

Abstract
Background:
Nowadays, the prevalence of coronary heart disease has challenged the lives of families around the world. Anxiety is one of the most important consequences of coronavirus. The nurse-led telephone follow-ups (tele-nursing) are a way to train nurses to further improve nursing services and increase the patients' well-being. The aim of this study was to determine the effect of nurse-led telephone follow-ups (tele-nursing) on the level of anxiety of people with coronavirus who spend their quarantine and treatment at home.
Methods:
In this semi-experimental study, the number of sample was 100 newly diagnosed patients with Corona, who were tested positive using the CT scan of the lungs and were selected by continuous sampling. In this study, Spielberger's state-trait anxiety inventory was used to collect data before and after the intervention. Samples were randomly divided into control and intervention groups (50 subjects in each group) after receiving initial training in the form of lectures on the corona disease, and the tele-nursing program was implemented on the intervention group every other day for 21 consecutive days. Finally, after the end of the 21st day and the completion of the tele-nursing intervention, the questionnaire was again completed by the control and intervention groups and the results of both groups were compared.
Results:
The results indicated that the level of anxiety in the two groups after the training program and tele-nursing were significantly different (p < 0.001) and the mean score of the anxiety level after the training program and tele-nursing was significantly reduced (p < 0.001).
Conclusion:
This study showed that tele-nursing has had a significant effect on reducing the anxiety level of people with Cavid-19 virus. As the telephone technology is available in most clients' homes and its use is easy and accessible, it is recommend including this technology in the field of nursing care and training especially in relation to people with coronavirus.
Keywords: Anxiety, coronavirus, tele-nursing
Introduction
Today, the name coronavirus is widely used and many people in the world are losing their lives due to the infection with this virus. In December 2019, Covid-19 as an acute respiratory disease was identified in China. The researchers followed the spread of the virus and developed a diagnostic test for Covid-19. Coronaviruses are a large family of viruses that cause respiratory infections ranging from colds to more severe illnesses such as MERS and SARS. Recently, the virus is called Covid-19.[1] The Middle East Respiratory Syndrome or MERS is also a viral respiratory disease that was first reported in 2012 in Saudi Arabia and spread to several countries until now. Severe acute respiratory syndrome (SARS) is a viral respiratory illness caused by a Covid-SARS coronavirus. SARS was first reported in Asia in February 2003. In 2003, SARS spread to more than a dozen countries in North America, South America, Europe, and Asia.[2] The virus caused by Covid-19 is easily spread in the society in some geographical areas. This local spread means that people in an area are infected with the virus. Some people are not sure how or where they became infected.[3] Coronavirus has spread rapidly in various cities in Iran, causing people to experience varying degrees of anxiety. The symptoms of this virus vary from mild to severe. Symptoms and signs of infection include fever, cough, and difficulty in breathing.[4] Anxiety is a common symptom in patients with chronic respiratory disorders and it could reduce patients' quality of life significantly. Almost all cases of anxiety assessment include physical cases that can overlap with the symptoms of chronic respiratory disease and the side effects of medications.[5] Chronic lung diseases, including lung disorders, are highly associated with anxiety disorders. As the disease becomes more severe and prolonged, the association with anxiety is greater.[6] In various studies, the higher prevalence of depression and anxiety in patients with chronic lung disease has been reported compared to other disorders. A study conducted by Coventry on patients with chronic obstructive pulmonary disease (COPD), it was found that 20–40 percent of these patients had anxiety symptoms.[7] Pietras et al. found that there was a positive association between anxiety and dyspepsia.[8] Clinical anxiety involves up to two-thirds of chronic respiratory patients, which leads to reduced quality of life and physical function. Little research has been done on the experiences of anxiety in patients with severe respiratory symptoms.[9] Anxiety about Covid-19 is common, which is due to the unknown and cognitive ambiguities among the individuals about the virus. Fear of the unknown reduces the perception of human immunity and causes anxiety among humans.[10] In the case of Covid-19, the low scientific knowledge continues to exacerbate this anxiety.[11] One of the ways through which enables nurses to train to enhance nursing services and achieve increased patient well-being, is tele-nursing. Tele-nursing is a branch of telemedicine. In tele-nursing, nurses can provide nursing care to patients through telecommunication facilities and information technology remotely. Tele-nursing provides patient education without time or space constraints. It reduces the costs and improves the quality of nursing care.[12] Providing the tele-nursing services allows high flexibility in the creativity and innovation of the nursing process and the development of professional nursing services in various aspects of the profession, including training, research, management, and clinical services.[13] Because of the increase in the prevalence of coronavirus, the importance of the effect of this disease on the level of anxiety of the infected people, and considering that people with Covid-19 have several problems, it is decided to affect their level of anxiety using tele-nursing.
