

Abstract
OBJECTIVE
Coronavirus disease 2019 (COVID-19) mortality is high in patients with hypertension, obesity, and diabetes. We examined the association between hypertension, obesity, and diabetes, individually and clustered as metabolic syndrome (MetS), and COVID-19 outcomes in patients hospitalized in New Orleans during the peak of the outbreak.
RESEARCH DESIGN AND METHODS
Data were collected from 287 consecutive patients with COVID-19 hospitalized at two hospitals in New Orleans, LA, from 30 March to 5 April 2020. MetS was identified per World Health Organization criteria.
RESULTS
Among 287 patients (mean age 61.5 years; female, 56.8%; non-Hispanic Black, 85.4%), MetS was present in 188 (66%). MetS was significantly associated with mortality (adjusted odds ratio [aOR] 3.42 [95% CI 1.52–7.69]), intensive care unit requirement (ICU) (aOR 4.59 [CI 2.53–8.32]), invasive mechanical ventilation (IMV) (aOR 4.71 [95% CI 2.50–8.87]), and acute respiratory distress syndrome (ARDS) (aOR 4.70 [95% CI 2.25–9.82]) compared with non-MetS. Multivariable analyses of hypertension, obesity, and diabetes individually showed no association with mortality. Obesity was associated with ICU (aOR 2.18 [95% CI 1.25–3.81]), ARDS (aOR 2.44 [95% CI 1.28–4.65]), and IMV (aOR 2.36 [95% CI 1.33–4.21]). Diabetes was associated with ICU (aOR 2.22 [95% CI 1.24–3.98]) and IMV (aOR 2.12 [95% CI 1.16–3.89]). Hypertension was not significantly associated with any outcome. Inflammatory biomarkers associated with MetS, CRP and lactate dehydrogenase (LDH), were associated with mortality (CRP [aOR 3.66] [95% CI 1.22–10.97] and LDH [aOR 3.49] [95% CI 1.78–6.83]).
CONCLUSIONS
In predominantly Black patients hospitalized for COVID-19, the clustering of hypertension, obesity, and diabetes as MetS increased the odds of mortality compared with these comorbidities individually.
Introduction
Coronavirus disease 2019 (COVID-19), first described in Wuhan, China, in December 2019, is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (1). It has spread rapidly worldwide, infecting >7 million people as of 18 June 2020, with the U.S. leading the world both in number of cases (∼2 million) and fatalities (>100,000) (2). New Orleans, LA, was an early epicenter, with the highest death rate per capita in the U.S. (37.93 per 100,000 people) noted in early April (3). One-third of individuals hospitalized for COVID-19 have severe pneumonia requiring admission to an intensive care unit (ICU) (4), often resulting in acute respiratory distress syndrome (ARDS) (5). A subset of critically ill patients with COVID-19 develop a “cytokine storm” (6,7), similar to that described in prior β-coronavirus outbreaks (8). It is proposed that high levels of proinflammatory chemokines and cytokines are seen in the cytokine storm, and the subsequent recruitment of effector inflammatory cells into the lungs, rather than the virus itself, drives COVID-19–related ARDS (8).
Cases of severe and fatal COVID-19 are associated with comorbid conditions including hypertension, obesity, diabetes, and cardiovascular disease (1,4,9–12). Among case subjects with fatal COVID-19, obesity, hypertension, and diabetes are almost always present in higher proportion than chronic heart or pulmonary disease. However, a pathophysiological mechanism explaining these associations has not been established. Metabolic syndrome (MetS) is defined by the coexistence of metabolic comorbidities that contribute to an increased risk of cardiovascular disease and is diagnosed if three or more of the following five metabolic comorbidities exist: obesity, prediabetes/diabetes, hypertension, hypertriglyceridemia, and reduced HDL levels (13). MetS is a chronic low-grade inflammatory state, with elevated circulating concentrations of CRP, interleukin 6 (IL-6), and IL-1β (14,15). We studied the relationship between hypertension, obesity, and diabetes—individually and clustered as MetS—and COVID-19 severe and fatal outcomes in the urban population of New Orleans, LA, a population with high risk of metabolic disease. Louisiana is among the states with the highest prevalence of diabetes, obesity, and hypertension, with some of the worst health outcomes in the U.S. (16).
