

Abstract
Objective:
This study aimed to investigate the mediating role of social support in the relationship between resilience and quality of life (QoL) among Turkish patients with early-stage breast cancer.
Methods:
The study used a descriptive and cross-sectional design and was carried out in the oncology ward of a hospital in the Central Anatolia region of Turkey. A demographic-disease survey, the Turkish version of the Connor–Davidson Resilience Scale 25, the Multidimensional Perceived Social Support Scale, the European Organization for Research and Treatment of Cancer QoL Questionnaire Core, and the QoL Questionnaire Breast Cancer 23 were used to interview 113 patients with breast cancer.
Results:
Social support played a partial mediator role in the relationship between resilience and functional QoL. There was a negative correlation between functional QoL Questionnaire Breast Cancer 23 and psychological resilience and social support (P < 0.005). The mediation effect ratio was 10.2% (R2 = 0.102). Social support was found to not have a mediating role in the relationship between psychological resilience and general QoL (P < 0.05).
Conclusions:
Patients do not want social support to end, and their weakness in the eyes of others may have a negative impact on their QoL and resilience.
Keywords: Breast cancer, psychological resilience, Quality of life, social support
Introduction
In Turkey, which is a developing country, and around the world, breast cancer is one of the most commonly diagnosed types of cancer in women and is associated with a considerable rate of mortality. As a matter of fact, it is observed in one in every four women.[1,2] With the increase in current screening methods and treatment options, survival rates are also increasing in women diagnosed with breast cancer.[3] Therefore, quality of life (QoL) and mental health are gaining importance among breast cancer survivors.[4]
Regardless of age, ethnicity, or stage of life, women with breast cancer need to adapt to this life-threatening disease and to cope with the side effects of treatment.[5] The diagnosis of breast cancer and subsequent clinical treatment has a strong impact on the emotional system and QoL of women.[6,7] Being suddenly confronted with a life-threatening disease and the serious physiological side effects associated with cancer treatment may lead to deterioration of daily life and social activities.[7] Studies have reported that 75% of cancer survivors have serious psychosocial problems.[8] In addition, breast cancer treatment has been shown to lead to many negative emotional changes in women, such as severe stress, anxiety, fear, depression, social withdrawal, and aggression.[6,9,10] These negative emotional responses adversely affect the QoL.[11]
One of the important psychosocial factors associated with the negative emotional reactions of patients with breast cancer is their psychological resilience. Resilience refers to a person's mental health and his/her ability to protect himself/herself or to recover despite the difficulties faced.[3] It is not a single personal trait but rather the result of interactions between multiple personality traits and environmental factors.[12] For this reason, higher levels of psychological resilience in patients with breast cancer are associated with better QoL and less negative emotional responses. Recent studies emphasize that psychological resilience as a personal factor and social support as an environmental factor both act as a buffer against stress and increase QoL by decreasing emotional distress in patients with cancer.[11,13]
Social support is an interaction that begins with communication and establishes an empathic relationship, thereby forming a safety net for the patient.[14] It can be defined as the support received by individuals from family, friends, neighbors, and institutions that strengthen psychological dynamics and provide emotional, material, and cognitive assistance to the individual such that he/she may cope with emotional problems.[15] Social support is an important protective factor that enables individuals to cope with stress. Besides, it is believed to be necessary to increase psychological resilience.[11] Notably, some studies reported that patients with breast cancer who receive social support show less anxiety and depression and can return to their normal lives more quickly.[16,17,18] Strong social support in patients with breast cancer has been associated with psychological well-being.[19] By assuming a buffering and protective role, social support serves as a mediator between psychological resilience and QoL, particularly in maintaining physical and mental well-being.[11]
The World Health Organization states that patients with cancer should be provided with psychosocial support in cancer treatment as part of a care plan.[20] To this end, the management of treatment and care of breast cancer, which causes serious emotional and social problems to emerge in the patient in addition to being a medical problem, requires a professional and holistic approach.[15] Nurses, who are among health-care professionals, should ensure adaptation of the individual and their family to the disease by assuming the role of a mediator in social support systems.[11,19] In line with the concept of psychological resilience, successful adaptation means positive interaction of the individual with various social environment factors.[3] Thus, reducing psychological stress and improving QoL by increasing the psychological resilience of patients with breast cancer includes a holistic approach to cancer treatment.[15]
In this context, this study aimed to determine the mediating role played by social support in psychological resilience and QoL in patients with early-stage breast cancer.
Methods
Procedures
At the outset, the approval of the ethics committee of a university was obtained (Approval No. 2018.05.47). In addition, written permission was obtained from the chief physician of a city hospital regarding the conduct of the study. The patients were informed about the scope and purpose of the study and the confidentiality of their information before data collection, and individuals who volunteered to participate in the study were included in the study. Compliance with the ethical principles of “informed consent,” “confidentiality and protection of data,” and “respect for autonomy” was ensured. The participants were encouraged to complete the questionnaires in a private room, and the interviews lasted about 25–30 min.
