

Key Points
Question
What patient characteristics are associated with 30-day all-cause mortality among symptomatic nursing home residents with coronavirus disease 2019 (COVID-19)?
Findings
In this cohort study of 5256 US nursing home residents with COVID-19, increased age, male sex, and impaired cognitive and physical function were independent risk factors for all-cause 30-day mortality.
Meaning
This cohort study of 5256 nursing home residents suggests that several characteristics, including sociodemographic characteristics, symptoms, comorbidities, and physical and cognitive functional impairments, can facilitate risk stratification among nursing home residents with COVID-19.
Abstract
Importance
The coronavirus disease 2019 (COVID-19) pandemic has severely affected nursing homes. Vulnerable nursing home residents are at high risk for adverse outcomes, but improved understanding is needed to identify risk factors for mortality among nursing home residents.
Objective
To identify risk factors for 30-day all-cause mortality among US nursing home residents with COVID-19.
Design, Setting, and Participants
This cohort study was conducted at 351 US nursing homes among 5256 nursing home residents with COVID-19–related symptoms who had severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection confirmed by polymerase chain reaction testing between March 16 and September 15, 2020.
Exposures
Resident-level characteristics, including age, sex, race/ethnicity, symptoms, chronic conditions, and physical and cognitive function.
Main Outcomes and Measures
Death due to any cause within 30 days of the first positive SARS-CoV-2 test result.
Results
The study included 5256 nursing home residents (3185 women [61%]; median age, 79 years [interquartile range, 69-88 years]; and 3741 White residents [71%], 909 Black residents [17%], and 586 individuals of other races/ethnicities [11%]) with COVID-19. Compared with residents aged 75 to 79 years, the odds of death were 1.46 (95% CI, 1.14-1.86) times higher for residents aged 80 to 84 years, 1.59 (95% CI, 1.25-2.03) times higher for residents aged 85 to 89 years, and 2.14 (95% CI, 1.70-2.69) times higher for residents aged 90 years or older. Women had lower risk for 30-day mortality than men (odds ratio [OR], 0.69 [95% CI, 0.60-0.80]). Two comorbidities were associated with mortality: diabetes (OR, 1.21 [95% CI, 1.05-1.40]) and chronic kidney disease (OR, 1.33 [95%, 1.11-1.61]). Fever (OR, 1.66 [95% CI, 1.41-1.96]), shortness of breath (OR, 2.52 [95% CI, 2.00-3.16]), tachycardia (OR, 1.31 [95% CI, 1.04-1.64]), and hypoxia (OR, 2.05 [95% CI, 1.68-2.50]) were also associated with increased risk of 30-day mortality. Compared with cognitively intact residents, the odds of death among residents with moderate cognitive impairment were 2.09 (95% CI, 1.68-2.59) times higher, and the odds of death among residents with severe cognitive impairment were 2.79 (95% CI, 2.14-3.66) times higher. Compared with residents with no or limited impairment in physical function, the odds of death among residents with moderate impairment were 1.49 (95% CI, 1.18-1.88) times higher, and the odds of death among residents with severe impairment were 1.64 (95% CI, 1.30-2.08) times higher.
Conclusions and Relevance
In this cohort study of US nursing home residents with COVID-19, increased age, male sex, and impaired cognitive and physical function were independently associated with mortality. Understanding these risk factors can aid in the development of clinical prediction models of mortality in this population.
This cohort study examines risk factors for 30-day all-cause mortality among US nursing home residents with COVID-19.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has had profound effects on long-term care residents, accounting for a disproportionate share of deaths both in the US and internationally.1,2 At least 283 000 residents in approximately 12 000 US facilities have been infected and more than 56 000 have died as of July 9, 2020, accounting for 10% of all US cases but 44% of US deaths.1
Nursing homes provide care for a vulnerable population of frail older adults who are unable to live independently because of a combination of underlying chronic conditions, cognitive and physical impairments, and other age-related disabilities.3 Residents often face increased risks of SARS-CoV-2 infection and COVID-19 illnesses owing to extrinsic factors, such as a lack of adequate infection prevention and control measures to prevent transmission within homes. Once infected, patient-level characteristics place some residents at higher risk of death than others.4,5,6,7,8,9,10 These characteristics, combined with the communal living environment and high-touch care required, make nursing homes residents uniquely vulnerable to COVID-19 and its adverse outcomes.
Still, the forces shaping the vulnerability to adverse COVID-19 outcomes within nursing homes are not well understood. Although COVID-19 mortality increases with age, there has been limited evidence as to what factors differentiate between nursing home residents at higher and lower risk of death. With older adults being a clinically heterogeneous population, there is a need to evaluate patient characteristics beyond age that can help identify residents who are at high risk of death after SARS-CoV-2 infection. Few studies using resident-level data are available, and include data from a single facility or a small number of facilities, which limits their generalizability across states, resident populations, and COVID-19 dynamics.11,12,13 There is little evidence as to what characteristics differentiate nursing home residents from the general population and could thus be associated with the increased rates of COVID-19 mortality in this population. In 1 Maryland nursing home, residents undergoing dialysis had higher infection rates, and once infected, higher rates of hospitalization than residents not undergoing dialysis, but no differences in mortality rates.13 Among residents of a large Massachusetts nursing home, mortality was increased among residents with advanced frailty.11 In a study of 4 nursing homes in the United Kingdom, residents with COVID-19 who died were more likely to be male and had higher rates of cardiovascular disease than those who survived.12
The COVID-19 burden has also disproportionally affected Black and Hispanic individuals, both in the overall population and in nursing homes specifically.14,15,16 Nursing homes with more Black residents have been found to be at higher risk for outbreak, but whether this is primarily a function of nursing home location or disparities in outcomes for Black residents within facilities is unknown.14,15,16 These findings suggest that considering a patient’s comorbid conditions, demographics, and frailty is likely to improve estimation of COVID-19 outcomes.
