

Abstract
We examine how labor together with social participation protects against cognitive impairment and depression, with a focus on gender differences. Data are drawn from four waves of the Korean Longitudinal Study of Aging (2006–2012). Both paid work and unpaid work are considered labor participation. Social participation includes the frequency of participation in formal social institutions, religious groups, grandparenting, and interactions with family and friends. Using growth curve models, we find that social and labor participation are independently associated with outcomes and effects vary by gender. Religious group activity was beneficial only for women, whereas inability to work was detrimental for men only. Informal social gatherings and labor participation, paid or unpaid, were beneficial for both genders. Findings on gender differences highlight how social identities can shape social roles and confine activity space, and productive engagement, affecting outcomes for mental health in later life.
Keywords: mental health, gender, social participation, labor force participation, aging in Asia, Korea
Introduction
Remaining active and productive is critical for older adults to maintain their health and well-being. In fact, participation in various social and economic activities has long been considered an important factor that contributes to “Successful Aging” (Rowe and Kahn 1997). Attendance at family gatherings, volunteering, civic engagement, caregiving, and labor force participation have all been linked to better health outcomes in later life (for a review, Adams, Leibbrandt, and Moon 2011; Staudinger et al. 2016), especially cognitive and mental health. Prior studies suggest that participation in these activities may provide opportunities to access material and/or psychosocial resources, maintain identity and self-worth, and reduce stress and loneliness, all of which are important pathways to remaining healthy at older ages.
Health benefits of activity participation have received growing attention particularly in societies undergoing the significant demographic shift to an aging society, such as South Korea (Korea hereinafter). Korea is projected to have one of the oldest populations in the world by 2050, with more than 30% of the population aged 65 years and over (Keese 2006; Kwon 2008). As a result, age-related mental and neurological disorders have become major public health challenges in Korea. The most common mental and neurological disorders in this age group are dementia and depression, affecting approximately 10% to 30% of Korean older adults (Kim et al. 2011; Park et al. 2012; Statistics Korea 2011). Both conditions are more prevalent among women than men. This is particularly problematic as social spending on long-term health care is limited in Korea, resulting in inadequate social protection for the health of the aging population (Yoon 2013), especially for older women who tend to outlive men.
Several studies have examined the impact of activity participation on these health problems, with an aim to create interventions to reduce further disparities. However, the evidence is inconclusive. Previous work in the Korean literature has focused largely on social participation without much attention to labor participation as an important (and simultaneously) contributing factor, although a large proportion of Korean older adults still remain in or have reentered the labor force. Senior labor force participation in Korea is the second highest among Organisation for Economic Co-operation and Development (OECD) countries, and is far more common than in the West. Despite the large number of older workers, however, empirical evidence on work and mental health in late adulthood in the Korean context is largely limited. It is also unknown how labor and social participation matter simultaneously for mental health, although there is a growing recognition that engaging in more than one domain of activity participation provides significant health benefits (Glass et al. 2006; Morrow-Howell et al. 2014). Furthermore, little is known about the role of gender, although Korean older women likely experience social and labor participation differently compared with men, given limited access due to a gender division of labor deeply rooted in traditional Korean culture. If men and women are socially expected to engage in different types of participation, health benefits from each type of participation are likely to vary by gender.
We extend prior work by considering social and labor participation simultaneously, using four waves of the Korean Longitudinal Study of Aging (2006–2012). We focus on the occurrence of cognitive impairment and depression over a six-year period as important markers of poor later-life health. Because we expect that patterns of activity participation may differ by gender, we stratify the sample by gender. We posit that gender differences in the association between activity participation and the measured outcomes may be partly attributed to different life experiences and opportunities available for men and women over the life course.
Background
Social Participation, Psychosocial Resources, and Mental Health
Several established theories in social science, including social engagement theory (Lemon, Bengtson, and Peterson 1972) and the successful aging model (Rowe and Kahn 1997), emphasize that social participation is critical for the lives of older adults. These theories define social participation as attending organized groups or gatherings. Social participation includes group activities that are formally organized in institutional contexts to do things together such as attending religious services, meetings of a local political or community organization, playing team sports, or volunteering. It also includes informal social gatherings that often occur within personal settings including family, friends, and neighbors.
Social participation encourages the formation of new social relationships or may strengthen existing relationships, both of which may increase participants’ sources of support (Cohen 2004). Furthermore, emotional support obtained through spending time with family and friends may positively influence older adults’ well-being by reducing stress and social isolation, among other benefits (Chen and Feeley 2014). In addition, older adults can share their values and beliefs with others through participation in organized group activities such as volunteering and civic engagement, which may, in turn, enhance their sense of belonging and identity (Berkman and Glass 2000; Haslam, Cruwys, and Haslam 2014; Thoits 2011). Research has shown that social roles gained through participation in such formal settings may help maintain self-efficacy and self-esteem (Berkman and Glass 2000), resources which can benefit overall mental health at older ages. Research based on social capital theory suggests that social connections gained through community programs may provide opportunities to access various kinds of information and knowledge, which may demand more attention and stimulate cognitive activity (Carlson et al. 2008). Conversely, lower levels of social engagement have been associated with higher levels of loneliness and distress (Cornwell and Waite 2009), potentially compromising cognitive function in later life (Cacioppo and Hawkley 2009).
To date, several studies in Korea have examined the role of social participation in mental health and cognitive aging. Using nationally representative samples of Korean older adults, prior work showed that attending informal social gatherings with alumni and friends reduces the risk of cognitive impairment (Choi et al. 2016; Kim, Arai, and Kim 2017; Lee and Kim 2016). Frequent interaction with family members is also likely to slow progression of depressive symptoms (Roh et al. 2015). This line of work generally supports the idea that informal social participation is protective of Korean older adults’ mental health—preventing depression and slowing down age-related cognitive decline as in the Western context.
Evidence on formal social participation remains inconclusive, especially in Asia. Studies in Korea often fail to find a relationship between mental health and formal social participation (Choi et al. 2016; Kim et al. 2017), unlike previous studies conducted in Western aging populations (Greenfield and Marks 2004; Harris and Thoresen 2005). This may be, in part, due to the ambiguous operationalization of social participation in the Korean literature. Although informal and formal social participation are distinct (though related) constructs, most existing research conflates the two by collapsing them into one measure of social participation. Recent evidence outside of Korea has shown that formal and informal social participation have different and independent implications for older adult health (Ang 2018), suggesting the need for a more nuanced approach in measuring social participation when examining the association between social participation and health. We thus expand prior work by investigating the implications of informal and formal social participation separately and simultaneously.
Labor Participation, Mental Stimulation, and Mental Health
Labor participation is another distinct form of activity engagement at older ages that influences the lives of older adults. John W. Rowe and Robert L. Kahn (1997) consider social and economic participation (whether paid or unpaid) as equally important factors determining “Successful Aging.” In fact, a growing body of research outside of Asia finds that the two factors independently predict older adult health (Adams et al. 2011; Burr, Mutchler, and Caro 2007; Hinterlong, Morrow-Howell, and Rozario 2007). This implies that labor participation may capture some other important mechanisms by which activity participation impacts later-life health that social participation alone may not fully explain.
There is good evidence that labor participation helps older adults maintain optimal cognitive function and mental well-being in later life (for a review see Nexø, Meng, and Borg 2016). This line of research is largely based on the “use it or lose it” hypothesis—mental work demands and job control help stimulate and keep the brain/mind sharp and alert, which can help create cognitive reserve (Tucker and Stern 2011). Studies of U.S. and Chinese older adults report that those who have worked in an occupation with a high demand of mental work for a long time have higher levels of cognitive function in later life, compared with those whose occupation does not have such a demand (Fisher et al. 2014; Liang et al. 2019). Others speculate that working at older ages may have potential benefits to later-life mental health through the learned ability to navigate social cues and adapt to new social roles in a new social group (Flatt and Hughes 2013). In a study of Singaporean older adults, Andiara Schwingel et al. (2009) found that engaging in a new social group at work may enhance an older adult’s psychological health and protect against depressive symptoms by cultivating postretirement adjustment.
In contrast, there is relatively little work on the topic in the Korean literature. The lack of attention to labor participation and later-life mental health in the current literature may be because of the strong assumption that older adults discontinue their labor participation once they reach retirement age. However, a closer look at labor participation becomes more important as more seniors remain or reenter the labor market as a result of longer life spans and changes in family structure (Flochel et al. 2015; Klassen and Yang 2013). Adult children no longer serve as a security blanket for their aging parents; continuing to work and maintaining financial security after retirement age has become a necessity rather than a conscious choice for many Korean older adults. In fact, the employment rate of the elderly population in Korea has remained relatively high compared with the OECD average (OECD 2012). This rate is higher in Korea compared with those of Western populations such as the United States, as well as other Asian countries like China and Singapore (Giles, Wang, and Cai 2012; Ministry of Community Development, Youth and Sports 2008; OECD 2006). Although a few Korean studies have examined the effect of continued employment status on cognitive functioning (Min et al. 2015) and depression (Kang et al. 2016), less evidence exists on whether social and labor participation are independently associated with mental health. How social and labor participation simultaneously contribute to mental health in the Korean context remains largely unknown, although there is a growing recognition that engaging in a much broader spectrum of activity than just one domain may provide significant health benefits (Glass et al. 2006; Morrow-Howell et al. 2014). This study begins to fill this gap.