Research Design and Methods
We performed a retrospective, observational study of hospitalized patients with COVID-19 (confirmed by SARS-CoV-2 PCR) at two tertiary academic hospitals in New Orleans, LA, from 30 March to 5 April 2020. This study was reviewed and approved with waivers of consent by the Tulane University Biomedical Institutional Review Board and the University Medical Center New Orleans Research Review Council.
Data Collection, Study Cohorts, and Outcome Measures
Demographic and clinical data were collected via chart review by four study investigators with duplicated data collection efforts to ensure fidelity of data, with any discrepancies resolved by chart review from the primary investigator. The data set, including information from hospital admission to discharge or death, was complete as of 27 May 2020, with no patients remaining in the hospital. Data included age, sex, race, ethnicity, admission/discharge dates, ICU admission, invasive mechanical ventilation (IMV), hospital mortality, comorbid conditions to calculate the Charlson Comorbidity Index (17), last recorded hemoglobin A1c, BMI on admission calculated from height and weight, history of hypertension or antihypertensive medication use, last recorded triglyceride (TG) level, last recorded HDL level along with history of hyperlipidemia and concurrent statin use, and other laboratory values on admission (specifically ferritin, CRP, and lactate dehydrogenase [LDH]). Both TG and HDL levels used were obtained from the patient’s record prior to admission when possible as a more accurate measure, recognizing that these levels may fluctuate with decreased diet and acute inflammation (18). TG levels were not included in the MetS calculation or in subgroup analyses if the patient had received or was currently receiving propofol infusion, as propofol infusions may lead to hypertriglyceridemia (19). In these cases, TG levels were recorded from either before admission or prior to propofol initiation, if available.
Patients were divided into two cohorts, MetS and non-MetS, according to modified World Health Organization criteria (13). MetS was defined as having at least three of the following five factors: 1) prediabetes (hemoglobin A1c ≥5.7%) or documented history of diabetes or diabetic medication use, 2) obesity (BMI ≥30 kg/m2), 3) history of hypertension or antihypertensive medication use, 4) TG ≥150 mg/dL, and 5) HDL <50 mg/dL for women and <40 mg/dL for men or use of a cholesterol-lowering medication with documented history of hypercholesterolemia. These modified criteria allow for improved reproducibility of these study results using similar large data sets (20). The primary outcome for all analyses was hospital mortality. Secondary outcomes included need for ICU, IMV, a diagnosis of ARDS using the ratio of arterial oxygen partial pressure (PAo2) to fractional inspired oxygen (FIo2) as defined by Berlin criteria (21), hospital length of stay (LOS), and hospital readmission after initial discharge. To examine the association between clinically significant elevations in inflammatory markers and patient outcomes in MetS, appropriate cutoff values were chosen from published data that have previously been described to affect mortality in patients with COVID-19. These cutoff values include: CRP >41.2 mg/L (22), LDH >365 units/L (22), and ferritin >300 ng/mL (1). These inflammatory markers were also analyzed as continuous variables in a separate analysis. Prespecified subgroup analyses were also completed to determine the association of the individual MetS-associated factors defined above with primary and secondary outcomes. Given the high percentage of Black non-Hispanic patients, post hoc analyses examining these subjects were performed in a similar manner as described for the overall population.
Statistical Analysis
Student t test was used for statistical comparison of numerical variables in different groups, with a two-tailed P value ≤0.05 set as statistically significant. Pearson χ2 test was used to compare categorical variables. For the comparison of outcomes among MetS and non-MetS, a multivariable logistic regression model (or multivariable linear regression model when appropriate) was constructed including age, sex, race, individual hospital site, and Charlson Comorbidity Index as covariates. Separate but similar models were constructed for each subgroup analysis to evaluate the risk of each MetS diagnostic criteria individually (i.e., prediabetes/diabetes, hypertension, obesity, elevated TG, and low HDL) without inclusion of MetS itself in these models. Statistical analyses were performed using SAS Enterprise Guide, version 6.1, and SAS, version 9.4 (both from SAS Institute).
Results
Study Population
We collected data from 287 hospitalized patients with confirmed COVID-19. Mean age was 61.5 years, 56.8% were females, and the majority (245; 85.4%) self-identified as non-Hispanic Black. Baseline characteristics of our patient population are presented in Table 1. The most common comorbid conditions were hypertension (80%), obesity (65%), diabetes (54%), and low HDL (39%). These were present in higher proportion than congestive heart failure (14%) chronic obstructive pulmonary disease (10%), and asthma (10%). The median LOS was 10 days (interquartile range [IQR] 10). In total, 130 patients (45%) required admission to the ICU, of whom 108 (83%) required IMV, 81 (62%) developed ARDS, and 58 (20%) died during the study period. Characteristics of disease severity are presented for the patients who required ICU admission at any point during the hospitalization compared with patients who never required ICU admission (Table 1).
