

Abstract
Objective To assess the relationship between (1) task demands and workload, (2) task demands and performance, and (3) workload and performance, all during physician-computer interactions in a simulated environment.
Methods Two experiments were performed in 2 different electronic medical record (EMR) environments: WebCIS ( n = 12) and Epic ( n = 17). Each participant was instructed to complete a set of prespecified tasks on 3 routine clinical EMR-based scenarios: urinary tract infection (UTI), pneumonia (PN), and heart failure (HF). Task demands were quantified using behavioral responses (click and time analysis). At the end of each scenario, subjective workload was measured using the NASA-Task-Load Index (NASA-TLX). Physiological workload was measured using pupillary dilation and electroencephalography (EEG) data collected throughout the scenarios. Performance was quantified based on the maximum severity of omission errors.
Results Data analysis indicated that the PN and HF scenarios were significantly more demanding than the UTI scenario for participants using WebCIS ( P < .01), and that the PN scenario was significantly more demanding than the UTI and HF scenarios for participants using Epic ( P < .01). In both experiments, the regression analysis indicated a significant relationship only between task demands and performance ( P < .01).
Discussion Results suggest that task demands as experienced by participants are related to participants' performance. Future work may support the notion that task demands could be used as a quality metric that is likely representative of performance, and perhaps patient outcomes.
Conclusion The present study is a reasonable next step in a systematic assessment of how task demands and workload are related to performance in EMR-evolving environments.
Keywords: task demands, workload, performance, NASA-TLX, errors, EMR
BACKGROUND AND SIGNIFICANCE
There is increasing reliance on health information technology systems to perform clinical work. As part of their daily workflow, providers are required to interact continually with multiple, sometimes disparate, computer-based systems (eg, electronic medical records [EMRs], computerized physician order entry, image repositories, directories for paging, and the diverse informational offerings of the Internet) while providing care to patients, talking to family, or working with staff. There is no question that features of these computer-based systems afford unparalleled opportunities for improved patient care (eg, more ready access to patient-specific information, data integration, decision support, etc.) and thus have been vigorously embraced, explaining their near-universal implementation in provider health systems. 1–7
Nevertheless, the suboptimal levels of adoption and integration of health information technology in US hospitals, and the need for providers to interact with multiple computer-based systems, also raise serious challenges that can hinder quality care. 8,9 The unintended consequences include temporal productivity losses, 10 and increased rates of information processing errors 11–14 and catastrophic errors. 15–18 These studies are concerning and suggest that thoughtful systems design is required for effective electronic health records system implementation, incorporating only key safety- and quality-enhancing features while minimizing additional workload placed on providers.
Specifically, the extraction and integration of data from EMRs can be cumbersome to providers and add unnecessary work. Providers need to efficiently review and interpret diverse types of electronic information, including text (eg, clinical notes), quantitative data (eg, laboratory measures), and medical images. This can be challenging, especially as the amount of useful clinical data is rapidly growing. 5–7,19 If interfaces are designed and implemented suboptimally, they can increase task demands and providers’ workload, which in turn may negatively affect their performance and patient safety. 20–24 Numerous studies in various health care settings demonstrate that excess task demands and workload streaming from task complexities, 25–27 cross-coverage, 28 workflow interruptions, 29 suboptimal workflows, 30 job-related stress, 31 staffing levels, 32 and overall cognitive information processing 33–38 can hinder performance and safety. Workload in general has been shown to affect performance, including in aviation 39–42 and nuclear power. 44–45
OBJECTIVES
Thus it seems reasonable to further advance our understanding of the relationship between clinical task demands, workload, and performance. 46,47 This could allow providers to develop safer EMR systems for better care, and to acquire new skills and knowledge to proactively manage their task demands and workload while maintaining concern for patient safety. 49–51 The objective of this research was to assess the relationship between (1) task demands and subjective and physiological measures of workload, (2) task demands and performance, and (3) subjective and physiological measures of workload and performance, all during physician-computer interactions in a simulated environment ( Figure 1 ).
Figure 1:

Study Objectives
MATERIALS AND METHODS
Environment
Assessments were performed in a simulated environment as part of an Institutional Review Board approved study. All potential participants were given an opportunity to review a consent document that included information regarding study goals, procedures, risks and benefits, the voluntary nature of their participation, the confidentiality of data, etc. The following risks were also discussed with all potential participants (1) stress and anxiety during experiments, especially for participants with past experiences/memories of patient harm, and (2) possibility of boredom, mental fatigue, embarrassment at poor performance, frustration, and/or coercion. All participants had the right to decline participation at any time. All participants who were offered participation signed the consent form and participated in the study.
Scenarios
Each subject performed a set of predefined clinical tasks related to 3 scenarios (clinical task flows were based on the current best clinical practices). The 3 scenarios were designed by experienced physicians to vary by level of clinical complexity (the urinary tract infection [UTI] case being relatively “simple” with 5 tasks, and the pneumonia [PN] and heart failure [HF] cases being relatively more “difficult” with 8 and 9 tasks, respectively), and an increasing number of clinical tasks ( Table 1 ). Each task within each scenario corresponding to ordering tests and/or medications was preassigned a severity grade based on its potential clinical impact (Grade 0: no error; Grade 1: Mild with no direct meaningful clinical impact expected; Grade 2: Moderate with no meaningful clinical impact expected; Grade 3: Severe with meaningful clinical impact expected; Grade 4: Life-threatening clinical impact expected; Grade 5: Death) ( Table 1 ). The proposed severity grading system is analogous to the National Cancer Institute Common Terminology Criteria for Adverse Events. The grading was determined by a consensus of physicians who helped to create the scenarios.