The Korean Context: Filial Piety and Gender Division of Labor
Prior research has shown that the relationship between activity participation and later-life health varies by gender (Thomas 2011). The gender differences are expected to be more pronounced in societies with a strong gender hierarchy and greater gender inequality (Hsu 2005), but empirical evidence examining the role of gender in active aging and health has been largely absent in the Korean context. Yet, there are several theoretical reasons to expect that processes may work differently for men and women based on gender role expectations unique to the Korean culture and society.
First, Confucian values and traditional gender role expectations are deeply rooted in Korean society, exposing older women to different social opportunities and life chances over the life course. Korea is a family-oriented society wherein women are culturally expected to provide unpaid domestic work such as housework, whereas men generally become “breadwinners” by participating in paid work. Women, particularly those in earlier cohorts, had limited opportunities to attain higher education and social status. For instance, only 8% of Korean women aged 55 to 64 years in 2012 hold college degrees, the second lowest rate among all OECD countries (OECD 2014).
Second, due to expectations of traditional gender roles, women may have not only lower educational attainment but also limited work histories relative to men. Traditions of filial piety and seniority expect young married couples to cohabit with parents, and place the burden of caring for parents-in-law on married women. This was particularly true for women in older cohorts, which limited their opportunities to participate in the labor force (Sung 2003). Even as it becomes more socially acceptable for their daughters or daughters-in-law to continue working, many older women are unable to alleviate their family obligations because they are now expected to care for their grandchildren instead (Lee and Bauer 2013), imposing time constraints to participate in activities outside of the household.
Third, because educational attainment and paid employment may condition different institutional and social environments, the social lives of men and women may occur in different spaces and/or contexts, potentially providing different health effects. The theory of resource substitution (Ross, Masters, and Hummer 2012) suggests that individuals with fewer resources (e.g., income, power, and authority) are more likely to benefit from resources alternative to their own. Given that older women tend to have lower levels of schooling and are less likely to accumulate socioeconomic status (SES) than older men, women may rely more heavily on resources from social activities to gain health benefits, whereas men may have cumulatively gained health advantages from economic activities. Organizing family gatherings and managing various informal social networks are typically considered the responsibility of married women. Therefore, men may rely more on their spouses and be less motivated to maintain their social ties with family and friends, favoring social activity that is generally practiced in a formal setting and in the work environment. By contrast, social activity in an informal, unpaid setting such as family gatherings and caregiving might be more prevalent and consequential for women.
Only a few studies have examined the role of gender in the association between activity participation and Korean older adult mental health, and findings are mixed. Some studies show that social participation is beneficial for both men and women (Katagiri and Kim 2018; Lee et al. 2008), whereas others show that not all participation has the same impact on health. Some forms of activity participation, such as gatherings of family and friends, appear to have more pronounced effects for women than men in Korea (Roh et al. 2015). Formal social participation (Lee and Lee 2011) and continued labor force participation (Min et al. 2015) were more consequential for men’s mental health, supporting the idea that men typically participate in the activities outside of the home domain to which Korea older women may not have had equal access. Others found no gender differences in the associations between employment and depression (Jang et al. 2009).
These insights from previous studies are important, but existing findings are primarily based on cross-sectional studies, and less is known about associations over time. Longitudinal studies help us understand whether activity participation predicts changes in mental health status and whether gender differences exist in long-term relationships between participation and health. Prior work has also focused primarily on one domain of activity participation at a time, although the domains are clearly gendered and may result in different health consequences for men and women.
Hypotheses and Contributions of the Current Study
To build on previous work, we propose three hypotheses. First, older adults who are more socially engaged and who continue to participate in the workforce will be less likely to develop depression and cognitive impairment over time. Social and labor participation will each have significant impacts on measured outcomes, even after accounting for them simultaneously (Hypothesis 1). Second, due to gender role expectations within the Korean family and society, the same activities will have different impacts on women and men’s mental health over time. We expect that the effect of informal social gatherings will be more pronounced among women, whereas formal social participation may be more important to the health of men, compared with that of women (Hypothesis 2). Third, the protective effect of continued economic activities might be more pronounced for men than for women, in part, due to the compounding effect of cognitive reserve for men who have much longer work histories than women. In contrast, inability to work through disability and unemployment will have more pronounced effects for men than for women as it would damage men’s social identity as breadwinners (Hypothesis 3).
This study overcomes the limitations of previous research in three ways: (1) an integrated approach to activity participation—encompassing both social (formal and informal) and labor (paid and unpaid) participation; (2) the assessment of longitudinal associations of activity participation with mental health over a six-year period; and (3) the investigation of the role of gender in conditioning the effect of active engagement with life and mental health among Korean older adults.
Method
Data
Data were from four waves of the Korean Longitudinal Study of Aging (KLoSA 2006–2012). The KLoSA is a nationally representative panel survey of individuals aged 45 years and above in 2006, conducted every two years to elicit information on change over time. Using multistage stratified sampling, 10,254 individuals were interviewed from 6,171 households at the first wave in 2006. Appendix A illustrates how we derived the analytic sample. First, we excluded individuals who were aged below 60 years (n = 4,706) because the prevalence of cognitive impairment is relatively low below age 60 years and significantly increases thereafter (Salthouse 2009). We excluded those who were not cognitively sound at baseline (n = 2,457) to measure onset of cognitive impairment, but retained those who were depressed at baseline in the sample because depression is not an absorbing state (i.e., individuals may recover from depression). We also excluded individuals with unreliable values (i.e., large fluctuations from one wave to another) on the cognitive impairment score over the waves (n = 458), and individuals for whom one or more variables of interest were missing for all four waves (n = 60).
The final analytic sample predicting cognitive impairment consists of data from 2,573 participants, totaling 8,402 person-year observations over four waves. Only person-year observations with nonmissing information on all variables (i.e., complete cases) were used. This means that each participant could contribute anywhere between one and four person-year observations to the model (average person-year observations per respondent were 3.2). Following Yang Yang and Linda C. Lee (2009), we adjusted for selection biases by creating dummy variables for death (n = 257) and nonresponse (n = 589) at the individual level (Level 2). To maintain consistency and for ease of interpretation, we used the same analytical sample for models predicting depression (post hoc analysis shows that our findings on depression are robust to a number of different sample specifications).
Variables
Dependent Variables
We assessed cognitive impairment using the Korean version of the Mini-Mental State Examination (K-MMSE), a brief but reasonably accurate measure of cognitive function which has been previously shown to have sensitivity/specificity rates of above 90% (Folstein, Folstein, and McHugh 1975). Keeping in line with prior studies, we considered those who scored below 24 points (out of a possible 30 points) as cognitively impaired (Kim et al. 2019; Lyu and Kim 2016). This categorization was systematically validated for use in the Korean context (Kang, Na, and Hahn 1997) and has been widely adopted in prior research (Choi et al. 2016; Kim et al. 2017, 2019). We assessed depressive symptoms in KLoSA using the 10-item version of the Center for Epidemiologic Studies-Depression (CES-D) scale (Kohout et al. 1993). We constructed the score by summing responses (ranging from 0 to 3) across all items (with two positive items reverse coded), where a higher score indicated more depressive symptoms. A cutoff point of 10 (out of a possible 30) was used to denote depression, given past research in the Korean context supporting the use of this threshold (Lim et al. 2018).
Independent Variables
Activity participation was considered under two broad domains: social and labor participation. Consistent with previous work (Ang 2018; Utz et al. 2002), social participation was further subcategorized into formal and informal. Formal social participation was assessed according to respondents’ reports on how frequently they participate in (1) formal social activity and (2) religious group activity. For formal social activity, we coded 1 if they had participated in any of the following group activities that involve in formal organization settings: participation in senior community centers, educational/cultural/sports programs, alumni society, volunteer groups, and political groups. Informal social activities were measured by assessing respondents’ reports on time spent in (1) meeting with family and friends and (2) grandparenting. For grandparenting, we coded respondents as 1 if they had performed any grandparenting duties within the past year, and coded as 0 if they did not. For the rest of the other indicators for social activities (i.e., formal social activity, religious group activity, and meeting with family and friends), respondents were coded as 1 if they participated at least once a week in each of these activities, and coded as 0 otherwise. The cutoff point of “once a week” is a common threshold used to demarcate frequent attendance at social activities, based on past literature establishing associations between social activities and health (Glei et al. 2005; Sørensen, Waldorff, and Waldemar 2008).
Labor participation was assessed through work status. We grouped respondents into four mutually exclusive groups according to the type of work they were engaged in: (1) those who were retired (reference group), (2) paid labor (i.e., those with full-time or part-time employment, and those who were self-employed), (3) those working for their family without pay (for more than 18 hours a week), and (4) those economically inactive (i.e., disabled, unemployed, or not in the labor market).