Table 1.
Patient characteristics and severity of disease
| Characteristics | Total (n = 287) | ICU (n = 130) | Ward (n = 157) |
|---|---|---|---|
| Age, mean ± SD, years | 61.5 ± 15.2 | 63.2 ± 14.3 | 60.0 ± 15.8 |
| Female, n (%) | 163 (56.8) | 72 (55.4) | 91 (58.0) |
| Race/ethnicity, n (%) | |||
| Non-Hispanic Black | 245 (85.4) | 118 (90.8) | 127 (80.9) |
| Non-Hispanic White | 25 (8.7) | 10 (7.7) | 15 (9.6) |
| Othera | 17 (5.9) | 2 (1.5) | 15 (9.6) |
| BMIb, mean ± SD, kg/m2 | 33.8 ± 8.5 | 35.3 ± 8.0 | 32.6 ± 8.8 |
| Charlson Comorbidity Score, mean ± SD | 3.5 ± 2.3 | 3.7 ± 2.3 | 3.3 ± 2.4 |
| Selected comorbidities, n (%) | |||
| Hypertension | 230 (80.1) | 112 (86.2) | 118 (75.2) |
| Obesity (BMI ≥30 kg/m2) | 187 (65.2) | 94 (72.3) | 93 (59.2) |
| Severe obesity (BMI ≥40 kg/m2) | 63 (22.0) | 35 (26.9) | 28 (17.8) |
| Diabetes (type 1 or 2) | 154 (53.6) | 72 (55.4) | 82 (52.2) |
| HLD | 112 (39.0) | 65 (50.0) | 47 (29.9) |
| MetS | 188 (65.5) | 106 (81.5) | 82 (52.2) |
| Congestive heart failure | 41 (14.3) | 22 (16.9) | 19 (12.1) |
| COPD | 29 (10.1) | 18 (13.9) | 11 (7.0) |
| Asthma | 30 (10.5) | 24 (18.5) | 6 (3.8) |
| Obstructive sleep apnea | 29 (10.1) | 17 (13.1) | 12 (7.6) |
| Disease severity characteristics | |||
| ARDS, n (%) | 80 (27.9) | 76 (58.5) | 4 (2.6) |
| IMV, n (%) | 108 (37.6) | 108 (83.1) | 0 (0.0) |
| LOS, mean ± SD, days | 12.9 ± 10.5 | 17.5 ± 10.7 | 9.2 ± 8.8 |
| LOS, median (IQR), days | 10 (6–16) | 15 (10–24) | 7 (4–11) |
| Death, n (%) | 58 (20.21) | 57 (43.9) | 1 (0.6) |
| Hospital readmissionc, n (%) | 22/229 (9.6) | 9/73 (12.3) | 13/156 (8.3) |
COPD, chronic obstructive pulmonary disease; HLD, hyperlipidemia.
Includes Hispanic, Asian, and unknown.
BMI is weight in kilograms divided by the square of height in meters.
Hospital readmission data were available only for case subjects who survived to discharge.
Metabolic Syndrome Is Associated With Hospital Mortality
A total of 188 patients (66%) met the criteria for MetS, and the remaining 99 (34%) were included in the non-MetS control group (Table 2). The two cohorts did not differ in age or sex, but non-Hispanic Black patients were present in higher proportion in the MetS group than in the non-MetS group (91% vs. 75%, respectively; P = 0.0009). Among the entire cohort, CRP, LDH, and ferritin levels were available in 270, 273, and 275 patients, respectively. CRP and LDH serum concentrations were more elevated in the MetS group than in the non-MetS group (Table 2). Similar observations were made in the non-Hispanic Black population when analyzed by race (Supplementary Table 1).
Table 2.
