 1 cm above the base of the zygomatic arch. It is extended superiorly, about 1 cm behind the hairline, and curved gradually toward the ipsilateral midpupillary line. The superior border of the minipterional craniotomy is the superior temporal line.
CT angiography and a digital subtraction cerebral angiogram delineated a 27 mm saccular GIA at the junction of the ICA and posterior communicating cerebral artery [Figure 2]. Surgical and endovascular treatment modalities including coiling and flow diversion were taken into consideration. Given the aneurysm size, its relatively wide neck, and the patient’s young age, surgical clipping was preferred for longer durability.
Figure 2:
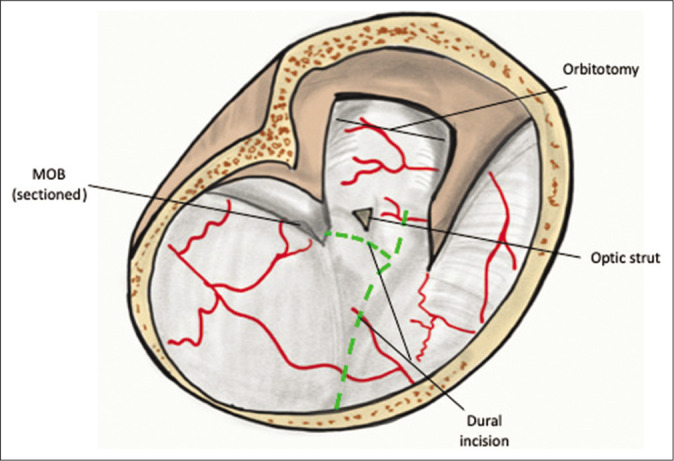
Extradural minipterional approach: the dural incision is shown by the dashed line. First, a linear cut, which follows the axis of the Sylvian fissure and is projected toward the space between the optic nerve and the internal carotid artery, is performed. The second cut is performed anterior to the optic nerve and directed inferiorly, in the direction of the cavernous sinus, followed by the division of the external dural ring. MOB: Meningo-orbital band.
The patient underwent surgical clipping through an extradural MPT craniotomy and combined anterior clinoidectomy. Postoperative angio-CT demonstrated complete aneurysm occlusion and patency of the parent vessels. The patient recovered fully from her previous deficits.
Informed consent for publication of the present manuscript was obtained from the patient. Elaboration of this work was performed in accordance with the ethical standards of our institution (institution #2) and the Helsinki Declaration.
RESULTS
Relevant surgical anatomy
The MPT craniotomy is a pterion-centered craniotomy entirely located below the superior temporal line.[2] The anterior edge of the pterion corresponds to the anterior Sylvian point.[10] The ASyP is the widest space along the Sylvian fissure and is considered a safe start point to proceed with a proximal Sylvian fissure dissection[10]
Periosteal and visceral layers of the dura converge at the lateral edge of the superior orbital fissure, creating a virtual space between them, that is used as a cleavage plane during the interdural dissection.[3] The parietal layer of the dura constitutes at this level the meningo-orbital band (MOB)
The paraclinoid segment of the ICA extends between two dural extensions of the cavernous sinus, the internal and external dural rings.[5] The external dural ring adheres closely to the ICA and the anterior clinoid process (ACP).[5]
Description of the technique
Positioning
The patient’s head is fixed in gentle extension and laterally rotated approximately 30° toward the contralateral side of the incision [Figure 1 and Video 1].
Incision and craniotomy
The skin is incised 1 cm behind the hairline between the midpupillary line and the zygoma [Figure 1]. After performing an interfascial dissection of the temporalis fascia, the temporalis muscle is inferiorly retracted to expose the pterion. A MPT craniotomy is performed.[2]
Extradural anterior clinoidectomy
We consider appropriate to further divide this stage in five simple steps:
The sphenoid ridge is drilled flat until the lateral MOB is exposed
Partial osteotomy of the lateral and superior wall of the orbit
Division of the MOB and mini-peeling of the middle fossa. The mini-peeling consists of an outer layer dissection of the lateral wall of the cavernous sinus in an interdural fashion, until the first and second branches of the trigeminal nerve are exposed. This maneuver allows temporal pole mobilization and exposes the ACP
Optic canal decompression by removal of the superior wall (unroofing) and drilling of the optic strut
Once the ACP is disconnected, the tip and body of the ACP is carefully removed using a curved rongeur.