The continued growth in COVID-19 cases throughout the US, combined with the significant vulnerability of frail older adults, calls for an improved understanding of mortality risk stratification among nursing home residents with COVID-19. To address this need, we leveraged unique electronic medical record data and other clinical data from a large multistate sample of US nursing homes to evaluate how key prognostic domains including age, comorbidities, COVID-19 symptom presentation, cognitive function, and physical function, individually and jointly are associated with 30-day all-cause mortality in this population.
Methods
Setting and Data Sources
We used electronic medical records, daily nursing home infection logs, and Minimum Data Set (MDS) resident assessments from a large provider of postacute care and long-term care that operates across 25 US states. The electronic medical record includes the daily census and disposition of all residents, vital signs, and nursing documentation. Residents undergo nursing assessments including vital signs 2 to 3 times daily to screen for new signs or symptoms of COVID-19. Nurses record any changes in condition in a structured form in the electronic medical record. Each facility also maintains separate infection logs documenting SARS-CoV-2 testing dates and results. Minimum Data Set assessments are mandatory resident assessments containing detailed demographic and clinical information completed on admission and discharge and at regular intervals during the nursing home stay, including after any significant change in resident condition. The study was reviewed and approved by the Brown University institutional review board, which waived the need for informed consent because the study was a minimal risk for participants and we had no direct access to or contact with any individuals in the study; the data are not considered deidentified. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Sample
We identified all residents with polymerase chain reaction–confirmed SARS-CoV-2 infection between March 16 and September 15, 2020, across 351 nursing homes. Testing during this period was generally performed owing to suspicion of SARS-CoV-2 infection or exposure; however, some residents were identified through facility-wide point prevalence surveys. In the current analysis, we were interested in mortality among symptomatic patients. We therefore included all residents who had positive test results regardless of the mode of testing and also had COVID-19–related symptoms starting in a time window ranging from 5 days prior to and up to 14 days after testing. We classified a resident as symptomatic if a change in condition was documented indicating any of the following symptoms, ie, cough, fever (a temperature of ≥37.8 °C), hypoxia (oxygen saturation <92% or a 3% decline from baseline), shortness of breath, chest congestion, nausea, vomiting, diarrhea, confusion, malaise, tachycardia, anosmia, rhinorrhea, sore throat, or nasal congestion.
Outcome
Our outcome was death due to any cause within 30 days of a resident’s first positive SARS-CoV-2 polymerase chain reaction test result. Mortality was ascertained from MDS discharge records as well as the electronic medical record resident census. This outcome operationalization was selected for consistency with randomized trials of COVID-19 treatments because factors associated with mortality could be potentially used to tailor such treatments to high-risk patients.
Variables
We considered a priori selected factors in key clinically meaningful domains including age, demographic characteristics (sex and race/ethnicity), comorbidities (heart failure, coronary artery disease, chronic kidney disease, chronic obstructive pulmonary disease, hypertension, and type 2 diabetes), cognitive function, and physical function. We also included symptoms at COVID-19 presentation (ie, tachycardia, shortness of breath, fever, and hypoxia), which capture disease severity.
Physical function was measured in the MDS with a validated 28-point composite score of activities of daily living (ADL), including dressing, personal hygiene, toilet use, locomotion on unit, transfer, bed mobility, and eating (eTable 1 in the Supplement).17 The ADL score ranges from 0 to 28 and describes a patient’s range from substantial to very severe impairment, with higher values indicating higher ADL impairment. To facilitate interpretation of findings, ADL scores were divided into 4 quartiles (ie, 0-14, 15-19, 20-21, and 22-28), consistent with previous work.18 Cognitive function was assessed in the MDS with the Cognitive Function Scale (CFS) score, which provides a valid single, integrated measure of nursing home residents’ cognitive function. The CFS is a hierarchical 4-level scale derived from a resident’s Brief Interview for Mental Status (BIMS) assessment and/or Cognitive Performance Scale (CPS) and integrates their findings into a single score. Accordingly, a resident’s cognitive function is assessed as severely impaired (ie, individuals who were not able to complete the BIMS by themselves or have a CPS score of 5 or 6), moderately impaired (ie, a BIMS score of ≤7 or a CPS score of 3-4), mildly impaired (ie, a BIMS score of 8-12 or a CPS score of ≤2), or cognitively intact (ie, individuals who were able to complete the BIMS and scored between 13 and 15).19
The BIMS is completed by residents who are cognitively intact; otherwise, it is completed by staff. It is categorized into 3 levels (ie, intact or borderline cognition [score, 13-15], moderate cognitive impairment [score, 8-12], and severe cognitive impairment [score, ≤7]). The CPS is completed by staff for residents who are deemed inappropriate or unable to complete the BIMS but is completed by residents who are able to complete the BIMS, regardless of their BIMS score. The CPS is calculated using a complex algorithm that assigns residents a score between 0 and 6 based on 5 MDS items (ie, daily decision-making, eating self-performance, ability to make self understood, short-term memory, and whether or not the resident is comatose). Both instruments have high sensitivity in identifying cognitive impairment.20
Statistical Analysis
Our goal was to examine how factors in the prognostic domains described above are associated with risk of death individually and when considered jointly. To examine individual risk factors, we used univariable logistic regression to identify prognostic indicators of 30-day mortality, estimating odds ratios (ORs) and corresponding 95% CIs. We then used multivariable logistic regression to assess the joint association of all risk factors together. Starting with a base model including the established risk factors of age, sex, race/ethnicity, and comorbidities, we used the likelihood ratio test to assess improvement in model fit when adding physical and cognitive functioning as well as symptoms. To assess the association of symptoms, physical function, and cognitive function with risk stratification, we estimated how much the area under the curve (AUC) for the base model (model 1) improved with the addition of symptoms only (model 2), ADL only (model 3), CFS only (model 4), and all factors together (full model). To reduce overfitting, we split our sample into a training set (one-third of the sample) and a validation set (two-thirds of the sample).21 We used bootstraping to obtain 95% CIs for each AUC and their differences.22 To show how the mortality risk changes as a resident moves from lower to higher risk, we computed the quartiles of estimated 30-day mortality risk and estimated the mean probability for each quartile. Last, we estimated separate multivariable models to obtain adjusted 30-day mortality rates on each day after the initial SARS-CoV-2 positive polymerase chain reaction test result. We illustrate cumulative mortality rates by age group and by levels of physical and cognitive function (ie, factors we hypothesized would be associated with death among nursing home residents).
