

Abstract
Context:
Osteoarthritis (OA) is a degenerative joint disease, having multifactorial etiology affecting mainly the articular cartilage. Knee OA with its physical symptoms affects daily activities thereby deteriorating the quality of life. Most of the patients delay their visit to health sectors for seeking medical care in musculoskeletal conditions.
Aims:
To find the prevalence and determinants of osteoarthritis among the adult population in the rural area and to assess their health-seeking behavior.
Settings and Design:
A community-based, cross-sectional study.
Methods and Material:
A community-based, cross-sectional study was conducted among 232 adults living in a rural area in village Kirpind of R.S. Pura block, Jammu. Knee OA was diagnosed using the clinical criteria laid down by the American College of Rheumatology (ACR).
Statistical Analysis Used:
Descriptive statistics, OR with 95% CI, and Chi-square test were used for the purpose of analysis.
Results:
The overall prevalence of knee osteoarthritis was 35.7% (females: 44.5% Males: 23.1%). Age more than 60 years, female gender, history of trauma, BMI >30 were found to be significantly associated with higher odds of OA knee (P < 0.05). Descriptive statistics, OR with 95% CI and Chi-square test were used for the purpose of analysis.
Conclusions:
Strategies focusing on creating awareness among the rural elderly regarding the role of a balanced diet, exercise, and weight management along sensitization of primary health care providers concerning benefits of early screening, diagnosis, and referral should be undertaken to minimize this burden.
Keywords: ACR criteria, determinants, knee OA, prevalence, primary care
Introduction
The epidemiologic transition has changed the pattern of diseases globally both in developed as well as developing regions. Innovations in public health and medicine along with overall improvement in socioeconomic status have attenuated the burden of infectious diseases but at the same time this has led to an increased prevalence of noncommunicable diseases. This is especially pertinent in a country like India, which is facing a double burden of communicable and noncommunicable diseases resulting in increased morbidity and mortality. Among non communicable diseases, the condition that affects people across the life course, in all regions of the world is musculoskeletal in nature.[1]
Musculoskeletal conditions comprised of 150 diseases or syndromes, which are usually progressive and painful.[2] Back and neck pain, rheumatoid arthritis, fractures, and osteoarthritis are among the most disabling among these. Osteoarthritis is a disease involving inflammation of the bone and joint cartilage in which all structures of the joint undergo pathologic changes, often in concert[3] and is most common arthritis encountered among the elderly. Apart from considerable morbidity, OA is known for reducing the quality of life, which is measured by Disability Adjusted Life Years and Years lived with Disability. The global burden of disease study, 2010 reported OA as the eleventh main cause of years lived with disability in the world.[4] It is the fourth most frequent predictor of health problems worldwide in women and the eighth-most common predictor in men.[5]
In India, many studies have reported osteoarthritis as the second most common rheumatologic problem[6] and the most frequently occurring joint disease with a prevalence ranging from 22% to 39%.[7] OA is broadly classified into primary and secondary. Primary osteoarthritis is having no known cause and is usually the result of ageing process while secondary OA is attributed to injuries related to squatting and kneeling jobs. Most commonly involved joints are knees, hips, lower spine region, and fingers but it can also affect the hands and feet.
Increasing age, female sex, obesity, sedentary lifestyle, no or minimal physical activity, improper dietary patterns all are contributing factors for osteoarthritis. The patient usually complains of grating sounds during joint movement, swelling, and tenderness of joints, and limited range of motion. Apart from these physical symptoms, it results in mental agony due to impairment of daily routine activities. Symptoms of joint pain are usually ignored for many years, especially by females as they usually relate it with excessive physical work during household chores. Health care is usually sought only when it hampers physical activity and usually, pain relief is the only symptom, which compels people to reach health care service providers.
Management of OA includes both pharmacological and nonpharmacological measures. Nonpharmacological measures include education, health awareness, weight loss, use of braces, and physiotherapy while pharmacological measures only improve the quality of life by assuaging the pain. Commonly used drugs are pain killers, NSAIDs, opioids, and intra articular corticosteroids. Surgery is required in some cases where pharmacological measures fail to ameliorate the symptoms.