Dural opening, subdural dissection, and clipping
The dura is opened in a linear fashion along the axis of the Sylvian fissure followed anteriorly to its proximal end between the optic nerve and the ICA [Figure 2]. Further brain relaxation is achieved by opening the carotid cistern and splitting of the proximal part of the Sylvian fissure. The distal dural ring is then completely incised to allow free mobilization of the anterior vertical segment of the ICA and for achieving proximal control. The anterior clinoidectomy facilitates the localization of the third cranial nerve sparing the dura at the oculomotor triangle [Figure 3]. The third cranial nerve is then followed backward and liberated from the aneurysm dome adhesions. This step is extremely important to decompress the oculomotor nerve and avoid reattachment or nerve torsion during clipping. After these steps are performed, proximal control is obtained, the aneurysm is deflated and clipped with a straight long D-clip (Peter Lazic, GmbH Microsurgical Innovations, Tuttlingen, Germany) and a straight 5 mm fenestrated clip.
Figure 3:
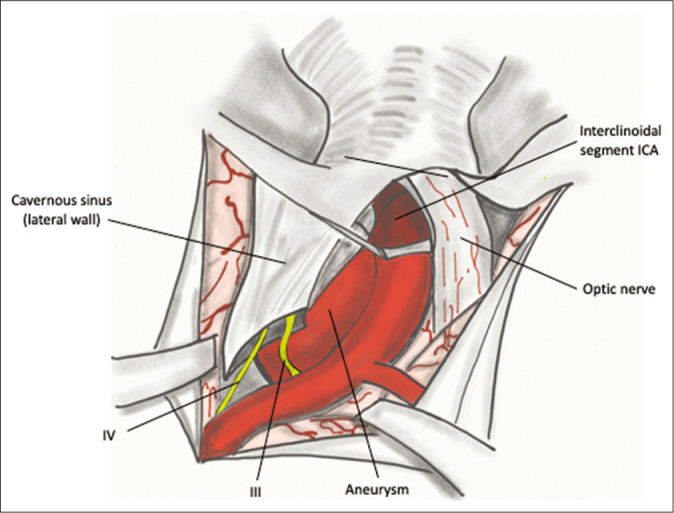
Extradural minipterional approach, subdural view: once the aneurysm is exposed, the third cranial nerve can be found as it enters the oculomotor triangle. The cisternal segment of the third cranial nerve is then followed posteriorly and liberated from its attachments to the aneurysm dome. ICA: Internal carotid artery, III: Third cranial nerve, IV: Fourth cranial nerve.
DISCUSSION
Indications
Unlike the traditional intradural MPT approach,[2] by exploiting the extradural corridor (maximization of the sphenoid ridge drilling, mini-peeling of the temporal fossa, and ACP removal), the extradural minipterional approach improves the surgical maneuverability in a narrow corridor, such as that provided by the MPT craniotomy.[8] These modifications enable the MPT suitability for approaching nonruptured complex aneurysms in the anterior circulation, including GIA, such as the case we are presenting.
Limitations
Although the extradural corridor can allow improved maneuverability compared to that provided by the traditional intradural MPT approach, the rather small craniotomy size might be insufficient for ruptured large and giant cerebral aneurysms.
Moreover, the access to the subfrontal corridor is hampered by the limited exposure of the frontal lobe. Hence, lesions located above the sphenoid ridge and near the midline are more suitable to be approached through shorter and more straightforward routes, such as a supraorbital or an extended supraorbital approach.[6]
How to avoid complications
Clips should always be selected preoperatively, and a tentative clipping strategy should be carefully planned ahead of time. This will help reduce the stress caused by an intraoperative rupture and increase chances of achieving a satisfactory result
Usage of indocyanine green video angiography is warranted to confirm aneurysm occlusion and rule out inadvertent clipping or kinking of perforators or distal branches
For large and giant paraclinoid aneurysms and in almost all vascular cases requiring an anterior clinoidectomy, it is advisable to expose the carotid bifurcation in the neck prior to proceeding with the subdural dissection, to achieve satisfactory proximal control
Section of the distal dural ring facilitates the mobilization of the paraclinoid ICA and allows better aneurysm visualization prior to clipping. Moreover, opening the distal dural ring allows to place a temporary clip right above the origin of the ophthalmic artery and facilitates proximal control intradurally.