All analyses included SEs clustered at the facility level. Data were analyzed using Stata MP, version 16.0 (StataCorp). All P values were 2-tailed at a type I error rate of .05.
Sensitivity Analysis
We repeated our multivariable analysis using a hierarchical logistic regression with a nursing home–specific random intercept to account for within-facility and between-facility variation in nursing home characteristics (such as quality) that could be associated with patient mortality within a facility.
Results
We identified 5256 nursing home residents (3185 women [61%]; median age, 79 years [interquartile range, 69-88 years]; 3741 White residents [71%], 909 Black residents [17%], and 586 individuals of other races/ethnicities [11%]) with symptomatic SARS-CoV-2 infection. Within 30 days of the first positive test result, 1129 residents (21%) died and 4127 (79%) were alive. Resident characteristics are described in Table 1.
Table 1. Characteristics of Symptomatic Nursing Home Residents Who Tested Positive for SARS-CoV-2.
| Characteristic | Nursing home residents, No. (%) (N = 5256) |
|---|---|
| Age, median (IQR), y | 79 (69-88) |
| Age group, y | |
| <65 | 765 (15) |
| 65-69 | 539 (10) |
| 70-74 | 687 (13) |
| 75-79 | 697 (13) |
| 80-84 | 789 (15) |
| 85-89 | 784 (15) |
| ≥90 | 994 (19) |
| Sex | |
| Male | 2051 (39) |
| Female | 3185 (61) |
| Race/ethnicity | |
| White | 3741 (71) |
| Black | 909 (17) |
| Othera | 586 (11) |
| ADL score, mean (SD) | 16.6 (6.4) |
| ADL dependency quartile | |
| 0-13 | 1327 (25) |
| 14-18 | 1320 (25) |
| 19-20 | 1179 (22) |
| 21-28 | 1410 (27) |
| Cognitive functionb | |
| Cognitively intact | 2023 (39) |
| Impairment | |
| Mild | 1179 (22) |
| Moderate | 1547 (29) |
| Severe | 463 (9) |
| Comorbidities | |
| Dementia | 2503 (48) |
| Heart failure | 1201 (23) |
| Coronary artery disease | 1227 (23) |
| Asthma or COPD | 1366 (26) |
| Chronic kidney disease | 1385 (26) |
| Hypertension | 4116 (78) |
| Type 2 diabetes | 2112 (40) |
| Symptoms | |
| Fever | 2654 (50) |
| Shortness of breath | 582 (11) |
| Tachycardia | 900 (17) |
| Hypoxia | 979 (19) |
Abbreviations: ADL, activities of daily living; COPD, chronic obstructive pulmonary disease; IQR, interquartile range; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Includes the following groups: Asian, Native Hawaiian or other Pacific Islander, and American Indian or Alaska Native.
Cognitive function was evaluated using the cognitive function scale in the Minimum Data Set 3.0.
Sociodemographic Characteristics and Mortality in Residents With COVID-19
The univariable and multivariable associations between resident characteristics and 30-day mortality are shown in Table 2. In both analyses, older age was associated with a higher probability of 30-day mortality. Compared with residents aged 75 to 79 years, the odds of death were 1.46 (95% CI, 1.14-1.86) times higher for residents aged 80 to 84 years, 1.59 (95% CI, 1.25-2.03) times higher for residents aged 85 to 89 years, and 2.14 (95% CI, 1.70-2.69) times higher for residents aged 90 years or older. However, the odds of death were lower for residents aged 70 to 74 years (OR, 0.74 [95% CI, 0.55-1.01]), 65 to 69 years (OR, 0.56 [95% CI, 0.40-0.78]), and younger than 65 years (OR, 0.23 [95% CI, 0.15-0.24]). With regard to other demographic risk factors, women had lower risk than men for 30-day mortality (OR, 0.69 [95% CI, 0.60-0.80]). Risk of death was lower among non-White residents compared with White residents (Black residents: OR, 0.77 [95% CI, 0.62-0.96]; residents of other racial/ethnic groups: OR, 0.60 [95% CI, 0.45-0.81]).
Table 2. Associations Between Clinical Risk Factors and 30-Day All-Cause Mortality in Symptomatic Nursing Home Residents Who Tested Positive for SARS-CoV-2.