Health seeking behavior of an individual or community is influenced by a multitude of factors like environment in which they are living, customs, and traditions, which are being followed in their community and last but not the least their financial condition. It is very important to comprehend the health care seeking patterns at the individual level so as to fill the gaps between the felt needs of the community and health care delivery both in urban as well as rural populations. Most of the studies on osteoarthritis are hospital-based and very limited data is available at the community level, especially from rural areas. This study is an attempt to delve into the epidemiological determinants of OA and to assess the health-seeking behavior of the elderly, which dictates their medical management.
Objective
To find the prevalence and determinants of osteoarthritis among the rural adult population and to assess their health-seeking behavior with regard to knee osteoarthritis.
Subjects and Methods
A community-based, cross-sectional study was conducted at village Kirpind, which comes under Miran Sahib Primary Health center, R.S. Pura block. The block is also the field practice area of the Department of Community Medicine. The study was done for a period of three months (May, June, and July 2019). The ethical clearance was taken from the Institutional Ethical Committee. Line listing of the total number of houses in the village was done and all the adults, both male and female above 50 years of age were enlisted as the eligible/potential participants. The subjects were explained about the study purpose and those who gave their verbal consent and were found eligible for participation in the study were chosen. Those who were not found in their respective homes even after two visits, who were bedridden, and did not give their consent for participation in the study were excluded. Following this method of nonprobability sampling, the final sample size turned out to be 232. House to house visits were done for data collection. A pretested questionnaire consisting of three parts was used in the study. The first part included socio-demographic details such as age, sex, religion, per capita income, physical activity, and socioeconomic status (according to modified Udhay Pareek scale). The second part had two subheadings; the first included clinical criteria used by ACR[8] to diagnose cases of osteoarthritis and the second subheading consisted of questions eliciting health care-seeking behavior of subjects. American College of Rheumatology uses three criteria for the classification of knee osteoarthritis clinical, laboratory, and radiographic criteria. Clinical criteria include knee pain plus at least any three of the six factors listed as follows a) age >50 years b) morning stiffness <30 min c) crepitus d) bony tenderness e) bony enlargement f) no palpable warmth. Diagnosis of knee OA was made in the presence of any three above listed factors along with knee pain. The third part of the proforma consisted of right and left knee joint examination and anthropometric measurements (weight, height, and waist circumference).
Data was entered in Microsoft Excel spreadsheet and analyzed using Open Epi tool kit version 3.01. Relationship between OA and various variables was assessed by calculating the odds ratio with corresponding 95% confidence interval, and its statistical significance was assessed by using Chi-square test. A P value of less than 0.05 was considered statistically significant, and all P values used were two-tailed.
Results
The overall prevalence of Knee osteoarthritis among study participants was 35.7% [Table 1] with female preponderance 44.5vs23.1 [Figure 1].
Table 1.
Prevalence of Knee OA among study participants
| Sex | Knee Osteoarthritis | Total | |||
|---|---|---|---|---|---|
| Present | Absent | ||||
| n | Percentage | n | Percentage | ||
| Male | 22 | 23.1 | 73 | 76.9 | 95 |
| Female | 61 | 44.5 | 76 | 55.4 | 137 |
| Total | 83 | 35.7 | 149 | 64.3 | 232 |
Figure 1.
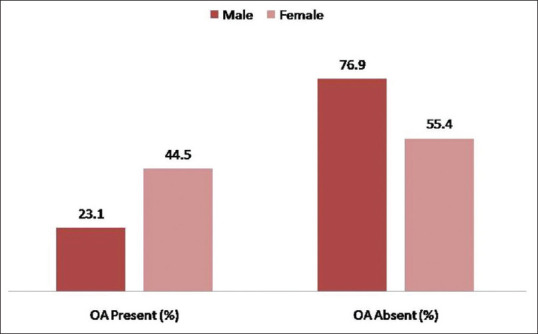
Gender wise prevalence of Osteoarthritis among Study participants
Pain in the knee was a universal symptom in all cases of osteoarthritis while a majority of positive cases also complained of bony tenderness, crepitus, and bony overgrowth [Figure 2]. However, morning stiffness was complained by only half of male cases, by the majority of females and was almost absent in normal adults. The warmth was a symptom in two-third males and one-third females suffering from OA [Table 2].