Sample
This study was conducted as a cross-sectional study in the oncology ward of a hospital in the Central Anatolia region of Turkey between April 2018 and January 2019. Patients were included in the sample according to some inclusion criteria. The inclusion criteria were as follows: (1) aged 18 years or more, (2) ability to speak Turkish, (3) having Stage I or II breast cancer without metastasis, (4) not having any problems that prevent communication, and (5) undergoing treatment for breast cancer. Patients who had previously been diagnosed for any cancer type, who had a major psychiatric disorder and were taking medication for this disorder, and who refused to participate in the study were excluded from the study. In total, 128 patients with breast cancer who were receiving medical treatment and met the inclusion criteria were included in the study. Of these patients, 15 refused to participate in the study and did not sign the informed consent form. Thus, a total of 113 patients with breast cancer were included in the study (participation rate: 88.28%).
Measurements
The demographic and clinical characteristics of the participants such as age, marital status, number of children, educational status, employment status, economic status (in Turkish currency), place of residence, time since diagnosis, breast cancer stage, and type of treatment and surgical procedure were recorded.
Resilience
The Connor–Davidson Psychological Resilience Scale-25 (CDPRS-25), developed by Connor and Davidson to measure psychological resilience, is a 5-point Likert-type self-assessment tool.[21] The Turkish adaptation of the scale was carried out by Karaırmak.[22] In our study, Cronbach's alpha internal consistency coefficient of the scale was found as 0.925. Items in the scale are scored as follows: not true at all (0), rarely true (1), sometimes true (2), often true (3), and true nearly all the time (4). This scale includes three subscales that evaluate Tenacity and personal competence (the highest available score, 60), tolerance of negative affect (the highest available score, 24), and the tendency toward spirituality (the highest available score, 16). The minimum and maximum scores that can be obtained from the scale range between 0 and 100, and there is no cutoff value. Higher scores obtained from the scale indicate greater psychological resilience.
Social support
Perceived social support was evaluated in patients with breast cancer using the Turkish version of the Multidimensional Perceived Social Support Scale (MPSSS).[23] The scale comprises 12 seven-point Likert-type items, and it measures the adequacy of the resources related to the social support of the individual. The scale is a questionnaire based on subjective evaluation of the social support received by individuals from the family, friends, and significant others in their social environment. A score between 12 and 84 can be obtained from the scale, and higher scores indicate a higher level of perceived social support. In our study, Cronbach's alpha internal consistency coefficient of the scale was found as 0.956.
Quality of life
In patients with breast cancer, QoL was evaluated using the Turkish versions of the European Organization for Research and Treatment of Cancer QoL Questionnaire Core 30 (EORTC QLQ-C30) and the Breast Cancer Module (EORTC QLQ-BR23). EORTC QLQ-C30 general health status (GHS) and QoL scale is a multidimensional scale comprising physical function, role function, cognitive function, emotional function, social function, and symptom scales (SCs). Higher scores obtained from the general well-being and functional scales (FSs) indicate a high QoL, whereas lower scores indicate a low QoL. In contrast, low scores from the SCs indicate a high QoL, whereas high scores indicate a low QoL. The lowest total score that can be obtained is 0 and the highest score is 100.[24] In our study, Cronbach's alpha internal consistency coefficient of the scale was found as 0.858.
The EORTC BR23 Breast Cancer Module QoL Scale is a QoL scale designed specifically for breast cancer. The validity and reliability study for the Turkish version of this scale was conducted previously. It comprises 23 questions evaluating body image, sexual function, sexual pleasure, future expectations, and symptoms. The lowest score that can be obtained from each component of the scale is 0 and the highest is 100. While higher scores from the FS indicate better functional status, higher scores from the SC indicate lower QoL.[25] In our study, Cronbach's alpha internal consistency coefficient of the scale was determined as 0.778.
Statistical analysis
The data were statistically analyzed using the Statistical Package for Social Sciences (SPSS) for Windows 23.0 (SPSS Inc, Chicago, Illinois) and Analysis of Moment Structures 21.0 software packages. The normal distribution of the variables was evaluated using the Shapiro–Wilk test, Q-Q graphs, and histograms. Categorical measurements were expressed as numbers and percentages, whereas numerical measurements were expressed as mean, standard deviation, and frequency values. Pearson's correlation analysis was used to evaluate the relationship between scale scores. The research model shown in Figures 1 and 2 is a simple mediation model. In this model, the mediation analysis was conducted to measure the direct and total effects or indirect effects of psychological resilience on the QoL through social support. The research model was tested using the PROCESS software developed by Hayes Andrew for SPSS.[26] When the mediating and independent variables are included in the regression analysis after the specified conditions have been met, a reduction or disappearance should be observed in the existing effect of the independent variable on the dependent variable. The bootstrap confidence interval was analyzed to determine whether the indirect effect of the social support scale was significant Thus, the total effect, direct effect, indirect effect, and bootstrap confidence intervals obtained within the scope of the research were reported.