| Risk factor | Patients with COVID-19, No. | Deaths, No. (%) | Odds ratio (95% CI) | |
|---|---|---|---|---|
| Univariable | Multivariable | |||
| Age group, y | ||||
| <65 | 765 | 44 (6) | 0.24 (0.16-0.37) | 0.23 (0.15-0.34) |
| 65-69 | 539 | 67 (12) | 0.57 (0.41-0.80) | 0.56 (0.40-0.78) |
| 70-74 | 687 | 108 (16) | 0.74 (0.54-1.02) | 0.74 (0.55-1.01) |
| 75-79 | 697 | 138 (20) | 1 [Reference] | 1 [Reference] |
| 80-84 | 789 | 215 (27) | 1.47 (1.15-1.89) | 1.46 (1.14-1.86) |
| 85-89 | 784 | 222 (28) | 1.55 (1.20-2.01) | 1.59 (1.25-2.03) |
| ≥90 | 994 | 334 (34) | 1.90 (1.53-2.36) | 2.14 (1.70-2.69) |
| Sex | ||||
| Male | 2051 | 451 (22) | 1 [Reference] | 1 [Reference] |
| Female | 3185 | 671 (21) | 0.90 (0.78-1.04) | 0.69 (0.60-0.80) |
| Race/ethnicity | ||||
| White | 3741 | 859 (23) | 1 [Reference] | 1 [Reference] |
| Black | 909 | 164 (18) | 0.75 (0.61-0.92) | 0.77 (0.62-0.96) |
| Othera | 586 | 99 (17) | 0.67 (0.50-0.89) | 0.60 (0.45-0.81) |
| ADL score | ||||
| 0-13 | 1327 | 209 (16) | 1 [Reference] | 1 [Reference] |
| 14-18 | 1320 | 221 (17) | 1.05 (0.84-1.32) | 0.98 (0.77-1.25) |
| 19-20 | 1179 | 288 (24) | 1.77 (1.41-2.23) | 1.49 (1.18-1.88) |
| 21-28 | 1410 | 404 (29) | 2.15 (1.71-2.70) | 1.64 (1.30-2.08) |
| Cognitive function | ||||
| Cognitively intact | 2023 | 275 (14) | 1 [Reference] | 1 [Reference] |
| Impairment | ||||
| Mild | 1179 | 202 (17) | 1.28 (1.04-1.59) | 1.11 (0.89-1.39) |
| Moderate | 1547 | 469 (30) | 2.61 (2.14-3.19) | 2.09 (1.68-2.59) |
| Severe | 463 | 165 (36) | 3.36 (2.58-4.39) | 2.79 (2.14-3.66) |
| Comorbidities | ||||
| Heart failure | ||||
| No | 4035 | 870 (22) | 1 [Reference] | 1 [Reference] |
| Yes | 1201 | 252 (21) | 0.95 (0.78-1.15) | 0.90 (0.74-1.10) |
| Coronary artery disease | ||||
| No | 4009 | 841 (21) | 1 [Reference] | 1 [Reference] |
| Yes | 1227 | 281 (23) | 1.14 (0.97-1.33) | 1.03 (0.86-1.23) |
| Asthma or COPD | ||||
| No | 3870 | 850 (22) | 1 [Reference] | 1 [Reference] |
| Yes | 1366 | 272 (20) | 0.90 (0.77-1.06) | 1.00 (0.84-1.17) |
| Chronic kidney disease | ||||
| No | 3851 | 783 (20) | 1 [Reference] | 1 [Reference] |
| Yes | 1385 | 339 (24) | 1.29 (1.08-1.54) | 1.33 (1.11-1.61) |
| Hypertension | ||||
| No | 1120 | 247 (22) | 1 [Reference] | 1 [Reference] |
| Yes | 4116 | 875 (21) | 1.00 (0.84-1.19) | 0.81 (0.69-0.96) |
| Type 2 diabetes | ||||
| No | 3124 | 695 (22) | 1 [Reference] | 1 [Reference] |
| Yes | 2112 | 427 (20) | 0.87 (0.76-0.99) | 1.21 (1.05-1.40) |
| Symptoms | ||||
| Fever | ||||
| No | 2602 | 472 (18) | 1 [Reference] | 1 [Reference] |
| Yes | 2654 | 657 (25) | 1.54 (1.33-1.78) | 1.66 (1.41-1.96) |
| Shortness of breath | ||||
| No | 4674 | 905 (19) | 1 [Reference] | 1 [Reference] |
| Yes | 582 | 224 (38) | 2.78 (2.29-3.38) | 2.52 (2.00-3.16) |
| Tachycardia | ||||
| No | 4356 | 886 (20) | 1 [Reference] | 1 [Reference] |
| Yes | 900 | 243 (27) | 1.96 (1.60, 2.41) | 1.31 (1.04-1.64) |
| Hypoxia | ||||
| No | 4277 | 798 (19) | 1 [Reference] | 1 [Reference] |
| Yes | 979 | 331 (34) | 2.15 (1.76-2.62) | 2.05 (1.68-2.50) |
Abbreviations: ADL, activities of daily living; COPD, chronic obstructive pulmonary disease; COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Includes the following groups: Asian, Native Hawaiian or other Pacific Islander, and American Indian or Alaska Native.
Comorbidities and Mortality in Residents With COVID-19
Among nursing home residents with COVID-19, 4116 (78%) had hypertension, 3189 (48%) had dementia, 2112 (40%) had type 2 diabetes, and 1385 (26%) had chronic kidney disease (Table 1). Less prevalent were asthma or chronic obstructive pulmonary disease (1366 [26%]), heart failure (1201 [23%]), and coronary artery disease (1227 [23%]). When considered together with clinical and demographic characteristics, diabetes (OR, 1.21 [95% CI, 1.05-1.40]) and chronic kidney disease (OR, 1.33 [95% CI, 1.11-1.61]) were the strongest risk factors of 30-day mortality (Table 2).
Symptoms and Mortality in Residents With COVID-19
Among nursing home residents with COVID-19, the most common symptom at presentation was fever (2654 [50%]), while 979 patients (19%) had hypoxia, 900 (17%) had tachycardia, and 582 (11%) had shortness of breath (Table 1). Each of the 4 symptoms was associated with mortality in both univariable and multivariable models. When considered along with other risk factors, the presence of fever (OR, 1.66 [95% CI, 1.41-1.96]), shortness of breath (OR, 2.52 [95% CI, 2.00-3.16]), tachycardia (OR, 1.31 [95% CI, 1.04-1.64]), and hypoxia (OR, 2.05 [95% CI, 1.68-2.50]) was associated with increased risk of 30-day mortality (Table 2).
Functional Impairment and Mortality in Residents With COVID-19
Nursing home residents with COVID-19 had a mean (SD) ADL score of 16.6 (6.4) and 3189 (61%) had some degree of cognitive impairment, including mild (1179 [22%]), moderate (1547 [29%]), or severe (463 [9%]) (Table 1). Moderate to severe cognitive and physical functional impairment were both associated with higher probability of 30-day mortality in univariable and multivariable analyses (Table 2). Compared with residents in the lowest quartile of ADL score, the odds of death among residents in the third ADL score quartile was 1.49 (95% CI, 1.18-1.88), and the odds of death among those in the fourth ADL score quartile was 1.64 (95% CI, 1.30-2.08) times higher. Compared with cognitively intact residents, the odds of death among residents with moderate cognitive impairment was 2.09 (95% CI, 1.68-2.59), and the odds of death among those with severe cognitive impairment was 2.79 (95% CI, 2.14-3.66) times higher.