Covariates
Baseline sociodemographic characteristics included age (range 60–91 years at baseline), education (1 = less than high school education; 0 = high school and above education), marital status (1 = married or partnered; 0 = separated, divorced, widowed, never married), log total annual household income (in tens of millions in Korean Won), rurality (1 = rural; 0 = not rural), and whether the respondent was living alone (1 = yes; 0 = no). Furthermore, we included two health-related covariates: the presence of heart-related diseases (including heart problems, stroke or hypertension) and limitations in activities of daily living (ADL) (including dressing oneself, bathing oneself, eating, using a toilet, and getting out of bed, and walking across a room). Heart-related diseases were dummy coded (1 = at least one disease; 0 = free of heart-related diseases), while the number of limitations for ADLs was used in the model. Furthermore, as cognitive function and depression may be associated, an indicator of depression was included as a covariate in cognitive outcome models, and vice versa. Health behavior was assessed by including a variable indicating how often respondents exercised (1 = at least once a week; 0 = less than once a week) in the model.
Analytic Strategy
To estimate the effects of activity participation on the onset of cognitive impairment and depression, we constructed growth curve models with mixed-effects logistic regression. This analytical framework accounts for partially missing (or unbalanced) data using maximum likelihood and often performs equally well (or better than) multiple imputation methods even with small samples (Shin, Davison, and Long 2017). The growth curve model framework accounts for the fact that within-individual probabilities for the onset of cognitive impairment and depression change over time. We nested observations from each wave of data collection (Level 1) within individuals (Level 2), using the Akaike information criterion (AIC) and Bayesian information criterion (BIC) as model selection criteria. We estimated both (1) random effects for the rate of growth and (2) interaction terms between the independent variables and the rate of growth, retaining these terms only if doing so improved model fit. Only random effects for the rate of growth in the models predicting depression improved overall model fit and were retained. None of the interaction terms between independent variables and rate of growth were significant across all models, signifying a lack of evidence that the association between independent variables and the outcome changed over time. We thus specify the more parsimonious model by constraining the association between independent variables and outcomes to be equal over time. The final model can be expressed formally with the following equations:
where subscripts i and j index the individual and person-year observation, respectively, μ denotes the fixed intercept, δ indicates fixed-effects for the linear and quadratic growth terms, and β is the vector of coefficients associated with the vector of independent variables and covariates X. α and γ terms represent normally distributed random-effects for the intercept and linear growth term, respectively. Finally, ϵ represents the error term for each person-year observation within individuals.
A key theoretical motivation in this paper is the inclusion of both labor and social activities to examine how they independently affect mental health and how the associations differ by gender. Therefore, we estimate three regression models using the following variable configurations: (1) social participation only, (2) labor participation only, and (3) both social and labor participation. Furthermore, we stratified the analyses by gender, given that unconditional growth curve models revealed substantial differences between male and female growth trajectories for both depression and cognitive impairment (see Figure 1). To assess if gender differences were statistically significant across the models, we ran a full (i.e., unstratified) model and included interaction terms between gender and every variable in the model (including independent variables and covariates) to test for equality of coefficients. A summary of results for unstratified models as well as the models including interaction terms can be found in Appendix B. A statistically significant interaction term between the independent variable and gender indicated the presence of gender difference in the association between activity participation and cognitive impairment/depression, and are highlighted in the “Results” section. We included sociodemographic and health covariates in all models, and all models were weighted at the individual level (Level 2) to adjust for the complex survey design in KLoSA.
Figure 1.
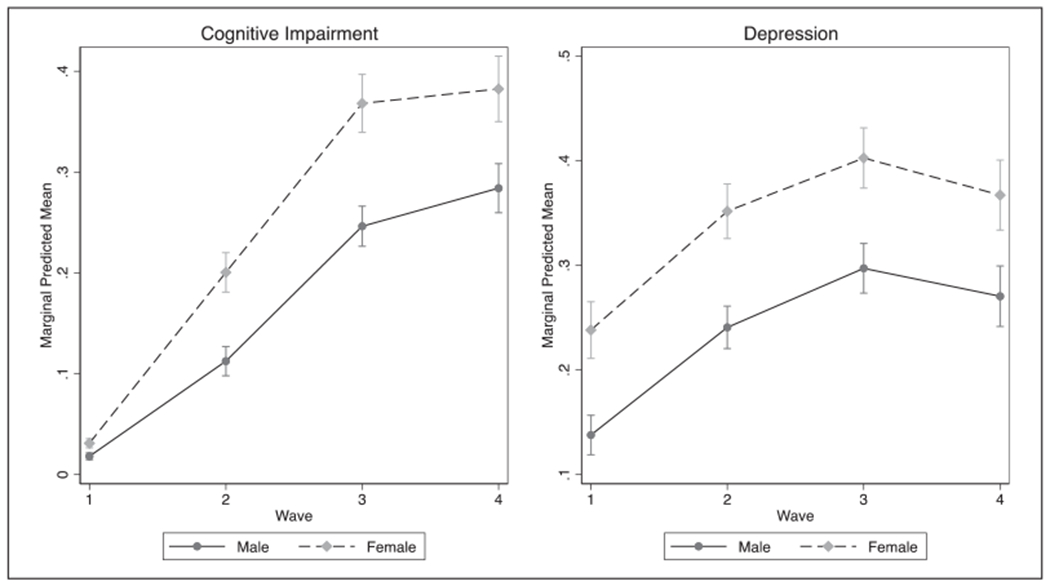
Unconditional growth curve trajectories for the risk of cognitive impairment and depression.
As part of sensitivity analyses, we ran all models with different sample specifications (e.g., excluding those who were depressed at baseline) and found that the overall findings were generally the same. We therefore chose to use the current sample specification (including those who had partially missing data due to death/nonresponse) because it retained most of the original sample. Furthermore, we initially included other covariates such as number of living children and number of living siblings as potential confounders, but estimated coefficients were not statistically significant. The remaining covariates were retained based on model fit criteria (i.e., AIC and BIC), as well as their ability to capture a set of key dimensions widely believed to influence mental health outcomes (i.e., SES, social relationships, physical health outcomes).
Results
Table 1 describes the sample at baseline, by gender. We used Wald tests to determine whether gender differences in each of the variables were statistically significant. For social participation, women were more likely than men to participate in a weekly religious group activity and have had grandparenting duties in the past year. In terms of labor participation, women were less likely to be involved in paid labor and to be retired, but more likely to work for family without pay or be economically inactive. These results align with previous studies and reflect traditional gender role expectations in Asia, where women often take on the role as primary family caregiver within the home and men go out to work as breadwinner of the family. Furthermore, socioeconomic and health factors were distributed differently by gender, with women being significantly more disadvantaged compared with men. Women were less likely than men to have graduated from high school, less likely to be partnered, and had lower levels of income compared with men. They also had a higher prevalence of heart-related disease, higher depressive symptom scores, and were less likely to exercise at least once a week relative to men. Figure 1 illustrates the unconditional growth curve models (i.e., without any covariates) for both dependent variables across the four waves. Across both outcomes, models show that women are more likely than men to experience cognitive impairment/depression at every time point.
Table 1.
Summary Statistics of Key Variables (n = 2,573).
| Proportion or mean (SD)a |
||
|---|---|---|
| Variable name | Menb (n = 1,426) | Women (n = 1,147) |
| Dependent variable | ||
| Cognitively impaired at W4 (2012) | 28.60 | 42.02 |
| Depressed at W4 (2012) | 26.09 | 37.59 |
| Social participation | ||
| Formal | ||
| Participated at least once a week in … (1 = yes; 0 = no) | ||
| Formal social activityc | 15.15d | 16.79 |
| Religious group activity | 14.10 | 23.78 |
| Informal | ||
| Frequent meetings with family and friends at least once a week (1 = yes; 0 = no) | 63.32d | 69.94 |
| Grandparenting in the past year (1 = yes; 0 = no) | 4.90 | 12.38 |
| Labor participation | ||
| Paid | ||
| Full-time, part-time, and self-employed | 43.42 | 11.36 |
| Unpaid | ||
| Work for family without pay | 0.70 | 5.85 |
| Retired (reference group) | 37.55 | 19.48 |
| Economically inactive (disabled/unemployed/not in the labor force) | 18.32 | 63.30 |
| Covariates | ||
| Age (range 60–91 years in W1) | 66.63 (5.82)d | 66.40 (5.65) |
| Less than high school (1 = yes; 0 = no) | 55.75 | 83.47 |
| Marital status (1 = partnered; 0 = nonpartnered) | 92.15 | 66.85 |
| Log total annual household income | 1.75 (2.19) | 1.36 (2.47) |
| Living alone (1 = yes; 0 = no) | 4.06 | 15.14 |
| Living in rural areas (1 = yes; 0 = no) | 28.08d | 24.46 |
| Heart-related disease (1 = yes; 0 = no) | 34.37 | 45.22 |
| Number of ADL | 0.03 (0.29)d | 0.03 (0.26) |
| Exercise at least once a week (1 = yes; 0 = no) | 47.81 | 40.66 |
Note. ADL = activities of daily living.
At baseline, using all available observations, unless otherwise stated.
Statistically significantly different from women, unless otherwise stated.
Activities considered include participation in senior community centers, educational/cultural/sports programs, alumni society, volunteer groups, and political groups.
Statistically not different from women.
Do social and labor participation independently predict cognitive impairment and depression?