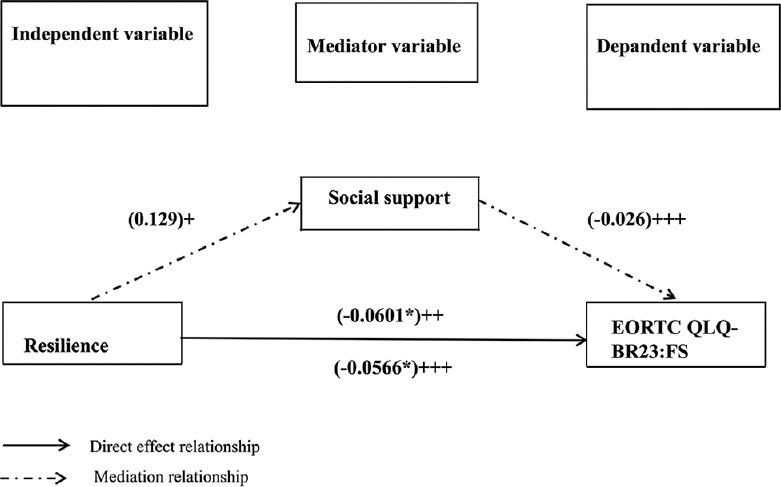
Figure 1.
The mediation model of social support for the relationship between resilience and QLQ (EORTC QLQ-BR23: FS). “+” The first step represents social support regressed on resilience. “++” The second step represents quality of life regressed on resilience. “+++” The third step represents quality of life regressed on resilience and social support. EORTC QLQ-BR23: FS: European Organization for Research and Treatment of Cancer Quality of Life Breast Cancer Module: Functional Scale
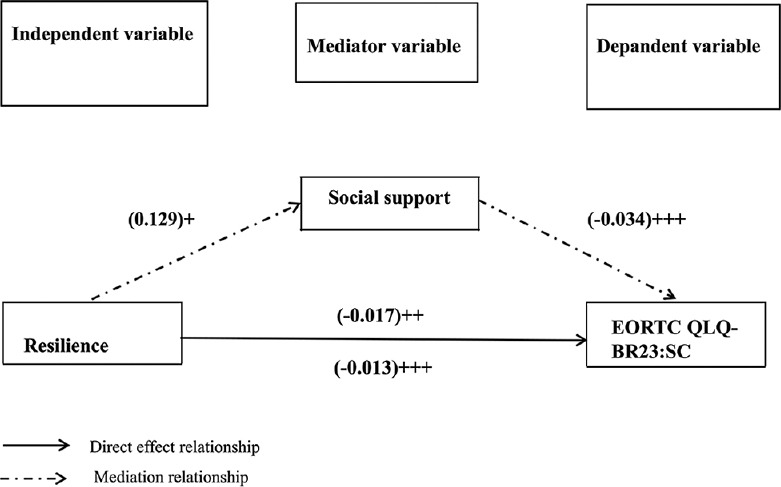
Figure 2.
The mediator model of social support for the relationship between resilience and QLQ (EORTC QLQ-BR23: SC). “+” The first step represents social support regressed on resilience. “++” The second step represents quality of life regressed on resilience. “+++” The third step represents quality of life regressed on resilience and social support. EORTC QLQ-BR23: SC: European Organization for Research and Treatment of Cancer Quality of Life Breast Cancer Module: Symptom Scale
Structural equation modeling (SEM) was conducted to examine the mediating effect of social support on resilience and EORTC QLQ-C30 [Figure 3]. A model was established with resilience as the independent variable, QLQ as the dependent variable, and perceived social support as the mediating variable. Relative Chi-square statistic (DF), Goodness-of-Fit Index (GFI), Adjusted Goodness of Comparative Fit Index (CFI), Adjusted GFI [AGFI], Normed Fit Index (NFI), Incremental Fit Index (IFI), and the Root Mean Square Error of Approximation (RMSEA) were used to investigate the fit indices of the SEM. In an acceptable model, GFI, NFI, IFI, CFI, and AGFI should be >0.90 and RMSEA should be <0.08 and ideally <0.05.[27]
Figure 3.

