

Abstract
We report a case of a 28-year-old male who presented in the emergency room with a history of two episodes of syncope in the last 3 days at home. ECG was done in the emergency room which was suggestive of complete heart block. The patient had a history of pain on and off in the right upper quadrant region (RUQ) after having a meal. Ultrasonography of the abdomen was advised which revealed acute calculous cholecystitis. A temporary pacemaker was inserted and an emergency laparoscopic cholecystectomy was planned. The patient recovered postoperatively and converted back to sinus rhythm. Considering the patient's age, normal cardiac workup, and his complete heart block disappeared after the removal of his gallbladder, it was postulated that this patient had a case of cardio-biliary reflex (Cope's sign).
Keywords: Acute calculous cholecystitis, cardio-biliary reflex, complete heart block
Introduction
A third-degree atrioventricular (AV) block or complete heart block is characterized by independent atrial and ventricular activity. The hemodynamic consequences depend on the ventricular rate and the presence of underlying heart disease.[1] A complete heart block is most commonly caused by coronary artery disease or by degeneration of the cardiac conduction system.
Acute cholecystitis is most commonly caused by gallstones. Acute cholecystitis develops in 1–3% of patients with symptomatic gallstones and is diagnosed based on symptoms and signs of inflammation in patients with localized peritonitis in the right upper quadrant (RUQ).[2] Abdominal ultrasound is the investigation of choice in suspected acute cholecystitis. Ultrasonography (USG) typically shows pericholecystic fluid, gallbladder distension, gallbladder wall edema, and gallstones.
In this case report, we would like to present the case of a 28-year-old male patient with acute calculous cholecystitis, which was complicated by complete heart block.[3]
Case Report
A 28-year-old male patient was brought into the emergency room (ER) with a history of two episodes of syncope at home. He also had a history of pain in the RUQ region on and off after having a meal. The pain was colicky, localized in the RUQ, and reflected back. The onset of pain began 3 days back after eating meals. He had multiple episodes of nausea and vomiting which had gastric contents in the last 3 days.
The patient was evaluated and examined. Upon physical examination, the patient was afebrile, blood pressure was 100/70 mmHg, pulse 38/min, no heart murmur was detected, RUQ tenderness without guarding, and a positive Murphy's sign. A surgical consultation was taken and USG was done which was suggestive of acute calculous cholecystitis.
The electrocardiogram (ECG) was recorded which was suggestive of complete heart block [Figure 1] with a heart rate 38/min. Cardiology consultation was taken and 2 D echocardiography was done which was normal.
Figure 1.
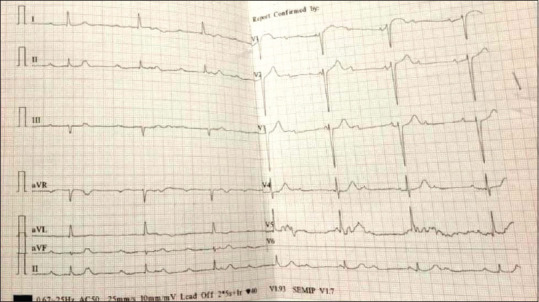
Electrocardiogram at presentation showing of complete heart block
The radiography of the abdomen was without abnormalities. Laboratory studies revealed hepatic amylase, lipase, and cardiac enzymes (troponins) which were within normal limits, and the patient's C-reactive protein and leukocytes were only mildly elevated.
Ultrasonography of the abdomen revealed that the gallbladder was 10 cm in length, with the wall thickening and findings of pericholecystic fluid. Multiple concrements were present in the gallbladder [Figure 2]. The cardiologist placed a temporary heart pacemaker via the femoral vein providing optimal ventricle stimulation. An emergency laparoscopic cholecystectomy was performed without any complications. The histopathological examination confirmed gangrenous acute cholecystitis. Almost 10 h after the surgical procedure the patient was in sinus rhythm [Figure 3] and, the temporary pacemaker was removed. Postoperative recovery was uneventful. The patient recovered quickly and completely from surgery without any residual sequelae.
Figure 2.
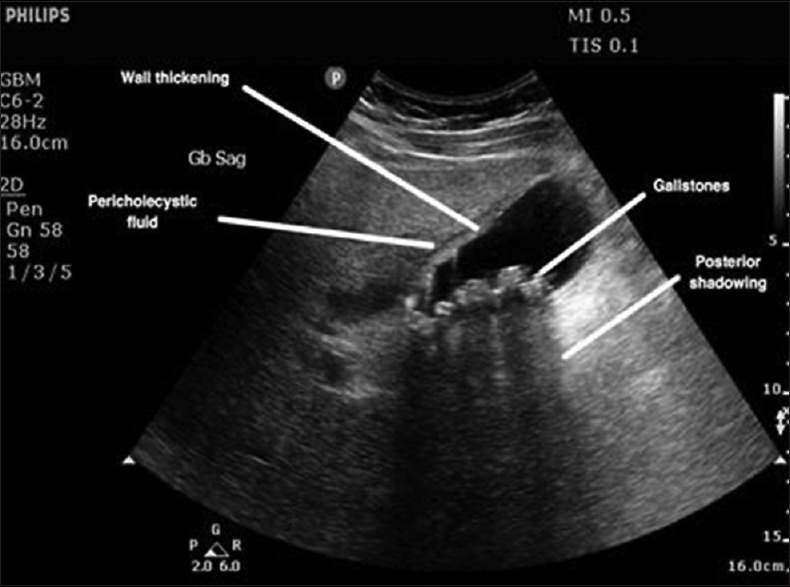
Ultrasonography abdomen showing features of cholecystitis with cholelithiasis
Figure 3.
