

Abstract
Cancer is the leading cause of death among men and women aged 60-79 years. Colorectal cancer is the third most common cancer in males and the second most common in females, with about 0.8 million deaths worldwide per year. Individuals older than 50 years account for 20-50% of colonic adenomas. Several measures have been proposed to decrease colorectal cancer risks, such as an increase in dietary fiber, use of aspirin, and physical activity. Nonsteroidal anti-inflammatory drugs have been proposed as protective agents against the development of colorectal cancer and colorectal adenomas. Aspirin was the first pharmacological agent endorsed by the United States Preventive Services Task Force screening for colorectal cancer chemoprevention. Although studies have shown up to 40% colorectal cancer risk reduction in individuals at average risk, data regarding this benefit are inconsistent. Several recent studies show that prophylactic use of aspirin in elderly subjects may not be beneficial in preventing the occurrence of colorectal cancers. Given the risks associated with aspirin, such as non-fatal and fatal bleeding events, aspirin’s role should be redefined, especially in individuals at risk of bleeding. This review provides a discussion of the recent studies on the role of aspirin use in elderly individuals at risk of colorectal cancer.
Keywords: Aspirin, colorectal cancer, elderly, cancer prevention, chemoprophylaxis
Introduction
Colorectal cancer (CRC) is a neoplasm developing from the colon or/and rectum. It is a global health problem, with more than 1.84 million new cases per year and 0.8 million deaths per year worldwide [1]. The incidence of and mortality from CRC is high in developed regions such as Australia, New Zealand, Europe, Eastern Asia, and North America [1]. This may be partially attributable to better screening practices and better access to health care. A low-fiber diet, low levels of physical activity, and environmental factors may play a role in the high incidence of CRC. The role of various diets and physical activity and the use of non-steroidal anti-inflammatory drugs has been discussed [2,3].
Aspirin use in CRC prevention has been reported in multiple studies in the recent past. Among the general population with an average risk of CRC, the United States Preventive Services Task Force (USPSTF) in 2015 recommended low-dose aspirin for subjects 50-59 years of age, regardless of sex [4]. It is a grade “B” recommendation for individuals with a 10-year atherosclerotic cardiovascular disease risk of 10% or higher, a life expectancy of at least 10 years, and no risk of bleeding (Table 1) [4,5]. For subjects 60-69 years of age with a 10% or higher risk of atherosclerotic cardiovascular disease, the USPSTF recommends an individualized decision (level of recommendation grade C). Potential difficulties associated with identifying candidacy include lack of predetermined endpoints (other than polyp recurrence), a relatively healthy population, drug-related adverse effects and drug-drug interaction, and relationship with comorbidities, which hampers the ability to identify the chemopreventive agents accurately. Recent studies show that the routine use of aspirin for primary prevention of atherosclerotic cardiovascular disease may be associated with a high risk of bleeding. Incidentally, aspirin use did not decrease the risk of cancer or all-cause mortality among patients with cancers (including CRC), especially in the elderly, in recent large trials [6,7].
Table 1.
Society guidelines for aspirin and primary prevention of colorectal cancer

Why focus on the elderly?
There are only limited data on the use of aspirin use for CRC prevention in the elderly. Elderly patients are a subset of the population who need special consideration for multiple reasons: they often have many comorbidities, a high risk of cancers, polypharmacy, often a discrepancy between physiological and chronological age, frailty, complex psychological issues, and a high risk of bleeding and thrombotic episodes [8-10]. The elderly are also at increased risk of gastrointestinal bleeding because of a higher prevalence of diverticula, intake of multiple drugs that affect the coagulation system, and advanced age per se [11]. The dose of antithrombotic agents, including aspirin, is also an important factor in the elderly because of their low glomerular filtration, low body weight and frequent drug-drug interactions [12]. Thus, the use of aspirin could increase gastrointestinal bleeding, interfere with chemotherapy, and potentially increase the risk of non-CRC-related in situ cancers [11,13,14].
This review presents the historical basis of the use of aspirin in the prevention of CRC, the theoretical basis of aspirin’s benefit in the prevention of CRC, and lastly, current data on the efficacy and safety of routine use of aspirin in light of recent studies in the elderly population.
History of aspirin use in cancer prevention
Aspirin (or acetylsalicylic acid) was obtained initially from willow bark. Its use dates back to 400 BC when salicylic tea was used by Hippocrates and was part of the western pharmacopoeia. Willow bark was proposed for the treatment of inflammatory pain and to relieve the pain of childbirth in the 5th century BC [15]. In 1820, salicin was extracted from willow bark, and renamed as salicylic acid. Felix Hoffman, a German scientist in 1897, acetylated the hydroxyl groups of salicylic acid, resulting in acetylsalicylic acid. Two years later, in 1899, Bayer marketed its new drug, ASPIRin (“A” Acetyl, “SPIR” spireae flower) [16]. In 1971 the effect of aspirin in inhibiting the cyclooxygenase (COX) enzyme was described, and this knowledge led to the use of aspirin as a potential chemotherapeutic agent for cancer prevention [17].
Chemoprevention is the use of a chemical agent for the prevention or interruption of events early in the course of a disease. Aspirin has long been proposed as a chemopreventive agent for cardiovascular disease. Predetermined cardiovascular disease endpoints used to determine the efficacy of aspirin have generally been myocardial infarction, cerebrovascular events, and death from cardiovascular disease. However, determining a “surrogate endpoint” for cancer prevention has been a matter of debate. The reduction in polyp or adenoma burden has been considered a significant endpoint in the prevention of CRC. This endpoint led clinicians and investigators to identify chemopreventive therapies such as aspirin and COX inhibitors. However, the challenge in defining the role of these strategies involves a relatively short duration of 10 years and the potential risk of crossover to other studies [18,19].
Mechanism of aspirin anti-cancer effects
The anti-cancer effects of aspirin are thought to be mediated by its COX-dependent and independent mechanisms [20-23]. The cellular effects of aspirin in the prevention of CRC are noted in Table 2.
Table 2.