Structural equation model of social support mediating the relationship between resilience and QLQ (EORTC QLQ-C30). Standardized estimates for significant paths at P < 0.05 are presented. FA: Family, FR: Friends, FS: Functional Scale, GHS: General health status, O: Other (special person), SC: Symptom scale, SS: Social support, TNE: Tolerance of negative affect, TPC: Tenacity and personal competence, TTS: Tendency toward spirituality, EORTC QLQ: European Organization for Research and Treatment of Cancer Quality of Life
Results
Sample characteristics
A total of 113 women with early-stage breast cancer participated in the study. A considerable number of the participants were aged between 41 and 50 years (40.7%), were primary school graduates (54.0%), were married (83.2%), and had children (91.2%). Of the participants, 95.6% were found to live with their families and 91.2% (n = 103) were homemakers. In addition, 45 women were diagnosed with cancer less than a year ago, and the majority (72.6%) had Stage II breast cancer. On the other hand, 85% had undergone surgery, with 49% being breast-conserving mastectomy. The treatment protocols of 100 women were available, and 54% were determined to receive chemotherapy + radiotherapy treatment. Another finding was that 33.6% had a chronic disease and 8.8% had first-degree relatives with breast cancer. The mean body mass index of the women was 29.89 ± 4.83 kg/m2. In addition, 38.9% (n = 44) of the women were overweight [Table 1].
Table 1.
Participants' demographic and disease characteristics (n=113)
| Characteristics | n | % |
|---|---|---|
| Age (years) | ||
| 18-40 | 11 | 9.7 |
| 41-50 | 46 | 40.7 |
| 51-60 | 27 | 23.9 |
| 61 and older | 29 | 25.7 |
| Marital status | ||
| Married | 94 | 83.2 |
| Single | 19 | 16.8 |
| Education level | ||
| Below primary school | 28 | 24.8 |
| Primary school | 61 | 54.0 |
| High school | 21 | 18.5 |
| University or higher | 3 | 2.7 |
| Children | ||
| Yes | 103 | 91.2 |
| No | 10 | 8.8 |
| People living together | ||
| Living alone | 5 | 4.4 |
| Living with family | 108 | 95.6 |
| Employed | ||
| Yes | 5 | 4.4 |
| No | 108 | 95.6 |
| Income status | ||
| Sufficient | 9 | 8.0 |
| Middle | 65 | 57.5 |
| Insufficient | 39 | 34.5 |
| Employment status | ||
| Currently working | 6 | 5.3 |
| Retired | 4 | 3.5 |
| Homemaker | 103 | 91.2 |
| Getting information about breast cancer before diagnosis | ||
| Yes | 21 | 18.6 |
| No | 92 | 81.4 |
| Information sources (n=21) | ||
| Health-care professionals | 12 | 57.1 |
| The internet | 5 | 23.8 |
| Other people | 4 | 19.0 |
| First-degree relative breast cancer | ||
| Yes | 10 | 8.8 |
| No | 103 | 91.2 |
| Chronic disease | ||
| Yes | 38 | 33.6 |
| No | 75 | 66.4 |
| BMI (kg/m2) | ||
| Normal weight (18.5-24.9) | 10 | 17.7 |
| Overweight (25-29-9) | 44 | 38.9 |
| Obese (≥30) | 49 | 43.4 |
| Time since diagnosis | ||
| <1 year | 45 | 39.8 |
| Between 1 and 2 years | 35 | 31.0 |
| Between 2 and 5 years | 33 | 29.2 |
| Stage of breast cancer | ||
| Stage 1 | 31 | 27.4 |
| Stage 2 | 82 | 72.6 |
| Surgery | ||
| Yes | 96 | 85.0 |
| No | 17 | 15.0 |
| Surgery type (n=96) | ||
| Simple mastectomy | 3 | 3.1 |
| Radical mastectomy | 42 | 43.8 |
| Skin-conserving surgery | 4 | 4.2 |
| Breast-conserving surgery | 47 | 49.0 |
| Treatment type (n=100) | ||
| Chemotherapy | 40 | 40.0 |
| Radiotherapy | 5 | 5.0 |
| Chemotherapy + radiotherapy | 54 | 54.0 |
| Hormone therapy | 1 | 1.0 |
BMI: Body mass index
Correlation analysis between resilience, social support, and quality of life
Table 2 shows the correlation between psychological resilience, social support, and QoL. The results of the correlation analysis revealed the following findings: (1) a significant positive correlation between the mean subscale scores of EORTC QLQ-C30: FS and EORTC BR23: FS (r = 0.342, P < 0.01) and EORTC BR23 SC (r = 0.679, P < 0.01); (2) a significant negative correlation between the EORTC QLQ-C30: FS and FR (r = –0.239, P < 0.05), O (r = –0.223, P < 0.05) subscale, and MPSSS total (r = –0.232, P < 0.05) mean scores; (3) a significant negative correlation between the mean subscale scores of EORTC QLQ-C30: GHS and EORTC BR23: FS (r = –0.226, P < 0.01) and EORTC BR23 SC (r = –0.445, P < 0.01); (4) a significant positive correlation between the mean subscale scores of EORTC QLQ-C30: SC and EORTC BR23: FS (r = 0.348, P < 0.01) and EORTC BR23: SC (r = 0.750, P < 0.01); and (5) a significant negative correlation between the EORTC BR23: FS subscale and tenacity and personal competence (r = –0.316, P < 0.01), tolerance of negative affect (r = –0.217, P < 0.05), tendency toward spirituality (r = –0.200, P < 0.05) mean subscale scores, and CDPRS-25 total (r = –0.321, P < 0.01) scale scores.