Specific perioperative considerations
Preoperative CT scan (bone window) and CTA are recommended to ascertain the distance between the aneurysm neck and the ACP and preoperatively determine the necessity of performing an anterior clinoidectomy [Figure 4]. MRI should be considered in cases in which there is a high suspicious of aneurysm thrombosis and mass effect [Figure 4]. Preoperative angiogram studies are also key to assess the chances of achieving a complete occlusion of the aneurysm with surgical clipping or the need of performing a surgical revascularization [Figure 5].
Figure 4:
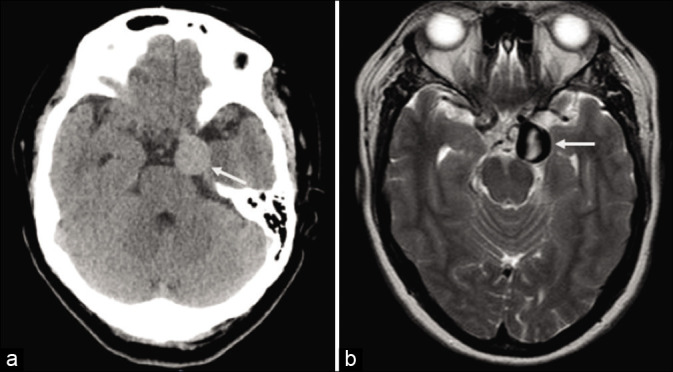
CT scan (a) and MR T2-weighted images (b) revealed a left 28 parasellar 27 mm partially thrombosed aneurysm (arrow).
Figure 5:

Preoperative diagnostic angiogram (a – anteroposterior view; b – lateral view; c – 3D reconstruction) showed a giant wide neck posterior communicating aneurysm. A fetal posterior communicating artery is noted (arrow heads).
Specific information to give to the patient and potential risks
The patient must know there is a small risk, <15%, of developing diplopia due to oculomotor nerve manipulation during the clinoidectomy or aneurysm manipulation, that might be transient or permanent.[12] If diplopia is presented prior to the intervention, there is an up to 50% chance to achieve complete recovery after treatment.[12] Another possible major complication is an intraoperative aneurysm rupture, which may lead to a disastrous outcome.[8,9]
CONCLUSION: KEY POINTS
The MPT craniotomy is a minimally invasive technique, whose clinical applicability is still regarded to be limited to small and superficial aneurysms of the anterior circulation[2]
The extradural MPT craniotomy is a modification of the aforementioned approach that includes a mini-peeling of the middle fossa and an anterior clinoidectomy[4,7,8]
These extradural steps, along with the proximal dissection of the Sylvian fissure, provide a wider corridor to approach the parasellar region through a minimally invasive approach
The extradural anterior clinoidectomy is a key step of the approach to aneurysms that are obscured by the ACP. This maneuver enhances the surgical corridor and facilitates better understanding of the anatomy
Beyond the cosmetic and time-saving advantages of the MPT craniotomy, the illustrated case shows how the extMPTa can be safely and efficiently applied to a paraclinoid GIA [Figure 6].
Figure 6:
Postoperative CTA confirmed complete occlusion of the giant aneurysm and patency of the ipsilateral posterior communicating artery and all other parent vessels.
Supplementary Material
Footnotes
How to cite this article: Martinez-Perez R, Tsimpas A, Joswig H, Hernandez-Alvarez V, Mura J. Extradural minipterional approach for giant intracranial aneurysms. Surg Neurol Int 2020;11:382.
Contributor Information
Rafael Martinez-Perez, Email: rafa11safin@hotmail.com.
Asterios Tsimpas, Email: atsimpas@gmail.com.
Holger Joswig, Email: holger.joswig@googlemail.com.
Victor Hernandez-Alvarez, Email: victor.hernandez.a@hotmail.com.