MetS characteristics
| Characteristics | MetS (n = 188) | Non-MetS (n = 99) | P value |
|---|---|---|---|
| Age, mean ± SD, years | 61.6 ± 13.9 | 61.2 ± 17.4 | 0.8181 |
| Female, n (%) | 111 (59.0) | 52 (52.5) | 0.2894 |
| Race, n (%) | 0.0009 | ||
| Non-Hispanic Black | 171 (90.9) | 74 (74.8) | |
| Non-Hispanic White | 11 (5.9) | 14 (14.1) | |
| Othera | 6 (3.2) | 11 (11.1) | |
| BMIb, mean ± SD, kg/m2 | 35.4 ± 8.5 | 30.8 ± 7.8 | <0.0001 |
| Charlson Index score, mean ± SD | 3.9 ± 2.3 | 2.8 ± 2.3 | 0.0002 |
| MetS comorbidities, n (%) | |||
| Prediabetes/diabetesc | 169 (89.9) | 31 (31.3) | <0.0001 |
| Obesityd | 136 (72.3) | 51 (54.5) | 0.0004 |
| Hypertensione | 176 (93.6) | 54 (54.5) | <0.0001 |
| TG >150 mg/dLf | 40/136 (29.4) | 1/24 (4.1) | 0.0090 |
| Low HDLg | 139 (73.9) | 8 (8.1) | <0.0001 |
| Laboratory values, mean ± SD (n measured) | |||
| Ferritin, ng/mL | 922 ± 1,503 (180) | 771 ± 886 (95) | 0.2958 |
| CRP, mg/L | 126 ± 88 (176) | 96 ± 87 (94) | 0.0079 |
| LDH, units/L | 403 ± 162 (177) | 357 ± 173 (96) | 0.0306 |
Includes Hispanic, Asian, and unknown.
BMI is weight in kilograms divided by the square of height in meters.
Prediabetes defined by World Health Organization criteria: hemoglobin A1c ≥5.7%.
BMI >30 kg/m2.
Defined as history of hypertension or antihypertensive medication.
TG levels were available for a limited number of patients, and some were excluded if propofol had been administered prior.
HDL <50 mg/dL for women and <40 mg/dL for men or those on a statin with documented history of hyperlipidemia.
In adjusted outcome analyses, MetS was associated with 3.42 increased odds of hospital mortality (95% CI 1.52–7.69), 4.59 increased odds of ICU requirement (95% CI 2.53–8.32), 4.71 increased odds of IMV (95% CI 2.50–8.87), and 4.70 increased odds of ARDS (95% CI 2.25–9.82) when compared with non-MetS (Table 3). Similar observations were noted in the non-Hispanic Black population when analyzed by race (Supplementary Table 2).
Table 3.
Multivariable analyses, MetS vs. non-MetS
| Outcomes | MetS (n = 188) | Non-MetS (n = 99) | Risk difference, % (95% CI) | Adjusted ORa (95% CI) | P value |
|---|---|---|---|---|---|
| Hospital mortality, n (%) | 48 (25.5) | 10 (10.1) | 15.4 (6.8–24.0) | 3.42 (1.52–7.69) | 0.0030 |
| ICU requirement, n (%) | 106 (56.4) | 24 (24.2) | 32.1 (21.1, 43.2) | 4.59 (2.53–8.32) | <0.0001 |
| ARDSb, n (%) | 69 (36.7) | 11 (11.1) | 25.6 (16.3–34.9) | 4.70 (2.25–9.82) | <0.0001 |
| IMV, n (%) | 90 (47.9) | 18 (18.2) | 29.7 (19.3–40.1) | 4.71 (2.50–8.87) | <0.0001 |
| LOS, mean ± SD, days | 14.1 ± 10.6 | 10.7 ± 10.1 | n/a | n/a | 0.0097 |
| LOS, median (IQR), days | 11 (7.0–20.5) | 7 (4.0–14.0) | n/a | n/a | 0.0062 |
| Hospital readmission,c n (%) | 16/140 (11.4) | 6/89 (6.7) | 4.7 (−1.7 to 12.1) | 1.19 (0.40–3.61) | 0.7533 |
n/a, not available.
Multivariable logistic regression model adjusted for age, sex, race, hospital site, and Charlson Comorbidity Index.
ARDS defined according to Berlin criteria.
Hospital readmission data were available only for case subjects who survived to discharge.