Table 1:
Required tasks for each clinical scenario
| Scenario 1: Urinary Tract Infection | Severity Grade |
|---|---|
| Review the clinical history and physical exam notes. | |
| Specify low risk for venous thromboembolism (VTE) prophylaxis. | 1 |
| Note: Ambulatory, out-of-bed, and education are sufficient prophylaxis. | |
| Order any necessary urine test(s). | 3 |
| Check results of test(s). | |
| Order the appropriate treatment for the patient. | 3 |
| Scenario 2: Pneumonia | |
| Review the clinical history and physical exam. | |
| Specify low risk for VTE prophylaxis. | 1 |
| Note : Ambulatory, out of bed, and education are sufficient prophylaxis. | |
| Write admission orders: | |
| Admit to Med wing G. | 2 |
| Supplemental O2/nasal cannula, wean per nursing. | 3 |
| IV antibiotics, arterial blood gas, blood and sputum cultures, posterior-anterior and lateral chest X-ray (PA/Lat CXR). | 4 |
| AM labs: Complete blood count with differential, basic metabolic panel. | 2 |
| Check results of tests and PA/Lat CXR. | |
| Order CT of chest w/o contrast. | 2 |
| Check results of CT. | |
| Change to oral antibiotics and write discharge order; schedule for follow-up to Medicine clinic in 1 week. | 3 |
| Scenario 3: Heart Failure | |
| Review the History and Physical. This contains pertinent clinical history as well as physical exam. | |
| Specify high risk for VTE prophylaxis. | 3 |
| Subcutaneous heparin. | 3 |
| Order labs: complete blood count, chemistry, trans-thoracic echocardiogram. | 3 |
| Check results of labs. | |
| Write admission orders including daily weights and low-salt diet. | 2 |
| Restart meds. | 3 |
| Tobacco cessation consult. | 1 |
| Order IV Lasix. | 3 |
Participants
For the experiment run in the Web Computer Information System (WebCIS) environment, invitations to participate in the research study were sent to all residents and fellows in the school of medicine to form a relatively heterogeneous group with variable levels of clinical and WebCIS experience as related to our simulated scenarios ( Table 2 ). For the experiment in the Epic environment, experiment invitations were sent only to medical students and resident physicians from the Emergency and Internal Medicine departments to form a relatively homogenous group with a relatively similar level of clinical and EMR experience as related to our simulated scenarios ( Table 2 ).
Table 2:
Composition of participants within each experiment
| Post-graduate year | No. of participants | Experience with EMR (years) | |
|---|---|---|---|
| WebCIS | 1 | 1 | 1 |
| 2 | 2 | 0.5–2 | |
| 3 | 4 | 0.5–3 | |
| 4 | 1 | 2 | |
| 5 | 2 | 0.5–2 | |
| >5 | 2 | ||
| Epic | 0 a | 7 | 0.5 |
| 1 | 4 | ||
| 2 | 1 | ||
| 3 | 2 | ||
| 4 | 2 | ||
| 5 | 1 |
a Medical students
All participants were incentivized to participate with a $100 gift card. Final selections were made based on participants’ availability to participate in the study during designated weeks for data collection. Twelve participants completed the WebCIS experiment and 17 participants completed the Epic experiment, all from 1 teaching hospital. Each participant was instructed to complete a set of prespecified tasks on 3 routine clinical EMR-based scenarios under a “cross-coverage” status (not familiar with the patients) in a simulated environment ( Table 1 ).
Data collection and processing
Quantification of scenario-specific demands
To obtain the click- and time-related data, scenario workflows were reconstructed from recorded screen-capture videos, including eye movements and computer pointer movements and clicks.
Click analysis: The total number of clicks for participants to complete each scenario was quantified, and further subcategorized into: (i) navigation clicks (eg, moving from one window to another window on the screen, etc.), (ii) decision clicks (eg, selecting a test or medication, etc.), (iii) search clicks (eg, initiating the search option for medications/orders, etc.), and (iv) total clicks (sum of navigation, decision, and search clicks).
Time analysis: The total time for participants to complete each scenario was quantified.
Quantification of subjective workload
The NASA-Task-Load Index (TLX) is widely considered to be a valid and reliable subjective measure of workload, and is used across many disciplines. 52,53 The NASA-TLX considers 6 dimensions: mental, physical, temporal demands, frustration, effort, and performance. At the end of each simulated scenario, participants completed the NASA-TLX questionnaire without being aware of their actual clinical performance. First, each participant performed 15 separate pair-wise comparisons between the 6 dimensions (mental, physical, and temporal demands, frustration, effort, and performance) to determine the relevance (and hence a greater weight) of that dimension for a given scenario for that participant. Second, participants marked a workload score ranked from “low” (corresponding to 0) to “high” (corresponding to 100) for each dimension for each scenario. Finally, the composite NASA-TLX score for each scenario was obtained by multiplying the dimension weight (number of times a dimension was chosen) with the corresponding NASA-TLX dimension score, summing across all dimensions, and dividing by 15.
Quantification of physiological workload (eye-data)
For the WebCIS experiment, pupil dilation data was recorded from the left eye using the 60 Hz VisionTrak (ISCAN Inc., Burlington, MA, USA) head-mounted eye-tracking system. For the Epic experiment, pupil dilation data was recorded as an average value derived from both eyes using the 60 Hz Tobi TX-60 remote eye-tracking system. For both experiments, the baseline pupillary data regarding cognitive work was computed by averaging the pupillary dilation collected during the last 1 second prior to recall of the 3-letter memorization tasks repeated 10 times, as previously recommended by experts. 54–57
Eye blinks and other artifacts (partial closures and outliers, based on visual inspection by an expert) were removed from the raw pupil diameter data and linearly interpolated to fill the missing data, resulting in <10% loss for any participant. We used the average pupil diameter and the percent of time that a subject’s pupil was dilated by ≥0.45 mm, calculated from our baseline as measures of workload. As shown by scholars, in both basic and practical applications, maximum pupillary dilation response under cognitive load ranges from ≈0.5–0.7 mm (corresponding to about a 6-digit memorization task), and pupil dilation ≥0.45 mm was considered as “high” workload where performance degradation might be expected.