Table 2.
Correlation matrix for resilience, social support, and quality of life (n=113)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1- EORTC QLQ-C30: FS | 1.000 | ||||||||||||
| P | - | ||||||||||||
| 2- EORTC QLQ-C30: GHS | -0.420 | 1.000 | |||||||||||
| P | 0.000** | - | |||||||||||
| 3- EORTC QLQ-C30: SC | 0.646 | -0.433 | 1.000 | ||||||||||
| P | 0.000** | 0.000** | - | ||||||||||
| 4- EORTC BR23: FS | 0.342 | -0.226 | 0.348 | 0.363 | 1.000 | ||||||||
| P | 0.000** | 0.000** | 0.000** | 0.000** | - | ||||||||
| 5- EORTC BR23: SC | 0.679 | −0.445 | 0.750 | 0.752 | 0.340 | 1.000 | |||||||
| P | 0.000** | 0.000** | 0.000** | 0.000** | 0.000** | - | |||||||
| 6- TPC | −0.007 | 0.064 | 0.016 | 0.016 | −0.316 | −0.045 | −0.170 | 1.000 | |||||
| P | 0.940 | 0.501 | 0.868 | 0.868 | 0.001** | 0.636 | 0.071 | - | |||||
| 7- TNE | −0.086 | 0.045 | −0.079 | −0.089 | −0.217 | −0.089 | −0.162 | 0.583 | 1.000 | ||||
| P | 0.363 | 0.639 | 0.407 | 0.347 | 0.021* | 0.348 | 0.087 | 0.000** | - | ||||
| 8- TTS | 0.004 | −0.014 | −0.021 | −0.011 | −0.200 | −0.012 | −0.095 | 0.579 | 0.369 | 1.000 | |||
| P | 0.968 | 0.883 | 0.824 | 0.909 | 0.034* | 0.897 | 0.316 | 0.000** | 0.000** | - | |||
| 9- CDPRS-25 Total | −0.038 | 0.056 | −0.025 | −0.027 | −0.321 | −0.065 | −0.184 | 0.937 | 0.814 | 0.650 | 1.000 | ||
| P | 0.688 | 0.559 | 0.796 | 0.774 | 0.000** | 0.492 | 0.051 | 0.000** | 0.000** | 0.000** | - | ||
| 10- FA | −0.145 | 0.180 | −0.057 | −0.092 | −0.152 | −0.132 | −0.167 | 0.003 | 0.038 | 0.161 | 0.040 | 1.000 | |
| P | 0.126 | 0.056 | 0.546 | 0.334 | 0.107 | 0.162 | 0.077 | 0.978 | 0.691 | 0.089 | 0.678 | - | |
| 11- FR | −0.239 | 0.093 | −0.002 | −0.146 | −0.127 | −0.079 | −0.116 | 0.163 | 0.077 | 0.070 | 0.142 | 0.422 | 1.000 |
| P | 0.011* | 0.325 | 0.985 | 0.123 | 0.179 | 0.404 | 0.223 | 0.085 | 0.417 | 0.458 | 0.133 | 0.000** | - |
| 12- O | −0.223 | 0.111 | 0.007 | −0.127 | −0.088 | −0.043 | −0.071 | 0.110 | 0.037 | 0.026 | 0.087 | 0.396 | 0.945 |
| P | 0.018* | 0.243 | 0.945 | 0.181 | 0.353 | 0.651 | 0.455 | 0.246 | 0.698 | 0.78 | 0.360 | 0.000** | 0.000** |
| 13- MPSSS Total | −0.232 | 0.120 | −0.031 | −0.151 | −0.139 | −0.128 | −0.158 | 0.094 | 0.038 | 0.055 | 0.082 | 0.587 | 0.923 |
| P | 0.013* | 0.207 | 0.744 | 0.111 | 0.141 | 0.177 | 0.094 | 0.321 | 0.691 | 0.562 | 0.390 | 0.000** | 0.000** |
*P<0.05, **P<0.001. CDPRS 25: Connor-Davidson Psychological Resilience Scale 25, EORTC QLQ-BR23: European Organization for Research and Treatment of Cancer Quality of Life Breast Cancer Module 23, EORTC QLQ-C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30, MPSSS: Multidimensional Perceived Social Support Scale, FA: Family, FR: Friends, FS: Functional scale, GHS: General health status, O: Other (special person), SC: Symptom scale, TNE: Tolerance of negative effect, TPC: Tenacity and personal competence, TTS: Tendency toward spirituality
Mediating effect of social support on the relation between resilience and quality of life
The analysis as shown in Table 3 revealed the direct effect of psychological resilience on the EORTC BR23 functional subscale (β = –0.0601; P < 0.05) when the social support was not included in the model [Figure 1] as a mediating variable, and its indirect effect decreased when social support was included (β = –0.0566; P < 0.05). Accordingly, social support was determined to have a partial (10.2%) mediating variable role in the effect of psychological resilience on the EORTC BR23 functional subscale (R2 = 0.102). Psychological resilience had no direct effect on the EORTC BR23 symptom subscale when social support was not included in the model [Figure 2] as a mediating variable (β = –0.0177; P > 0.05), and there was no indirect effect when social support was included (β = –0.0132; P > 0.05; R2 = 0.0154).