Tables 2 and 3 illustrate coefficients (in odds ratios [OR]) from growth curve models predicting onset of cognitive impairment. These ORs relate to the intercept (and not the slope) and therefore characterize time-invariant associations between the independent variables and the outcome (depression/cognitive impairment). Throughout both tables, coefficients from Model 1 (social only) and Model 2 (labor only) remained fairly consistent (in the size/direction of the coefficient and p-values) even after controlling for both types of activity participation (Model 3), demonstrating that effects from social and labor activity on cognitive impairment are independent from one another. Model fit indices also showed that the full model was preferable, high-lighting the need to consider both types of activity participation together. Tables 3 and 4 display the results from growth curve models predicting risk of depression. Similar to the results from cognitive impairment, model fit was improved by considering both social and labor activities together, and coefficients were consistent across the models.
Table 2.
Results of Estimating the Role of Social and Labor Activities on the Onset of Cognitive Impairment Using Growth Curve Models for Men, KLoSA 2006–2012.
| Men (n = 4,627 person-year observations) |
|||
|---|---|---|---|
| Variables | Model 1 | Model 2 | Model 3 |
| Social participation | |||
| Formal social activity | 1.48* | — | 1.45* |
| Religious group activity | 0.91 | — | 0.96 |
| Grandparenting | 0.90 | — | 0.84 |
| Frequent meetings with family and friends | 0.57** | — | 0.59** |
| Labor participation | |||
| Retired (reference group) | — | — | — |
| Paid work | — | 0.67† | 0.68† |
| Unpaid work (for family)a | — | 0.03** | 0.03** |
| Economically inactivea | — | 1.37 | 1.31 |
| Covariates | |||
| Age | 1.14*** | 1.13*** | 1.13*** |
| Less than high school | 3.44*** | 3.39*** | 3.43*** |
| Partnered | 0.80 | 0.87 | 0.85 |
| Total household income (logged) | 1.10 | 1.15* | 1.13* |
| Living alone | 1.04 | 1.11 | 1.06 |
| Living in rural areas | 0.85 | 0.85 | 0.92 |
| Nonresponse | 2.43** | 2.39** | 2.38** |
| Death | 2.25** | 2.22** | 2.16* |
| Heart-related disease | 1.16 | 1.13 | 1.13 |
| ADL | 3.03*** | 2.99*** | 2.92*** |
| Weekly exercise | 0.63** | 0.58** | 0.59** |
| Depressed | 2.82*** | 2.81*** | 2.69*** |
| Fit indices | |||
| AIC | 3,707,117 | 3,703,705 | 3,686,014 |
| BIC | 3,707,246 | 3,703,827 | 3,686,162 |
Note. Coefficients presented are in odds ratios. KLoSA = Korean Longitudinal Study of Aging; ADL = activities of daily living; AIC = Akaike information criterion; BIC = Bayesian information criterion.
Statistically significant gender differences in the coefficients were found through interaction terms.
p < .10.
p < .05.
p < .01.
p < .001 (tests are two-tailed).
Table 3.
Results of Estimating the Role of Social and Labor Participation on the Onset of Cognitive Impairment Using Growth Curve Models for Women, KLoSA 2006–2012.
| Women (n = 3,775 person-year observations) |
|||
|---|---|---|---|
| Variables | Model 1 | Model 2 | Model 3 |
| Social participation | |||
| Formal social activity | 0.92 | — | 0.89 |
| Religious group activity | 0.70† | — | 0.66* |
| Grandparenting | 1.40 | — | 1.40 |
| Frequent meetings with family and friends | 0.71† | — | 0.70† |
| Labor participation | |||
| Retired (reference group) | — | — | — |
| Paid work | — | 0.53† | 0.50* |
| Unpaid work (for family)a | — | 0.49† | 0.47† |
| Economically inactivea | — | 0.7l† | 0.67* |
| Covariates | |||
| Age | 1.19*** | 1.18*** | 1.19*** |
| Less than high school | 2.81*** | 3.10*** | 2.99*** |
| Partnered | 1.12 | 1.13 | 1.14 |
| Total household income (logged) | 1.01 | 1.03 | 1.03 |
| Living alone | 1.07 | 1.04 | 1.09 |
| Living in rural areas | 1.48† | 1.60* | 1.65* |
| Nonresponse | 2.05* | 2.02* | 2.07** |
| Death | 1.00 | 0.85 | 0.91 |
| Heart-related disease | 2.05* | 2.02* | 2.07** |
| ADL | 1.84* | 1.90* | 1.86* |
| Weekly exercise | 0.72 | 0.68* | 0.69* |
| Depressed | 3.12*** | 3.14*** | 3.04*** |
| Fit indices | |||
| AIC | 3,766,445 | 3,771,187 | 3,754,397 |
| BIC | 3,766,570 | 3,771,305 | 3,754,540 |
Note. Coefficients presented are in odds ratios. KLoSA = Korean Longitudinal Study of Aging; ADL = activities of daily living; AIC = Akaike information criterion; BIC = Bayesian information criterion.
Statistically significant gender differences in the coefficients were found through interaction terms.
p < .10.
p < .05.
p < .01.
p < .001 (tests are two-tailed).
Table 4.
Results of Estimating the Role of Social and Labor Participation on the Risk of Depression Using Growth Curve Models for Men, KLoSA 2006–2012.
| Men (n = 4,627 person-year observations) |
|||
|---|---|---|---|
| Variables | Model 1 | Model 2 | Model 3 |
| Social participation | |||
| Formal social activity | 1.34† | — | 1.31† |
| Religious group activity | 1.06 | — | 1.10 |
| Grandparenting | 1.22 | — | 1.11 |
| Frequent meetings with family and friends | 0.52*** | — | 0.55** |
| Labor participation | |||
| Retired (reference group) | — | — | — |
| Paid work | — | 0.57*** | 0.59** |
| Unpaid work (for family) | — | 0.26† | 0.25† |
| Economically inactivea | — | 2.04*** | 1.99*** |
| Covariates | |||
| Age | 1.03* | 1.02 | 1.02† |
| Less than high school | 1.38* | 1.36* | 1.35* |
| Partnered | 0.27*** | 0.29*** | 0.29*** |
| Total household income (logged) | 0.91* | 0.96 | 0.95 |
| Living alone | 0.92 | 0.93 | 0.93 |
| Living in rural areas | 1.10 | 1.07 | 1.20 |
| Nonresponse | 1.28 | 1.31 | 1.29 |
| Death | 1.91** | 1.90** | 1.83** |
| Heart-related disease | 0.91 | 0.90 | 0.89 |
| ADL | 2.43*** | 2.40*** | 2.30*** |
| Weekly exercise | 0.79* | 0.70** | 0.72** |
| Cognitively impaired | 2.96*** | 2.88*** | 2.77*** |
| Fit indices | |||
| AIC | 5,913,698 | 5,871,353 | 5,834,851 |
| BIC | 5,913,833 | 5,871,481 | 5,835,006 |
Note. Coefficients presented are in odds ratios. KLoSA = Korean Longitudinal Study of Aging; ADL = activities of daily living; AIC = Akaike information criterion; BIC = Bayesian information criterion.
Statistically significant gender differences in the coefficients were found through interaction terms.
p < .10.
p < .05.
p < .01.
p < .001 (tests are two-tailed).
Are there gender differences?
For cognitive impairment (men in Table 2 and women in Table 3)—among social activities, having frequent interaction with family/friends/relatives was protective against cognitive impairment for both men and women (Model 3: OR = 0.59, p < .01 for men; OR = 0.70, p < .10 for women). Formal social participation was found to be deleterious for men (OR = 1.45, p < .05), but not for women. Religious group activity was significantly protective for women (OR = 0.66, p < .05) and not for men, but further statistical testing indicates that the coefficient of religious group activity on cognitive impairment among women was not significantly different from that among men. For labor participation, those who were engaged in unpaid work were less likely than those who were retired (i.e., the reference group) to become cognitively impaired, and this effect was significantly stronger among men (OR = 0.03, p < .01) compared with women (OR = 0.47, p < .10). It is worth noting, however, that very few men in our sample (~1%) were engaged in unpaid work. Paid work was similarly protective for both men (OR = 0.68, p < .10) and women (OR = 0.50, p < .05). Being economically inactive was beneficial for women (OR = 0.67, p < .05), but not for men.
For depression (men in Table 4 and female in Table 5), frequent interaction with family and friends was also protective against depressive symptoms for both men (OR = 0.55, p < .01) and women (OR = 0.53, p < .001). Furthermore, formal social activity was associated with a higher risk of depression for both men (OR = 1.31, p < .10) and women (OR = 1.34, p < .05). For labor participation, being involved in paid work was protective for both men (OR = 0.59, p < .01) and women (OR = 0.54, p < .01) even after adjusting for social participation. Being economically inactive, however, led to a higher risk of being depressed (OR = 1.99, p < .001) for men, but not for women (OR = 0.78, p < .10). Doing unpaid work for family was marginally significantly protective for both men and women.
Table 5.