Quantification of physiological workload (EEG)
During the experiment in the WebCIS environment, electroencephalography (EEG) data were collected using a Nicolet nEEG V32 amplifier. Electrodes were placed using the 10–20 international system on Fp1, Fp2, F3, F4, T3, T4, Cz, O1, O2 with reference and ground electrodes at FCz/A1 and A2 and CPz, respectively. Data processing was accomplished by subtracting the averaged A1/A2 reference signal from the remaining 9 neural signals. Data was filtered using the fourth-order Butterworth band-pass filter with cutoff frequencies of 0.3 Hz and 250 Hz. Independent component analysis 58 was performed to remove temporal muscle activity from signals. Extreme value rejection was performed on epoched data (1 s event-locked trials) with a rejection threshold at 3 times the largest standard deviation across all electrode sites. Frequency content extraction was accomplished using a Morlet wavelet, 59 for 0.5–50 Hz at 0.5 Hz increments, allowing us to analyze EEG rhythmic activity frequency bands. We compared the average power of the frontal midline theta signal (6–7 Hz) at Fz, with the power of the posterior midline alpha signal at Pz (8–10 Hz). The averaged data have been converted to z -scores for each participant across the scenarios and then averaged across participants. This methodology was originally developed to measure working memory load, 60,61 and was further refined by Smith, Gevins, and colleagues 62 for monitoring task loading during complex forms of human-computer interactions (eg, air traffic control), with increase (synchronization) in theta and decrease (de-synchronization) in alpha power indicating higher mental effort to perform the task.
During experiment in the Epic environment, EEG data collection was done using the X-10 wireless EEG headset system from Advanced Brain Monitoring (ABM). The ABM system included multiple bipolar sensor sites: Fz, F3, F4, Cz, C3, C4, POz, P3, and P4. In general, ABM software filters EEG signals with a band-pass filter (0.5–65 Hz) before the analog-to-digital conversion. In order to remove environmental artifacts from the power network, sharp notch filters at 50 Hz, 60 Hz, 100 Hz, and 120 Hz are applied. The algorithm automatically detects and removes a number of artifacts in the time-domain EEG signal, including spikes caused by tapping or bumping of the sensors, amplifier saturation, and excursions that occur during the onset or recovery of saturations. In addition to the conventional data analysis methodology (power of theta [6–7 Hz] at Fz versus power of alpha signal at Pz [8–10 Hz]), 62 the ABM’s algorithm automatically calculated the index of cognitive workload using quadratic and linear discriminant function analyses of model-selected EEG variables derived from the power spectral analysis of the 1 Hz bins from 1–40 Hz, 63,64 which is different from the conventional analysis. 60–62 It has been shown that ABM’s workload index increases with working memory load and increasing difficulty of cognitive tasks (eg, arithmetic, problem-solving), and has been validated in a variety of “simple” and “complex” environments, including military, industrial, and educational simulation environments. 65–68
Quantification of performance
From a patient’s perspective, clinical outcome is arguably the most meaningful endpoint. Performance is the most immediate upstream surrogate for clinical outcome, and is therefore a commonly considered metric. 1,6,11,13,16,33,69 Performance was quantified using the following set of metrics:
Data analysis
As physicians vary in how they interact with computer-based systems (ie, use different workflows to complete tasks), the actual task demands as experienced by participants needed to be determined as part of data analysis. The standard least square regression analysis was used to check for significant differences in task demands between scenarios as quantified by the total number of clicks and the time to complete scenarios, while treating the scenarios (UTI, PN, HF) as a fixed effect and participants as a random variable. This allowed us to rank tasks demands as “low” or “high,” which was further used during analyses of main objectives.
The relationship between (1) task demands and workload was determined using standard least square regression analysis. The relationships between (2) task demands and performance and (3) workload and performance were determined using ordinal regression analysis. Before data analysis, we completed tests for normality and equal variance for all study variables using Shapiro-Wilk's and Bartlett tests, respectively. Results indicated that assumptions were satisfied (normality: all P > .05; equal variance: all P > .05). All our data analyses were conducted using JMP 10 software while specifying missing data (during the WebCIS experiment, our research team neglected to collect one NASA-TLX score for the HF scenario; we also lost 4 data points related to click analysis due to corrupted video-recording files).
RESULTS
Quantification of task demands
Descriptive statistics of task demands, subjective and objective workloads, and performance for each scenario are provided in Table 3 . The fixed effects test indicated significant differences between scenarios as quantified by the total number of clicks: WebCIS: F (2,19) = 13.99, P < .01 with PN and HF significantly >UTI; Epic: F (2,32) = 31.86, P < .01 with PN significantly > UTI and HF; and time to complete scenarios: WebCIS: F (2,22) = 25.53, P < .01 with PN and HF significantly > UTI; Epic: F (2,32) = 29.01, P < .01 with PN significantly > HF and UTI. This allowed us to establish appropriate ranking of task demands as experienced by participants (WebCIS: PN and HF > UTI; Epic: PN > UTI and HF). MANOVA revealed significant differences (with at least P < .05) between all types of clicks (navigation, decision, searching) in both experiments (further reassuring the ranking; see Table 1 ). Overall, in both the UTI and HF cases in both experiments, the severity of omission errors was generally < grade 3 (no meaningful clinical impact). In the PN case, participants in each experiment were more likely to be noted with severity ≥ grade 3. The number of participants with omission errors and the associated range of severity grade are presented in Table 3 .