Table 3.
Mediating effect of social support on quality of life (EORTC BR23)
| Mediating effect of social support | Total effect | Direct effect | Mediation effect | Bootstrap confidence interval (BootLLCI.BootMULCI) | R2 | Mediating effect |
|---|---|---|---|---|---|---|
| CDPRS 25- EORTC QLQ-BR23: FS | −0.0601 | −0.0566 | −0.003* | −0.0155-0.0024 | 0.102 | Partial effect |
| CDPRS 25- EORTC QLQ-BR23: SC | −0.017 | −0.013 | −0.0007 | −0.0033-0.0010 | 0.0154 | Reject |
*P<0.05. CDPRS 25: Connor-Davidson Psychological Resilience Scale 25, EORTC QLQ-BR23: European Organization for Research and Treatment of Cancer Quality of Life Breast Cancer Module 23, FS: Functional scale, SC: Symptom scale, LLCI: Lower Limit of the Confidence Interval, ULCI: Upper Limit of the Confidence Interval
The mediation model, social support, and standardized coefficients for each variable are shown in Figure 3. SEM revealed significant regression and correlation paths, and all beta path coefficients were not in the expected direction, and they were statistically nonsignificant (P > 0.05). Fit indices were used to test the conformity of the established structural equation model.[27] The GFIs were determined as χ2/df = 2.095, AGFI = 0.460, CFI = 0.664, GFI = 0.495, NFI = 0.512, IFI = 0.667, and RMSEA = 0.099. The model did not provide the index values, indicating goodness of fit, and social support had no mediating effect on the correlation between psychological resilience and QoL [EORTC C30; Table 4].
Table 4.
Hypothesis results in the context of structural equation modeling model of research
| Effect | Estimation | Standard error | t | P | Results |
|---|---|---|---|---|---|
| R → SS | 0.206 | 0.149 | 1.378 | 0.168 | Reject |
| SS → EORTC QLQ-C30 | −0.056 | 0.059 | −0.955 | 0.339 | Reject |
| R → EORTC QLQ-C30 | −0.028 | 0.083 | −0.337 | 0.736 | Reject |
Compliance indexes: χ2/df=2.095; AGFI=0.460; CFI=0.664; GFI=0.495; NFI=0.512; IFI=0.667; RMSEA=0.099. EORTC QLQ-C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30, R: Resistance, SS: Social support, AGFI: Adjusted Goodness of Comparative Fit Index, GFI: Goodness-of-Fit Index, CFI: Comparative Fit Index, IFI: Incremental Fit Index, NFI: Normed Fit Index, RMSEA: Root mean square error of approximation
Discussion
The results revealed that social support had a mediating variable role of 10.2% in the correlation between psychological resilience and functional QoL specific to breast cancer (R2 = 0.102). There was a negative correlation between functional QoL Questionnaire Breast Cancer 23 and psychological resilience and social support (P < 0.005). However, social support had no mediating role in overall QoL and psychological resilience.