Results of Estimating the Role of Social and Labor Participation on the Risk of Depression Using Growth Curve Models for Women, KLoSA 2006–2012.
| Women (n = 3,775 person-year observations) |
|||
|---|---|---|---|
| Variables | Model 1 | Model 2 | Model 3 |
| Social participation | |||
| Formal social activity | 1.37* | — | 1.34* |
| Religious group activity | 0.83 | — | 0.80 |
| Grandparenting | 1.10 | — | 1.07 |
| Frequent meetings with family and friends | 0.53*** | — | 0.53*** |
| Labor participation | |||
| Retired (reference group) | — | — | — |
| Paid work | — | 0.57* | 0.54** |
| Unpaid work (for family) | — | 0.49† | 0.50† |
| Economically inactivea | — | 0.83 | 0.78† |
| Covariates | |||
| Age | 1.01 | 1.01 | 1.01 |
| Less than high school | 1.47 | 1.56* | 1.53* |
| Partnered | 0.66* | 0.68* | 0.67* |
| Total household income (logged) | 0.92* | 0.93† | 0.93* |
| Living alone | 1.46† | 1.44 | 1.49† |
| Living in rural areas | 1.00 | 1.05 | 1.10 |
| Nonresponse | 0.79 | 0.78 | 0.79 |
| Death | 1.78 | 1.59 | 1.67 |
| Heart-related disease | 1.46** | 1.42* | 1.44* |
| ADL | 1.67** | 1.71** | 1.68** |
| Weekly exercise | 0.57*** | 0.54*** | 0.55*** |
| Cognitively impaired | 2.95*** | 3.00*** | 2.89*** |
| Fit indices | |||
| AIC | 5,528,101 | 5,558,794 | 5,512,311 |
| BIC | 5,528,232 | 5,558,919 | 5,512,461 |
Note. Coefficients presented are in odds ratios. KLoSA = Korean Longitudinal Study of Aging; ADL = activities of daily living; AIC = Akaike information criterion; BIC = Bayesian information criterion.
Statistically significant gender differences in the coefficients were found through interaction terms.
p < .10.
p < .05.
p < .01.
p < .001.
Discussion
We highlight five main findings from our study. First, we found that both men and women participated in productive activities to some extent, but generally in different types of activities which reflected the traditional division of labor. Second, results from growth curve models assessing the simultaneous effects of social and labor participation indicate that each type of participation is independently associated with mental health. Third, among other variables, social gatherings with family and friends and paid work were particularly beneficial for mental health for both men and women. Fourth, some of the effects of social participation varied by gender, and not all social activities were beneficial. Men who participated in formal social groups had higher risk of cognitive impairment, but there was little to no effect for women. Women who attended religious services had lower risk of cognitive impairment, and we did not find this relationship among men. Fifth, inability to work was associated with adverse health consequences, especially depression, whereas unpaid work reduces risk of cognitive impairment. These associations were more salient among men.
What mechanisms could possibly explain the gender differences in the association between labor participation and mental health? First, the theory of role identification (Haslam et al. 2014; Turner 1978) could account for why the effect of labor participation may provide stronger health advantages and disadvantages (when they are unable to work) for Korean men. Role identification theory is often used to explain how performance of social roles through engagement in productive activity may afford individual access to psychosocial resources that buffer against adverse mental outcomes (Hinterlong et al. 2007). According to this theory, Korean older men who participate in paid work may continue to maintain their social roles as breadwinners, which enhances a sense of belonging to the family and society as well as meaning in life; whereas separation from or inability to work may threat men’s willingness to continue traditional roles as breadwinners and damage their sense of self-mastery. We observed the opposite pattern for women—lower risk of cognitive impairment and depression for those who are economically inactive. This may be, in part, because those women who did not have to work are likely from families with higher levels of social standing—granting them resources such as access to preventive health care and other health advantages. Second, we recognize that, similar to paid work, working for family without pay also lowers the risk of cognitive impairment for men. It is possible that providing assistance to family in old age may help maintain their self-esteem by making them feel useful (Rowe and Kahn 1997). Providing assistance to family may also reconnect men to their family and become a source of social support through increased interactions with family members. Third, the cognitive reserve model may help explain the way in which labor participation may confer cognitive benefits for women (Tucker and Stern 2011). The cognitive reserve model explains how aspects of life such as employment may protect against dementia and Alzheimer’s disease by increasing skills or repertoires of coping strategies that conserve cognitive functioning. Despite limited access to education and employment for Korean older women throughout their life course, our results show that women are less likely to be cognitively impaired and depressed if they participate in paid work in later life. This suggests that, regardless of social disadvantages that Korean older women may have faced due to lack of early life experiences and opportunities, working in later life may still protect against poor mental health by increasing levels of mental demands and skills that preserve cognition.
Although not hypothesized, formal social participation such as religious group activity was found to be more important for women’s health compared with men’s. This may be because women find this as an opportunity to take a break from their traditional role by engaging in different social circles beyond their families that can be mentally stimulating and rewarding (Jung 2014). It is also possible that women tend to form informal social networks with members of religious groups that could be sources of support and protection. The theory of resource substitution suggests that women may rely on this alternative resource for their well-being to cope with their disadvantaged conditions or statuses. As indicated by social network theory, members of religious groups may share advice, influence, and information (Son and Lin 2008), providing surveillance of behaviors and access to resources from others in the network, which can diversify resources for older women and benefit their health.
We find that formal social participation increases the probabilities of developing cognitive impairment and depression over time. Although this may be surprising in light of a large literature in the West on the positive health consequences of formal social participation, there is some empirical evidence in support of the finding found in Asian contexts. A recent study conducted among Singaporean older adults found a detrimental effect of formal social participation on health outcomes (Ang 2016, 2018), suggesting that formal social participation may exhibit different associations with older adult health within Asian contexts. One possible explanation for this is that institutions in Korea (and Singapore) may tend to be overly hierarchical and/or legalistic, often making it unpleasant to deal with formal organizations (or organizers) who may not empathize with older adults (Suen and Thang 2018). It is also possible that volunteering in Korea, for instance, may simply be an arena for the “young-old” to provide care for the “old-old” in the absence of sufficient support from children, in contrast to Western settings where volunteering usually connotes positive experiences such as skill training and formal group activity (Carr 2018; Thoits and Hewitt 2001). As mentioned in a study conducted among Chinese older adults (Li et al. 2014), this may be partly because formal social participation such as civic engagement and volunteering is underdeveloped within the Asian cultural context (especially among older cohorts), in contrast to the West. Future studies disaggregating the effects of formal social participation and disentangling the specific activities that are most consequential for the health of Korean older adults could investigate this possibility.
One strength of this study is that we extend the concept of “activity” for older adults. Building on social engagement theory and the successful aging model, we elected to assess labor together with social participation as later-life productive contexts. Our findings—the independent effects of social and labor participation on onset of cognitive impairment and depression—clarify possible contexts in which daily activities of older adults are situated. Although our findings are in agreement with previous reports that results have considered both social and labor participation (Luoh and Herzog 2002; Wang et al. 2002), no study yet has examined this in the context of Korea. Unlike the traditional expectation that older adults leave the labor market after retirement age, our results showed that a substantial percentage of Korean older adults are in fact actively engaged in the labor market. The proportion of employed older adults in our study sample was much higher than adults aged 65 years and older in the United States (43.42% for men in Korea; 22.1% for men in the United States: U.S. Census Bureau 2011). This may be related to the recent increase in the minimum retirement age (mandated retirement age at age of 60 years), emphasizing workforces in Korea will gradually shift toward older employees. Despite the apparent growth of senior labor force participation, less attention has been given to the potential role of labor participation in health thus far. To our knowledge, our study is one of the first large, population-based studies assessing both measures of social and labor participation while disentangling their differential impacts on mental health in Korea.
We acknowledge several limitations in our study. First, although we observed parsimonious effects of paid work—that is, the directions of the coefficients are consistent for both cognition and depression outcomes—the results should be interpreted with caution. Paid work in KLoSA was self-reported, without much elaboration on job characteristics (high vs. low levels of mental demands). One may suspect that the health effect for someone who works manual labor would be different from workers who perform professional jobs, because different occupations require different levels of cognitive skills and mental involvement. This may, in turn, result in different trajectories of health by job characteristics. Occupational classifications and their associations with health therefore need further exploration. Second, as our analytic sample contains only those who were not cognitively impaired at baseline, the observed results are not specific to the entire Korean population. Third, unobserved variables such as social support and distress may potentially confound the association between activity participation and the mental health of older adults, but KLoSA does not assess these psychosocial characteristics. Finally, although our models controlled for a variety of demographic and health-related risk factors that are commonly related to both outcomes, it is worth nothing that unmeasured biological risks may contribute to each outcome differently.
We conclude that continued engagement in social and labor participation benefits the mental health of Korean older adults, but interpretation of these effects should be gender-specific. By considering the specific cultural context in which health decrements take root, our findings provide evidence that gendered patterns of activity participation may have different consequences for cognitive and mental functioning. This highlights that gender-specific assessments of activity participation may foster the early identification and treatment of mental health problems. The beneficial effect of labor participation, whether paid or unpaid, suggests that a national aging strategy in Korea should explore the ways to promote and prolong older adults’ participation in working beyond the traditional retirement age. To do that, working environments that are older-adults-friendly should be established by protecting employees from age discrimination and loosening the strict enforcement of mandatory retirement. Furthermore, a program that strengthens and expands training opportunities for older workers may be a key component of motivating them to continue to work beyond retirement age.