Associations of All Novel Factors With Risk Stratification
The addition of ADL and CFS, alone or with the symptoms of tachycardia, shortness of breath, fever, and hypoxia, led to significant (likelihood ratio test P < .001) improvement compared with a base model including age, sex, and comorbidities. As shown in Figure 1, the validation-based AUC of the base model (AUC, 0.66 [95% CI, 0.65-0.69]) improved by 0.05 (95% CI, 0.03-0.07) when adding symptoms (model 2 AUC, 0.71 [95% CI, 0.70-0.74]), improved by 0.02 (95% CI, 0.01- 0.04) when adding ADL (model 3 AUC, 0.68 [95% CI, 0.67-0.71]), improved by 0.03 (95% CI, 0.02-0.05) when adding CFS (model 4 AUC, 0.69 [95% CI, 0.68-0.72]), and improved by 0.08 (95% CI, 0.06-0.10) when all symptoms, ADL, and CFS were added (full model AUC, 0.74; [95% CI, 0.73-0.77]). For all pairwise AUC comparisons, we derived P < .001 indicating significant AUC differences.
Figure 1. Receiver Operating Characteristic (ROC) Curves for 30-Day All-Cause Mortality Based on 5 Different Models.

The base mode consists of established risk factors (ie, age, sex, race/ethnicity, and comorbidities). ADL indicates activities of daily living; and CFS, Cognitive Function Scale.
The distribution of 30-day mortality risk based on the full model is shown in eFigure 1 in the Supplement. The quartiles of mortality risk were as follows: lowest-risk quartile from 0.8% to 9.1%, second risk quartile from 9.2% to 17.3%, third risk quartile from 17.4% to 29.5%, and highest-risk quartile from 29.6% to 85.8%. Figure 2 shows the gradient of risk as the resident moves from lower to higher quartiles of estimated risk. The mean probability was 5.2% in the lowest risk quartile, 12.9% in the second risk quartile, 23.0% in the third risk quartile, and 44.1% in the highest-risk quartile. eFigure 2 in the Supplement shows the adjusted mortality rates for residents in each quartile.
Figure 2. Stratification of 30-Day All-Cause Mortality.

The gradient of risk increases as a resident moves from higher quartiles of estimated risk. The box plot lines correspond from bottom of box to top: 25th percentile, median percentile, 75th percentile. The diamond indicates the mean. The whiskers extend to the minimum (25th percentile − 1.5 × interquartile range) and maximum (75th percentile + 1.5 × interquartile range) values. The dots indicate outliers.
Sensitivity Analysis
For all risk factors, point estimates remained consistent when we accounted for nursing facility random effects (eTable 2 in the Supplement).
Cumulative Mortality Rates
Figure 3 illustrates adjusted cumulative mortality rates on each day during the 30 days after the first positive test result, by age group (Figure 3A), physical functioning categories (Figure 3B), and degree of cognitive impairment (Figure 3C). Cumulative mortality rates were higher among residents in older age groups and those with increased levels of physical and cognitive impairments.
Figure 3. Cumulative Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Mortality Rates.
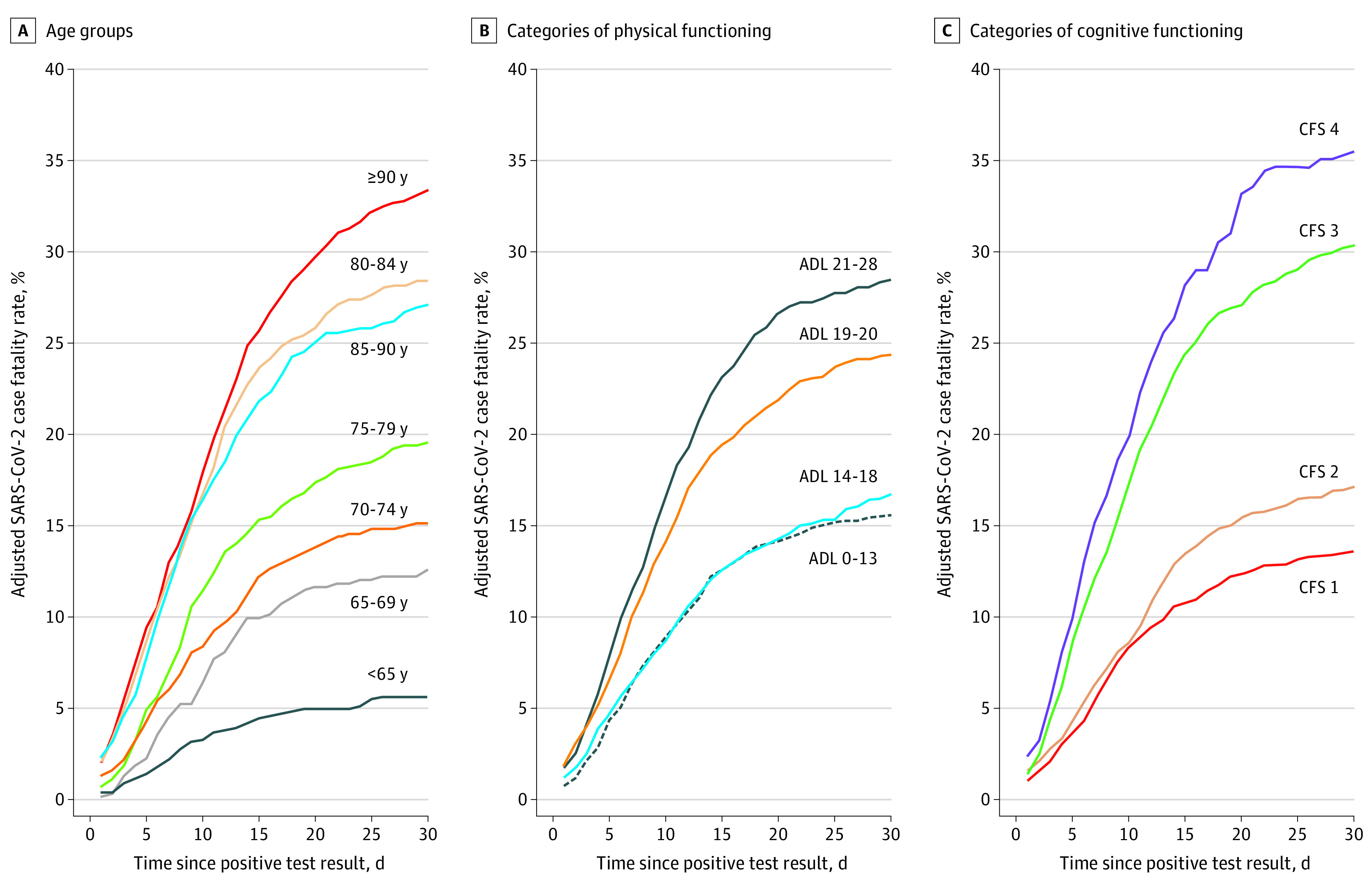
A, Age groups. B, Categories of physical functioning. C, Categories of cognitive functioning. Physical functioning was assessed with the activities of daily living (ADL) score, which ranges from 0 to 28 and describes a patient’s range of impairment from substantial to very severe, with higher values indicating greater impairment. To facilitate interpretation of findings, scores were divided into 4 quartiles (ie, 0-14, 15-19, 20-21, and 22-28). Cognitive functioning was assessed with the Cognitive Function Scale (CFS), which is a hierarchical 4-level scale derived from a resident’s Brief Interview for Mental Status (BIMS) assessment and/or Cognitive Performance Scale (CPS) and integrates their findings into a single score. Accordingly, a residents’ cognitive function is assessed as severely impaired (ie, individuals who were not able to complete the BIMS by themselves or have a CPS score of 5 or 6), moderately impaired (ie, a BIMS score of ≤7 or a CPS score of 3-4), mildly impaired (ie, a BIMS score of 8-12 or a CPS score of ≤2), or cognitively intact (ie, individuals who were able to complete the BIMS and scored between 13 and 15).
Discussion
In this cohort of more than 5000 nursing home residents with COVID-19 in 351 facilities, the 30-day all-cause mortality rate was 21%. We identified several patient characteristics as being associated with mortality, including increased age, male sex, diabetes, chronic kidney disease, fever, hypoxia, shortness of breath, tachycardia, and cognitive and physical impairment. When considered jointly, these factors improve estimation in this population beyond what is achieved when considering them individually. More important, the associations of these factors with mortality were not accounted for by variations in nursing home quality.