Table 3:
Averages and standard deviations of workload measures for each scenario within each experiment
| Scenario | Total Clicks | Navigation Clicks | Decision Clicks | Search Clicks | Time to Scenario Completion (sec) | No. of Participants with Omission Errors | Severity Grade of Omission Errors (Range) | |
|---|---|---|---|---|---|---|---|---|
| WebCIS Average (SD) n = 12 | Urinary tract infection | 63 | 24 | 32 | 7 | 308 | 0 | 0 |
| (18) | (4) | (9) | (3) | (121) | ||||
| Pneumonia | 188 | 48 | 114 | 24 | 770 | 7 | 1–4 | |
| (16) | (4) | (12) | (3) | (316) | ||||
| Heart failure | 176 | 49 | 107 | 20 | 575 | 2 | 1–3 | |
| (16) | (4) | (12) | (3) | (254) | ||||
| Epic Average (SD) n = 17 | Urinary tract infection | 128 | 52 | 59 | 17 | 570 | 2 | 2 |
| (44) | (20) | (19) | (7) | (245) | ||||
| Pneumonia | 185 | 58 | 95 | 32 | 863 | 13 | 1–4 | |
| (39) | (14) | (19) | (12) | (375) | ||||
| Heart failure | 113 | 37 | 59 | 17 | 506 | 7 | 1–3 | |
| (22) | (10) | (12) | (7) | (223) |
Relationship between task demands and subjective workload (NASA-TLX)
Standard least square analysis indicated a significant relationship between task demands and NASA-TLX scores in the WebCIS experiment: F (1,33) = 10.54, with parameter estimate = 12.93, P < .01, with NASA-TLX scores UTI [30 (12)], PN [46 (11)], and HF [39 (9)] ( Figure 2 a); but not in the Epic experiment, with NASA-TLX scores UTI [41 (18)], PN [48 (17)], and HF [43 (20)] ( Figure 2 b). Considering all NASA-TLX dimensions as dependent variables simultaneously, the MANOVA revealed significant differences in both experiments (WebCIS: mental (46) > effort (40) > temporal (39) > frustration (36) > performance (26), with physical dimension not applicable [not selected during pair-wise comparisons]; Epic: mental (51) > effort (48) > temporal (44) > frustration (32) > performance (32), with physical dimension not applicable [not selected during pair-wise comparisons]).
Figure 2:
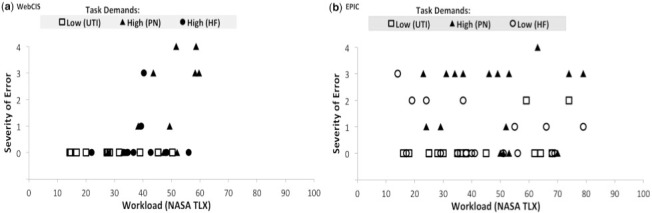
Relationship between tasks demands as experienced by participants (ranking: Low task demands versus High task demands), subjective workload as quantified by NASA-TLX, and performance as quantified by severity grade of omission errors (Grade 0: no error; Grade 1: Mild with no direct meaningful clinical impact expected; Grade 2: Moderate with no meaningful clinical impact expected; Grade 3: Severe with meaningful clinical impact expected; Grade 4: Life-threatening clinical impact expected; Grade 5: Death). In both graphs, squares represent the UTI scenario, triangles represent the PN scenario, and circles represent the HF scenario. Data analysis indicated that the PN and HF scenarios were significantly more demanding than the UTI scenario for participants using WebCIS ( P < .01), and that the PN scenario was significantly more demanding than the UTI and HF scenarios for participants using Epic ( P < .01). In both experiments, the regression analysis indicated a significant relationship only between task demands and performance (objective #2; P < .01). In the WebCIS experiment, there was also a relationship between task demands and subjective measures of workload (objective #1; P < .01). (a) Results from WebCIS experiment. (b) Results from Epic experiment.
Relationship between task demands and physiological workload (eye data)
In both experiments there were no significant relationships between task demands and eye data as quantified by frequency of pupillary dilations > 0.45 mm and average amplitude from the 3-letter memorization baseline.
Relationship between task demands and physiological workload (EEG data)
In both experiments there were no significant relationships between scenario-specific demands and EEG as quantified by conventional methods (theta versus alpha powers) and the ABM’s index of workload.
Relationship between task demands and performance
Ordinal regression analysis indicated a significant relationship between scenario-specific demands and severity of errors in the WebCIS , P < .01 ( Figure 2 a) and Epic , P < .01 ( Figure 2 b) experiments.
Relationship between subjective and objective measures of workload and performance
Ordinal regression analysis indicated a significant relationship between subjective workload, as quantified by the NASA-TLX, and severity of errors in the WebCIS , P < .01 ( Figure 2 a) but not in the Epic experiment. There were no significant relationships in either experiment between physiological measures of workload and performance.
DISCUSSION
The results suggest that there was a significant relationship between tasks demands as experienced by participants and performance as quantified by the severity of omission errors. This relationship was seen in both experiments irrespective of study group and type of EMR, thus suggesting that task demands as experienced by physicians (eg, more clicks, more time) are related to performance (more omission errors). This is most evident in the PN case, which demanded that participants complete a set of predefined admission orders (see step 3 in Table 2 ) with relatively detailed instructions, resulting in more omission errors (eg, forgetting to complete the order, not being able to find the order set/item). A relationship between task demands and severity of omission errors has not been widely quantified and reported for physicians interacting with EMRs. Future work may support the notion that human-computer behavioral data (clicks) as well as total time spent to complete EMR-based tasks could also be used as quality metrics that are likely representative of performance, and perhaps patient outcomes. This could be operationalized using automated scoring technology in EMRs (eg, an unusually high number of total/navigation/search/decision clicks, etc.).
Our results also suggest the existence of relationships between the subjective measure of workload as quantified by the NASA-TLX scores and (i) task demands as quantified by the behavioral interactions (clicks and time to complete) and (ii) performance as quantified by the severity of omission errors. However, these relationships were only found in the WebCIS experiment, which included a relatively heterogeneous group of participants with a variable level of clinical and EMR experience as related to our simulated scenarios. Future work may support the notion that perceived workload by physicians could also be considered as a quality metric that is representative of performance and perhaps patient outcomes. Asking providers to score their workload at the end of a preselected task involving EMRs could be relatively easily operationalized in actual clinical environments. However, in the more homogeneous group of participants tested in the Epic environment, there was no relationship between either subjective measures of workload and task demands or performance. This suggests that the subjective evaluation of workload may be masked by participants’ experience (or confidence) and therefore might not reflect the actual suboptimal behavioral experience (more clicks, time) with the EMR.