Figure 2.
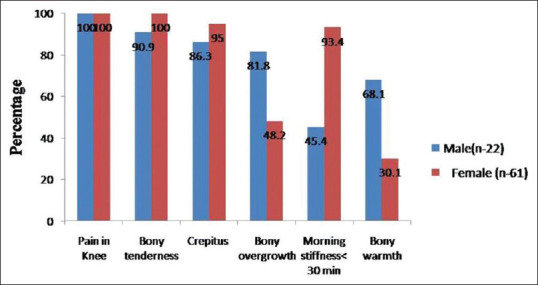
Clinical Profile of Study Participants with OA according to ACR criteria
Table 2.
Clinical profile of Study participants according to ACR criteria
| ACR Criteria | Osteoarthritis Present (n-83) | Osteoarthritis Absent (n-149) | ||||||
|---|---|---|---|---|---|---|---|---|
| Male (n-22) | Female (n-61) | Male (n-73) | Female (n-76) | |||||
| n | Percentage | n | Percentage | n | Percentage | n | Percentage | |
| Pain in Knee | 22 | 100 | 61 | 100 | 19 | 26.0 | 23 | 30.2 |
| Bony tenderness | 20 | 90.9 | 61 | 100 | 04 | 5.4 | 03 | 3.9 |
| Crepitus | 19 | 86.3 | 58 | 95.0 | 03 | 4.1 | 01 | 1.3 |
| Bony overgrowth | 18 | 81.8 | 40 | 48.2 | 01 | 1.3 | 00 | 00 |
| Morning stiffness <30 min | 10 | 45.4 | 57 | 93.4 | 00 | 00 | 02 | 2.6 |
| Bony warmth | 15 | 68.1 | 25 | 30.1 | 06 | 8.2 | 02 | 2.6 |
A total of 232 subjects participated in the study out of which two-fifth were males and three- fifth were females. 75% of participants were in the age group of 50–69 years. Nearly 40% of them had normal BMI scores. Two-third of participants were sedentary workers. Hindus contributed a major share of study participants followed by Sikhs. The odds of OA were three times more in adults who were 60 plus as compared to those in the age group of 50–59 years. Similarly, being female was associated with significantly higher odds of osteoarthritis in comparison to males. Being sedentary, overweight, vegetarian, and having a history of trauma also showed significantly higher chances of suffering from knee OA [Table 3].
Table 3.
Association of Socio demographic variables with OA Knee Joint
| Characteristic | Osteoarthritis | Total | OR (95% CI) | P | |
|---|---|---|---|---|---|
| Present n % | Absent n% | ||||
| Gender | |||||
| Female | 61 (44.5) | 76 (55.5) | 137 | 2.66 (1.4- 1.7) | 0.0008 S |
| Male | 22 (23.1) | 73 (76.9) | 95 | ||
| Age (yrs) | |||||
| ≥60 | 63 (46.3) | 73 (53.7) | 136 | 3.26 (1.8-6.0) | 0.0006 S |
| 50-59 | 20 (26.3) | 76 (79.7) | 96 | ||
| Per capita monthly income | |||||
| ≤5000 | 36 (37.8) | 59 (62.2) | 95 | REF | 0.1NS |
| 5000-10000 | 20 (28.1) | 51 (71.9) | 71 | 1.5 (0.8-3.0) | |
| ≥10,000 | 27 (40.9) | 39 (59.1) | 66 | 0.8 (0.4-1.6) | |
| BMI | 0.0001S | ||||
| >30 | 20 (60.0) | 13 (40.0) | 33 | 3.32(1.5-7.0) | |
| ≤30 | 63 (31.0) | 136 (69.0) | 199 | ||
| H/o Trauma to knee joint | |||||
| Yes | 70 (43.0) | 90 (57.0) | 160 | 3.53 (1.7-6.9) | 0.0001 S |
| No | 13 (18.1) | 59 (81.9) | 72 | ||
| Eating Habits | |||||
| Vegetarian | 49 (48.0) | 53 (52.0) | 102 | 2.61(1.5-4.5) | 0.0001S |
| Non vegetarian | 34 (26.0) | 96 (74.0) | 130 | ||
| Physical activity | 0.0001S | ||||
| Sedentary | |||||
| Moderate | 65 (83.3) | 13 (16.6) | 78 | ||
| Religion | |||||
| Hindu | 55 (36.3) | 100 (66.7) | 150 | REF | 0.6 NS |
| Muslim | 20 (32.2) | 42 (67.8) | 62 | 1.15 (0.6-2.1) | |
| Sikh | 8 (40.0) | 12 (60.0) | 20 | 0.8 (0.3-2.1) | |
Oil, drugs, and massage were the most common remedial measures taken by the patients suffering from osteoarthritis. The distance was the most common reason for not seeking treatment [Table 4].
