

Abstract
Tislelizumab, an anti‐programmed death protein‐1 (PD‐1) monoclonal antibody, was engineered to minimize binding to the FcγR on macrophages to abrogate antibody‐dependent phagocytosis, a mechanism of T‐cell clearance and potential resistance to anti‐PD‐1 therapy. This single‐arm phase 2 trial (NCT04004221/CTR20170071) assessed the safety, tolerability, and efficacy of tislelizumab in patients with PD‐L1‐positive urothelial carcinoma who progressed during/following platinum‐containing therapy and had no prior PD‐(L)1 inhibitor treatment. Patients were considered PD‐L1 positive if ≥ 25% of tumor/immune cells expressed PD‐L1 when using the VENTANA™ PD‐L1 (SP263) assay. The primary endpoint was objective response rate by independent review committee. As of September 16, 2019, 113 patients had a median study follow‐up time of 9.4 mo. Most patients (76%) had visceral metastases, including 24% with liver and 23% with bone metastases. Among 104 efficacy‐evaluable patients, confirmed objective response rate was 24% (95% confidence interval, 16, 33), including 10 complete and 15 partial responses. Median duration of response was not reached. Among 25 responders, 17/25 (68%) had ongoing responses. Median progression‐free survival and overall survival times were 2.1 and 9.8 mo, respectively. The most common treatment‐related adverse events were anemia (27%) and pyrexia (19%). Anemia (7%) and hyponatremia (5%) were the only grade 3‐4 treatment‐related adverse events and occurred in ≥ 5% of patients. Three investigator‐assessed deaths were considered to be possibly related to study treatment (hepatic failure, n = 2; respiratory arrest, n = 1). Tislelizumab demonstrated meaningful clinical benefits in patients with previously treated locally advanced or metastatic PD‐L1‐positive urothelial carcinoma and had a manageable safety profile.
Keywords: Asian population, immunotherapy, programed death protein‐1, tislelizumab, urothelial carcinoma
Tislelizumab is a unique anti‐PD‐1 antibody that was engineered specifically to minimize FcγR binding in order to limit antibody‐dependent phagocytosis, a potential mechanism of resistance to anti‐PD‐1 therapy. In the current study, tislelizumab demonstrated clinically meaningful antitumor activity in patients with previously treated locally advanced or metastatic PD‐L1‐positive urothelial carcinoma and had a manageable safety profile with no new safety signals compared with other anti‐PD‐L1/PD‐1 therapies. A phase 3 study of tislelizumab as treatment for urothelial carcinoma (NCT03967977) is currently ongoing and is recruiting patients.

Abbreviations
- AE
adverse event
- CI
confidence interval
- CR
complete response
- DoR
duration of response
- IC
immune cell
- irAE
immune‐related adverse event
- IRC
independent review committee
- ORR
objective response rate
- OS
overall survival
- PD‐1
programmed death protein‐1
- PD‐L1−
PD‐L1 negative
- PD‐L1
programmed death ligand 1
- PD‐L1+
PD‐L1 positive
- PFS
progression‐free survival
- PR
partial response
- Q3W
every 3 wk
- TC
tumor cell
- TRAE
treatment‐related adverse event
- UC
urothelial carcinoma
1. INTRODUCTION
The 5‐y survival rate for all patients diagnosed with bladder cancer is 77%, but falls to 36% for those with disease that spreads to regional lymph nodes and to <5% for those with distant metastases. 1 Until recently, initial treatments for patients with metastatic UC have been limited to platinum‐based chemotherapy. 2 Median OS was reported as between 14.1 and 15.5 mo for patients who received cisplatin‐containing regimens 3 , 4 and 13.8 mo for patients who received carboplatin‐containing regimens. 3 For patients ineligible for cisplatin‐containing regimens, median survival was only 8‐9 mo with carboplatin‐based combination chemotherapy. 5 The clinical benefit of salvage chemotherapy with taxanes or vinflunine is low, resulting in a median survival of 6‐8 mo. 6
Dysregulation of the programmed cell death protein‐1/programmed death ligand 1 (PD‐1/PD‐L1) axis can allow cancer cells to evade the immune system 7 , 8 and PD‐L1 overexpression by tumors is associated with poor outcomes for patients with melanoma, ovarian cancer, and lung cancers. 9 Antibodies against PD‐1/PD‐L1 have emerged as first‐line treatment options for patients with UC, as well as for patients who have progressed during or after platinum chemotherapy. For approved anti‐PD‐1/PD‐L1 therapies, median OS was 7.9 mo to 13.7 mo with ORRs of approximately 15‐30% in the second‐line setting; lower response rates were seen in patients with visceral metastases. 10 Because PD‐1/PD‐L1 expression on tumors and ICs is correlated with response to anti‐PD‐1/PD‐L1 therapy in several tumor types, 11 including UC, 12 the current study selected patients who had high PD‐L1 expression to potentially achieve greater clinical benefit. However, additional clinical data are needed to demonstrate the role of PD‐L1 as a predictive biomarker in UC. 12
Tislelizumab, a humanized monoclonal antibody with high affinity and specificity for PD‐1, was engineered to minimize binding to Fcγ receptors on macrophages in order to abrogate antibody‐dependent cellular phagocytosis, a mechanism of T‐cell clearance and potential resistance to anti‐PD‐1 therapy. 7 , 13 Tislelizumab mainly binds to the front β‐sheet face, which comprises the primary interface for PD‐L1 binding, without involvement of the flexible loops of PD‐1. 14 This binding mode of tislelizumab differs from that of nivolumab or pembrolizumab and may contribute to its higher affinity and approximately 100‐fold and 50‐fold slower dissociation rates, respectively. 14 , 15 , 16