In recent years, many psychosocial studies have been carried out on cancer aiming to determine the factors that affect the QoL and resilience of patients. Factors such as depressive symptoms,[17] hope,[28] and social support[11,29] have been studied as protective elements in patients with breast cancer. Zhang et al. investigated the role of mediators, that is, social support, in psychological resilience, and QoL in patients with breast cancer, and found that psychological resilience had a direct effect on QoL and an indirect effect on QoL through social support at a rate of 28%.[11] Cancer threatens one's independence and ability to actively interact with the family and society; therefore, cancer patients lack competence and self-confidence. In addition, the cancer diagnosis may affect or cause loss of personal, family, and social roles and may result in avoidance of social support systems.[30] The results of the study might be due to the patients' discovery that emotional support systems would not help them. Although psychosocial factors have a significant effect on the QoL of cancer patients, the needs of these patients cannot be met to a considerable extent.[31] The results revealed that the resources of psychosocial support offered to patients with breast cancer in Turkey were limited. Moreover, there are some insights into the neurobiological aspects. When patients with breast cancer perceive the stressful effects of breast cancer as well as the adverse effects associated with treatment, the hypothalamic–pituitary–adrenocortical (HPA) system containing the stress response is strongly activated.[11] The regulation of social support is mostly dependent on two neuropeptides (oxytocin and vasopressin) that can promote social behavior and prevent the transformation of the HPA axis reactivity into stress.[32,33] In this context, flexible individuals can contribute to social support systems via their brain mechanisms to maintain a state of psychological well-being.[11] There was a negative correlation between functional QoL and psychological resilience and social support. In addition, social support had a partial mediating effect on the correlation between psychological resilience and QoL by 10.2%. In contrast, it was considered that the patients may have attributed a negative meaning to these concepts when evaluated from a neurobiological perspective. The presence of a traditional family structure in Turkey, commitment of family members and relatives to each other, and consideration that neighbors should collaborate in times of difficulty may have influenced the results of the study. Patients do not want this support to end, and their weakness in the eyes of others may have a negative impact on their QoL. For this reason, the patients might have thought that the care and support provided to them would decrease if they appeared psychologically resilient, so they may have chosen to be psychologically weak. In addition, the fear that their family members or their spouse might abandon them especially when they needed support may have affected the patients' perception of psychological resilience and social support about QoL.
Limitations
The perception of social support may vary individually depending on the time when the patient needs it and difficult conditions. Collecting data from patients in an environment where they need support such as a hospital environment is the limitation of the study.
Conclusions
Social support has a mediating role of 10.2% in the correlation of psychological resilience with the functional QoL specific to Turkish women with early-stage breast cancer. However, social support does not play a mediating role in the correlation between overall QoL and psychological resilience. In breast cancer patients, social support resources can negatively affect psychological resilience and functional QoL. The quality of social support resources, as well as their quantity, offered to patients with breast cancer, should be evaluated by health professionals.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:359–86. doi: 10.1002/ijc.29210. [DOI] [PubMed] [Google Scholar]
- 2.Turkey Cancer Cancer Statistics: Public Health Agency of Turkey. 2017. [Last accessed on 2019 Apr 19]. Available from: https://hsgmsaglikgovtr/tr/kanser-istatistikleri .
- 3.Zhang T, Li H, Liu A, Wang H, Mei Y, Dou W. Factors promoting resilience among breast cancer patients: A qualitative study. Contemp Nurse. 2018;54:293–303. doi: 10.1080/10376178.2018.1502615. [DOI] [PubMed] [Google Scholar]
- 4.Davis CM, Myers HF, Nyamathi AM, Lewis M, Brecht ML. The meaning of survivorship as defined by African American breast cancer survivors. J Transcult Nurs. 2016;27:277–85. doi: 10.1177/1043659614561678. [DOI] [PubMed] [Google Scholar]
- 5.Sammarco A. Quality of life of breast cancer survivors: A comparative study of age cohorts. Cancer Nurs. 2009;32:347–56. doi: 10.1097/NCC.0b013e31819e23b7. [DOI] [PubMed] [Google Scholar]
- 6.Di Giacomo D, Cannita K, Ranieri J, Cocciolone V, Passafiume D, Ficorella C. Breast cancer and psychological resilience among young women. J Psychopathol. 2016;22:191–5. [Google Scholar]
- 7.Schroevers MJ, Helgeson VS, Sanderman R, Ranchor AV. Type of social support matters for prediction of posttraumatic growth among cancer survivors. Psycho Oncol. 2010;19:46–53. doi: 10.1002/pon.1501. [DOI] [PubMed] [Google Scholar]