Acknowledgments
The authors are grateful to Jacqui Smith and Lindsay Ryan for their feedback on a prior version of this manuscript and the anonymous reviewers for their helpful comments. Data were made available by the Gateway to Global Aging Data Aging Project, the Center for Economic and Social Research, University of Southern California. The Gateway Project bears no responsibility for the analyses or interpretations presented here.
Funding
The author(s) disclosed receipt of the following financial support for research, authorship, and/or publication of this article: This work was supported by an NIH/NIA training grant at the University of Southern California (T32AG000037). The Gateway to Global Aging Data Aging Project was funded by National Institute on Aging, National Institutes of Health (R01 AG030153, RC2 AG036619, R03 AG043052, and R24 AG048024). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health and National Institute on Aging.
Biographies
Author Biographies
Haena Lee is a National Institute on Aging Postdoctoral fellow in Gerontology at the University of Southern California. Her research focuses on social inequality and health across the life course with particular interests in childhood adversity, neighborhood context, and health disparities by race and gender. Her work has been published in journals such as The Gerontologist, Journals of Gerontology: Social Sciences, and Journal of Aging and Health.
Shannon Ang is a PhD candidate in the Department of Sociology at University of Michigan. His interests lie at the intersection of aging, social relationships, and health. His work has been published in journals such as Social Science and Medicine, Journals of Gerontology Series B: Psychological and Social Sciences, and Aging and Mental Health, among other journals.
Appendix A
Figure A1.
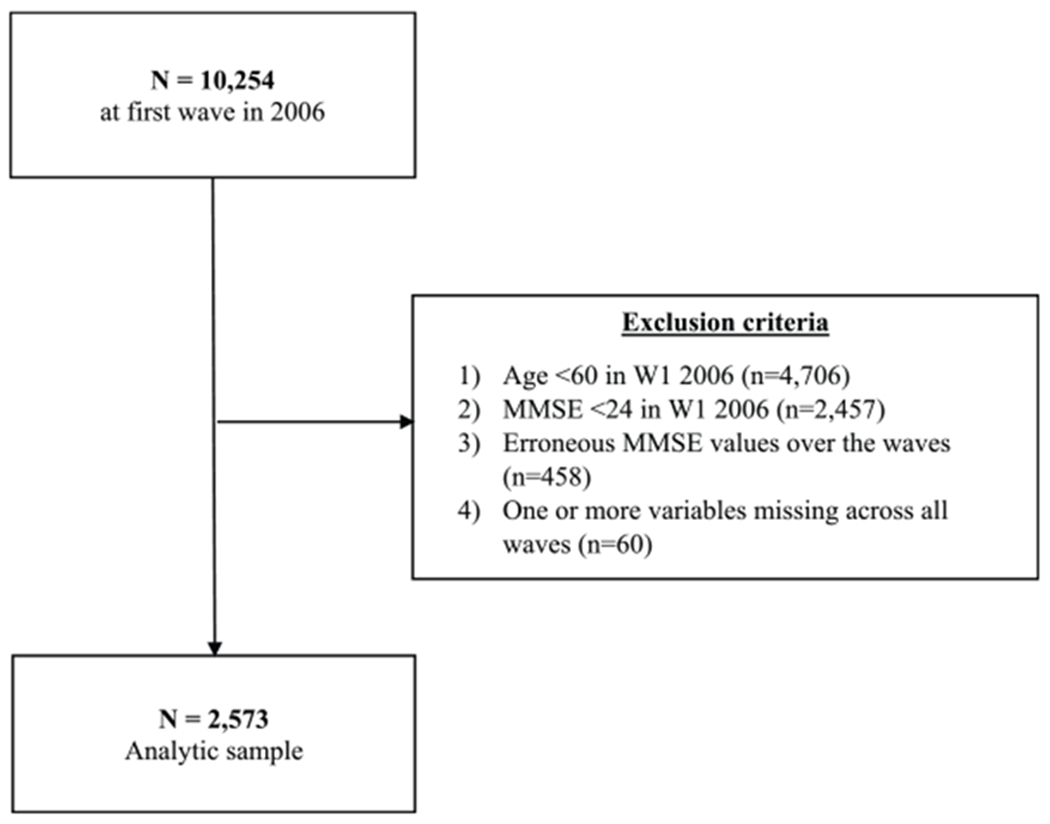
Attrition chart.
Note. MMSE = Mini-Mental State Examination.
Appendix B
Results from Pooled Models Prediction Cognitive Impairment and Depression.
| Overall (n = 8,402 person-year observations) |
||||
|---|---|---|---|---|
| Variables | Cognitive impairment | Cognition impairment with interactions | Depression | Depression with interactions |
| Social participation | ||||
| Formal social activity | 1.14 | 1.46* | 1.30* | 1.24 |
| Religious group activity | 0.82 | 0.95 | 0.93 | 1.08 |
| Grandparenting | 1.23 | 0.83 | 1.08 | 1.16 |
| Frequent meetings with family and friends | 0.65** | 0.58** | 0.55*** | 0.59*** |
| Labor participation | ||||
| Retired (reference group) | ||||
| Paid work | 0.55*** | 0.68 | 0.51*** | 0.61*** |
| Unpaid work (for family) | 0.66 | 0.03** | 0.61 | 0.30† |
| Economically inactive | 1.01 | 1.31 | 1.16 | 1 87*** |
| Interaction terms | ||||
| Formal Social Activity × Female | — | 0.62† | — | 1.06 |
| Religious Group Activity × Female | — | 0.70 | — | 0.74 |
| Grandparenting × Female | — | 1.67 | — | 0.88 |
| Frequent Meetings with Family and Friends × Female | — | 1.23 | — | 0.95 |
| Paid Work (Full-time/part-time/self-employed) × Female | — | 0.74 | — | 0.91 |
| Unpaid Work (for family) × Female | — | 15.32* | — | 1.77 |
| Economically Inactive × Female | — | 0.52* | — | 0 42*** |
| Fit indices | ||||
| AIC | 7,514,798 | 7,442,541 | 11,439,781 | 11,395,456 |
| BIC | 7,514,960 | 7,442,850 | 11,439,949 | 11,395,766 |
Note. Coefficients presented are in odds ratios. All models are fully adjusted for covariates. AIC = Akaike Information Criterion; BIC = Bayesian Information Criterion.
p < .10.
p < .05.
p < .01.
p < .001 (tests are two-tailed).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Adams Kathryn Betts, Leibbrandt Sylvia, and Moon Heehyul. 2011. “A Critical Review of the Literature on Social and Leisure Activity and Wellbeing in Later Life.” Ageing & Society 31(4):683–712. [Google Scholar]
- Ang Shannon. 2016. “Social Participation and Mortality among Older Adults in Singapore: Does Ethnicity Explain Gender Differences?” The Journals of Gerontology Series B: Psychological Sciences & Social Sciences 73:1470–79. [DOI] [PubMed] [Google Scholar]
- Ang Shannon. 2018. “How Social Participation Benefits the Chronically Ill: Self-management as a Mediating Pathway.” Journal of Aging and Health 31:1134–54. [DOI] [PubMed] [Google Scholar]
- Berkman Lisa F. and Glass Thomas. 2000. “Social Integration, Social Networks, Social Support, and Health.” Social Epidemiology 1:137–73. [Google Scholar]
- Burr Jeffrey A., Mutchler Jan E., and Caro Francis G.. 2007. “Productive Activity Clusters among Middle-aged and Older Adults: Intersecting Forms and Time Commitments.” The Journals of Gerontology Series B: Psychological Sciences & Social Sciences 62(4):267–75. [DOI] [PubMed] [Google Scholar]
- Cacioppo John T. and Hawkley Louise C.. 2009. “Perceived Social Isolation and Cognition.” Trends in Cognitive Sciences 13(10):447–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson Michelle C., Saczynski Jane S., Rebok George W., Seeman Teresa, Glass Thomas A., Sylvia McGill James Tielsch, Frick Kevin D., Hill Joel, and Fried Linda P.. 2008. “Exploring the Effects of an ‘Everyday’ Activity Program on Executive Function and Memory in Older Adults: Experience Corps®.” The Gerontologist 48(6):793–801. [DOI] [PubMed] [Google Scholar]
- Carr Deborah. 2018. “Volunteering among Older Adults: Life Course Correlates and Consequences.” The Journals of Gerontology Series B: Psychological Sciences & Social Sciences 73:479–81 [DOI] [PubMed] [Google Scholar]
- Chen Yixin and Thomas Hugh Feeley. 2014. “Social Support, Social Strain, Loneliness, and Well-being among Older Adults an Analysis of the Health and Retirement Study*.” Journal of Social and Personal Relationships 31(2):141–61. [Google Scholar]
- Choi Young, Park Sohee, Kyoung Hee Cho Sung-Youn Chun, and Park Eun-Cheol. 2016. “A Change in Social Activity Affect Cognitive Function in Middle-aged and Older Koreans: Analysis of a Korean Longitudinal Study on Aging (2006-2012).” International Journal of Geriatric Psychiatry 31(8):912–19. [DOI] [PubMed] [Google Scholar]
- Cohen Sheldon. 2004. “Social Relationships and Health.” American Psychologist 59(8):676–84. [DOI] [PubMed] [Google Scholar]
- Cornwell Erin York and Waite Linda J.. 2009. “Social Disconnectedness, Perceived Isolation, and Health among Older Adults.” Journal of Health and Social Behavior 50(1):31–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher Gwenith G., Stachowski Alicia, Infurna Frank J., Faul Jessica D., Grosch James, and Tetrick Lois E.. 2014. “Mental Work Demands, Retirement, and Longitudinal Trajectories of Cognitive Functioning.” Journal of Occupational Health Psychology 19(2):231–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flatt Jason D. and Hughes Tiffany F.. 2013. “Participation in Social Activities in Later Life: Does Enjoyment Have Important Implications for Cognitive Health?” Aging Health 9(2):149–58. [Google Scholar]
- Flochel Thomas, Ikeda Yuki, Moroz Harry, and Umapathi Nithin. 2015. “Macroeconomic Implications of Aging in East Asia Pacific: Demography, Labor Markets and Productivity.” (http://documents.world-bank.org/curated/en/869291468189255308/Macroeconomic-implications-of-aging-in-East-Asia-Pacific-demography-labor-markets-and-productivity). [Google Scholar]