Data from 2 phase 1 studies suggested that single‐agent tislelizumab was generally well tolerated and demonstrated preliminary antitumor activity in patients with advanced solid tumors, including UC. 17 , 18 , 19 , 20 In the global, phase 1A/1B first‐in‐human study (BGB‐A317‐001; NCT02407990), tislelizumab treatment across multiple tumor types resulted in an ORR of 13%. 19 Of the 17 evaluable patients with UC treated with tislelizumab 200 mg Q3W in the phase 1B dose‐expansion phase, an ORR of 29% was observed. Clinical responses were observed in both PD‐L1‐positive (PD‐L1+) and PD‐L1‐negative (PD‐L1−)/unknown UC patients; with ORRs of 24% for patients with PD‐L1+ UC and 21% for those with PD‐L1−/unknown tumors. 21 Similar results were observed in an open‐label phase 1/2 study conducted in China (BGB‐A317‐102; NCT04068519), which found that treatment with tislelizumab resulted in an ORR of 18% across all tumor types. 20 Among patients previously treated with UC (n = 22) in the phase 2 portion, the confirmed ORR was 14% and responses were observed regardless of PD‐L1 status. 19 , 20
This ongoing phase 2 clinical trial (CTR20170071), conducted in China and Korea, assessed the safety, tolerability, and efficacy of tislelizumab 200 mg administered intravenously Q3W in patients with locally advanced or metastatic PD‐L1+ UC who progressed during or following platinum‐containing therapy. Although tislelizumab has demonstrated clinical response in PD‐L1+ and PD‐L1−/unknown patients, this study enrolled a PD‐L1‐enriched population to potentially achieve greater clinical benefit.
2. MATERIALS AND METHODS
2.1. Study design and patient population
In this single‐arm, multicenter, phase 2 study, patients aged ≥ 18 y, with histologically or cytologically documented locally advanced or metastatic UC with at least 1 measurable lesion and an Eastern Cooperative Oncology Group (ECOG) performance score of ≤ 1 were eligible for enrollment. Patients could have received platinum‐containing therapy, but were ineligible if they received prior PD‐1/PD‐L1 inhibitor therapy or more than 2 prior lines of systemic therapy for metastatic UC.
This study was performed in accordance with the ethical principles of the Declaration of Helsinki, Good Clinical Practice guidelines, and the principles of informed consent. Written informed consent was obtained from each patient prior to screening. The protocol was reviewed and approved by an independent ethics committee at each study site prior to initiation.
2.2. Study assessments
Radiological assessment of tumor responses was performed every 9 wk and assessed by IRC based on Response Evaluation Criteria in Solid Tumors (RECIST) v1.1, 22 and by the investigators based on RECIST v1.1 and immune‐related RECIST. Efficacy sensitivity analysis was performed on patients with at least 1 post‐baseline tumor assessment. AEs were assessed per National Cancer Institute‐Common Terminology Criteria for Adverse Events v4.03.
During screening, archival tissue/fresh biopsies were tested by a central laboratory using the VENTANA PD‐L1 (SP263) immunohistochemistry assay. 23 Patients were considered PD‐L1+ if ICs involved > 1% of the tumor area and ≥ 25% of TCs or ICs had PD‐L1 expression; or if ICs involved ≤ 1% of the tumor area and ≥ 25% of TCs or 100% of ICs expressed PD‐L1. Blood and tissue (archival and fresh) samples were collected for assessments of tislelizumab pharmacokinetics, anti‐drug antibody levels, and potential prognostic biomarkers.
2.3. Study endpoints and statistical analysis
The primary endpoint was ORR assessed by IRC per RECIST v1.1. Secondary endpoints included DoR, PFS, disease control rate by IRC and investigator, and OS. The safety/tolerability profile of tislelizumab was also examined. The safety analysis set was used for all safety analyses and included all patients who received tislelizumab. Efficacy‐evaluable analysis set was used for most efficacy analyses (OS used the safety analysis set) and included all patients who were receiving tislelizumab and who had measurable disease per IRC at baseline. Time‐to‐event outcomes, such as DoR, PFS, and OS, were estimated using the Kaplan‐Meier method and corresponding 95% CIs were calculated using the Brookmeyer‐Crowley method. Subgroup analyses assessed ORR according to the percentage of PD‐L1 expression on TC and IC, as well as by population demographics and baseline disease characteristics.
Assuming a target ORR of 25%, the sample size of 110 PD‐L1+ patients would provide 99% power to reject the null hypothesis of a 10% ORR at a 1‐sided alpha of 0.025.
3. RESULTS
3.1. Patient disposition, demographics, and baseline characteristics
As of September 16, 2019, 113 patients with locally advanced or metastatic PD‐L1+ UC who progressed during/following a platinum‐containing regimen were treated with tislelizumab. Median duration of treatment was 15.3 wk (range, 2‐101 wk) and median follow‐up time was 9.4 mo (range, 0.4‐23.6). Twenty (18%) patients remained on treatment and 93 (82%) discontinued tislelizumab (Figure 1). Reasons for discontinuation included disease progression (n = 53), AEs (n = 19), withdrawal of consent (n = 11), and symptomatic deterioration (n = 10).