Materials and Methods
This study was a quasi-experimental investigation. The research environment included the emergency departments of selected hospitals for the admission of people with corona (Masih Daneshvari and Besat Hospitals). The research samples included 100 people (men and women) who were given a definitive diagnosis of corona after a coronary examination with a CT scan of their lungs, and the physician prescribed home quarantine, medication, and continued treatment at home that were selected by the continuous sampling in the research environment. The questionnaire used to collect data in this study consists of two parts. The first part was the researcher-made questionnaire that included demographic information (age, level of education, marital status, and job) and the second part was the standard Spielberger Anxiety Inventory, which showed the current level of anxiety in patients. This inventory is widely used in the clinical activities and research and it contains separate self-assessment scales to measure the obvious and hidden anxiety. It is translated into 30 living languages of the world and adapted to Iranian culture for example standardized.[14] Mahram (1994) calculated the reliability of the mentioned test through Cronbach's alpha on the norm population (0.9452). Generally, the scores of 20–42, 43–64, and 65–85 are classified as mild, moderate and severe anxiety.[15] All research samples that had the conditions to enter the study (Corona test and positive lung CT scan showed that Corona was definitively diagnosed) and were selected as continuous sampling, filled the informed consent form to participate in the study. Then the training program was implemented on the samples using the lecture method associated with the corona disease. In this training program, information about the nature of corona disease, symptoms, and methods of preventing the transmission of this virus to others were provided to the samples. In the next step, the samples were randomly divided into control and intervention groups. The standard Spielberger anxiety questionnaire was completed by all subjects (control and case groups). Only the training program was implemented on the control group through lectures and 21 days after completing the first questionnaire, the Spielberger Anxiety Inventory was completed again by this group. For the intervention group, in addition to the training program, Tele-Nursing counseling was performed for 3 weeks every other day. Finally, the standardized Spielberger's anxiety was completed by the intervention group three weeks after the end of the tele-nursing program. SPSS software, Chi-square, Fisher's exact, paired t, and independent t tests were used to analyze the data.
Results
The research results showed that the mean age in patients in the control group was 42.44 ± 9.02 and that of the intervention group was 42.66 ± 9.39. The independent t-test showed that the two groups were not significantly different in terms of age (p-value = 0.921). The results of the Fisher's exact and Chi-square tests indicate that both groups were homogeneous in terms of demographic characteristics such as gender, marital status, level of education, and job. The level of anxiety in each group was assessed before the training and after the training using the paired t-test [Table 1 and Figures 1-4]. The results showed that there is a statistically significant difference between the groups before and after the training. The level of the anxiety score decreased after training, which indicates an improvement in the condition. However, the two training groups were compared only through lecturing and the group that in addition to training through lecturing had distance learning (tele-nessing). The results of the independent t-test showed that before the training, the anxiety level score did not have a statistically significant difference and was homogeneous in the two groups. However, after training, the anxiety level score between the two groups had a statistically significant difference. Although anxiety levels were reduced and improved in both groups, they were further reduced in the intervention group, which in addition to educational lectures had distance learning as well.
Table 1.
Comparison of anxiety level between control and intervention group in pretest and posttest step along with paired t-test between same treatment for pre and post step
| Control | Intervention | Independent sample t-test | P | |
|---|---|---|---|---|
| Pretest | 67.06±5.23 | 68.09±4.47 | -1.02 | 0.23 |
| Posttest | 44.39±4.47 | 31.01±4.23 | 15.38 | <0.001 |
| Paired t-test | 1.08 | 1.19 | - | - |
| P | <0.001 | <0.001 | - | - |
Figure 1.