- Folstein Marshal F., Folstein Susan E., and McHugh Paul R.. 1975. “‘Mini-mental State’: A Practical Method for Grading the Cognitive State of Patients for the Clinician.” Journal of Psychiatric Research 12(3):189–98. [DOI] [PubMed] [Google Scholar]
- Giles John, Wang Dewen, and Cai Wei. 2012. “The Labor Supply and Retirement Behavior of China’s Older Workers and Elderly in Comparative Perspective.” National Academies Press; Retrieved November 19, 2019 (http://documents.worldbank.org/curated/en/863881468021633654/The-labor-supply-and-retirement-behavior-of-Chinas-older-workers-and-elderly-in-comparative-perspective). [Google Scholar]
- Glass Thomas A., Mendes De Leon Carlos F., Bassuk Shari S., and Berkman Lisa F.. 2006. “Social Engagement and Depressive Symptoms in Late Life: Longitudinal Findings.” Journal of Aging and Health 18(4):604–28. [DOI] [PubMed] [Google Scholar]
- Glei Dana A., Landau David A., Goldman Noreen, Chuang Yi-Li, Rodríguez Germán, and Weinstein Maxine. 2005. “Participating in Social Activities Helps Preserve Cognitive Function: An Analysis of a Longitudinal, Population-based Study of the Elderly.” International Journal of Epidemiology 34(4):864–71. [DOI] [PubMed] [Google Scholar]
- Greenfield Emily A. and Marks Nadine F.. 2004. “Formal Volunteering as a Protective Factor for Older Adults’ Psychological Well-being.” The Journals of Gerontology Series B: Psychological Sciences & Social Sciences 59(5):258–64. [DOI] [PubMed] [Google Scholar]
- Harris Alex H. S. and Thoresen Carl E.. 2005. “Volunteering Is Associated with Delayed Mortality in Older People: Analysis of the Longitudinal Study of Aging.” Journal of Health Psychology 10(6):739–52. [DOI] [PubMed] [Google Scholar]
- Haslam Catherine, Cruwys Tegan, and Alexander Haslam S. 2014. “‘The We’s Have It’: Evidence for the Distinctive Benefits of Group Engagement in Enhancing Cognitive Health in Aging.” Social Science & Medicine 120:57–66. [DOI] [PubMed] [Google Scholar]
- Hinterlong James E., Morrow-Howell Nancy, and Rozario Philip A.. 2007. “Productive Engagement and Late Life Physical and Mental Health: Findings from a Nationally Representative Panel Study.” Research on Aging 29(4):348–70. [Google Scholar]
- Hsu Hui-Chuan. 2005. “Gender Disparity of Successful Aging in Taiwan.” Women & Health 42(1):1–21. [DOI] [PubMed] [Google Scholar]
- Jang Soong-Nang, Cho Sung-Il, Chang Jiyeun, Boo Kachung, Shin Hyun-Goo, Lee Hyejung, and Berkman Lisa F.. 2009. “Employment Status and Depressive Symptoms in Koreans: Results from a Baseline Survey of the Korean Longitudinal Study of Aging.” Journals of Gerontology Series B: Psychological Sciences & Social Sciences 64(5):677–83. [DOI] [PubMed] [Google Scholar]
- Jung Jong Hyun. 2014. “Religious Attendance, Stress, and Happiness in South Korea: Do Gender and Religious Affiliation Matter?” Social Indicators Research 118(3):1125–45. [Google Scholar]
- Kang Mo-Yeol, Kang Young-Joong, Lee Woncheol, and Yoon Jin-Ha. 2016. “Does Long-term Experience of Nonstandard Employment Increase the Incidence of Depression in the Elderly?” Journal of Occupational Health 58(3):247–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kang Yeonwook, Na Duk L., and Hahn Seunghae. 1997. “A validity study on the Korean Mini-Mental State Examination (K-MMSE) in Dementia Patients.” J Korean Neurol Assoc 15(2):300–308. [Google Scholar]
- Katagiri Keiko and Kim Ju-Hyun. 2018. “Factors Determining the Social Participation of Older Adults: A Comparison between Japan and Korea Using EASS 2012.” PLoS ONE 13(4):e0194703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keese Mark. 2006. Live Longer, Work Longer. Organisation for Economic Co-operation and Development; Retrieved November 19, 2019 (http://www.oecd.org/employment/livelongerworklonger.htm). [Google Scholar]
- Kim DaeHyun, Arai Hidenori, and Kim SungHi. 2017. “Social Activities Are Associated with Cognitive Decline in Older Koreans.” Geriatrics & Gerontology International 17(8):1191–96. [DOI] [PubMed] [Google Scholar]
- Kim Gyu Ri, Sun Jiyu, Han Minkyung, Chung Mo Nam, and Sohee Park. 2019. “Evaluation of the Directional Relationship between Handgrip Strength and Cognitive Function: The Korean Longitudinal Study of Ageing.” Age and Ageing 48(3):426–32. [DOI] [PubMed] [Google Scholar]
- Kim Ki Woong, Joon Hyuk Park Myoung-Hee Kim, Moon Doo Kim Bong-Jo Kim, Kim Shin-Kyum, Jeong Lan Kim Seok Woo Moon, Jae Nam Bae Jong Inn Woo, Ryu Seung-Ho, Jong Chul Yoon Nam Jin Lee, Dong Young Lee Dong Woo Lee, Seok Bum Lee Jung Jae Lee, Lee Jun-Young, Lee Chang-Uk, Sung Man Chang Jin Hyeong Jhoo, and Maeng Je Cho. 2011. “A Nationwide Survey on the Prevalence of Dementia and Mild Cognitive Impairment in South Korea.” Journal of Alzheimer’s Disease 23(2):281–91. [DOI] [PubMed] [Google Scholar]
- Klassen Thomas R. and Yang Yunjeong. 2013. Korea’s Retirement Predicament: The Ageing Tiger. Vol. 28 New York: Routledge. [Google Scholar]
- Kohout Frank J., Berkman Lisa F., Evans Denis A., and Joan Comoni-Huntley. 1993. “Two Shorter Forms of the CES-D Depression Symptoms Index.” Journal of Aging and Health 5(2):179–93. [DOI] [PubMed] [Google Scholar]
- Kwon Soonman. 2008. “Future of Long-term Care Financing for the Elderly in Korea.” Journal of Aging & Social Policy 20(1):119–36. [DOI] [PubMed] [Google Scholar]
- Lee EunKyoung Othelia and Lee Jungui. 2011. “Gender Differences in Predictors of Mental Health among Older Adults in South Korea.” The International Journal of Aging and Human Development 72(3):207–23. [DOI] [PubMed] [Google Scholar]
- Lee Hyo Young, Jang Soong-Nang, Lee Seonja, Cho Sung-Il, and Park Eun-Ok. 2008. “The Relationship between Social Participation and Self-rated Health by Sex and Age: A Cross-sectional Survey.” International Journal of Nursing Studies 45(7):1042–54. [DOI] [PubMed] [Google Scholar]
- Lee Jaerim and Bauer Jean W.. 2013. “Motivations for Providing and Utilizing Child Care by Grandmothers in South Korea.” Journal of Marriage and Family 75(2):381–402. [Google Scholar]
- Lee Seung Hee and Kim Young Bum. 2016. “Which Type of Social Activities May Reduce Cognitive Decline in the Elderly? A Longitudinal Population-based Study.” BMC Geriatrics 16:165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lemon Bruce W., Bengtson Vern L., and Peterson James A.. 1972. “An Exploration of the Activity Theory of Aging: Activity Types and Life Satisfaction among In-movers to a Retirement Community.” Journal of Gerontology 27(4):511–23. [DOI] [PubMed] [Google Scholar]
- Li Yawen, Xu Ling, Chi Iris, and Guo Ping. 2014. “Participation in Productive Activities and Health Outcomes among Older Adults in Urban China.” The Gerontologist 54(5):784–96. [DOI] [PubMed] [Google Scholar]
- Liang Xiaoniu, Chen Zhao, Dong Xinqi, Zhao Qianhua, Guo Qihao, Zheng Li, Deng Wei, Luo Jianfeng, and Ding Ding. 2019. “Mental Work Demands and Late-life Cognitive Impairment: Results from the Shanghai Aging Study.” Journal of Aging and Health 31(5):883–98. [DOI] [PubMed] [Google Scholar]
- Lim Young-Mee, Sa Ra Lee Eun Ji Choi, Jeong Kyungah, and Chung Hye Won. 2018. “Urinary Incontinence Is Strongly Associated with Depression in Middle-aged and Older Korean Women: Data from the Korean Longitudinal Study of Ageing.” European Journal of Obstetrics & Gynecology and Reproductive Biology 220:69–73. [DOI] [PubMed] [Google Scholar]