FIGURE 1.
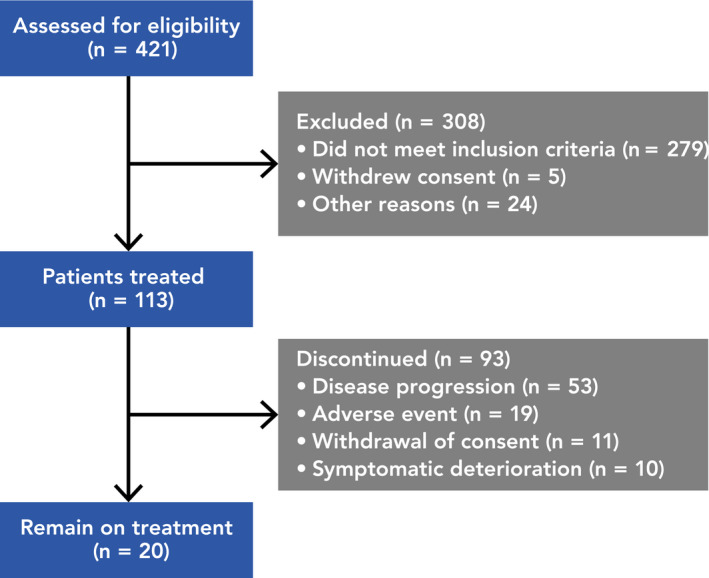
Patient disposition
Median patient age was 63 y (range, 36‐81); most patients were male (n = 84; 74%) and from China (n = 108; 96%) (Table 1). Primary tumors were most commonly found in the urinary bladder (n = 50) and renal pelvis (n = 31). At baseline, 24% of patients had only lymph node metastases and 24% had liver metastases. All patients (100%) received a prior platinum‐containing treatment regimen. Most patients received 1 (n = 69; 61%) or 2 (n = 37; 33%) prior anticancer regimens.
TABLE 1.
Patient demographics and baseline disease characteristics
| Characteristic | Patients (N = 113) |
|---|---|
| Age, y | |
| Median (range) | 63 (36, 81) |
| Gender, n (%) | |
| Male | 84 (74) |
| Female | 29 (26) |
| Smoking status, n (%) | |
| Never | 60 (53) |
| Current | 13 (12) |
| Former | 40 (35) |
| ECOG performance at baseline, n (%) | |
| 0 | 53 (47) |
| 1 | 60 (53) |
| Hemoglobin level at baseline, n (%) | |
| <10 g/dL | 18 (16) |
| ≥10 g/dL | 95 (84) |
| Site of primary tumor, n (%) | |
| Urinary bladder | 50 (44) |
| Renal pelvis | 31 (27) |
| Ureter | 24 (21) |
| Urethra | 3 (3) |
| Other | 5 (4) |
| Known metastasis at baseline, n (%) | |
| Visceral metastasis a | 86 (76) |
| Liver metastasis | 27 (24) |
| Lymph node only | 27 (24) |
| Number of prior regimens of anticancer therapies, n (%) | |
| 1 | 69 (61) |
| 2 | 37 (33) |
| ≥3 | 7 (6) |
| Prior platinum‐based therapy, n (%) b | |
| Cisplatin‐based | 85 (75) |
| Carboplatin‐based | 24 (21) |
| Other platinum‐based | 49 (43) |
| Intent of last therapy, n (%) | |
| First line for advanced disease | 73 (65) |
| Second line for advanced disease | 19 (17) |
| Adjuvant | 20 (18) |
| Neoadjuvant | 1 (<1) |
| PD‐L1 expression, n (%) | |
| TC < 50% and IC < 50% | 77 (68) |
| TC ≥ 50% or IC ≥ 50% | 36 (32) |
Abbreviations: IC, immune cell; PD‐L1, programmed death ligand 1; TC, tumor cell.
Considered as lung, bone, or any non‐lymph node or soft tissue metastasis.
Patients could receive multiple platinum‐based therapies prior to study entry.
3.2. Antitumor activity
Of the 104 (92%) patients in the efficacy‐evaluable population, confirmed objective responses were observed in 25 patients (ORR, 24%, 95% CI, 16, 33), including 10 CRs and 15 PRs per IRC assessment (Table 2). An efficacy sensitivity analysis excluded 17 patients who discontinued study treatment before their first tumor assessment and found that 25 (29%) of these patients had confirmed objective responses, 10 (11%) of which were CRs and 15 (17%) of which were PRs (Table 2).
TABLE 2.
Disease response per RECIST v1.1 by independent review committee in evaluable patients with PD‐L1+ urothelial carcinoma
| Response category | All patients (N = 104) | Sensitivity analysis (n = 87) |
|---|---|---|
| Best overall response, n (%) | ||
| Complete response | 10 (10) | 10 (11) |
| Partial response | 15 (14) | 15 (17) |
| Stable disease | 15 (14) | 15 (17) |
| Progressive disease | 47 (45) | 47 (54) |
| Not evaluable for response | 17 (16) | 0 |
| Objective response rate, % (95% CI) | 24 (16, 33) | 29 (20, 39) |
| Disease control rate, % (95% CI) | 38 (29, 49) | 46 (35, 57) |
| Clinical benefit rate, % (95% CI) | 29 (20, 39) | 34.5 (25, 45) |
Objective response rate was the proportion of patients who had confirmed complete response or partial response using RECIST v1.1; disease control rate was the proportion of patients who achieved complete response or partial response or stable disease using RECIST v1.1; clinical benefit rate was defined as patients with complete response or partial response or ≥ 24 wk of stable disease.