In contrast to comorbidities clustered as MetS, in separate subgroup multivariable analyses, none of the individual MetS-associated comorbidities were significantly associated with hospital mortality (Fig. 1). However, obesity was associated with increased odds of ICU requirement (adjusted odds ratio [aOR] 2.18 [95% CI 1.25–3.81]), ARDS (aOR 2.44 [95% CI 1.28–4.65]), and IMV (aOR 2.36 [95% CI 1.33–4.21]). Similarly, prediabetes/diabetes was associated with increased odds of ICU requirement (aOR 2.22 [95% CI 1.24–3.98]) and IMV (aOR 2.12 [95% CI 1.16–3.89]). Low HDL was associated with increased odds of ICU requirement (aOR 2.16 [95% CI 1.29–3.60]), ARDS (aOR 2.29 [95% CI 1.28–4.09]), and IMV (aOR 1.72 [95% CI 1.02–2.89]). TG and hypertension were not associated with any primary or secondary outcomes (Fig. 1). In non-Hispanic Black patients, MetS was similarly associated with hospital mortality (aOR 3.30 [95% CI 1.31–8.32]), but none of the individual MetS-associated comorbidities were in separate subgroup multivariable analyses (Supplementary Fig. 1). In non-Hispanic Black patients, obesity was associated with increased odds of ICU requirement (aOR 2.76 [95% CI 1.49–5.11]), ARDS (aOR 2.88 [95% CI 1.43–5.79]), and IMV (aOR 3.14 [95% CI 1.64–6.03]). Diabetes and hypertension were not associated with primary or secondary outcomes (Supplementary Fig. 1).
Figure 1.
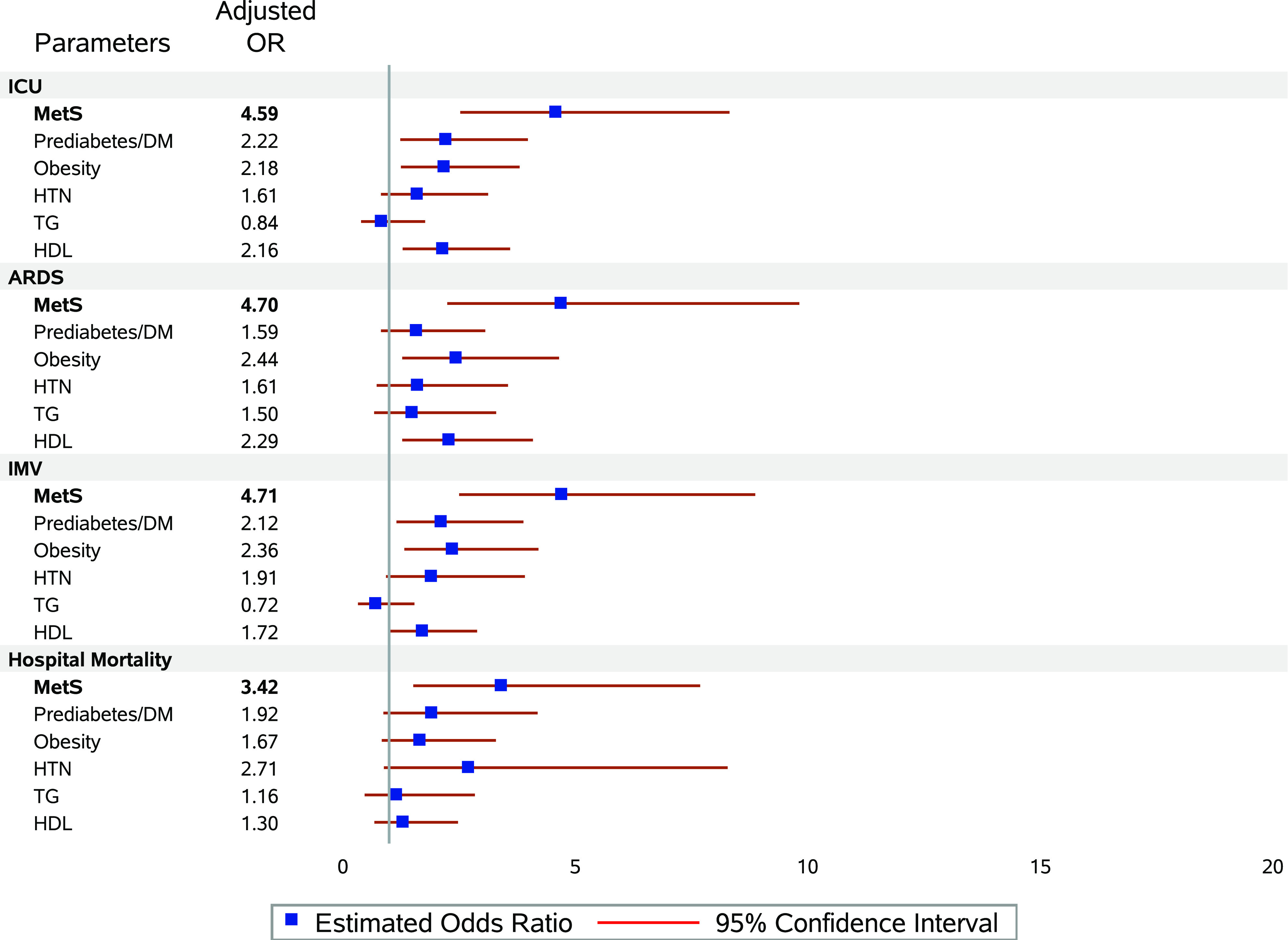
Forrest plot of MetS and individual MetS components on primary and secondary outcomes. Multivariable regression analysis for MetS itself and separate analyses for MetS components were performed. All analyses were adjusted for age, sex, race/ethnicity, hospital site, and the Charlson Comorbidity Index. DM, diabetes mellitus; HTN, hypertension.