No significant relationships were found between task demands and physiological measures of workload. This is somewhat contradictory to previous findings supporting the applicability of physiological measures of workload to detect differences in task demands or performance. 60–68,70–72 This might be indicative of limitations to our data processing and quantification procedures and methods, or the presence of other confounding factors related to cognitive information processing or general cognitive states (eg, arousal, anxiety, stress) experienced by participants during our simulated experiments. It is also possible that the physiological measures of workload used in this study, which were primarily developed and validated based on activations related to working memory, 60–64 might not be appropriate (ie, sensitive and specific enough) to reflect the complex information processing experienced by participants during our experiments. We also acknowledge the possibility that despite significant differences in task demands (eg, clicks, time), the workload experienced by participants was not “distinctive” enough to produce significant differences in their physiological responses.
There are several limitations to this study, and thus caution should be exercised in generalizing our findings. First, the results are based on 2 experiments, each with a limited number of participants (medical students, residents, and fellows) from 1 teaching hospital, performed on a set of specific scenarios without random assignment of scenarios to participants. In the WebCIS experiment, we purposefully sampled from a relatively heterogeneous population of participants with variable levels of clinical and EMR experience as related to our simulated scenarios, so that we could sample a range of capabilities. However, inclusion of 2 particular residents who committed the most errors and most severe errors, including the highest severity scores (both indicated performance degradation at the end of the experiment), may have unduly affected the results. The analysis was repeated with the 2 residents excluded, and the overall conclusions regarding our findings remained virtually unchanged. None of the participants in the Epic experiment indicated performance degradations at the end of the experiment. Similarly, we repeated our analysis while excluding the 1 participant with the severity score of 4, and the overall conclusions regarding our findings also remained virtually unchanged. Nonetheless, larger studies, controlling for levels of clinical and EMR experience, could allow for a regression of provider-specific factors like specialty, training level, etc. We also purposefully did not randomly assign scenarios to participants in order to avoid potential differences in the learning curve and to control for a potential carryover of a workload effect from scenario to scenario, which could unexpectedly bias the study. To minimize this effect, we elected to administer experiments consistently across all participants starting with the UTI case and followed by the PN and HF cases.
Second, performing the tasks in the simulated environment, where the participants knew that their work was going to be critiqued, may have caused stress and anxiety that could influence their physiological measures and performance. On the other hand, performing the tasks in the simulated environment might have induced less attentiveness and vigilance in participants as perceived by no possibility of real harm to patients based on performance. 70 This potential bias is present in essentially all simulation-based research. To minimize this effect, all participants were informed (via the consent form and verbally by the researchers before the experiments) that they had the right to decline participation and that the subject-specific findings would remain confidential. None of the participants voiced any concerns to the researchers over this issue, and no participants declined participation in the study.
Third, reporting workload via NASA-TLX is subjective and can be challenging for some participants. Our research group has had extensive experience with the NASA-TLX tool in the clinical and simulated environment, and investigators in the present study felt most comfortable instructing participants on how to complete this assessment. Further, some of the NASA-TLX dimensions might not be relevant for this research setting (eg, physical demand). 53 Using multiple instruments and measures could provide more robust results and protect against potential interpretive errors. Nevertheless, the NASA-TLX is currently the most widely accepted instrument to perform such assessments. 53 We repeated the analyses for a modified NASA-TLX excluding the physical demand component from the global score, and the results were largely unchanged.
Fourth, the techniques used to assess human-computer interaction behaviors are inexact. For example, the investigators may or may not have accurately interpreted all clicks (decision versus navigation versus search) related to the appropriate behavior while reviewing the videos. To minimize this source of error, 2 investigators of this study independently reviewed the original analysis to ensure accuracy.
Fifth, the use of different instrumentation for collection of physiological data could have affected participants differently (eg, differences in setup). However, it is not likely that instrumentation would affect participants’ overall performance. Sixth, our simulation environment did not fully replicate a real clinical environment, as some components or conditions of the studied scenarios were not easily emulated in our simulation. For example, some participants wanted to look up documentation in an alternative piece of software while conducting a simulated scenario, or had a question regarding how to locate a particular test or medication within the EMR. Thus, all participants were informed about the limitations of our simulated environment before the experiments (eg, no access to additional software, no consultations/help regarding the use of EMR, etc.). Despite these limitations, we believe that the findings support the use of task demands and subjective evaluation of workload as quality metrics representative of performance, and perhaps patient outcomes.
Directions for future research include: (i) random assignment of scenarios to participants with additional assessments and with a larger sample size, (ii) assessment of the targeted population of physicians in terms of academic background and EMR experience, and (iii) additional studies involving alternative EMR environments. It might be particularly valuable to perform studies focused on task demands, workload, and performance in real clinical settings. In the future, one might be able to perform a prospective assessment of an intervention using projected task demands and workload metrics to distribute work more evenly among staff in order to prevent dangerous task demands and workload thresholds from being crossed. This would need to be carefully done in order to control for confounding variables such as system design, varying technologies, communication, workflow, and environment. Indeed, it is the presence of such confounding variables that makes simulation-based research appealing. 70 There is also a need to further develop and assess the utility of physiological measures of workload to predict performance while considering potential confounding factors streaming from cognitive information processing or general cognitive states (eg, participants’ arousal, anxiety, and stress).
CONCLUSION
It is widely believed that health information technology, when designed, implemented, and used appropriately, can enhance patient safety and improve quality of care. However, designed and applied inappropriately, health information technology can add complexity and frustration, increase task demands, increase workload, and reduce performance that can negatively affect clinical care. Physicians will continue to be challenged by the increasing reliance on computer-based tools in the clinical environment. Much has been written about the unforeseen consequences of health information technology, with many scholars and practitioners raising concerns about decreased quality of care. The present study is a reasonable next step in the systematic assessment of how task demands and workload are related to performance in EMR-evolving environments.