Abbreviations: CI, confidence interval; PD‐L1+, programmed death ligand 1 positive; RECIST v1.1, Response Evaluation Criteria in Solid Tumors version 1.1.
Per IRC assessment, 35 (34%) of 104 efficacy‐evaluable patients had a reduction of ≥30% in the sum of target lesion diameter from baseline (Figure 2). Among these 35 patients, 25 had a best overall response (BOR) of CR or PR; 2 patients with a BOR of progressive disease had new lesions and 8 had unconfirmed PRs, resulting in a BOR of stable disease. Even with a median follow‐up time of 9.4 mo, median DoR was not yet reached. Of 25 responders (Figure 3), 17 (68%) had ongoing responses at data cut‐off. Consistent response rates were observed among most population subgroups (Figure 4). Notably, higher ORRs were observed in subgroups of lymph node only (ORR, 44%; 95% CI, 23, 66) and no liver metastasis (ORR, 30%; 95% CI, 20, 42) (Figure 4). However, due to the small sample size, these data should be interpreted with caution.
FIGURE 2.
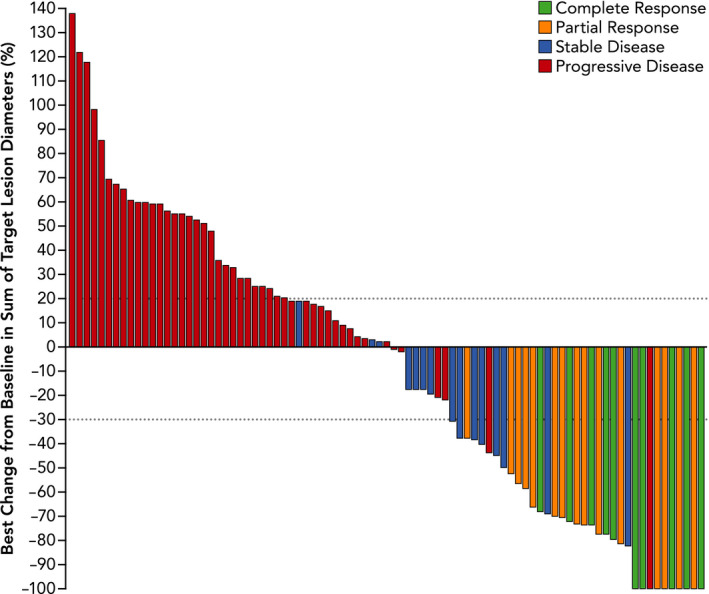
Best percent change in sum of target lesion diameters from baseline per independent review committee in efficacy‐evaluable patients with programmed death ligand 1‐positive urothelial carcinoma
FIGURE 3.
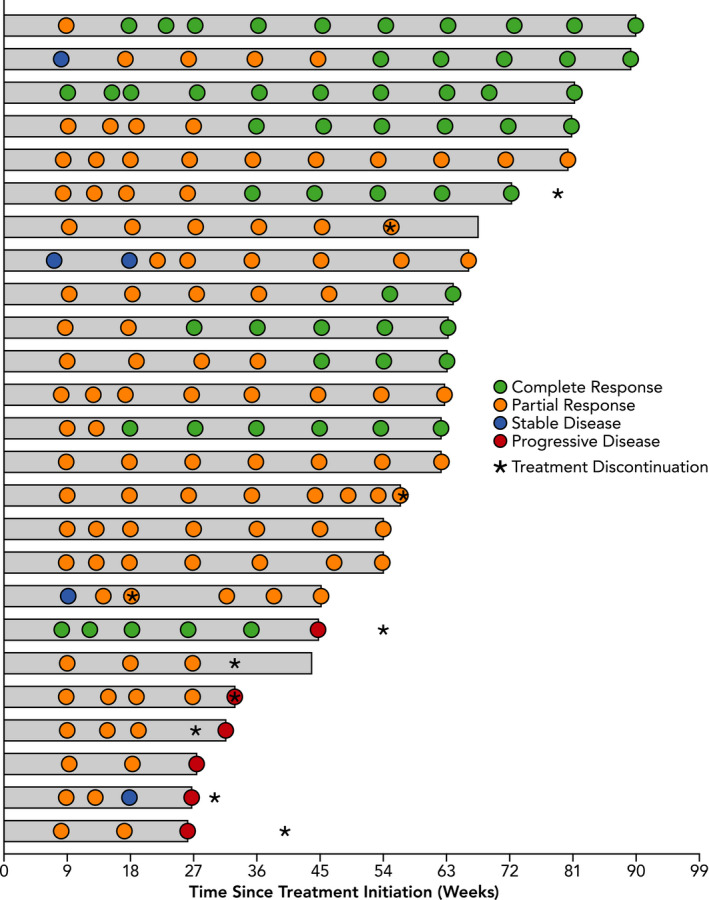
Time and duration of confirmed responses per RECIST v1.1 by independent review committee. Gray bars represent the duration of response
FIGURE 4.