Inflammatory Markers Are Associated With Hospital Mortality
Using previously described cutoff values shown to correlate with increased disease severity or mortality in patients with COVID-19, the inflammatory markers CRP and LDH were significantly associated with MetS (Supplementary Table 3). Ferritin was the only biomarker that did not show a significant association with MetS. In non-Hispanic Black patients, MetS was associated only with increased CRP (Supplementary Table 4). When inflammatory markers were compared with patient outcomes (Supplementary Fig. 2), CRP, ferritin, and LDH were all significantly associated with the need for ICU, IMV, and a diagnosis of ARDS, but only CRP and LDH were significantly associated with hospital mortality: CRP (aOR 3.66 [95% CI 1.22–10.97]) and LDH (aOR 3.49 [95% CI 1.78–6.83]). Similar observations were made in non-Hispanic Black patients, except CRP was also not associated with hospital mortality (Supplementary Fig. 3).
Conclusions
The main finding of this multicenter, observational study of hospitalized patients with COVID-19 in New Orleans during the peak of the outbreak is that patients with MetS exhibited a roughly four times greater odds of severe and especially fatal COVID-19 outcomes compared with those without MetS, following multivariable analyses that accounted for age, sex, race, hospital site, and the Charlson Comorbidity Index. In separate subgroup multivariable analyses, however, hypertension, obesity, prediabetes/diabetes, and low HDL, although associated individually with disease severity, were not associated individually with mortality. This suggests that MetS should be considered a composite predictor of COVID-19 lethal outcome, increasing the odds of mortality by the combined effects of its individual components. Previous studies have reported that obese patients are at increased risk for the severe manifestations of COVID-19 (10,23,24). In this study, hospital mortality was not increased by obesity alone. Diabetes has also been reported to increase the risk of ICU requirement by two- to threefold in patients with COVID-19, as well as mortality rates, compared with the overall population (25). However, hospital mortality was not significantly increased by diabetes alone in our population. Hypertension has been reported as the most frequently associated comorbidity in fatal COVID-19 outcomes (1,4,9–12). In our population, hypertension was not associated with any primary or secondary outcomes. Together, this suggests that a combined effect of these comorbidities may be driving the association of MetS with COVID-19 fatal outcomes.
The relationship between hypertension, obesity, and diabetes and critical COVID-19 outcomes has been observed in many large cohort studies (1,4,9–12). Among case subjects with fatal COVID-19, hypertension, obesity, and diabetes were always present in higher proportion than pulmonary or heart disease, suggesting that metabolic diseases predict worse outcomes in COVID-19 than diseases in which lung and heart functions are compromised. One possible explanation, as our study suggests, is that these metabolic comorbidities (combined as MetS) are characterized by a low-grade systemic inflammation (14). Previous reports show that compared with case subjects with moderate COVID-19, case subjects with severe COVID-19 exhibited higher serum levels of inflammatory markers such as CRP, ferritin, d-dimer, and LDH, as well as markedly higher levels of proinflammatory cytokines such as IL-6 and tumor necrosis factor-α (26,27). Similarly, our MetS cohort exhibited increased inflammatory biomarkers (CRP and LDH) when using cutoffs shown to predict COVID-19 mortality. Notably, CRP, ferritin, and LDH were all associated with two- to threefold increased odds of severe outcomes, and CRP and LDH were associated with 3.5-fold increased odds of hospital death. Therefore, the chronic low-grade systemic inflammation that characterizes individuals with MetS may provide a permissive inflammatory environment that intensifies the evolution toward ARDS and death (12). Further research into the underlying mechanisms by which MetS increases COVID-19 mortality is needed.