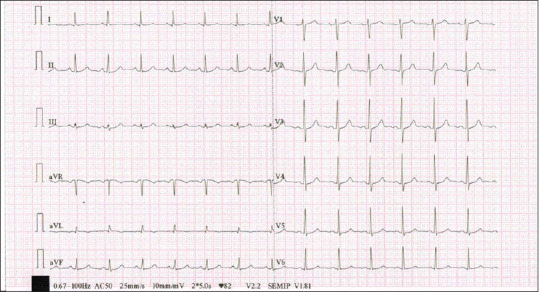
Postoperative electrocardiogram showing normal sinus rhythm
Discussion
Cope's sign was named by Sir Zachary Cope who was the first patient reported with cardio-biliary reflex.[4] Cardio-biliary reflex is thought to be vagally mediated. More specifically, cardio-biliary reflex has been triggered by pain in the gallbladder via autonomic vagal innervations.[5] Bradyarrhythmia is the most common clinical presentation of the cardio-biliary reflex. Cardiac enzymes, especially serum troponin, play a crucial role in the differential diagnosis in such cases, as dynamic ECG changes due to the reflex (ST-segment elevation, T wave inversion, right bundle branch block) are not uncommon. A case-control study in 1967 by Kaufman and Lubera[6] reported that the gallbladder could increase vagal tone, which could mimic myocardial infarction or cause bradyarrhythmia and even complete heart block. Franzen et al.[7] reported a 48-year-old healthy male patient who suffered three syncopal episodes while awaiting a cholecystectomy. During the third syncope, an episode of complete AV block without escape rhythm for 9 s was documented through an ECG. A laparoscopic cholecystectomy was performed and the patient remained symptom-free after the 1-year follow-up period. In another similar case, Vloka et al.[8] presented a patient with complete AV block due to chronic cholecystitis.
Conclusion
Cardio-biliary reflex can cause severe bradyarrhythmia, even a complete heart block. Considering the patient's age, normal cardiac biomarkers tests, and the disappearance of the complete heart block after the removal of the gallbladder, it was postulated that this patient had a case of cardio-biliary reflex. Cardio-biliary reflex does exist and can results in serious consequences. Special attention to patients with acute cholecystitis having abnormal ECG changes should be considered, well-monitored, and managed correctly to avoid possible complications.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Hayden GE, Brady WJ, Pollack M, Harrigan RA. Electrocardiographic manifestations: Diagnosis of atrioventricular block in the emergency department. J Emerg Med. 2004;26:95–106. doi: 10.1016/j.jemermed.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 2.Indar AA, Beckingham IJ. Acute cholecystitis. Br Med J. 2002;325:639–43. doi: 10.1136/bmj.325.7365.639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Franzen D, Jung S, Fatio R, Brunckhorst CB. Complete atrioventricular block in a patient with acute cholecystitis: A case of cardio-biliary reflex? Eur J Emerg Med. 2009;16:346–7. doi: 10.1097/MEJ.0b013e32832baed8. [DOI] [PubMed] [Google Scholar]
- 4.Cope Z. A sign of gall -bladder disease. Br Med J. 1970;3:147–8. doi: 10.1136/bmj.3.5715.147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lau YM, Hui WM, Lau CP. Asystole complicating acalculous cholecystitis, the “Cope's sign” revisited. Int J Cardiol. 2015;182:447–8. doi: 10.1016/j.ijcard.2014.12.153. [DOI] [PubMed] [Google Scholar]
- 6.Kaufman JM, Lubera R. Preoperative use of atropine and electrocardiographic changes. Differentiation of ischemic from biliary-induced abnormalities. JAMA. 1967;200:197–200. [PubMed] [Google Scholar]
- 7.Franzen D, Jung S, Fatio R, Brunckhorst CB. Complete atrioventricular block in a patient with acute cholecystitis: A case of cardio-biliary reflex? Eur J Emerg Med. 2009;16:346–7. doi: 10.1097/MEJ.0b013e32832baed8. [DOI] [PubMed] [Google Scholar]
- 8.Vloka ME, Tamis JE, Steinberg JS. Neurally mediated syncope in 2 patients with extracardiac disease. Arch Intern Med. 1999;159:625–7. doi: 10.1001/archinte.159.6.625. [DOI] [PubMed] [Google Scholar]