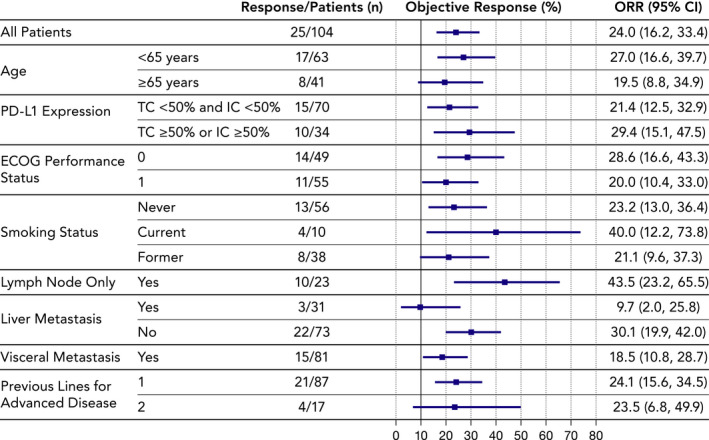
Objective response rates (ORRs) per RECIST v1.1 by independent review committee by population subgroup. Abbreviations: CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; IC, immune cell; PD‐L1, programmed death ligand 1; TC, tumor cell
3.3. Survival estimates
Across the entire population, median OS was 9.8 mo (95% CI, 7.5, 12.5) with 6‐mo and 12‐mo OS rates of 67% (95% CI, 57, 74) and 43% (95% CI, 33, 52), respectively (Figure 5). Median PFS among efficacy‐evaluable patients per IRC was 2.1 mo (95% CI, 2.0, 3.2); the proportion of patients with PFS at 6 mo and 12 mo was 32% (95% CI, 23, 41) and 20% (95% CI, 12, 28), respectively (Figure 6).
FIGURE 5.
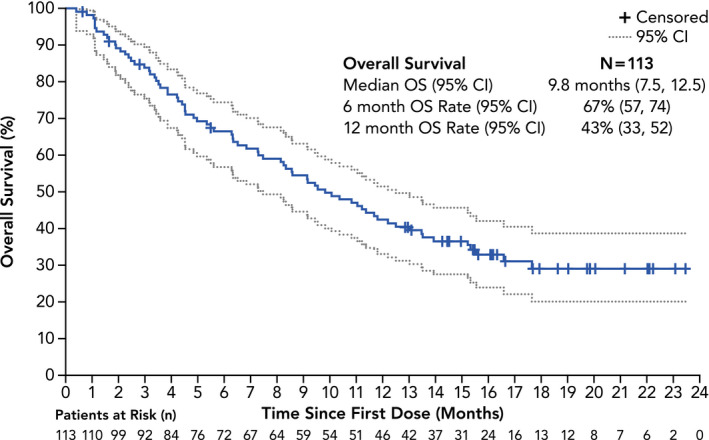
Kaplan‐Meier plot of overall survival (OS) (safety analysis set). Abbreviation: CI, confidence interval
FIGURE 6.
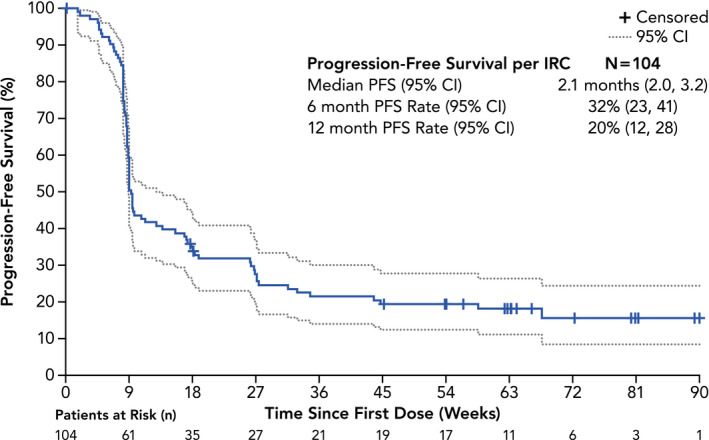
Kaplan‐Meier plot of PFS per RECIST version 1.1 by IRC (efficacy‐evaluable set). Abbreviations: CI, confidence interval; IRC, independent review committee; PFS, progression‐free survival; RECIST v1.1, Response Evaluation Criteria in Solid Tumors version 1.1.
3.4. Safety and tolerability of tislelizumab
A total of 106 (94%) patients experienced at least 1 AE considered to be related to tislelizumab by the investigator (AEs definitely related, probably related, possibly related, or possibly unrelated to tislelizumab, as well as those missing causal relationships, were defined as related AEs). Anemia (n = 31; 27%) and pyrexia (n = 22; 20%) were the most common treatment‐related AEs (TRAEs). Most reported TRAEs were grade 1‐2 in severity; anemia (n = 8; 7%) and hyponatremia (n = 6; 5%) were the only grade 3‐4 TRAEs occurring in ≥5% patients (Table 3). TRAEs led to treatment discontinuation of 16 (14%) patients; drug eruption (n = 3; 3%) and renal failure (n = 2; 2%) were the only TRAEs occurring in at least 1 patient.
TABLE 3.