Mechanism of actions of aspirin in colorectal cancer

COX-dependent mechanisms
A- COX-1-mediated effects: Aspirin is rapidly absorbed in the stomach and upper intestine. It is hydrolyzed by esterases in the gastrointestinal mucosa and liver to form salicylic acid [24]. It enters the portal circulation and comes in contact with platelets for the first time. Levels of aspirin are significantly higher in the portal circulation than in the systemic circulation, because of its rapid clearance and half-life of 15-20 min [25]. While platelets express only COX-1, epithelial cells express both COX-1 and COX-2 enzymes [25]. Since non-nucleated platelets are unable to resynthesize the COX enzymes, exposure of platelets to aspirin, even for a short time, can have an effect that lasts their entire life in the circulation (Fig. 1, Table 2).
Figure 1.
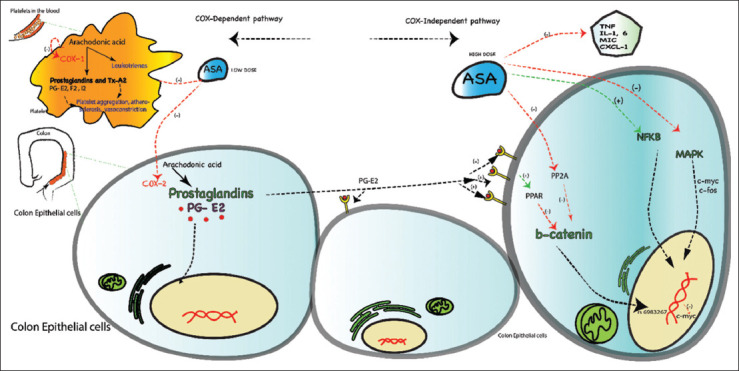
Schematic illustration of aspirin’s role in colorectal cancer prevention Cyclooxygenase (COX) dependent pathway (Left panel): Inhibition of COX-1 in platelets and COX-2 in epithelial cells. Prostaglandins (PGs) are important derivatives of arachidonic acid. Prostaglandins and thromboxane A2 (TXA2) play a role in platelet aggregation, atherosclerosis, and vasoconstriction. Prostaglandin E2 (PGE2) receptor is involved in cell growth, survival, and proliferation. It is an essential target for hydroxyprostaglandin dehydrogenase (HPDG). COX metabolism also involves gene by environment (GxE), single nucleotide polymorphisms (SNP) rs2920421 and rs2965667, and prostaglandin M (PG-M). COX independent pathway (Right panel): WNT β-catenin is an important target for aspirin by inhibition of protein phosphatase 2A (PP2A). It is also inhibited by the peroxisome proliferator activated receptor (PPAR) induced by the paracrine effect of PGE2. Chromosome 8q24 has an important SNP, rs6983267, which lowers the expression of MYC proto-oncogene via WNT signaling. Furthermore, aspirin mediates its effects via a mitogenic activated protein kinase (MAPK) signaling cascade, nuclear factor kappa beta (NF-kB) and resulting apoptosis (via c-myc and c-fos). Aspirin exerts its anti-inflammatory effects by targeting soluble tumor necrosis factor (TNF) receptor 2 and macrophage inhibitory cytokine (MIC). These actions induce a reduction in the generation of cytokines interleukin (IL) -1 and -6, TNF and chemokines
High levels of the drug are needed to inhibit COX-2 in epithelial cells compared to COX-1 in platelets [26]. COX-1 inhibition leads to decreased thromboxane (TXA2) formation, involved in platelet aggregation, atherogenesis and vasoconstriction. Aspirin also inhibits the formation of platelet aggregation inhibitor and vasodilator prostaglandin I2 (PGI2) in the vessel wall. While aspirin inhibits both TXA2 and PGI2, the TXA2 inhibitory effects predominate [27]. COX-1 inhibition by aspirin also inhibits the formation of prostaglandin E2 (PGE2). Suppression of PGE2 also contributes to aspirin’s anti-neoplastic effects in the colon. PGE2 inhibition has been implicated in the aspirin role in colorectal chemoprevention [28].
B- COX-2-mediated effects: In addition to COX-1 inhibition, COX-2 inhibition also contributes to a reduction in colorectal carcinogenesis, especially in humans [29-32]. COX-2-dependent generation of lipoxins and polycyclic aromatic hydrocarbons is responsible for cell proliferation and carcinogenesis [29,32]. COX-2 is induced at sites of inflammation in response to cytokines such as interleukin 1 (IL-1, a and b), IL-6, tumor necrosis factor (TNF), interferon-y and chemokines (CXCL1). These proinflammatory cytokines are elevated in CRC patients. Aspirin-mediated inhibition of C inhibitory cytokine-1, whose levels are elevated in the plasma of CRC OX-2, results in the reduction in these inflammatory cytokines [31].
Similarly, levels of macrophages are reduced by aspirin, conferring a theoretically protective effect against CRC [32]. Aspirin has also been shown to reduce the risk of CRC among individuals with certain single-nucleotide polymorphisms. An example of such polymorphisms includes the rs2965667-AA phenotype located on chromosome 12 [33]. Further, by inhibiting COX-2, aspirin reduces the expression of a wide variety of angiogenic factors, such as vascular endothelial growth factor, endothelin-1, nitric oxide synthase, and fibroblast growth factors. These antiangiogenic effects of aspirin may contribute to its salutary effects against the development of gastrointestinal cancers [34].
Aspirin also exerts its antineoplastic influence via indirect pathways that affect COX metabolism, acting on targets such as hydroxy PG dehydrogenase (HPGD), SLC02A1 (the gene responsible for PG transporter), gene by environment (GxE), single nucleotide polymorphisms (SNP) rs2920421 and rs2965667, and PG-M, all of which are associated with the development of CRC [33,35,36].
COX-independent pathways
Aspirin’s mechanism of action has been elucidated in multiple studies, and inhibition of platelet function and formation of PGs remain the most important among its anti-cancer effects [20]. However, COX-independent effects of aspirin, noted at high concentrations achieved with the intake of doses >300 mg per day, may also contribute to its cancer-limiting effect.