Our cohort is unique. Our hospitals care for a predominantly non-Hispanic Black population (85% of our cohort) with a high prevalence of comorbidities who have been greatly affected by the COVID-19 pandemic (3,28). A recent study including >1,000 hospitalized non-Hispanic Black patients from a hospital system in Louisiana caring for a healthier population (only 9% were uninsured) (29) reported a mean Charlson Comorbidity Index of 1.3 (29). By contrast, our cohort of 245 hospitalized Black non-Hispanic patients in downtown New Orleans (74% from a public hospital and mostly uninsured) exhibited a mean Charlson Comorbidity Index of 3.5. This is further highlighted by our control group, which, despite not meeting criteria for MetS, showed elevated rates of hypertension (54%), obesity (53%), and prediabetes/diabetes (31%) and mean Charlson Comorbidity Score (2.8).
Another important consideration of our study is the effect of sex on COVID-19 outcomes. Our hospitalized population exhibited a predominance of women (56%), which was also observed in another study in non-Hispanic Black patients from southeastern Louisiana (29). This predominance of women contrasts with most large studies in predominantly non-Hispanic White, European, or Asian patients in whom COVID-19 hospitalization showed a strong predominance of men, averaging 70% (11,30–34). Thus, in our population, COVID-19 could affect women and men differently.
This study has several limitations. As a retrospective observational study, our conclusions can only be based on associations and do not imply causation. Although we used multivariable regression models to adjust for relevant covariates and clinically relevant data evaluations (e.g., taking into account the consideration of propofol infusion with regard to TG levels), these data cannot fully account for all unknown potential confounders.
Conclusion
In a predominantly non-Hispanic Black population hospitalized for COVID-19, the clustering of hypertension, obesity, and diabetes as MetS and inflammatory markers increased the odds of mortality compared with these comorbidities individually. These findings suggest that MetS is a composite predictor of COVID-19 lethal outcome, in which the combined effect of its related comorbidities was significantly associated with mortality, possibly via inflammation.
Article Information
Funding. Funding for this work was provided in part by the Tulane University Physician Scientist Pipeline Program (to J.L.D.); American Diabetes Association grants 7-20-COVID-053 (to J.L.D.) and 7-20-COVID-051 (to F.M.-J.); National Institute of General Medical Sciences/National Institutes of Health award U54 GM104940, which funds the Louisiana Clinical and Translational Science Center (to J.L.D.); National Institutes of Health awards DK074970 and DK107444 (to F.M.-J.); and the U.S. Department of Veterans Affairs Merit Review Award BX003725 (to F.M.-J.).
Duality of Interest. No potential conflicts of interest relevant to this article were reported.
Author Contributions. J.X., A.A., T.T.P., and F.G. performed retrospective chart review. Y.Z. and L.M. analyzed the raw data and performed statistics. J.X., A.J., S.R., and J.L.D. wrote the initial manuscript. F.M.-J. and J.L.D. analyzed the final data and wrote and edited the final draft. G.C., L.M., J.S.Z., C.M.B., and N.F.M. critically reviewed the manuscript. All authors read and approved the final manuscript. J.L.D. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
See accompanying articles, pp. 1, 8, 11, and 258.
This article contains supplementary material online at https://doi.org/10.2337/figshare.12753707.
This article is part of a special article collection available at https://care.diabetesjournals.org/collection/diabetes-and-COVID19.