Treatment‐related adverse events occurring in ≥ 5% of patients
| Events | All Grades | Grade 3‐4 |
|---|---|---|
| Patients with ≥ 1 treatment‐related adverse event, n (%) | 106 (94) | 43 (38) |
| Anemia | 31 (27) | 8 (7) |
| Pyrexia | 22 (19) | 0 |
| Decreased appetite | 21 (19) | 4 (4) |
| Increased aspartate aminotransferase | 19 (17) | 2 (2) |
| Increased alanine aminotransferase | 18 (16) | 4 (4) |
| Increased blood creatinine | 17 (15) | 2 (2) |
| Constipation | 17 (15) | 0 |
| Hyponatremia | 17 (15) | 6 (5) |
| Pruritus | 17 (15) | 0 |
| Urinary tract infection | 16 (14) | 4 (4) |
| Rash | 15 (13) | 0 |
| Hypoalbuminemia | 14 (12) | 0 |
| Hypothyroidism | 11 (10) | 0 |
| Upper respiratory tract infection | 10 (9) | 3 (3) |
| Nausea | 9 (8) | 0 |
| Vomiting | 9 (8) | 0 |
| Increased blood bilirubin | 8 (7) | 3 (3) |
| Increased blood urea | 8 (7) | 0 |
| Abdominal distension | 7 (6) | 0 |
| Asthenia | 7 (6) | 1 (1) |
| Diarrhea | 7 (6) | 2 (2) |
| Increased blood alkaline phosphatase | 7 (6) | 1 (1) |
| Increased gamma‐glutamyl transferase | 7 (6) | 3 (3) |
| Proteinuria | 7 (6) | 0 |
| Abdominal pain | 6 (5) | 2 (2) |
| Decreased neutrophil count | 6 (5) | 0 |
| Decreased white blood cell count | 6 (5) | 0 |
| Edema peripheral | 6 (5) | 1 (1) |
| Fatigue | 6 (5) | 1 (1) |
| Hematuria | 6 (5) | 2 (2) |
| Hyperglycemia | 6 (5) | 1 (1) |
| Hyperthyroidism | 6 (5) | 0 |
| Increased blood lactate dehydrogenase | 6 (5) | 0 |
Immune‐related AEs (irAEs) occurred in 31 (27%) patients; irAEs occurred in ≥5% of patients included skin adverse reactions (n = 13; 12%), hypothyroidism (n = 12; 11%), and hyperthyroidism (n = 7; 6%) (Table 4). Eight (7%) patients had irAEs of grade ≥ 3; no fatal irAEs were reported. Serious TRAEs occurred in 42 (37%) patients, the most common being pyrexia (n = 4; 4%) and upper respiratory tract infection, urinary tract infection, and drug eruption (n = 3; 3% each). Among the 7 patients with a TRAE leading to death, 3 were considered possibly related to study treatment by the investigators (hepatic failure, n = 2; respiratory arrest, n = 1); 3 were considered possibly unrelated to study treatment by the investigators (renal failure, n = 1; renal impairment, n = 1; general physical health deterioration, n = 1); and 1 patient did not have causality of death assigned by the investigator (unexplained death, n = 1).
TABLE 4.
Immune‐related TEAEs
| Events | All Grades | Grade 3‐4 |
|---|---|---|
| Patients with ≥ 1 immune‐related TEAE, n (%) | 31 (27) | 8 (7) |
| Skin adverse reaction | 13 (12) | 3 (3) |
| Hypothyroidism | 12 (11) | 0 |
| Hyperthyroidism | 7 (6) | 0 |
| Hepatitis | 3 (3) | 3 (3) |
| Thyroiditis | 2 (2) | 0 |
| Type 1 diabetes mellitus | 2 (2) | 0 |
| Nephritis and renal dysfunction | 2 (2) | 1 (<1) |
| Pancreatitis | 2 (2) | 2 (2) |
| Colitis | 1 (<1) | 1 (<1) |
| Pneumonitis | 1 (<1) | 0 |
| Other reactions | 1 (<1) | 0 |
Abbreviation: TEAE, treatment‐emergent adverse event.
4. DISCUSSION
Tislelizumab showed a predictable and manageable safety/tolerability profile and demonstrated clinically meaningful antitumor activity in patients with PD‐L1+ UC. At data cut‐off, median duration of study follow‐up was 9.4 mo (range, 0.4‐23.6) and 20 (18%) patients remained on treatment. Of 113 Asian patients treated, 106 (94%) experienced any grade of TRAE. Fifty (44%) patients reported a grade ≥ 3 TRAE. Seven patients experienced a fatal investigator‐assessed TRAE, of which 3 deaths were considered to be possibly related to study treatment by the investigators. The confirmed ORR was 24%; 40% (10/25) of patients with confirmed responses had CRs. Subgroup analyses showed higher ORRs in subgroups of lymph node only (ORR, 44%, 95% CI, 23, 66) and no liver metastasis (ORR, 30%; 95% CI, 20%, 42%). The safety profile observed was similar to that of other PD‐1/L1 inhibitor therapies and was consistent with previous published reports of tislelizumab in other advanced solid tumors. No new safety signals were observed.