Table 4.
Health Care Seeking Behavior of the Study Participants
| Health care seeking behavior | Number (n-83) | Percentage |
|---|---|---|
| Have you sought treatment for the disease | ||
| Yes | 56 | 67.4 |
| No | 27 | 32.6 |
| Choice of practitioner by the participants Allopathic Doctor | 30 | 36.1 |
| Chemist | 08 | 9.6 |
| Ayurvedic Doctor | 18 | 21.7 |
| None | 27 | 32.6 |
| *Modalities of treatment chosen by the participants | ||
| Balm | 08 | 9.6 |
| Oil | 32 | 38.6 |
| Massage | 15 | 18.0 |
| Hot fomentation | 12 | 14.5 |
| Drugs | 16 | 19.3 |
| Treatment compliance | ||
| Yes | 49 | 59.0 |
| No | 34 | 41.0 |
| Physiotherapy and Exercise | ||
| Yes | 22 | 26.6 |
| No | 61 | 73.4 |
| *Reason by participants for not seeking treatment (n-27) | ||
| Distance | 12 | 44.5 |
| None to accompany | 06 | 22.2 |
| Ignorance | 04 | 14.8 |
| Financial problems | 05 | 18.5 |
*Multiple answers
Discussion
Various studies conducted in different settings and in different communities have reported the overall prevalence of knee osteoarthritis in the range of (19.5%–56%).[9,10,11,12] In our study, the overall prevalence of knee OA was 35.7% with higher prevalence among females (44.5%), which is almost similar (41.6%) to the study done by Anitha Bhaskar et al.[13] and 23.1% among males, which is in concordance with the study done by other authors.[14,15] Female predominance can be attributed to hormonal changes after menopause and their preponderance among study participants. Elderly adults that are older than 60 years in our study were at greater risk for having knee osteoarthritis as compared to adults less than 60 years of age. Age-related changes in the joint are responsible for an increase in the prevalence of osteoarthritis in the geriatric group. This was in tune with other studies.[16,17,18,19] Those with a positive history of knee trauma had 3.5 times higher odds as compared to those having no history of trauma in our study. MK Sasidharan et al. in their study also reported similar findings.[20] Obesity is a well-known modifiable risk for osteoarthritis and BMI has been considered a useful measure of obesity. Coggon et al.[21] reported that subjects with a BMI >30 kg/meter square were 6.8 times more likely to develop knee OA than normal weighing controls whereas in our study, the odds were 3.32 times. Trauma results in an unstable joint, which in turn activates several molecular mechanisms, which contribute to the progression of OA.[22] Previous injuries to joint, being overweight, and obese were also found to be predictive of lower limb OA by a study conducted by Schram Ben et al.[22,23] Similar findings were observed in a case-control study conducted in Pakistan by Maghimi Nasrin et al.[24]
Diet and physical activity of an individual play an important role in bone health. Indians from rural areas usually rely on a vegetarian diet and are more prone to micronutrient deficiencies, especially calcium, phosphorus, magnesium, iron, etc., due to ignorance, which contributes to bone and joint problems. Vegetarian diet and sedentary lifestyle in our study were associated with higher odds of getting osteoarthritis (2.67 and 36.7 times). A study conducted by J Venkatachalam et al. also found a higher risk of developing OA with no physical activity.[14]
Though there is limited literature on health-seeking behaviors, our study found that nearly two-thirds of the subjects sought treatment for osteoarthritis, and more than one-third of adults preferred allopathic treatment. Nearly three-fourth of subjects were unaware of the beneficial effects of exercise and physiotherapy. In a study conducted by Deshmukh et al. about half of the study population was unaware of nonpharmacological but effective measures for osteoarthritis.[25] This highlights the need to increase awareness among the rural population.