References
- 1.Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020;395:1054–1062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Johns Hopkins University & Medicin e. COVID-19 case tracker. Accessed 26 May 2020. Available from https://coronavirus.jhu.edu/us-map
- 3.Louisiana Department of Health COVID-19. Accessed 31 May 2020. Available from https://ldh.la.gov/Coronavirus/
- 4.Richardson S, Hirsch JS, Narasimhan M, et al.; and the Northwell COVID-19 Research Consortium . Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020;323:2052–2059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bhatraju PK, Ghassemieh BJ, Nichols M, et al. Covid-19 in critically ill patients in the seattle region - case series. N Engl J Med 2020;382:2012–2022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ruscitti P, Berardicurti O, Iagnocco A, Giacomelli R. Cytokine storm syndrome in severe COVID-19. Autoimmun Rev 2020;19:102562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.McGonagle D, Sharif K, O’Regan A, Bridgewood C. The role of cytokines including interleukin-6 in COVID-19 induced pneumonia and macrophage activation syndrome-like disease. Autoimmun Rev 2020;19:102537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Channappanavar R, Perlman S. Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. Semin Immunopathol 2017;39:529–539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ 2020;369:m1966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gao F, Zheng KI, Wang XB, et al. Obesity is a risk factor for greater COVID-19 severity. Diabetes Care 2020;43:e72–e74 [DOI] [PubMed] [Google Scholar]
- 11.Guan WJ, Ni ZY, Hu Y, et al.; China Medical Treatment Expert Group for Covid-19 . Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 2020;382:1708–1720 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mauvais-Jarvis F Aging, male sex, obesity, and metabolic inflammation create the perfect storm for COVID-19. Diabetes 2020;69:1857–1863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Grundy SM, Cleeman JI, Daniels SR, et al.; American Heart Association; National Heart, Lung, and Blood Institute . Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005;112:2735–2752 [DOI] [PubMed] [Google Scholar]
- 14.Saltiel AR, Olefsky JM. Inflammatory mechanisms linking obesity and metabolic disease. J Clin Invest 2017;127:1–4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Esser N, Legrand-Poels S, Piette J, Scheen AJ, Paquot N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabetes Res Clin Pract 2014;105:141–150 [DOI] [PubMed] [Google Scholar]
- 16.Shrestha SS, Honeycutt AA, Yang W, et al. Economic costs attributable to diabetes in each U.S. State. Diabetes Care 2018;41:2526–2534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373–383 [DOI] [PubMed] [Google Scholar]
- 18.Jahangiri A High-density lipoprotein and the acute phase response. Curr Opin Endocrinol Diabetes Obes 2010;17:156–160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Devlin JW, Lau AK, Tanios MA. Propofol-associated hypertriglyceridemia and pancreatitis in the intensive care unit: an analysis of frequency and risk factors. Pharmacotherapy 2005;25:1348–1352 [DOI] [PubMed] [Google Scholar]
- 20.Kobo O, Leiba R, Avizohar O, Karban A. Normal body mass index (BMI) can rule out metabolic syndrome: an Israeli cohort study. Medicine (Baltimore) 2019;98:e14712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ranieri VM, Rubenfeld GD, Thompson BT, et al.; ARDS Definition Task Force . Acute respiratory distress syndrome: the Berlin Definition. JAMA 2012;307:2526–2533 [DOI] [PubMed] [Google Scholar]
- 22.Yan L, Zhang H-T, Goncalves J, et al. An interpretable mortality prediction model for COVID-19 patients. Nat Mach Intell 2020;2:283–288 [Google Scholar]
- 23.Zhu L, She ZG, Cheng X, et al. Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell Metab 2020;31:1068–1077.e3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Cai Q, Chen F, Wang T, et al. Obesity and COVID-19 severity in a designated hospital in Shenzhen, China. Diabetes Care 2020;43:1392–1398 [DOI] [PubMed] [Google Scholar]
- 25.Riddle MC, Buse JB, Franks PW, et al. COVID-19 in people with diabetes: urgently needed lessons from early reports. Diabetes Care 2020;43:1378–1381 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chen G, Wu D, Guo W, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest 2020;130:2620–2629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020;395:497–506 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Yancy CW COVID-19 and African Americans. JAMA 2020;323:1891–1892 [DOI] [PubMed] [Google Scholar]
- 29.Price-Haywood EG, Burton J, Fort D, Seoane L. Hospitalization and mortality among black patients and white patients with Covid-19. N Engl J Med 2020;382:2534–2543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mauvais-Jarvis F, Bairey Merz N, Barnes PJ, et al. Sex and gender: modifiers of health, disease and medicine. Lancet 2020;396:565–582 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020;323:1775–1776 [DOI] [PubMed] [Google Scholar]
- 32.COVID-19 National Emergency Response Center, Epidemiology and Case Management Team, Korea Centers for Disease Control and Prevention Coronavirus disease-19: the first 7,755 cases in the Republic of Korea [published correction appears in Osong Public Health Res Perspect 2020;11:146]. Osong Public Health Res Perspect 2020;11:85–9032257774 [Google Scholar]
- 33.Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW; Northwell COVID-19 Research Consortium . Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020;323:2052–2059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Klein SL, Dhakal S, Ursin RL, Deshpande S, Sandberg K, Mauvais-Jarvis F. Biological sex impacts COVID-19 outcomes. PLoS Pathog 2020;16:e1008570. [DOI] [PMC free article] [PubMed] [Google Scholar]