A- Aspirin-induced apoptosis: Apoptosis is critical for the control of colon epithelial cell number. Aspirin induces apoptosis via various mechanisms (Fig. 1) [37]. It modulates the mitogen-activated protein kinase (MAPK) signaling cascade involved in proto-oncogene BRAF mutations. It has been shown to lower the risk of BRAF wild type CRC through epigenetic dysregulation affecting the serrated cancer pathway [38,39]. Aspirin is known to induce nuclear translocation of the transcription factor NF-kB. The repression of NF-kB-driven transcription, irrespective of p53, induces DNA mismatch and halts the repair status [40]. Further, aspirin also induces caspase-dependent externalization of phosphatidylserine in colon cancer cell lines, even before nuclear condensation. These mechanisms, in part or in combination with its COX inhibitory effects, could explain aspirin’s role in cell death by apoptosis.
B- Role of WNT β-catenin signaling axis: WNT β-catenin is a pathway dysregulated in a number of CRCs [41]. This pathway is activated by an extracellular ligand (WNT) on the cell surface receptors, which causes the stabilization of β-catenin and translocation of β-catenin to the nucleus. In the nucleus, it binds to transcriptional factors to form an activated complex responsible for gene expression, cell proliferation, and migration [42]. Reduced levels of β-catenin inhibit cell proliferation and CRC progression. A loss of function of the adenomatous polyposis coli gene leads to abnormal activation of WNT signaling, leading to cytosolic and nuclear accumulation of β-catenin, observed in the majority of CRC cases [43]. Aspirin reduces the pool of cytoplasmic β-catenin in CRC cell lines through its inhibitory effect on protein phosphatase 2A (PP2A) and the resulting ubiquitylation of β-catenin (Fig. 1). PGE-2 also effects β-catenin, in part via the EP2 receptor. PGE2 also increases transcription of peroxisome proliferator-activated receptor (PPAR), which combines with β-catenin to form a complex. This has been associated with the apoptotic resistance of CRC cell lines. Aspirin affects the PPAR pathway by targeting β-catenin and its downstream effects [44,45]. Chromosome 8q24 has an important SNP named rs 6983267, which lowers the expression of MYC proto-oncogene via WNT signaling and reduction in CRC by 17% [46]. Regular use of aspirin altered the risk of CRC expression in individuals with this SNP rs6983267; however, the details differed according to the genotype. Compared to non-users, regular use of aspirin was associated with reduced odds of CRC in GT genotype (odds ratio [OR] 0.61, 95% confidence interval [CI] 0.47-0.79) and in TT genotype (OR 0.52, 95%CI 0.35-0.78), whereas no benefit was noted in GG genotype (OR 0.99, 95%CI 0.70-1.40) [35].
C- Paracrine upregulation of COX enzymes: Paracrine upregulation of PGs is noted in CRC tissue. This is mediated by increased activity of the COX enzyme. Epithelial cells and macrophages in CRC have high COX-2 activity with increased dysplasia and submucosal invasion [47]. It is hypothesized that this increase in COX activity is probably from additional recruitment of platelets from excess inflammation and mucosal injury noted in the tumor tissue [48]. Some of these epithelial cells communicate with platelets in a paracrine fashion. Low-dose aspirin can irreversibly inhibit the COX activity in platelets, interfering with tumorigenesis. In addition, this combined antiplatelet and anti-inflammatory action of aspirin induces inhibition of the tumor growth [47].
D- Modulation of host immune response: Chronic inflammation, combined with modulation of the host immune response, plays a role in CRC progression. As PG synthesis increases at these sites, aspirin reduces the levels of cytokines and overall inflammation [49]. These effects are exerted by targeting multiple cytokines, such as soluble TNF receptor 2, macrophage inhibitory cytokine (MIC), IL-1 and 6, TNF, and chemokines [50]. Among these, aspirin use with high plasma levels of soluble TNF receptor 2 was associated with a lower risk of CRC (relative risk [RR] 0.39, 95%CI 0.41-1.79) [31]. Similarly, higher levels of macrophage inhibitory cytokine 1 were associated with a 93% increased risk of CRC (hazard ratio [HR] 1.93, 95%CI 1.27-2.94), while the use of aspirin reduced the risk in PG-synthase-2-positive patients (RR 0.60, 95%CI 0.41-0.88) [51]. These anti-inflammatory effects may be another mechanism through which aspirin reduces tumor-related inflammation and tumor growth [52].
E- Inhibition of proto-oncogene: CRC in adults is mostly sporadic, and the majority of cases go through classic pathways of adenoma-carcinoma sequence [53]. An alternate pathway involves serrated polyp progression to serrated CRC in the last 5-10 years. This process involves the development of colonic mucosal cell mutations, and epigenetic alterations contributed by tumor-promoting factors from adjacent tissue (gut microbiome) [39]. The time required for this accumulation of mutations and the development of cancer is about 10-15 years. BRAF, a proto-oncogene in the MAPK signaling cascade, is strongly associated with the serrated CRC pathway [36]. Aspirin use was associated with a lower risk of BRAF wild type CRC (HR 0.73, 95%CI 0.64-0.83) [54]. By inhibiting this proto-oncogene, aspirin could potentially interrupt the serrated-carcinoma sequence.
Aspirin chemoprevention trials
In 1988, the Melbourne CRC study first identified that patients with CRC had a decreased use of aspirin-containing medications [55]. This was followed by multiple randomized controlled trials (RCTs) to evaluate the protective role of aspirin. Many subsequent RCTs studied the role of aspirin for CRC prevention. Important questions, however, remain regarding the dose of aspirin, duration of its use, population specificity, follow-up duration and type of aspirin (enteric-coated or not) in relation to its protective value against CRC, particularly in patients aged more than 60 years [19,56].
RCTs involving aspirin for CRC for chemoprevention
The results of some major RCTs on the role of aspirin in CRC prevention are shown in Table 3 [19,57-64]. As shown in Table 4, data related to the efficacy of aspirin for the prevention of CRC in subjects over the age of >60 years appear less robust [6,62,65] (Tables 3,4).
Table 3.
Trials of aspirin in colorectal cancer chemoprevention regardless of age

Table 4.