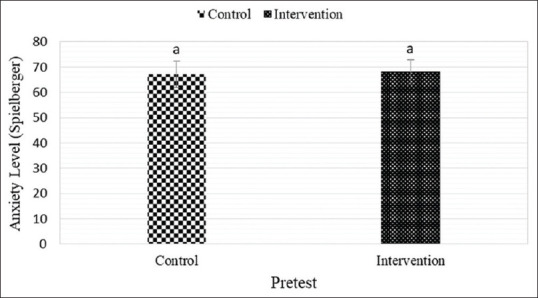
Independent sample t test between control and intervention groups in pretest step for anxiety level. Same letters means non-significant differences for anxiety level between groups
Figure 4.
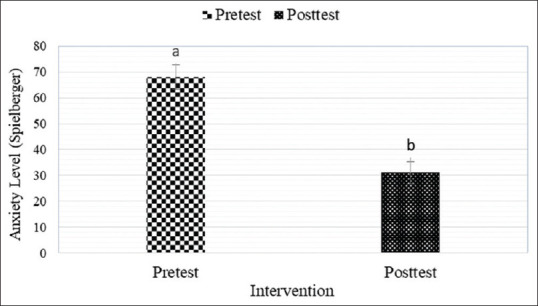
Paired t test between pretest and posttest steps in intervention group for anxiety level. Different letters means significant differences for anxiety level between steps
Figure 2.
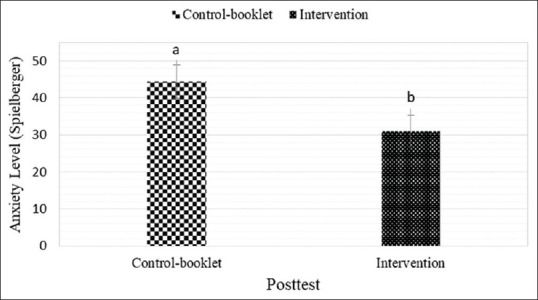
Independent sample t test between control and intervention groups in posttest step for anxiety level. Different letters means significant differences for anxiety level between groups
Figure 3.
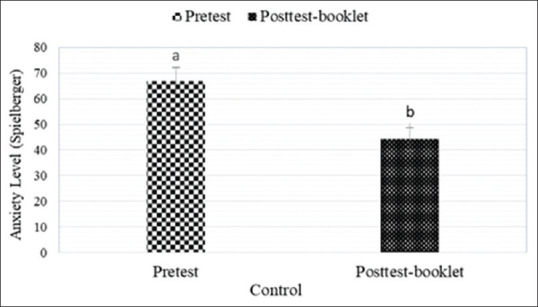
Paired t test between pretest and posttest steps in control group for anxiety level. Different letters means significant differences for anxiety level between steps
Discussion and Conclusion
The study, which measured the effect of tele-nursing on anxiety levels in patients with corona, clarifies that the disease (Covid-19) increased anxiety in most patients and training through lecturing and tele-nursing played a significant role in reducing anxiety. The most appropriate training providers in hospital departments are nurses in these wards, who, in addition to frequently encountering similar patients, have the most time to communicate with them.[15] After detecting anxiety in patients, nurses could take steps to effectively deal with these unwanted conditions in the patients through appropriate and correct training.[16] The results of this study showed that the levels of anxiety of the patients were 67.06 and 68.09 in the control and intervention groups before the intervention, which is higher than the average score of the research tool in both groups. However, after presenting the training booklet to the control group, their anxiety level was reduced to 44.39 and it was 31.01 in the intervention group that received tele-nursing besides the booklet, which is lower than the average score of the research tool in both groups. Moreover, the results of the independent t-test in this study showed a significant statistical difference between the two groups after the intervention. Ghoulami and Esmaeilpour (2018) in a study on the role of tele-nursing in the care of chronic diseases, pointed to the positive effect of tele-nursing on patients with chronic lung problems.[17] Masrat et al. (2011) in their research entitled tele-nursing as a suitable option to improve the process of patient education, stated the positive and successful effect of tele-nursing on training patients with chronic diseases,[12] which confirmed the results of this study. Therefore, tele-nursing is an effective method in reducing the level of anxiety of patients with corona and this method can be used to improve their condition.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient (s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.World Health Organization. Coronavirus disease 2019 (COVID-19) situation report–34. Geneva, Switzerland: World Health Organization; 2020. Available from: https://wwwwhoint/docs/default-source/coronaviruse/situation-reports/20200223-sitrep-34-covid-19pdfsfvrsn=44ff8fd3_2pdf icon . [Google Scholar]