Our results are largely consistent with those of previous studies on hospitalized or community-based older adults,6,23,24,25 although we did not find an association with mortality for certain chronic conditions, including coronary artery disease, heart failure, and hypertension. A prior study of nursing home residents in the UK found that, when considered individually, cardiovascular disease is associated with mortality.12 However, that study’s findings are not directly comparable with our multivariable models in which the joint associations of multiple risk factors were assessed. Other analyses using multivariable models in populations that are clinically similar to ours (eg, veterans) have found no associations of cardiovascular diseases and chronic obstructive pulmonary disease with mortality.26
The strongest factors associated with all-cause mortality in our sample were advanced age, symptoms at presentation, certain comorbidities, and impaired physical and cognitive function. Increased age, male sex, and chronic conditions have been previously identified as risk factors for mortality in critically ill patients with COVID-19 and those admitted to the ICU,23,24 the general population,6 and among patients with certain high-mortality conditions such as cancer.25 As nursing home residents are older, have multiple chronic illnesses, and have substantial levels of cognitive and physical impairment, it is not surprising that the mortality rate in our population was substantially higher than in the general population with COVID-19.6,27
Consistent with data on hospitalized patients with COVID-19 in Europe9 as well as multiple studies on patients without COVID-19,28,29 cognitive impairment and ADL impairment are strong risk factors for mortality in nursing home residents with COVID-19 and improve estimation of mortality when added to existing risk factors. Individuals with advanced dementia often have concurrent dysphagia, which is associated with increased risks of malnutrition, aspiration, bacterial pneumonia, and delirium, all of which complicate the course of COVID-19. These individuals generally require extensive assistance with ADL, including bathing and feeding, putting them in regular close proximity with many staff members who may be asymptomatically infected with viral strains from the community. This increases not only the risk of SARS-CoV-2 transmission from staff to resident but also the risk of exposure to a higher viral load at the time of infection, which has been found to correlate with mortality risk.30
Although the association of frailty with mortality outcomes among patients with COVID-19 has been demonstrated in studies of hospitalized or community-based older adults,7,8,9,31 our findings add an illustration of how different components of frailty are associated with mortality risk in an already vulnerable population of nursing home residents. We also build on previous evidence from a single nursing home11 showing a higher prevalence of mortality among residents with the highest vs lowest frailty indices by analyzing a large multistate, multifacility resident sample to show the individual associations of different markers of frailty.
Age is a well-established risk factor for mortality in patients with COVID-19, while shortness of breath, tachycardia, hypoxia, and fever are measures of COVID-19 severity. However, our findings suggest that even within this vulnerable population of older nursing home residents, there are gradations of risk and this risk can be further delineated by considering the frailty that characterizes the long-term care population.32 In particular, 2 important elements of frailty (ie, cognitive impairment [an indicator of advanced dementia] and ADL dependence) are associated with mortality beyond age, symptoms, and comorbidities. Both elements are known risk factors for mortality among nursing home residents without COVID-19.28,29 Considering all these risk factors jointly and aggregating their individual associations with risk will be important for identifying nursing home residents with COVID-19 who are at increased risk of death. For example, our identified risk factors can be used by future studies to independently develop and validate mortality risk scores in the nursing home population.