Aspirin in colorectal cancer chemoprevention in elderly

A- In-favor trials (protective role) of aspirin in CRC: Studies conducted until 2014 showed a protective effect of aspirin against CRC adenomas and cancer incidence and mortality [66,67]. The aspirin doses in the studies ranged from 81-325 mg [68]. Few studies were conducted in patients at high risk of developing CRC (with the history of multiple polyps diagnosed on prior colonoscopy or adenocarcinoma restricted to the mucosa). In 2007, the British Doctor Aspirin Trial and the UK-TIA Aspirin Trial showed that aspirin reduced the incidence of CRC if it was given for 5 years or more in patients with a mean age of 60 years or higher [69]. However, this effect was only seen after a latency of 10 years and was most pronounced 10-14 years after randomization. Analyses of multiple RCTs to assess revealed a chemoprotective effect after 3 years of exposure of aspirin [63]. In multiple RCTs performed to evaluate the protective role of aspirin in cardiovascular disease (Table 5), gastrointestinal and overall cancer risk was noted along with a higher incidence of bleeding [70-76]. In 2017, the incidence of CRC in individuals free of cardiovascular disease was assessed in cohorts with and without low-dose aspirin. It was noted that individuals aged 40-79 years taking low-dose aspirin for a mean period of 5 years had a lower incidence of CRC compared to non-aspirin users. However, this protective effect was not observed in subjects 80-89 years of age [77] (Table 5).
Table 5.
The role of aspirin in cardiovascular disease prevention with reduction of GI cancer and bleeding risks

B- Not-in-favor trials (non-protective role) of aspirin in CRC: A recently published RCT (ASPREE) showed that the use of 81-100 mg of aspirin in adults 70 years or higher (age 65 years and more blacks and Hispanics in the USA cohort) with a mean follow up of 4.7 years showed an increased risk of CRC-related mortality (HR 1.77, 95%CI 1.02-3.06; P<0.05) [6]. The study population in this trial was predominantly Australian (16,703 patients) and had no previous exposure to aspirin. In addition to CRC, non-CRC-related deaths (breast, lung, lung, esophageal, and stomach) were higher in subjects given aspirin. In addition, the risk of death from any cause was 12.7 events per 1000 person-years in the aspirin group and 11.1 events per 1000 person-years in the placebo group (HR 1.14, 95%CI 1.01-1.29). Bleeding was not the primary cause of death in these patients (28 patients died from major hemorrhage among 558 deaths [0.3%]). A systematic review, published in 2019, of multiple published RCTs involving 165,502 participants showed that, compared with control, aspirin was associated with similar rates of cancer and cancer-related deaths, even on secondary analysis restricted to long-term follow-up trials (>5 years). Use of aspirin was associated with a higher risk of major bleeding (RR 1.5, 95%CI 1.33-1.69), intracranial bleeding (RR 1.32, 95%CI 1.12-1.55), and major bleeding (RR 1.52, 95%CI 1.34-1.73) [7].
On the other hand, a study in late 2019 that reported a prostate, lung, colorectal and ovarian cancer screening trial in elderly patients (aged 65 years or above) showed a protective effect, since the use of aspirin 3 times or more per week reduced the risk of CRC (HR 0.71, 95%CI 0.61-0.84; P<0.001) [78]. A similar trend was observed with all-cause mortality, any cancer, and gastrointestinal cancer (HR 0.75, 95%CI 0.66-0.84; P<0.001). The authors performed a subgroup analysis based on body mass index and frequency of aspirin intake (1-3 times intake per month, 1-2 times per week, or more than 3 times per week). Participants who were underweight (body mass index less than 20) did not benefit from aspirin use, while those with higher body mass index (20 kg/m2 or higher) had reduced overall mortality, including CRC mortality [78]. Further, the authors noted the use of ibuprofen (<3 times per week) in the participants. This concomitant use of a non-steroidal anti-inflammatory agent could be a potential confounder in reducing the risk of CRC [78]. This highlights the importance of the duration and dosing of aspirin, frequency of administration, prior exposure to aspirin, and patient characteristics (body mass index and bleeding risks).
These findings suggest a need to explore the role of aspirin in elderly individuals, especially in those above 70 years. Due to advancing age, the incidence of age-adjusted cancer has risen significantly. Whether the initiation of aspirin in these individuals without prior exposure would theoretically increase the risk of cancer needs further study. Recent studies showing a lack of benefit of aspirin in primary prevention suggest a close evaluation of patients’ cardiovascular disease status, age, and risk of overall cancer. Given the trend towards primary prevention with the use of statins, aggressive blood pressure control, decreasing trends of smoking, the risk of cardiovascular diseases in the individuals enrolled in these RCTs have decreased to <10%. In addition, there is also the risk of overestimating the atherosclerotic cardiovascular disease risk in a “real-world” population [79]. This might decrease the protective effects of aspirin in these populations, which could probably explain the results. Furthermore, the risk of bias (survivor, type of indication for aspirin use, reverse causation) needs to be assessed when the results of these studies are interpreted [80]. Lastly, older age and male sex may increase the aspirin-induced risks of bleeding and might affect the results of these RCTs. Some of the ongoing clinical trials designed to determine the chemopreventive role of aspirin in elderly individuals are shown in Table 6 [59,81-83]. As more data emerge from these studies, some of the effects of reduced atherosclerotic cardiovascular disease risks and the role of age in aspirin-induced CRC chemoprevention may become clearer.
Table 6.
Clinical trials investigating the role of aspirin in chemoprevention of colorectal cancer in the elderly as of December 31, 2019

Ongoing trials of aspirin in CRC chemoprevention among the elderly
In response to the ongoing concerns about the effects of aspirin in the elderly population, various clinical trials have been initiated and are currently in different phases. Table 6 provides a list of clinical trials, completion date and dosing of aspirin used in these trials. For instance, aspirin intervention for the reduction in CRC risk (ASPIRED) is a prospective, double-blind, placebo-controlled randomized trial involving 180 participants, which is comparing the effects of low-dose (81 mg) and standard-dose (325 mg) aspirin on CRC [59]. Similarly, an observational study involving 1005 participants in Italy was initiated in 2019 to evaluate patients’ preferences and their perspectives on the benefits and risks of low-dose aspirin for CRC prevention [81]. A randomized clinical trial in Spain of 60 participants is underway to assess the dosing and mechanisms of aspirin-induced chemoprevention in CRC. This study is currently in phase 2. Also in phase 2 is a clinical trial in the United States involving 90 participants to evaluate the role of intermittent dosing of aspirin for CRC prevention. It is estimated that this study could be completed by July 1, 2021 [83]. These clinical trials might shed light on the mechanism of aspirin-induced chemoprotection against colorectal carcinogenesis, especially in the elderly.