Tislelizumab demonstrated clinically meaningful responses in a hard‐to‐treat population including patients with advanced disease, all of whom had received prior platinum‐containing treatment. Roughly three‐quarters of patients had visceral metastases, including 24% with liver metastases and 23% with bone metastases. Of the PD‐L1+ patients included in this study, 32% of patients had PD‐L1 expression of ≥ 50% on IC and/or TCs; responses were consistent in these patients compared with those with < 50% TC/IC PD‐L1 expression. Although this study only recruited PD‐L1+ patients, comparable ORR was seen in tislelizumab trials that included PD‐L1− patients with UC, 17 , 18 , 19 , 20 , 21 suggesting further exploration into both patient populations is warranted. The proportion of patients achieving CR was comparable with tislelizumab vs other PD‐1/PD‐L1 inhibitors 24 and the longest CR was observed for > 2 y, which may indicate a longer DoR and clinical benefit.
Although anti‐PD‐1/PD‐L1 antibodies have demonstrated favorable efficacy for metastatic UC, none of these therapeutics have been approved for locally advanced or metastatic UC in China. This trial is the first registrational study in China for metastatic UC, and the results presented demonstrate that tislelizumab is a promising treatment option for patients after failure of prior platinum‐based chemotherapy. Furthermore, this is the largest study of Chinese patients with UC and led to the conditional approval of tislelizumab from China's National Medical Products Administration for patients with previously treated locally advanced or metastatic UC with PD‐L1–high expression.
Although the single‐arm design of the current study did not allow for a direct assessment, the antitumor activity presented is consistent with reports from other checkpoint inhibitors. The phase 3 KEYNOTE‐045 study reported that patients with advanced UC who received second‐line pembrolizumab monotherapy had a similar ORR (21%) and rates of CR (9%) and PR (12%), as we report with tislelizumab in the current study. 25 Additionally, due to the small sample size and a relatively homogenous study population, generalization and conclusions may be limited. However, the preliminary safety/tolerability profile, as well as the deep and durable antitumor activity demonstrated in the current study, supported continued development of tislelizumab in patients with UC. A phase 3 study of tislelizumab in combination with platinum‐containing chemotherapy as a first‐line treatment for UC (NCT03967977) is currently ongoing and is recruiting patients.
DISCLOSURE STATEMENT
Dingwei Ye, Jiyan Liu, Aiping Zhou, Qing Zou, Hanzhong Li, Cheng Fu, Hailong Hu, Jian Huang, Shaoxing Zhu, Jie Jin, Lulin Ma, Jianming Guo, Jun Xiao, Se Hoon Park, Dahong Zhang, and Feng Bi have nothing to disclose. Xiusong Qiu, Yuanyuan Bao, Lilin Zhang, and Wei Shen are employees of BeiGene, Ltd. The study was designed under the responsibility of BeiGene, Ltd, in conjunction with the steering committee. The study was funded, and tislelizumab was provided by, BeiGene Ltd. Additionally, BeiGene, Ltd. collected and analyzed the data and contributed to the interpretation of the study. All authors had full access to all of the data in the study and had final responsibility for the decision to submit for publication.
ACKNOWLEDGMENTS
The authors wish to acknowledge the investigative center study staff and to recognize those from BeiGene, Ltd. who have contributed substantially to the development of this publication. Writing and editorial assistance was provided by Stephan Lindsey, PhD, and Elizabeth Hermans, PhD (OPEN Health Medical Communications, Chicago, IL, USA), and funded by the sponsor.
Ye D, Liu J, Zhou A, et al. Tislelizumab in Asian patients with previously treated locally advanced or metastatic urothelial carcinoma. Cancer Sci. 2021;112:305–313. 10.1111/cas.14681
Ye and Liu contributed equally as first authors.
DATA AVAILABILITY STATEMENT
Upon request, and subject to certain criteria, conditions, and exceptions, BeiGene will provide access to individual de‐identified participant data from BeiGene‐sponsored global interventional clinical studies conducted for medicines: (1) for indications that have been approved, or (2) in programs that have been terminated. BeiGene will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data requests may be submitted to medicalinformation@beigene.com
REFERENCES
- 1. Apetoh L, Ladoire S, Coukos G, Ghiringhelli F. Combining immunotherapy and anticancer agents: the right path to achieve cancer cure? Ann Oncol. 2015;26(9):1813‐1823. [DOI] [PubMed] [Google Scholar]
- 2. Gartrell BA, He T, Sharma J, Sonpavde G. Update of systemic immunotherapy for advanced urothelial carcinoma. Urol Oncol. 2017;35(12):678‐686. [DOI] [PubMed] [Google Scholar]
- 3. Dreicer R, Manola J, Roth BJ, et al. Phase III trial of methotrexate, vinblastine, doxorubicin, and cisplatin versus carboplatin and paclitaxel in patients with advanced carcinoma of the urothelium. Cancer. 2004;100(8):1639‐1645. [DOI] [PubMed] [Google Scholar]
- 4. Sternberg CN, de Mulder PH, Schornagel JH, et al. Randomized Phase III Trial of High–Dose‐Intensity Methotrexate, Vinblastine, Doxorubicin, and Cisplatin (MVAC) Chemotherapy and Recombinant Human Granulocyte Colony‐Stimulating Factor Versus Classic MVAC in Advanced Urothelial Tract Tumors: European Organization for Research and Treatment of Cancer Protocol No. 30924. J Clin Oncol. 2001;19(10):2638‐2646. [DOI] [PubMed] [Google Scholar]