In this study we did not find that mortality rates were higher among Black residents with COVID-19 compared with White residents or residents of other racial/ethnic groups, which is consistent with previous studies.26 This lack of disparities in our sample could be owing to the fact that disparities are driven by factors associated with COVID-19 acquisition. Other studies have linked SARs-CoV-2 outbreaks to nursing homes with more Black residents located in communities with larger Black populations.9,11 However, in our study we included patients who had positive test results for SARS-CoV-2 rather than the whole population of nursing home residents, which would capture disparities in risk from infection acquisition to subsequent death. For example, it is plausible that Black residents are at higher risk of SARS-CoV-2 acquisition but once infected they are not more likely to die.
Limitations
Our findings should be considered in the light of certain limitations. First, our study was designed to identify factors associated with mortality from COVID-19 and the estimates of associations reported here may not reflect causal effects. Second, our study population included only older nursing home residents, who are typically frailer than physically independent individuals living in the community; therefore, our findings are not applicable to community-dwelling adults. Third, our findings may not be generalizable to asymptomatic nursing home residents with COVID-19, who likely have a different disease severity and clinical course from symptomatic residents with COVID-19.33 Fourth, the mortality events occurred during the first wave of the pandemic and primarily in facilities in Northeastern states with outbreaks up to mid-September 2020. Because the pandemic is still ongoing and data from more recently affected states (eg, Florida and Arizona) are emerging, updated analyses would be needed to confirm our findings. Fifth, we did not have data on hospitalizations and mechanical ventilation, which could help us understand the role of do-not-resuscitate and do-not-hospitalize orders among patients with severe cognitive impairment. However, these events may be uncommon in the nursing home population given that recent clinical practice guidelines have recommended that this patient population be treated supportively in the nursing home setting.34,35 Sixth, our findings may have been associated with decreased case detection owing to limited testing availability in the early phases of the pandemic. If this is the case, our observed mortality rate is likely an underestimate of the actual rate, which is potentially higher than 25%.
Conclusions
In this cohort study of US nursing home residents with COVID-19, the all-cause 30-day mortality rate was 21%. Once infected, those with baseline functional limitations, cognitive impairment, and disease severity are at heightened risk for mortality, with these impairments playing an important role in differentiating which patients are at higher and lower risk beyond what can be established based on age and comorbidities. These findings can be used to aid in prognostication and risk stratification in this population to inform treatment decisions and conversations around goals of care.
eTable 1. Results of Sensitivity Analysis Using Random-Effects Logistic Regression to Account for Facility Effects
eTable 2. MDS Activities of Daily Living and Scoring Methodology
eFigure 1. Distribution of Predicted All-Cause 30-Day Mortality Risk Among Nursing Home Residents With COVID-19
eFigure 2. Adjusted All-Cause 30-Day Mortality Rates by Quartile of Predicted Risk
References
- 1.Kaiser Family Foundation . State data and policy actions to address coronavirus. Published November 18, 2020. Accessed November 19, 2020. https://www.kff.org/health-costs/issue-brief/state-data-and-policy-actions-to-address-coronavirus/
- 2.Comas-Herrera A, Zalakaín J, Lemmon E, et al. Mortality associated with COVID-19 outbreaks in care homes: early international evidence. International Long-Term Care Policy Network. Updated October 14, 2020. November 19, 2020. https://ltccovid.org/2020/04/12/mortality-associated-with-covid-19-outbreaks-in-care-homes-early-international-evidence/
- 3.Tjia J, Rothman MR, Kiely DK, et al. Daily medication use in nursing home residents with advanced dementia. J Am Geriatr Soc. 2010;58(5):880-888. doi: 10.1111/j.1532-5415.2010.02819.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jordan RE, Adab P, Cheng KK. Covid-19: risk factors for severe disease and death. BMJ. 2020;368:m1198. doi: 10.1136/bmj.m1198 [DOI] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention . People with certain medical conditions. Updated November 2, 2020. Accessed November 19, 2020. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/groups-at-higher-risk.html
- 6.Williamson EJ, Walker AJ, Bhaskaran K, et al. Factors associated with COVID–related death using OpenSAFELY. Nature. 2020;584(7821):430-436. doi: 10.1038/s41586-020-2521-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.De Smet R, Mellaerts B, Vandewinckele H, et al. Frailty and mortality in hospitalized older adults with COVID-19: retrospective observational study. J Am Med Dir Assoc. 2020;21(7):928-932.e1. doi: 10.1016/j.jamda.2020.06.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hägg S, Jylhävä J, Wang Y, et al. Age, frailty and comorbidity as prognostic factors for short-term outcomes in patients with coronavirus disease 2019 in geriatric care. J Am Med Dir Assoc. 2020;21(11):1555-1559.e2. doi: 10.1016/j.jamda.2020.08.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hewitt J, Carter B, Vilches-Moraga A, et al. ; COPE Study Collaborators . The effect of frailty on survival in patients with COVID-19 (COPE): a multicentre, European, observational cohort study. Lancet Public Health. 2020;5(8):e444-e451. doi: 10.1016/S2468-2667(20)30146-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zhao HL, Huang YM, Huang Y. Mortality in older patients with COVID-19. J Am Geriatr Soc. 2020;68(8):1685-1687. doi: 10.1111/jgs.16649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shi SM, Bakaev I, Chen H, Travison TG, Berry SD. Risk factors, presentation, and course of coronavirus disease 2019 in a large, academic long-term care facility. J Am Med Dir Assoc. 2020;21(10):1378-1383.e1. doi: 10.1016/j.jamda.2020.08.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Graham NSN, Junghans C, Downes R, et al. SARS-CoV-2 infection, clinical features and outcome of COVID-19 in United Kingdom nursing homes. J Infect. 2020;81(3):411-419. doi: 10.1016/j.jinf.2020.05.073 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bigelow BF, Tang O, Toci GR, et al. Transmission of SARS-CoV-2 involving residents receiving dialysis in a nursing home—Maryland, April 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1089-1094. doi: 10.15585/mmwr.mm6932e4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Abrams HR, Loomer L, Gandhi A, Grabowski DC. Characteristics of U.S. nursing homes with COVID-19 cases. J Am Geriatr Soc. 2020;68(8):1653-1656. doi: 10.1111/jgs.16661 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Testimony of R. Tamara Konetzka, PhD, Professor, Departments of Public Health Sciences and Medicine Biological Sciences Division University of Chicago: Caring for seniors amid the COVID-19 crisis. Special Committee on Aging. 116th Congress, 2nd Session ed 2020. Date of testimony: May 12, 2020. Last accessed: December 1, 2020.