Clinical message
Aspirin is one of the most commonly prescribed pharmacological agent in the United States and beyond for a number of indications. Prophylactic use of aspirin for chemoprevention of CRC has been recommended by preventive task force for non-elderly average-risk individuals. However, data in elderly individuals have been inconsistent, with recent trials showing aspirin may not be beneficial, and the possibility of harm has been noted, with an increased risk of fatal and non-fatal bleeding events. Given these findings, prescribers should actively participate in educating their patients about the results of these recent studies. Furthermore, as our understanding of aspirin-induced chemoprevention in the elderly evolves, indications for this agent could potentially change in the future.
Concluding remarks
Chemoprevention of CRC with aspirin is dependent on age, risk factors for CRC, and the presence of comorbidities. Inhibition of the COX pathway is probably the most important mechanism by which aspirin exerts its preventative effect against CRC. Though there is some evidence of a protective effect of aspirin in chemoprevention against CRC from earlier studies, recent studies show little if any benefit, suggesting that the age and cardiovascular disease risk profile of the enrolled population play a role [6,7]. Although aspirin has been widely studied as a chemopreventive agent against CRC, gastrointestinal and renal toxicity in the long term preclude its widespread use [14]. Identifying the risk status of an individual (age, sex, mutations, environmental factors, baseline cardiovascular risks, risks of major gastrointestinal bleeding) [84] with an assessment of cumulative benefits (cardiovascular disease prevention) provides the best strategy for the use of aspirin to prevent CRC. As data emerge from ongoing trials, the CRC-preventing effect of aspirin may become evident, especially in the elderly population.
Biography
University of Arkansas for Medical Sciences, Little Rock, AR; The Wright Center for Graduate Medical Education, Scranton, PA; Central Arkansas Veterans Healthcare System and the University of Arkansas for Medical Sciences, Little Rock, AR, USA
Footnotes
Conflict of Interest: None
References
- 1.WHO. Colorectal Cancer, GLOBOCAN. 2018 [Google Scholar]
- 2.Cross AJ, Ferrucci LM, Risch A, et al. A large prospective study of meat consumption and colorectal cancer risk: an investigation of potential mechanisms underlying this association. Cancer Res. 2010;70:2406–2414. doi: 10.1158/0008-5472.CAN-09-3929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chan DS, Lau R, Aune D, et al. Red and processed meat and colorectal cancer incidence:meta-analysis of prospective studies. PLoS One. 2011;6:e20456. doi: 10.1371/journal.pone.0020456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bibbins-Domingo K U.S. Preventive Services Task Force. Aspirin use for the primary prevention of cardiovascular disease and colorectal cancer:U.S. Preventive services task force recommendation statement. Ann Intern Med. 2016;164:836–845. doi: 10.7326/M16-0577. [DOI] [PubMed] [Google Scholar]
- 5.John JS. Screening benefit - Clinical Guidelines Network, Australia 2017. [Accessed 27 October 2020]. Available from: https://wiki.cancer.org.au/australia/Clinical_question:Population_screening_in_colorectal_cancer .
- 6.McNeil JJ, Nelson MR, Woods RL, et al. ASPREE Investigator Group. Effect of aspirin on all-cause mortality in the healthy elderly. N Engl J Med. 2018;379:1519–1528. doi: 10.1056/NEJMoa1803955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abdelaziz HK, Saad M, Pothineni NVK, et al. Aspirin for primary prevention of cardiovascular events. J Am Coll Cardiol. 2019;73:2915–2929. doi: 10.1016/j.jacc.2019.03.501. [DOI] [PubMed] [Google Scholar]
- 8.Farrell JJ, Friedman LS. Gastrointestinal bleeding in the elderly. Gastroenterol Clin North Am. 2001;30:377–407. doi: 10.1016/s0889-8553(05)70187-4. [DOI] [PubMed] [Google Scholar]
- 9.Millan M, Merino S, Caro A, Feliu F, Escuder J, Francesch T. Treatment of colorectal cancer in the elderly. World J Gastrointest Oncol. 2015;7:204–220. doi: 10.4251/wjgo.v7.i10.204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Leiss W, Méan M, Limacher A, et al. Polypharmacy is associated with an increased risk of bleeding in elderly patients with venous thromboembolism. J Gen Intern Med. 2015;30:17–24. doi: 10.1007/s11606-014-2993-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lenti MV, Pasina L, Cococcia S, et al. REPOSI Investigators. Mortality rate and risk factors for gastrointestinal bleeding in elderly patients. Eur J Intern Med. 2019;61:54–61. doi: 10.1016/j.ejim.2018.11.003. [DOI] [PubMed] [Google Scholar]
- 12.Capodanno D, Angiolillo DJ. Antithrombotic therapy in the elderly. J Am Coll Cardiol. 2010;56:1683–1692. doi: 10.1016/j.jacc.2010.04.063. [DOI] [PubMed] [Google Scholar]
- 13.Hurria A, Lichtman SM. Pharmacokinetics of chemotherapy in the older patient. Cancer Control. 2007;14:32–43. doi: 10.1177/107327480701400105. [DOI] [PubMed] [Google Scholar]
- 14.Aaldriks AA, van der Geest LG, Giltay EJ, et al. Frailty and malnutrition predictive of mortality risk in older patients with advanced colorectal cancer receiving chemotherapy. J Geriatr Oncol. 2013;4:218–226. doi: 10.1016/j.jgo.2013.04.001. [DOI] [PubMed] [Google Scholar]
- 15.Jeffreys D. Aspirin:The Remarkable Story of a Wonder Drug. 2019 [Google Scholar]
- 16.Mann J. Oxford: Oxford University Press; 2019. Murder, Magic and Medicine. [Google Scholar]
- 17.Richmond C. Sir John Vane. BMJ. 2004;329:1406. [Google Scholar]