- 5. De Santis M, Bellmunt J, Mead G, et al. Randomized phase II/III trial assessing gemcitabine/carboplatin and methotrexate/carboplatin/vinblastine in patients with advanced urothelial cancer who are unfit for cisplatin‐based chemotherapy: EORTC study 30986. J Clin Oncol. 2012;30(2):191‐199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Sonpavde G. PD‐1 and PD‐L1 inhibitors as salvage therapy for urothelial carcinoma. N Engl J Med. 2017;376(11):1073‐1074. [DOI] [PubMed] [Google Scholar]
- 7. Dahan R, Sega E, Engelhardt J, Selby M, Korman AJ, Ravetch JV. FcgammaRs modulate the anti‐tumor activity of antibodies targeting the PD‐1/PD‐L1 axis. Cancer Cell. 2015;28(3):285‐295. [DOI] [PubMed] [Google Scholar]
- 8. Mahoney KM, Freeman GJ, McDermott DF. The next immune‐checkpoint inhibitors: PD‐1/PD‐L1 blockade in melanoma. Clin Ther. 2015;37(4):764‐782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Wang X, Teng F, Kong L, Yu J. PD‐L1 expression in human cancers and its association with clinical outcomes. Onco Targets Ther. 2016;9:5023‐5039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Siefker‐Radtke A, Curti B. Immunotherapy in metastatic urothelial carcinoma: focus on immune checkpoint inhibition. Nat Rev Urol. 2018;15(2):112‐124. [DOI] [PubMed] [Google Scholar]
- 11. Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti‐PD‐1 antibody in cancer. N Engl J Med. 2012;366(26):2443‐2454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Zhou TC, Sankin AI, Porcelli SA, Perlin DS, Schoenberg MP, Zang X. A review of the PD‐1/PD‐L1 checkpoint in bladder cancer: From mediator of immune escape to target for treatment. Urol Oncol. 2017;35(1):14‐20. [DOI] [PubMed] [Google Scholar]
- 13. Zhang T, Song X, Xu L, et al. The binding of an anti‐PD‐1 antibody to FcgammaRIota has a profound impact on its biological functions. Cancer Immunol Immunother. 2018;67(7):1079‐1090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Lee SH, Lee HT, Lim H, Kim Y, Park UB, Heo Y‐S. Crystal structure of PD‐1 in complex with an antibody‐drug tislelizumab used in tumor immune checkpoint therapy. Biochem Biophys Res Commun. 2020;527(1):226‐231. [DOI] [PubMed] [Google Scholar]
- 15. Lee A, Keam SJ. Tislelizumab: first approval. Drugs. 2020;80(6):617‐624. [DOI] [PubMed] [Google Scholar]
- 16. Feng Y, Hong Y, Sun H, et al. The molecular binding mechanism of tislelizumab, an investigational anti‐PD‐1 antibody, is differentiated from pembrolizumab and nivolumab. Presented at the 110th Annual Meeting of the American Association for Cancer Research, Atlanta, GA. March 29‐April 3, 2019; Abstract 2382.
- 17. Guo J, Yuan Y, Bai Y, et al.Tislelizumab in Chinese patients with melanoma, urothelial carcinoma (UC), and renal cell carcinoma (RCC). Presented at 22nd Annual Chinese Society for Clinical Oncology Congress; September 18–22, 2019; Xiamen, China.
- 18. Sandhu S, Hill A, Gan H, et al. Tislelizumab, an anti‐PD‐1 antibody, in patients with urothelial carcinoma (UC): results from an ongoing phase I/II study. Ann Oncol. 2018;29(Suppl 10):X28. [Google Scholar]
- 19. Desai J, Deva S, Lee JS, et al. Phase IA/IB study of single‐agent tislelizumab, an investigational anti‐PD‐1 antibody, in solid tumors. J Immunother Cancer. 2020;8(1):e000453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Shen L, Guo J, Zhang Q, et al. Tislelizumab in Chinese patients with advanced solid tumors: an open‐label, non‐comparative, phase 1/2 study. J Immunother Cancer. 2020;8(1):e000437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Ye D, Liu J, Zhou A, et al. First report of efficacy and safety from a phase 2 trial of tislelizumab, an anti‐pd‐1 antibody, for the treatment of pd‐l1+ locally advanced or metastatic urothelial carcinoma in Asian patients. Ann Oncol. 2019;30(Suppl 5):V367. [Google Scholar]
- 22. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228‐247. [DOI] [PubMed] [Google Scholar]
- 23. Zajac M, Boothman AM, Ben Y, et al. Analytical validation and clinical utility of an immunohistochemical programmed death ligand‐1 diagnostic assay and combined tumor and immune cell scoring algorithm for durvalumab in urothelial carcinoma. Arch Pathol Lab Med. 2019;143(6):722‐731. [DOI] [PubMed] [Google Scholar]
- 24. Powles T, Necchi A, Rosen G, Hariharan S, Ab A. Anti‐programmed cell death 1/ligand 1 (PD‐1/PD‐L1) antibodies for the treatment of urothelial carcinoma: State of the art and future development. Clin Genitourin Cancer. 2018;16(2):117‐129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Fradet Y, Bellmunt J, Vaughn DJ, et al. Randomized phase III KEYNOTE‐045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: results of >2 years of follow‐up. Ann Oncol. 2019;30(6):970‐976. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Upon request, and subject to certain criteria, conditions, and exceptions, BeiGene will provide access to individual de‐identified participant data from BeiGene‐sponsored global interventional clinical studies conducted for medicines: (1) for indications that have been approved, or (2) in programs that have been terminated. BeiGene will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data requests may be submitted to medicalinformation@beigene.com