Jorge Mura, Email: doctormapez@gmail.com.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos available on:
REFERENCES
- 1.Davies JM, Lawton MT. Advances in open microsurgery for cerebral aneurysms. Neurosurgery. 2014;74(Suppl 1):S7–16. doi: 10.1227/NEU.0000000000000193. [DOI] [PubMed] [Google Scholar]
- 2.Figueiredo EG, Deshmukh P, Nakaji P, Crusius MU, Crawford N, Spetzler RF, et al. The minipterional craniotomy: Technical description and anatomic assessment. Neurosurgery. 2007;61:256–64. doi: 10.1227/01.neu.0000303978.11752.45. [DOI] [PubMed] [Google Scholar]
- 3.Fukuda H, Evins AI, Burrell JC, Iwasaki K, Stieg PE, Bernardo A. The meningo-orbital band: Microsurgical anatomy and surgical detachment of the membranous structures through a frontotemporal craniotomy with removal of the anterior clinoid process. J Neurol Surg B Skull Base. 2014;75:125–32. doi: 10.1055/s-0033-1359302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hakuba A, Nishimura S, Shirakata S, Tsukamoto M. Surgical approaches to the cavernous sinus. Report of 19 cases (author’s transl) Neurol Med Chir (Tokyo) 1982;22:295–308. doi: 10.2176/nmc.22.295. [DOI] [PubMed] [Google Scholar]
- 5.Joo W, Funaki T, Yoshioka F, Rhoton AL. Microsurgical anatomy of the carotid cave. Neurosurgery. 2012;70:300–11. doi: 10.1227/NEU.0b013e3182431767. [DOI] [PubMed] [Google Scholar]
- 6.Martínez-Pérez R, Albonette-Felicio T, Hardesty DA, Prevedello DM. Comparative anatomical analysis between the minipterional and supraorbital approaches. J Neurosurg. 2020 doi: 10.3171/2019.12.JNS193196. [DOI] [PubMed] [Google Scholar]
- 7.Martínez-Pérez R, Hernández-Álvarez V, Maturana R, Mura JM. The extradural minipterional pretemporal approach for the treatment of spheno-petro-clival meningiomas. Acta Neurochir (Wien) 2019;161:2577–82. doi: 10.1007/s00701-019-04064-3. [DOI] [PubMed] [Google Scholar]
- 8.Martinez-Perez R, Joswig H, Albiña P, Perales I, Poblete T, Mura JM. The extradural minipterional approach for the treatment of paraclinoid aneurysms: A cadaver stepwise dissection and clinical case series. Neurosurg Rev. 2020;43:361–70. doi: 10.1007/s10143-019-01219-9. [DOI] [PubMed] [Google Scholar]
- 9.Mattingly T, Kole MK, Nicolle D, Boulton M, Pelz D, Lownie SP. Visual outcomes for surgical treatment of large and giant carotid ophthalmic segment aneurysms: A case series utilizing retrograde suction decompression (the “Dallas technique”) J Neurosurg. 2013;118:937–46. doi: 10.3171/2013.2.JNS12735. [DOI] [PubMed] [Google Scholar]
- 10.Ribas GC, Yasuda A, Ribas EC, Nishikuni K, Rodrigues AJ. Surgical anatomy of microneurosurgical sulcal key points. Neurosurgery. 2006;59:ONS177–210. doi: 10.1227/01.NEU.0000240682.28616.b2. [DOI] [PubMed] [Google Scholar]
- 11.Rychen J, Croci D, Roethlisberger M, Nossek E, Potts MB, Radovanovic I, et al. Keyhole approaches for surgical treatment of intracranial aneurysms: A short review. Neurol Res. 2019;41:68–76. doi: 10.1080/01616412.2018.1531202. [DOI] [PubMed] [Google Scholar]
- 12.Signorelli F, Pop R, Ganau M, Cebula H, Scibilia A, Gallinaro P, et al. Endovascular versus surgical treatment for improvement of oculomotor nerve palsy caused by unruptured posterior communicating artery aneurysms. J Neurointerv Surg. 2020;12:964–7. doi: 10.1136/neurintsurg-2020-015802. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.