- 18.Stürmer T, Glynn RJ, Lee IM, Manson JE, Buring JE, Hennekens CH. Aspirin use and colorectal cancer:post-trial follow-up data from the Physicians'Health Study. Ann Intern Med. 1998;128:713–720. doi: 10.7326/0003-4819-128-9-199805010-00003. [DOI] [PubMed] [Google Scholar]
- 19.Rothwell PM, Wilson M, Elwin CE, et al. Long-term effect of aspirin on colorectal cancer incidence and mortality:20-year follow-up of five randomised trials. Lancet. 2010;376:1741–1750. doi: 10.1016/S0140-6736(10)61543-7. [DOI] [PubMed] [Google Scholar]
- 20.Ranger GS. Current concepts in colorectal cancer prevention with cyclooxygenase inhibitors. Anticancer Res. 2014;34:6277–6282. [PubMed] [Google Scholar]
- 21.Patrignani P, Patrono C. Cyclooxygenase inhibitors:From pharmacology to clinical read-outs. Biochim Biophys Acta. 2015;1851:422–432. doi: 10.1016/j.bbalip.2014.09.016. [DOI] [PubMed] [Google Scholar]
- 22.Schrör K. Pharmacology and cellular/molecular mechanisms of action of aspirin and non-aspirin NSAIDs in colorectal cancer. Best Pract Res Clin Gastroenterol. 2011;25:473–484. doi: 10.1016/j.bpg.2011.10.016. [DOI] [PubMed] [Google Scholar]
- 23.Chan AT, Ogino S, Fuchs CS. Aspirin and the risk of colorectal cancer in relation to the expression of COX-2. N Engl J Med. 2007;356:2131–2142. doi: 10.1056/NEJMoa067208. [DOI] [PubMed] [Google Scholar]
- 24.Pedersen AK, FitzGerald GA. Dose-related kinetics of aspirin. Presystemic acetylation of platelet cyclooxygenase. N Engl J Med. 1984;311:1206–1211. doi: 10.1056/NEJM198411083111902. [DOI] [PubMed] [Google Scholar]
- 25.Thun MJ, Jacobs EJ, Patrono C. The role of aspirin in cancer prevention. Nat Rev Clin Oncol. 2012;9:259–267. doi: 10.1038/nrclinonc.2011.199. [DOI] [PubMed] [Google Scholar]
- 26.Loll PJ, Picot D, Garavito RM. The structural basis of aspirin activity inferred from the crystal structure of inactivated prostaglandin H2 synthase. Nat Struct Biol. 1995;2:637–643. doi: 10.1038/nsb0895-637. [DOI] [PubMed] [Google Scholar]
- 27.Patrono C, García Rodríguez LA, Landolfi R, Baigent C. Low-dose aspirin for the prevention of atherothrombosis. N Engl J Med. 2005;353:2373–2383. doi: 10.1056/NEJMra052717. [DOI] [PubMed] [Google Scholar]
- 28.Ruffin MT, 4th, Krishnan K, Rock CL, et al. Suppression of human colorectal mucosal prostaglandins:determining the lowest effective aspirin dose. J Natl Cancer Inst. 1997;89:1152–1160. doi: 10.1093/jnci/89.15.1152. [DOI] [PubMed] [Google Scholar]
- 29.Clària J, Lee MH, Serhan CN. Aspirin-triggered lipoxins (15-epi-LX) are generated by the human lung adenocarcinoma cell line (A549)-neutrophil interactions and are potent inhibitors of cell proliferation. Mol Med. 1996;2:583–596. [PMC free article] [PubMed] [Google Scholar]
- 30.Craven PA, DeRubertis FR. Effects of aspirin on 1,2-dimethylhydrazine-induced colonic carcinogenesis. Carcinogenesis. 1992;13:541–546. doi: 10.1093/carcin/13.4.541. [DOI] [PubMed] [Google Scholar]
- 31.Chan AT, Ogino S, Giovannucci EL, Fuchs CS. Inflammatory markers are associated with risk of colorectal cancer and chemopreventive response to anti-inflammatory drugs. Gastroenterology. 2011;140:799–808. doi: 10.1053/j.gastro.2010.11.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mehta RS, Song M, Bezawada N, et al. A prospective study of macrophage inhibitory cytokine-1 (MIC-1/GDF15) and risk of colorectal cancer. J Natl Cancer Inst. 2014;106:dju016. doi: 10.1093/jnci/dju016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Nan H, Hutter CM, Lin Y, et al. GECCO. Association of aspirin and NSAID use with risk of colorectal cancer according to genetic variants. JAMA. 2015;313:1133–1142. doi: 10.1001/jama.2015.1815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Tsujii M, Kawano S, Tsuji S, Sawaoka H, Hori M, DuBois RN. Cyclooxygenase regulates angiogenesis induced by colon cancer cells. Cell. 1998;93:705–716. doi: 10.1016/s0092-8674(00)81433-6. [DOI] [PubMed] [Google Scholar]
- 35.Nan H, Morikawa T, Suuriniemi M, et al. Aspirin use 8q24 single nucleotide polymorphism rs6983267, and colorectal cancer according to CTNNB1 alterations. J Natl Cancer Inst. 2013;105:1852–1861. doi: 10.1093/jnci/djt331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Nishihara R, Lochhead P, Kuchiba A, et al. Aspirin use and risk of colorectal cancer according to BRAF mutation status. JAMA. 2013;309:2563–2571. doi: 10.1001/jama.2013.6599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Castaño E, Dalmau M, Barragán M, Pueyo G, Bartrons R, Gil J. Aspirin induces cell death and caspase-dependent phosphatidylserine externalization in HT-29 human colon adenocarcinoma cells. Br J Cancer. 1999;81:294–299. doi: 10.1038/sj.bjc.6690690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kedrin D, Gala MK. Genetics of the serrated pathway to colorectal cancer. Clin Transl Gastroenterol. 2015;6:e84. doi: 10.1038/ctg.2015.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.IJspeert JE, Vermeulen L, Meijer GA, Dekker E. Serrated neoplasia-role in colorectal carcinogenesis and clinical implications. Nat Rev Gastroenterol Hepatol. 2015;12:401–409. doi: 10.1038/nrgastro.2015.73. [DOI] [PubMed] [Google Scholar]
- 40.Din FV, Stark LA, Dunlop MG. Aspirin-induced nuclear translocation of NFkappaB and apoptosis in colorectal cancer is independent of p53 status and DNA mismatch repair proficiency. Br J Cancer. 2005;92:1137–1143. doi: 10.1038/sj.bjc.6602455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell. 1990;61:759–767. doi: 10.1016/0092-8674(90)90186-i. [DOI] [PubMed] [Google Scholar]
- 42.MacDonald BT, Tamai K, He X. Wnt/beta-catenin Signaling:Components Mechanisms, and Diseases. Dev Cell. 2009;17:9–26. doi: 10.1016/j.devcel.2009.06.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Fearon ER. Molecular genetics of colorectal cancer. Annu Rev Pathol. 2011;6:479–507. doi: 10.1146/annurev-pathol-011110-130235. [DOI] [PubMed] [Google Scholar]