Acknowledgments
This study was originally funded by the Innovation Center at the University of North Carolina (UNC) and the UNC Health Care System. The data analysis of subjective and psychological measures of workload was partially supported by grants R18HS023458 and R21HS024062 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality. We want to thank Dr Flavio Frohlich and his graduate student Michael Boyle from the Department of Psychiatry, Cell Biology and Physiology, and Biomedical Engineering at UNC for their support in collecting and analyzing the EEG-related data. We would also like to thank Drs Shereef Elnahal and Joseph Herman from the Department of Radiation Oncology and Molecular Radiation Sciences at Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University School of Medicine in Baltimore, MD, for reviewing and providing their insightful inputs regarding study designs and results. Finally, we want to express our gratitude to all participants for their time and effort while participating in our experiments.
REFERENCES
- 1. Bates DW Leape LL Cullen DJ et al. . Effect of computerized physician order entry and a team intervention on prevention of serious medication errors . JAMA. 1998. ; 280 : 1311 – 1316 . [DOI] [PubMed] [Google Scholar]
- 2. Elnahal SM Joynt KE Bristol JS et al. . Electronic health record functions differ between best and worst hospitals . Am J Manag Care. 2011. ; 17 : e121 – e147 . [PMC free article] [PubMed] [Google Scholar]
- 3. Blumenthal D Glaser JP . Information technology comes to medicine . N Engl J Med. 2007. ; 356 : 2527 – 2534 . [DOI] [PubMed] [Google Scholar]
- 4. Aarts J Koppel R . Implementation of computerized physician order entry in seven countries . Health Aff. 2009. ; 28 : 404 – 414 . [DOI] [PubMed] [Google Scholar]
- 5. Chaudhry B Wu S Maglione M et al. . Systematic review: impact of health information technology on quality, efficiency, and costs of medical care . Ann Intern Med. 2006. ; 144 : e12 – e22 . [DOI] [PubMed] [Google Scholar]
- 6. Kaushal R Shojania KG Bates DW . Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review . Arch Intern Med. 2003. ; 23;163 : 1409 – 1416 . [DOI] [PubMed] [Google Scholar]
- 7. DesRoches CM Campbell EG Vogeli C et al. . Electronic health records’ limited successes suggest more targeted uses . Health Aff. 2010. ; 29 : 639 – 646 . [DOI] [PubMed] [Google Scholar]
- 8. Jha AK DesRoches CM Campbell EG et al. . Use of electronic health records in U.S. hospitals . N Engl J Med. 2009. ; 360 : 1628 – 1638 . [DOI] [PubMed] [Google Scholar]
- 9. Leape LL . Errors in medicine . Clin Chim Acta. 2009. ; 404 : 2 – 5 . [DOI] [PubMed] [Google Scholar]
- 10. Cheriff AD Kapur AG Qiu M et al. . Physician productivity and the ambulatory EHR in a large academic multi-specialty physician group . Int J Med Inform. 2010. ; 49 : 492 – 500 [DOI] [PubMed] [Google Scholar]
- 11. Ash JS Berg M Coiera E . Some unintended consequences of information technology in health care: the nature of patient care information system related errors . J Am Med Inform Assoc. 2004. ; 11 : 104 – 112 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ash JS Sittig DF Dykstra RH et al. . Categorizing the unintended sociotechnical consequences of computerized provider order entry . Int J Med Inform. 2007. ; 76 ( Suppl 1 ): 21 – 27 . [DOI] [PubMed] [Google Scholar]
- 13. Ash JS Sittig DF Dykstra R et al. . The unintended consequences of computerized provider order entry: findings from a mixed methods exploration . Int J Med Inform. 2009. ; 78 ( Suppl 1 ): 69 – 76 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Campbell EM Sittig DF Ash JS et al. . Types of unintended consequences related to computerized provider order entry . J Am Med Inform Assoc. 2006. ; 13 : 547 – 556 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Dexter PR Perkins SM Maharry KS et al. . Inpatient computer-based standing orders vs. physician reminders to increase influenza and pneumococcal vaccination rates: a randomized trial . JAMA. 2004. ; 292 : 2366 – 2371 . [DOI] [PubMed] [Google Scholar]
- 16. Han YY Carcillo JA Venkataraman ST et al. . Unexpected increased mortality after implementation of a commercially sold computerized physician order entry system . Pediatrics. 2005. ; 116 : 1506 – 1512 . [DOI] [PubMed] [Google Scholar]
- 17. Harrison MI Koppel R . Interactive sociotechnical analysis: identifying and coping with unintended consequences of IT implementation . In Khoumbati K, Dwivedi YK, Srivastava A, Lal B , eds. Handbook of Research on Advances in Health Informatics and Electronic Healthcare Applications: Global Adoption and Impact of Information Communication Technologies . Hershey, PA: : IGI Global; ; 2010. : 31 – 49 . [Google Scholar]
- 18. Dekker S . Doctors are more dangerous than gun owners: a rejoinder to error counting . Hum Factors. 2007. ; 49 : 177 – 184 . [DOI] [PubMed] [Google Scholar]
- 19. Carayon P Smith P Hundt AS et al. . Implementation of an electronic health records system in a small clinic: the viewpoint of clinic staff . Behav Inf Technol. 2009. ; 28 : 5 – 20 . [Google Scholar]
- 20. Vicente KJ . Cognitive Work Analysis: Toward Safe, Productive and Healthy Computer-based Work . Mahwah, NJ: : Lawrence Erlbaum Associates; ; 1999. . [Google Scholar]