- Luoh Ming-Ching and Regula Herzog A. 2002. “Individual Consequences of Volunteer and Paid Work in Old Age: Health and Mortality.” Journal of Health and Social Behavior 43(4):490–509. [PubMed] [Google Scholar]
- Lyu Jiyoung and Kim Hae-Young. 2016. “Gender-specific Incidence and Predictors of Cognitive Impairment among Older Koreans: Findings from a 6-year Prospective Cohort Study.” Psychiatry Investigation 13(5):473–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Min Jin-young, Jae Bum Park Kyung-jong Lee, and Min Kyoung-bok. 2015. “The Impact of Occupational Experience on Cognitive and Physical Functional Status among Older Adults in a Representative Sample of Korean Subjects.” Annals of Occupational and Environmental Medicine 27:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ministry of Community Development, Youth and Sports. 2008. “State of the Elderly in Singapore.” (https://www.moh.gov.sg/content/dam/moh_web/Publications/Reports/2009/1/State%20of%20the%20Elderly_Release%202.pdf). [Google Scholar]
- Morrow-Howell Nancy, Putnam Michelle, Yung Soo Lee Jennifer C. Greenfield, Inoue Megumi, and Chen Huajuan. 2014. “An Investigation of Activity Profiles of Older Adults.” The Journals of Gerontology Series B: Psychological Sciences & Social Sciences 69(5):809–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nexø Mette Andersen, Meng Annette, and Borg Vilhelm. 2016. “Can Psychosocial Work Conditions Protect against Age-related Cognitive Decline? Results from a Systematic Review.” Occupational & Environmental Medicine 73(7):487–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Organisation for Economic Co-operation and Development. 2006. “Ageing and Employment Policies in Korea—The Challenge of an Ageing Population.” (http://www.oecd.org/employment/emp/33906935.pdf). [Google Scholar]
- Organisation for Economic Co-operation and Development. 2012. “Older Workers Korea.” (http://www.oecd.org/els/emp/Older%20Workers%20Korea-MOD.pdf). [Google Scholar]
- Organisation for Economic Co-operation and Development. 2014. “Education at a Glance in 2014: Korea.” (https://www.oecd.org/edu/Korea-EAG2014-Country-Note.pdf). [Google Scholar]
- Park Joon Hyuk, Ki Woong Kim Myoung-Hee Kim, Moon Doo Kim Bong-Jo Kim, Kim Shin-Kyum, Jeong Lan Kim Seok Woo Moon, Jae Nam Bae Jong Inn Woo, Ryu Seung-Ho, Jong Chul Yoon Nam-Jin Lee, Dong Young Lee Dong Woo Lee, Seok Bum Lee Jung Jae Lee, Lee Jun-Young, Lee Chang-Uk, Sung Man Chang Jin Hyeong Jhoo, and Maeng Je Cho. 2012. “A Nationwide Survey on the Prevalence and Risk Factors of Late Life Depression in South Korea.” Journal of Affective Disorders 138(1–2):34–40. [DOI] [PubMed] [Google Scholar]
- Roh Hyun Woong, Chang Hyung Hong Yunhwan Lee, Byoung Hoon Oh Kang Soo Lee, Ki Jung Chang Dae Ryong Kang, Kim Jinhee, Lee SooJin, Joung Hwan Back Young Ki Chung, Ki Young Lim Jai Sung Noh, Kim Dongsoo, and Sang Joon Son. 2015. “Participation in Physical, Social, and Religious Activity and Risk of Depression in the Elderly: A Community-based Three-year Longitudinal Study in Korea.” PLoS ONE 10(7):e0132838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ross Catherine E., Masters Ryan K., and Hummer Robert A.. 2012. “Education and the Gender Gaps in Health and Mortality.” Demography 49(4):1157–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rowe John W. and Kahn Robert L.. 1997. “Successful Aging.” The Gerontologist 37(4):433–40. [DOI] [PubMed] [Google Scholar]
- Salthouse Timothy A. 2009. “When Does Age-related Cognitive Decline Begin?” Neurobiology of Aging 30(4):507–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwingel Andiara, Niti Mathew M., Tang Catherine, and Tze Pin Ng. 2009. “Continued Work Employment and Volunteerism and Mental Well-being of Older Adults: Singapore Longitudinal Ageing Studies.” Age and Ageing 38(5):531–37. [DOI] [PubMed] [Google Scholar]
- Shin Tacksoo, Davison Mark L., and Long Jeffrey D.. 2017. “Maximum Likelihood versus Multiple Imputation for Missing Data in Small Longitudinal Samples with Nonnormality.” Psychological Methods 22(3):426–49. [DOI] [PubMed] [Google Scholar]
- Son Joonmo and Lin Nan. 2008. “Social Capital and Civic Action: A Network-based Approach.” Social Science Research 37(1):330–49. [Google Scholar]
- Sørensen Lisbeth Villemoes, Frans Boch Waldorff, and Gunhild Waldemar. 2008. “Social Participation in Home-living Patients with Mild Alzheimer’s Disease.” Archives of Gerontology and Geriatrics 47(3):291–301. [DOI] [PubMed] [Google Scholar]
- Statistics Korea. 2011. “Symptom of Depression by General Feature of Older Persons.” (http://kosis.kr/statHtml/statHtml.do?orgId=117&tblId=DT_11771_2011N043&vw_cd=MT_ETITLE&list_id=&scrId=&seqNo=&language=en&obj_var_id=&itm_id=&conn_path=E3&path=%252Feng%252Fsearch%252Fsearch01_List.jsp). [Google Scholar]
- Staudinger Ursula M., Finkelstein Ruth, Calvo Esteban, and Sivaramakrishnan Kavita. 2016. “A Global View on the Effects of Work on Health in Later Life.” The Gerontologist 56(Suppl.):2281–92. [DOI] [PubMed] [Google Scholar]
- Suen Johan and Leng Leng Thang. 2018. “Contextual Challenges and the Mosaic of Support: Understanding the Vulnerabilities of Low-income Informal Caregivers of Dependent Elders in Singapore.” Journal of Cross-Cultural Gerontology 33(2):163–81. [DOI] [PubMed] [Google Scholar]
- Sung Sirin. 2003. “Women Reconciling Paid and Unpaid Work in a Confucian Welfare State: The Case of South Korea.” Social Policy & Administration 37(4):342–60. [Google Scholar]
- Thoits Peggy A. 2011. “Mechanisms Linking Social Ties and Support to Physical and Mental Health.” Journal of Health and Social Behavior 52(2):145–61. [DOI] [PubMed] [Google Scholar]
- Thoits Peggy A. and Hewitt Lyndi N.. 2001. “Volunteer Work and Well-being.” Journal of Health and Social Behavior 42:115–31. [PubMed] [Google Scholar]
- Thomas Patricia A. 2011. “Gender, Social Engagement, and Limitations in Late Life.” Social Science & Medicine 73(9):1428–35. [DOI] [PubMed] [Google Scholar]
- Tucker Adrienne M. and Stern Yaakov. 2011. “Cognitive Reserve in Aging.” Current Alzheimer Research 8(4):354–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turner Ralph H. 1978. “The Role and the Person.” American Journal of Sociology 84(1):1–23. [Google Scholar]
- U.S. Census Bureau. 2011. “Labor Force Statistics.” [Google Scholar]
- Utz Rebecca L., Carr Deborah, Nesse Randolph, and Wortman Camille B.. 2002. “The Effect of Widowhood on Older Adults’ Social Participation an Evaluation of Activity, Disengagement, and Continuity Theories.” The Gerontologist 42(4):522–33. [DOI] [PubMed] [Google Scholar]
- Wang Hui-Xin, Karp Anita, Winblad Bengt, and Fratiglioni Laura. 2002. “Late-life Engagement in Social and Leisure Activities Is Associated with a Decreased Risk of Dementia: A Longitudinal Study from the Kungsholmen Project.” American Journal of Epidemiology 155(12):1081–87. [DOI] [PubMed] [Google Scholar]
- Yang Yang and Lee Linda C.. 2009. “Sex and Race Disparities in Health: Cohort Variations in Life Course Patterns.” Social Forces 87(4):2093–2124. [Google Scholar]
- Yoon Hyun-Sook. 2013. “Korea: Balancing Economic Growth and Social Protection for Older Adults.” The Gerontologist 53(3):361–68. [DOI] [PubMed] [Google Scholar]