- 44.He TC, Chan TA, Vogelstein B, Kinzler KW. PPARdelta is an APC-regulated target of nonsteroidal anti-inflammatory drugs. Cell. 1999;99:335–345. doi: 10.1016/s0092-8674(00)81664-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Gupta RA, Wang D, Katkuri S, Wang H, Dey SK, DuBois RN. Activation of nuclear hormone receptor peroxisome proliferator-activated receptor-delta accelerates intestinal adenoma growth. Nat Med. 2004;10:245–247. doi: 10.1038/nm993. [DOI] [PubMed] [Google Scholar]
- 46.Pomerantz MM, Ahmadiyeh N, Jia L, et al. The 8q24 cancer risk variant rs6983267 shows long-range interaction with MYC in colorectal cancer. Nat Genet. 2009;41:882–884. doi: 10.1038/ng.403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hull MA, Cuthbert RJ, Ko CWS, et al. Paracrine cyclooxygenase-2 activity by macrophages drives colorectal adenoma progression in the ApcMin/+ mouse model of intestinal tumorigenesis. Sci Rep. 2017;7:6074. doi: 10.1038/s41598-017-06253-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dixon DA, Tolley ND, Bemis-Standoli K, et al. Expression of COX-2 in platelet-monocyte interactions occurs via combinatorial regulation involving adhesion and cytokine signaling. J Clin Invest. 2006;116:2727–2738. doi: 10.1172/JCI27209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Wang D, Dubois RN. The role of COX-2 in intestinal inflammation and colorectal cancer. Oncogene. 2010;29:781–788. doi: 10.1038/onc.2009.421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Montrose DC, Nakanishi M, Murphy RC, et al. The role of PGE2 in intestinal inflammation and tumorigenesis. Prostaglandins Other Lipid Mediat. 2015;116-117:26–36. doi: 10.1016/j.prostaglandins.2014.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Mehta RS, Song M, Bezawada N, et al. A prospective study of macrophage inhibitory cytokine-1 (MIC-1/GDF15) and risk of colorectal cancer. J Natl Cancer Inst. 2014;106:dju016. doi: 10.1093/jnci/dju016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Klampfer L. Cytokines, inflammation and colon cancer. Curr Cancer Drug Targets. 2011;11:451–464. doi: 10.2174/156800911795538066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Vogelstein B, Fearon ER, Hamilton SR, et al. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988;319:525–532. doi: 10.1056/NEJM198809013190901. [DOI] [PubMed] [Google Scholar]
- 54.Bettington M, Walker N, Clouston A, Brown I, Leggett B, Whitehall V. The serrated pathway to colorectal carcinoma:current concepts and challenges. Histopathology. 2013;62:367–386. doi: 10.1111/his.12055. [DOI] [PubMed] [Google Scholar]
- 55.Kune GA, Kune S, Watson LF. Colorectal cancer risk chronic illnesses operations, and medications:case control results from the Melbourne Colorectal Cancer Study. Cancer Res. 1988;48:4399–4404. [PubMed] [Google Scholar]
- 56.Chan AT, Arber N, Burn J, et al. Aspirin in the chemoprevention of colorectal neoplasia:an overview. Cancer Prev Res (Phila) 2012;5:164–178. doi: 10.1158/1940-6207.CAPR-11-0391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Baron JA, Cole BF, Sandler RS, et al. A randomized trial of aspirin to prevent colorectal adenomas. N Engl J Med. 2003;348:891–899. doi: 10.1056/NEJMoa021735. [DOI] [PubMed] [Google Scholar]
- 58.Benamouzig R, Deyra J, Martin A, et al. Daily soluble aspirin and prevention of colorectal adenoma recurrence:one-year results of the APACC trial. Gastroenterology. 2003;125:328–336. doi: 10.1016/s0016-5085(03)00887-4. [DOI] [PubMed] [Google Scholar]
- 59.Drew DA, Chin SM, Gilpin KK, et al. ASPirin Intervention for the REDuction of colorectal cancer risk (ASPIRED):a study protocol for a randomized controlled trial. Trials. 2017;18:50. doi: 10.1186/s13063-016-1744-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Cook NR, Lee IM, Zhang SM, Moorthy MV, Buring JE. Alternate-day, low-dose aspirin and cancer risk:long-term observational follow-up of a randomized trial. Ann Intern Med. 2013;159:77–85. doi: 10.7326/0003-4819-159-2-201307160-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Ishikawa H, Mutoh M, Suzuki S, et al. The preventive effects of low-dose enteric-coated aspirin tablets on the development of colorectal tumours in Asian patients:a randomised trial. Gut. 2014;63:1755–1759. doi: 10.1136/gutjnl-2013-305827. [DOI] [PubMed] [Google Scholar]
- 62.Logan RF, Grainge MJ, Shepherd VC, Armitage NC, Muir KR ukCAP Trial Group. Aspirin and folic acid for the prevention of recurrent colorectal adenomas. Gastroenterology. 2008;134:29–38. doi: 10.1053/j.gastro.2007.10.014. [DOI] [PubMed] [Google Scholar]
- 63.Rothwell PM, Price JF, Fowkes FG, et al. Short-term effects of daily aspirin on cancer incidence mortality, and non-vascular death: analysis of the time course of risks and benefits in 51 randomised controlled trials. Lancet. 2012;379:1602–1612. doi: 10.1016/S0140-6736(11)61720-0. [DOI] [PubMed] [Google Scholar]
- 64.Sandler RS, Halabi S, Baron JA, et al. A randomized trial of aspirin to prevent colorectal adenomas in patients with previous colorectal cancer. N Engl J Med. 2003;348:883–890. doi: 10.1056/NEJMoa021633. [DOI] [PubMed] [Google Scholar]
- 65.Jacobs EJ, Thun MJ, Bain EB, Rodriguez C, Henley SJ, Calle EE. A large cohort study of long-term daily use of adult-strength aspirin and cancer incidence. J Natl Cancer Inst. 2007;99:608–615. doi: 10.1093/jnci/djk132. [DOI] [PubMed] [Google Scholar]