- 21. Peute LP Jaspers M . The significance of a usability evaluation of an emerging laboratory order entry system . Int J Med Inform. 2007. ; 76 : 157 – 168 . [DOI] [PubMed] [Google Scholar]
- 22. Wachter SB Johnson K Albeit R et al. . The evaluation of a pulmonary display to detect adverse respiratory events using high-resolution human simulator . J Am Med Inform Assoc. 2006. ; 13 : 635 – 642 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Russ AL Melton BL Russell SA et al. . Applying human factors principles to alert design increases efficiency and reduces prescribing errors in a scenario-based simulation . J Am Med Inform Assoc. 2014. ; 21 ( e2 ): 287 – 296 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Elliott DJ Young RS Brice J et al. . Effect of hospitalist workload on the quality and efficiency of care . JAMA Intern. 2014. ; 174 : 786 – 793 . [DOI] [PubMed] [Google Scholar]
- 25. Mazur LM Mosaly PR Jackson M et al. . Quantitative assessment of workload and stressors in clinical radiation oncology . Int J of Radiat Oncol Biol Phy. 2012. ; 83 : e571 – e576 . [DOI] [PubMed] [Google Scholar]
- 26. Yurko YY Scerbo MW Prabhu AS et al. . Higher mental workload is associated with poorer laparoscopic performance as measured by the NASA-TLX Tool . Simul Healthc. 2010. ; 5 : 267 – 271 . [DOI] [PubMed] [Google Scholar]
- 27. Zhang Y Padman R Levin JE . Reducing provider cognitive workload in CPOE use: optimizing order sets . Stud Health Technol Inform. 2013. ; 192 : 734 – 738 . [PubMed] [Google Scholar]
- 28. Mosaly PR Mazur LM Jones EL et al. . Quantifying the impact of cross coverage on physician’s workload and performance in radiation oncology . PRO. 2013. ; 3 : e179 – e186 . [DOI] [PubMed] [Google Scholar]
- 29. Weigl M Müller A Vincent C et al. . The association of workflow interruptions and hospital doctors' workload: a prospective observational study . BMJ Qual Saf. 2012. ; 21 : 399 – 407 . [DOI] [PubMed] [Google Scholar]
- 30. Perna G . Clinical alerts that cried wolf. As clinical alerts pose physician workflow problems, healthcare IT leaders look for answers . Healthc Inform. 2012. ; 29 : 18 – 20 . [PubMed] [Google Scholar]
- 31. Van den Hombergh P Kunzi B Elwyn G et al. . High workload and job stress are associated with lower practice performance in general practice: an observational study in 239 general practices in the Netherlands . BMC Health Serv Res. 2009. ; 9 : 118 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Tarnow-Mordi WO Hau C Warden A et al. . Hospital mortality in relation to staff workload: a 4-year study in adult intensive care unit . The Lancet. 2000. ; 356 : 185 – 189 . [DOI] [PubMed] [Google Scholar]
- 33. Slagle J Weinger MB . The effects of intraoperative reading on vigilance and workload during anesthesia care in an academic medical center . Anes. 2009. ; 110 : 275 – 283 . [DOI] [PubMed] [Google Scholar]
- 34. Avansino J Leu MG . Effects of CPOE on provider cognitive workload: a randomized crossover trial . Pediatrics. 2012. ; 130 : e547 – e552 . [DOI] [PubMed] [Google Scholar]
- 35. Carswell C . Assessing mental workload during laparoscopic surgery . Surg Innov. 2005. ; 12 : 80 – 90 . [DOI] [PubMed] [Google Scholar]
- 36. Gaba DM Lee T . Measuring the workload of the anesthesiologist . Anesth Analg. 1990. ; 71 : 354 – 361 . [DOI] [PubMed] [Google Scholar]
- 37. Young G Zavelina L Hooper V . Assessment of workload using NASA Task Load Index in perianesthesia nursing . J Perianesthesia Nurs. 2008. ; 3 : 102 – 110 . [DOI] [PubMed] [Google Scholar]
- 38. Byrne A . Measurement of mental workload in clinical medicine: a review study . Anaesth Pain Med. 2001. ; 1 : 90 – 94 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Ayaz H Willems B Bunce S et al. . Cognitive workload assessment of air traffic controllers using optical brain imaging sensors . In Marek T, Karwowski W, Rice V , eds. Advances in Understanding Human Performance: Neuroergonomics, Human Factors Design, and Special Populations . CRC Press, Taylor & Francis Group; ; 2010. : 21 – 32 . [Google Scholar]
- 40. Colle HA Reid GB . Mental workload redline in a simulated air-to-ground combat mission . Int J Aviat Psychol. 2005. ; 15 : 303 – 319 . [Google Scholar]
- 41. Lee KK Kerns K Bones R et al. . Development and validation of the controller acceptance rating scale (CARS): Results of empirical research. 4th USA/Europe Air Traffic Management Research and Development Seminar (ATM-2001) . Santa Fe, NM, 2001 . [Google Scholar]
- 42. Hoffman E Pene N Rognin L et al. . Introducing a new spacing instruction, impact of spacing tolerance on flight crew activity. Proceedings of the 47th Annual Meeting of the Human Factors and Ergonomics Society . Santa Monica, CA, 2003 . [Google Scholar]
- 43. Haga S Shinoda H Kokubun M . Effects of task difficulty and time-on-task on mental workload . Jpn Psychol Res. 2002. ; 44 : 134 – 143 . [Google Scholar]
- 44. Byun SN Choi SN . An evaluation of the operator mental workload of advanced control facilities in Korea next generation reactor . J Korean Inst of Ind Eng. 2002. ; 28 : 178 – 186 . [Google Scholar]
- 45. Liang GF Lin JT Hwang SL et al. . Evaluation and prediction of on-line maintenance workload in nuclear power plants . Hum Factors Ergon Manuf. 2009. ; 19 : 64 – 77 [Google Scholar]