Conclusion
More than one-third of the study participants were found to be suffering from Knee OA. OA knee is associated with high BMI, female sex, history of trauma to knee joint, and decreased physical activity as evident in the present study. The study also attempts to assess the true prevalence of knee OA so as to provide a baseline data from the grass-root level as not all patients seek health care due to a multitude of reasons. This data can aid in planning more in- depth and detailed intervention studies with larger sample sizes and for planning future cost- effective preventive strategies.
Recommendations
Attempts should be made to reach out to the adults in their middle age and possibly before, so that importance of healthy nutrition, weight management, and exercise coupled with equipping the target group with the right knowledge may be used as effective tools in ameliorating the ubiquitous challenge of osteoarthritis in our community.
Key Messages
Though pain alleviation is the goal of treatment seekers, it is health promotion by behavioral change communication, which is the need of the hour.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Musculoskeletal conditions. World Health Organization. Available from: https://wwwwhointnewsroom/factsheet/detail/musculoskeltal conditions .
- 2.Briggs AM, Woolf AD, Dreinhöfer K, Homb N, Hoy DG, Giles DK, et al. Reducing the global burden of musculoskeletal conditions. Bull World Health Organ. 2018;96:366–68. doi: 10.2471/BLT.17.204891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Longo D, Kasper A, Fauci V. Harrison's principles of internal medicine. New York: McGraw-Hill; 2012. [Google Scholar]
- 4.Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global burden of disease study 2010. Lancet. 2012;380:2163–96. doi: 10.1016/S0140-6736(12)61729-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Murray CJL, Alan D World Health Organization, World Bank & Harvard School of Public Health. (996) In: The Global Burden of disease: A comprehensive assessment of mortality and disability from diseases, injuries and risk factors in 1990 and Projected to 2020. Christopher J, L Murray, Alan D, editors. Lopez. Boston: Harvard School of Public Health; [Google Scholar]
- 6.Silman AJ, Hochberg MC. Epidemiology of the Rheumatic Diseases. 2nd ed. Oxford: Oxford University Press; 2001. [Google Scholar]
- 7.Symmons D, Mathers C, Pfleger B. Global burden of osteoarthritis in year 2000: Global burden of disease 2000 study World Health Report 2002; 5 Version 2 [Google Scholar]
- 8.Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, et al. The American college of rheumatology criteria for the classification and reporting of osteoarthritis of knee. Arthritis Rheum. 1986;29:1039–49. doi: 10.1002/art.1780290816. [DOI] [PubMed] [Google Scholar]
- 9.Kaur R, Sharma V, Singh A. Prevalence of knee osteoarthritis and its correlation in women of rural and urban parts of Hoshiarpur (Punjab) J Postgrad Med Edu Res. 2015;49:32–6. [Google Scholar]
- 10.Joshi K, Rajesh K, Avasthi A. Morbidity profile and its relationship with disability and psychological distress among elderly people in Northern India. Int J Epidemiol. 2003;32:978–87. doi: 10.1093/ije/dyg204. [DOI] [PubMed] [Google Scholar]
- 11.Salve H, Gupta V, Palanivel C, Yadav K, Singh B. Prevalence of knee osteoarthritis amongst perimenopausal women in an urban resettlement colony in South Delhi. Indian J Public Health. 2010;54:155–7. doi: 10.4103/0019-557X.75739. [DOI] [PubMed] [Google Scholar]