- 16.White EM, Kosar CM, Feifer RA, et al. Variation in SARS-CoV-2 prevalence in U.S. skilled nursing facilities. J Am Geriatr Soc. 2020;68(10):2167-2173. doi: 10.1111/jgs.16752 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Morris JN, Fries BE, Morris SA. Scaling ADLs within the MDS. J Gerontol A Biol Sci Med Sci. 1999;54(11):M546-M553. doi: 10.1093/gerona/54.11.M546 [DOI] [PubMed] [Google Scholar]
- 18.Kosar CM, Thomas KS, Gozalo PL, Mor V. Higher level of obesity is associated with intensive personal care assistance in the nursing home. J Am Med Dir Assoc. 2018;19(11):1015-1019. doi: 10.1016/j.jamda.2018.04.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Thomas KS, Dosa D, Wysocki A, Mor V. The Minimum Data Set 3.0 Cognitive Function Scale. Med Care. 2017;55(9):e68-e72. doi: 10.1097/MLR.0000000000000334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chodosh J, Edelen MO, Buchanan JL, et al. Nursing home assessment of cognitive impairment: development and testing of a brief instrument of mental status. J Am Geriatr Soc. 2008;56(11):2069-2075. doi: 10.1111/j.1532-5415.2008.01944.x [DOI] [PubMed] [Google Scholar]
- 21.Steyerberg EW. Clinical Prediction Models. Springer; 2019. doi: 10.1007/978-3-030-16399-0 [DOI] [Google Scholar]
- 22.Efron B. The Jackknife, the Bootstrap and Other Resampling Plans. SIAM; 1982. doi: 10.1137/1.9781611970319 [DOI] [Google Scholar]
- 23.Gupta S, Hayek SS, Wang W, et al. ; STOP-COVID Investigators . Factors associated with death in critically ill patients with coronavirus disease 2019 in the US. JAMA Intern Med. 2020. doi: 10.1001/jamainternmed.2020.3596 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Grasselli G, Greco M, Zanella A, et al. ; COVID-19 Lombardy ICU Network . Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern Med. 2020;180(10):1345-1355. doi: 10.1001/jamainternmed.2020.3539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kuderer NM, Choueiri TK, Shah DP, et al. ; COVID-19 and Cancer Consortium . Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study. Lancet. 2020;395(10241):1907-1918. doi: 10.1016/S0140-6736(20)31187-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ioannou GN, Locke E, Green P, et al. Risk factors for hospitalization, mechanical ventilation, or death among 10 131 US veterans with SARS-CoV-2 infection. JAMA Netw Open. 2020;3(9):e2022310. doi: 10.1001/jamanetworkopen.2020.22310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.About 38% of U.S. coronavirus deaths are linked to nursing homes. New York Times. Updated October 30, 2020. Accessed November 19, 2020. https://www.nytimes.com/interactive/2020/us/coronavirus-nursing-homes.html
- 28.Thomas JM, Cooney LM Jr, Fried TR. Systematic review: health-related characteristics of elderly hospitalized adults and nursing home residents associated with short-term mortality. J Am Geriatr Soc. 2013;61(6):902-911. doi: 10.1111/jgs.12273 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Thomas KS, Ogarek JA, Teno JM, Gozalo PL, Mor V. Development and validation of the nursing home Minimum Data Set 3.0 Mortality Risk Score (MRS3). J Gerontol A Biol Sci Med Sci. 2019;74(2):219-225. doi: 10.1093/gerona/gly044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Pujadas E, Chaudhry F, McBride R, et al. SARS-CoV-2 viral load predicts COVID-19 mortality. Lancet Respir Med. 2020;8(9):e70. doi: 10.1016/S2213-2600(20)30354-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hubbard RE, Maier AB, Hilmer SN, Naganathan V, Etherton-Beer C, Rockwood K. Frailty in the face of COVID-19. Age Ageing. 2020;49(4):499-500. doi: 10.1093/ageing/afaa095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Fried LP, Tangen CM, Walston J, et al. ; Cardiovascular Health Study Collaborative Research Group . Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-M156. doi: 10.1093/gerona/56.3.M146 [DOI] [PubMed] [Google Scholar]
- 33.Roxby AC, Greninger AL, Hatfield KM, et al. Outbreak investigation of COVID-19 among residents and staff of an independent and assisted living community for older adults in Seattle, Washington. JAMA Intern Med. 2020;180(8):1101-1105. doi: 10.1001/jamainternmed.2020.2233 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Farrell TW, Ferrante LE, Brown T, et al. AGS position statement: resource allocation strategies and age-related considerations in the COVID-19 era and beyond. J Am Geriatr Soc. 2020;68(6):1136-1142. doi: 10.1111/jgs.16537 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lester PE, Holahan T, Siskind D, Healy E. Policy recommendations regarding skilled nursing facility management of coronavirus 19 (COVID-19): lessons from New York state. J Am Med Dir Assoc. 2020;21(7):888-892. doi: 10.1016/j.jamda.2020.05.058 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Results of Sensitivity Analysis Using Random-Effects Logistic Regression to Account for Facility Effects
eTable 2. MDS Activities of Daily Living and Scoring Methodology
eFigure 1. Distribution of Predicted All-Cause 30-Day Mortality Risk Among Nursing Home Residents With COVID-19
eFigure 2. Adjusted All-Cause 30-Day Mortality Rates by Quartile of Predicted Risk