- 46. Holden RJ . Cognitive performance-altering effects of electronic medical records: An application of the human factors paradigm for patient safety . Cog Techno Work. 2011. ; 13 : 11 – 29 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Morrison L Smith R . Hamster health care: time to stop running faster and redesign health care . Br Med J. 2000. ; 321 : 1541 – 1542 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Karsh BT Holden RJ Alper SJ et al. . Human factors engineering paradigm for patient safety: designing to support the performance of the healthcare professional . Qual Saf in Health Care. 2006. ; 15 : 59 – 65 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Karsh BT Weinger MB Abbott PA et al. . Health information technology: fallacies and sober realities . J Am Med Inform Assoc. 2010. ; 17 : 617 – 623 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Warden GL Bagian JP . Health IT and Patient Safety: Builder Safer Systems for Better Care . Washington, DC: : Institute of Medicine, National Academies Press; ; 2011. . [PubMed] [Google Scholar]
- 51. Stead W Lin H . Computational Technology for Effective Health Care: Immediate Steps and Strategic Directions . Washington, DC: : National Academies Press; , 2009. . [PubMed] [Google Scholar]
- 52. Hart SG Staveland LE . Development of NASA-TLX (Task Load Index): Results of empirical and theoretical research . In: Hancock PA, Meshkati N , eds., Human Mental Workload . Amsterdam: : North Holland Press; ; 1988. : 139 – 183 . [Google Scholar]
- 53. Hart SG . NASA-TLX Load Index (NASA-TLX); 20 years later . 50th Annual Proceedings of the Human Factors and Ergonomics Society Meeting, Santa Monica, CA ; 2006 : 904 – 908 . [Google Scholar]
- 54. Beatty J Lucero-Wagoner B . The pupillary system . In Cacioppo JT, Tassinary LG, Berntson GG , eds. Handbook of Psychophysiology . New York: : Cambridge University Press; ; 2000. ; 2 : 142 – 162 . [Google Scholar]
- 55. Beatty J . Task-evoked pupillary responses, processing load, and the structure of processing resources . Psychol Bull. 1982. ; 91 ( 2 ): 276 – 292 . [PubMed] [Google Scholar]
- 56. Peavler WS . Pupil size, information overload, and performance differences . Psychophysiology. 1974. ; 11 : 559 – 566 . [DOI] [PubMed] [Google Scholar]
- 57. Kahneman D Beatty D . Pupillary responses in a pitch-discrimination task . Cereb Cortex. 1967. ; 2 : 101 – 105 . [Google Scholar]
- 58. Makeig S Bell AJ Jung T-P et al. . Independent component analysis of electroencephalographic data . Adv Neural Inf Process Syst. 1996. ; 8 : 145 – 151 . [Google Scholar]
- 59. Goupillaud P Grossman A Morlet J . Cycle-octave and related transforms in seismic signal analysis . Geoexploration. 1984. ; 23 : 85 – 102 . [Google Scholar]
- 60. Gevins A Smith ME McEvoy L et al. . High-resolution EEG mapping of cortical activation related to working memory: effects of task difficulty, type of processing, and practice . Cereb Cortex. 1997. ; 7 : 374 – 85 . [DOI] [PubMed] [Google Scholar]
- 61. Gevins A Smith ME Leong H et al. . Monitoring working memory load during computer-based tasks with EEG pattern recognition methods . Hum Factors. 1998. ; 40 : 79 – 91 . [DOI] [PubMed] [Google Scholar]
- 62. Smith ME Gevins A Leong H et al. . Monitoring task loading with multivariate EEG measures during complex forms of human-computer interactions . Hum Factors. 2001. ; 43 : 366 – 380 . [DOI] [PubMed] [Google Scholar]
- 63. Berka C Levendowski DJ Cvetinovic MM et al. . Real-time analysis of EEG indices of alertness, cognition, and memory with a wireless EEG headset . Inter J Hum-Comput Int. 2004. : 17 : 151 – 170 . [Google Scholar]
- 64. Berka C Levendowski DJ Lumicao MN . EEG correlates of task engagement and mental workload in vigilance, learning, and memory tasks . Aviat Space Environ Med. 2007. ; 78 ( 5 Suppl. ): B231 – B244 . [PubMed] [Google Scholar]
- 65. Tremoulet P Barton J Craven R et al. . Augmented cognition for tactical tomahawk weapons control system operators . In Schmorrow D, Stanney K, Reeves L , eds. Foundations of Augmented Cognition . Arlington, VA: : Strategic Analysis; ; 2006. : 313 – 318 . [Google Scholar]
- 66. Berka C Levendowski D Ramsey CK et al. . Evaluation of an EEG-workload model in an Aegis simulation environment . In Caldwell JA, Wesensten NJ , eds. Proceedings of SPIE Defense and Security Symposium, Biomonitoring for Physiological and Cognitive Performance during Military Operations . Orlando, FL: : The International Society for Optical Engineering; ; 2005. : 90 – 99 . [Google Scholar]
- 67. Berka C Levendowski D Westbrook P et al. . EEG Quantification of alertness: methods for early identification of individuals most susceptible to sleep deprivation . In Caldwell JA, Wesensten NJ , eds. Proceedings of SPIE Defense and Security Symposium, Biomonitoring for Physiological and Cognitive Performance during Military Operations . Orlando, FL: : The International Society for Optical Engineering; ; 2005. : 78 – 89 . [Google Scholar]
- 68. Dorneich MC Whitlow SD Mathan S et al. . Supporting real-time cognitive state classification on a mobile participant . J Cogn Eng Decis Making. 2007. ; 1 : 240 – 270 . [Google Scholar]
- 69. Mazur LM Mosaly P Hoyle L et al. . Relating physician’s workload with errors during radiotherapy planning . PRO. 2013. ; 4 : 71 – 75 . [DOI] [PubMed] [Google Scholar]
- 70. Henriksen K Patterson MD . Simulation in health care: setting realistic expectations . J Patient Saf . 2007. ; 3 : 127 – 134 . [Google Scholar]