- 2.Tong Z-D, Tang A, Li K-F, Li P, Wang H-L, Yi J-P. Potential presymptomatic transmission of SARS-CoV-2, Zhejiang Province, China, 2020. Emerg Infect Dis. 2020;26:1052–4. doi: 10.3201/eid2605.200198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jernigan JA, Low DE, Helfand RF. Combining clinical and epidemiologic features for early recognition of SARS. Emerg Infect Dis. 2004;10:327–33. doi: 10.3201/eid1002.030741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese center for disease control and prevention external icon. JAMA. 2020 doi: 10.1001/jama.2020.2648. doi: 101001/jama20202648. [DOI] [PubMed] [Google Scholar]
- 5.Dong X, Wang L, Tao Y, Suo X, Li Y, Liu F, et al. Psychometric properties of the anxiety inventory for respiratory disease in patients with COPD in China. Int J Chron Obstruct Pulmon Dis. 2017;12:49–58. doi: 10.2147/COPD.S117626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cassem NH, Bernstein JG. Depressed patients. In: Stern TA, Fricchione GL, Cassen WH, Jellinek MS, Rosenbanm JF, editors. Massachusetts general hospital handbook of general hospital psychiatry. 5th ed. Philadelphia, PA: Mosby/ Elsevier; 2004. pp. 25–68. [Google Scholar]
- 7.Coventry PA. Does pulmonary rehabilitation reduce anxiety and depression in chronic obstructive pulmonary disease? Curr Opin Pulm Med. 2009;15:143–9. doi: 10.1097/MCP.0b013e3283218318. [DOI] [PubMed] [Google Scholar]
- 8.Pietras T, Witusik A, Panek M, Hołub M, Gałecki P, Wujcik R, et al. Anxiety and depression in patients with obstructive diseases. Pol Merkur Lekarski. 2009;26:631–5. [PubMed] [Google Scholar]
- 9.Willgoss TG, Goldbart J, Fatoye F, Yohannes AM. The development and validation of the anxiety inventory for respiratory disease. Chest. 2013;144:1587–96. doi: 10.1378/chest.13-0168. [DOI] [PubMed] [Google Scholar]
- 10.Alipour A, Ghadami A, Alipour Z, Abdolahzadeh H. Preliminary validation of the corona disease anxiety scale (CDAS) in the Iranian sample. Quality J Health Psychol. 2020;8:163–75. [Google Scholar]
- 11.Bajema KL, Oster AM, McGovern OL, Lindstrom S, Stenger MR, Anderson TC, et al. Persons evaluated for 2019 novel coronavirus—United States, January 2020. MMWR Morb Mortal Wkly Rep. 2020;69:166–70. doi: 10.15585/mmwr.mm6906e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Elham M, Samadi N, Mehrnush N, Mohamad R, Zali M. Tele-nursing: The appropriate option for improvement in the process of training patient. Health Care J. 2011;13:47–52. [Google Scholar]
- 13.Darvish A. Medical IT. Tehran: Anna Medicine Publication; 2014. p. 57. [Google Scholar]
- 14.Basampour SH. The effect of preoperative training on the anxiety level of patients undergoing open heart surgery. Payesh J. 2004;3:139–44. [Google Scholar]
- 15.Behrouz M. Spielberger anxiety test norms in Mashhad, MSC Thesis, Assessment and Measurement in Psychology, Allameh Tabatabai University. 1994:32. [Google Scholar]
- 16.Pond E. A patient self-assessment tool for cardiac rehabilitation. Rehabil Nurs J. 1999;14:81–7. doi: 10.1002/j.2048-7940.1989.tb01425.x. [DOI] [PubMed] [Google Scholar]
- 17.Ghoulami-Shilsari F, Esmaeilpour Bandboni M. Tele-Nursing in chronic Disease Care. Jundishapur J Chronic Dis. 2019;8:e84379. [Google Scholar]