- 66.Garcia Rodriguez García Rodríguez LA, Soriano-Gabarró M, Bromley S, Lanas A, Cea Soriano L. New use of low-dose aspirin and risk of colorectal cancer by stage at diagnosis:a nested case-control study in UK general practice. BMC Cancer. 2017;17:637. doi: 10.1186/s12885-017-3594-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Cea Soriano L, Soriano-Gabarró M, García Rodríguez LA. The protective effect of low-dose aspirin against colorectal cancer is unlikely explained by selection bias:results from three different study designs in clinical practice. PLoS One. 2016;11:e0159179. doi: 10.1371/journal.pone.0159179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Rothwell PM, Cook NR, Gaziano JM, et al. Effects of aspirin on risks of vascular events and cancer according to bodyweight and dose:analysis of individual patient data from randomised trials. Lancet. 2018;392:387–399. doi: 10.1016/S0140-6736(18)31133-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Flossmann E, Rothwell PM British Doctors Aspirin Trial and the UK-TIA Aspirin Trial. Effect of aspirin on long-term risk of colorectal cancer:consistent evidence from randomised and observational studies. Lancet. 2007;369:1603–1613. doi: 10.1016/S0140-6736(07)60747-8. [DOI] [PubMed] [Google Scholar]
- 70.Gaziano JM, Brotons C, Coppolecchia R, et al. ARRIVE Executive Committee. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE):a randomised double-blind, placebo-controlled trial. Lancet. 2018;392:1036–1046. doi: 10.1016/S0140-6736(18)31924-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Bowman L, Mafham M, Wallendszus K, et al. ASCEND Study Collaborative Group. Effects of aspirin for primary prevention in persons with diabetes mellitus. N Engl J Med. 2018;379:1529–1539. doi: 10.1056/NEJMoa1804988. [DOI] [PubMed] [Google Scholar]
- 72.Fowkes FG, Price JF, Stewart MC, et al. Aspirin for Asymptomatic Atherosclerosis Trialists. Aspirin for prevention of cardiovascular events in a general population screened for a low ankle brachial index:a randomized controlled trial. JAMA. 2010;303:841–848. doi: 10.1001/jama.2010.221. [DOI] [PubMed] [Google Scholar]
- 73.Belch J, MacCuish A, Campbell I, et al. Royal College of Physicians Edinburgh. The prevention of progression of arterial disease and diabetes (POPADAD) trial:factorial randomised placebo controlled trial of aspirin and antioxidants in patients with diabetes and asymptomatic peripheral arterial disease. BMJ. 2008;337:a1840. doi: 10.1136/bmj.a1840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.de G, aetano G Collaborative Group of the Primary Prevention Project. Low-dose aspirin and vitamin E in people at cardiovascular risk:a randomised trial in general practice. Lancet. 2001;357:89–95. doi: 10.1016/s0140-6736(00)03539-x. [DOI] [PubMed] [Google Scholar]
- 75.Hansson L, Zanchetti A, Carruthers SG, et al. HOT Study Group. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension:principal results of the Hypertension Optimal Treatment (HOT) randomised trial. Lancet. 1998;351:1755–1762. doi: 10.1016/s0140-6736(98)04311-6. [DOI] [PubMed] [Google Scholar]
- 76.Peto R, Gray R, Collins R, et al. Randomised trial of prophylactic daily aspirin in British male doctors. Br Med J (Clin Res Ed) 1988;296:313–316. doi: 10.1136/bmj.296.6618.313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Cea Soriano L, Soriano-Gabarró M, García Rodríguez LA. Incidence of colorectal cancer in new users and non-users of low-dose aspirin without existing cardiovascular disease:A cohort study using The Health Improvement Network. Int J Cardiol. 2017;248:376–381. doi: 10.1016/j.ijcard.2017.06.052. [DOI] [PubMed] [Google Scholar]
- 78.Loomans-Kropp HA, Pinsky P, Cao Y, et al. Association of aspirin use with mortality risk among older adult participants in the prostate lung, colorectal and ovarian cancer screening trial. JAMA Netw Open. 2019;2:e1916729. doi: 10.1001/jamanetworkopen.2019.16729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Rana JS, Tabada GH, Solomon MD, et al. Accuracy of the atherosclerotic cardiovascular risk equation in a large contemporary, multiethnic population. J Am Coll Cardiol. 2016;67:2118–2130. doi: 10.1016/j.jacc.2016.02.055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Frouws MA, van Herk-Sukel MPP, Maas HA, et al. The mortality reducing effect of aspirin in colorectal cancer patients:Interpreting the evidence. Cancer Treat Rev. 2017;55:120–127. doi: 10.1016/j.ctrv.2016.12.008. [DOI] [PubMed] [Google Scholar]
- 81.Study to evaluate how patients regard the benefits and risks of low-dose aspirin for the prevention of heart and blood vessels disease and for the prevention of cancer of the colon and rectum - full text view - ClinicalTrials.gov. 2019. [Accessed 27 October 2020]. Available from: https://clinicaltrials.gov/ct2/show/NCT03603366 .
- 82.Assessment of direct biomarkers of aspirin action to develop a precision chemoprevention therapy of colorectal cancer - full text view - ClinicalTrials.gov. 2019. [Accessed 27 October 2020]. Available from: https://clinicaltrials.gov/ct2/show/NCT03957902 .
- 83.Alber KM, Murff H, Ness R, et al. Evaluating intermittent dosing of aspirin for colorectal cancer prevention. J Clin Oncol. 2018;36(15_suppl):TPS1594. [Google Scholar]
- 84.Lanas A, Polo-Tomás M, Casado-Arroyo R. The aspirin cardiovascular/gastrointestinal risk calculator--a tool to aid clinicians in practice. Aliment Pharmacol Ther. 2013;37:738–748. doi: 10.1111/apt.12240. [DOI] [PubMed] [Google Scholar]
- 85.Clinical practice guidelines for the prevention, early detection and management of colorectal cancer - Clinical Guidelines Wiki. 2019. [Accessed 27 October 2020]. Available from: https://wiki.cancer.org.au/australia/Guidelines:Colorectal_cancer .