- 12.Sharma MK, Swami HM, Bhatia V, Verma A, Bhatia SPS, Kaur G. An epidemiological study of correlates of osteo-arthritis in geriatric population of UT Chandigarh. Indian J Community Med. 2007;32:77–8. [Google Scholar]
- 13.Bhaskar A, Areekal B, Vasudevan B, Ajith R, Ravi S, Sankar S. Osteoarthritis of knee and factors associated with it in middle aged women in a rural area of central Kerala, India. Int J Community Med Public Health. 2016;3:2926–1. [Google Scholar]
- 14.Venkatachalam J, Natesan M, Eswaran M, Johnson AK, Bharath V, Singh Z. Prevalence of osteoarthritis of knee joint among adult population in a rural area of Kanchipuram District, Tamil Nadu. Indian J Public Health. 2018;62:117–22. doi: 10.4103/ijph.IJPH_344_16. [DOI] [PubMed] [Google Scholar]
- 15.Hakmaosa A, Baruah KK, Hajong S. A community based cross sectional study on morbidty pattern of elderly in Rani block, Kamrup (rural) district, Assam. Indian J Basic Appl Med Res. 2014;3:72–9. [Google Scholar]
- 16.Das AK, Routray D, Panigrahi TK. Prevalence and risk factors of knee osteoarthritis in a rural community of Odisha: A snap shot study. JMSCR. 2018;6:15–1. [Google Scholar]
- 17.Plotnikoff R, Karunamuni N, Lytvyak E, Penfold C, Schopflocher D, Imayama I, et al. Osteoarthritis prevalence and modifiable factors: A population study. BMC Public Health. 2015;15:1195. doi: 10.1186/s12889-015-2529-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ajit NE, Nandish B, Fernandes RJ, Roga G, Kasthuri A, Shanbhag D, et al. Prevalence of knee osteoarthritis in rural areas of Bangalore urban district. Inter J Rheumatol Clin Immunol. 2014;1(S1) doi: 1015305/ijrci/v1iS1/49. [Google Scholar]
- 19.Aimi Asyrani Zamri N, Harith S, Aini Mohd Yusoff N, Mat Hassan N, Qian Ong Y. Prevalence, risk factors and primary prevention of osteoarthritis in Asia: A scoping review. Elderly Health J. 2019;5:19–1. [Google Scholar]
- 20.Sasidharan MK, Pappu AK, Devakumar I, Vikram K, Surendran M, Jayasree JT. Risk factors of osteoarthritis – a hospital based case control study. Acad Med J India. 2014;2:49–1. [Google Scholar]
- 21.Coggon D, Reading I, Croft P, McLaren M, Barrett D, Cooper C. Knee osteoarthritis and obesity. Int J Obes Relat Metab Disord. 2001;25:622–7. doi: 10.1038/sj.ijo.0801585. [DOI] [PubMed] [Google Scholar]
- 22.Jimenz G, Cobo Molinos J, Antich C, Lopez Ruiz E. Osteoarthritis trauma vs disease. Adv Expo Med Bio. 2018;1059:63–3. doi: 10.1007/978-3-319-76735-2_3. [DOI] [PubMed] [Google Scholar]
- 23.Schram B, Orr R, Pope R, Canetti E, Knapik J. Risk factors for development of lower limb osteoarthritis in physically demanding occupations: A narrative umbrella review. J Occup Health. 2020;62:e12103. doi: 10.1002/1348-9585.12103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Moghimi N, Rahmani K, Delpisheh A, Saidi A, Azadi NA, Afkhamzadeh A. Risk factors of knee osteoarthritis: A case-control study. Pak J Med Sci. 2019;35:636–40. doi: 10.12669/pjms.35.3.277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Deshmukh SA, Kalkonde YV, Deshmukh MD, Bang AA, Bang AT. Healthcare seeking behavior for back and joint pain in rural Gadchiroli, India: A population-based cross-sectional study. Indian J Community Med. 2014;39:229–34. doi: 10.4103/0970-0218.143026. [DOI] [PMC free article] [PubMed] [Google Scholar]