- 8.Henry BJ. Quality of life and resilience: Exploring a fly fishing intervention for breast cancer survivors. Clin J Oncol Nurs. 2017;21:9–14. doi: 10.1188/17.CJON.E9-E14. [DOI] [PubMed] [Google Scholar]
- 9.Knobf MT. Clinical update: Psychosocial responses in breast cancer survivors. Seminars in Oncol Nurs. 2011;27:1–14. doi: 10.1016/j.soncn.2011.05.001. [DOI] [PubMed] [Google Scholar]
- 10.Pedersen AE, Sawatzky JA, Hack TF. The sequelae of anxiety in breast cancer: A human response to illness model. Oncol Nurs Forum. 2010;37:469–75. doi: 10.1188/10.ONF.469-475. [DOI] [PubMed] [Google Scholar]
- 11.Zhang H, Zhao Q, Cao P, Ren G. Resilience and quality of life: Exploring the mediator role of social support in patients with breast cancer. Med Sci Monit. 2017;23:5969–79. doi: 10.12659/MSM.907730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ristevska-Dimitrovska G, Stefanovski P, Smichkoska S, Raleva M, Dejanova B. Depression and resilience in breast cancer patients. Open Access J Maced Med Sci. 2015;3:661–5. doi: 10.3889/oamjms.2015.119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Min JA, Yoon S, Lee CU, Chae JH, Lee C, Song KY, et al. Psychological resilience contributes to low emotional distress in cancer patients. Support Care Cancer. 2013;21:2469–76. doi: 10.1007/s00520-013-1807-6. [DOI] [PubMed] [Google Scholar]
- 14.Alizadeh S, Khanahmadi S, Vedadhir A, Barjasteh S. The relationship between resilience with self-compassion, social support and sense of belonging in women with breast cancer. Asian Pac J Cancer Prev. 2018;19:2469–74. doi: 10.22034/APJCP.2018.19.9.2469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ülger E, Alacacıoǧlu A, Gülseren AŞ, Zencir G, Demir L, Tarhan MO. Psychosocıal problems in cancer and the importance of psychosocıal oncology. Dokuz EylüÜniversitesi Tıp Fakültesi Dergisi. 2014;28:85–92. [Google Scholar]
- 16.Kroenke CH, Quesenberry C, Kwan ML, Sweeney C, Castillo A, Caan BJ. Social networks, social support, and burden in relationships, and mortality after breast cancer diagnosis in the Life after Breast Cancer Epidemiology (LACE) study. Breast Cancer Res Treat. 2013;137:261–71. doi: 10.1007/s10549-012-2253-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Huang CY, Hsu MC. Social support as a moderator between depressive symptoms and quality of life outcomes of breast cancer survivors. Eur J Oncol Nurs. 2013;17:767–74. doi: 10.1016/j.ejon.2013.03.011. [DOI] [PubMed] [Google Scholar]
- 18.Ng CG, Mohamed S, See MH, Harun F, Dahlui M, Sulaiman AH, et al. Anxiety, depression, perceived social support and quality of life in Malaysian breast cancer patients: A 1-year prospective study. Health Qual Life Outcomes. 2015;13:205. doi: 10.1186/s12955-015-0401-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hill TD, Kaplan LM, French MT, Johnson RJ. Victimization in early life and mental health in adulthood: An examination of the mediating and moderating influences of psychosocial resources. J Health Soc Behav. 2010;51:48–63. doi: 10.1177/0022146509361194. [DOI] [PubMed] [Google Scholar]
- 20.Boyle P, Levin B. World cancer report 2008 IARC Press, International Agency for Research on Cancer (serial online) 2008. [Last accessed on 2019 Apr 19]. Available from: https://publicationsiarcfr/Non-Series-Publications/World-Cancer-Reports/World-Cancer-Report-2008 .
- 21.Connor KM, Davidson JR. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC) Depression Anxiety. 2013;18:76–82. doi: 10.1002/da.10113. [DOI] [PubMed] [Google Scholar]
- 22.Karaırmak Ö. Establishing the psychometric qualities of the Connor–Davidson Resilience Scale (CD-RISC) using exploratory and confirmatory factor analysis in a trauma survivor sample. Psychiatry Res. 2010;179:350–6. doi: 10.1016/j.psychres.2009.09.012. [DOI] [PubMed] [Google Scholar]
- 23.Eker D, Arkar H. The factorial structure, reliability and validity of the multidimensional social support scale. Tük Psikoloji Dergisi. 1995;10:45–55. [Google Scholar]
- 24.Guzelant A, Goksel T, Ozkok S, Tasbakan S, Aysan T, Bottomley A. The European organization for research and treatment of cancer QLQ-C30: An examination into the cultural validity and reliability of the Turkish version of the EORTC QLQ-C30. Eur J Cancer Care. 2004;13:135–44. doi: 10.1111/j.1365-2354.2003.00435.x. [DOI] [PubMed] [Google Scholar]
- 25.Demirci S, Eser E, Ozsaran Z, Tankisi D, Aras AB, Ozaydemir G, et al. Validation of the Turkish versions of EORTC QLQ-C30 and BR23 modules in breast cancer patients. Asian Pac J Cancer Prev. 2011;12:1283–7. [PubMed] [Google Scholar]
- 26.HayesAndrew F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression- Based Approach. New York: The Guilford Press; 2013. [Google Scholar]
- 27.Şimşek ÖF. Introduction to structural equation modeling (Basic principles and LISREL applications) Ankara: Ekinoks Press; 2007. [Google Scholar]
- 28.Saboonchi F, Petersson LM, Alexanderson K, Branstrom R, Wennman-Larsen A. Expecting the best and being prepared for the worst: Structure, profiles, and 2-year temporal stability of dispositional optimism in women with breast cancer. Psycho Oncol. 2016;25:957–63. doi: 10.1002/pon.4045. [DOI] [PubMed] [Google Scholar]
- 29.Spatuzzi R, Vespa A, Lorenzi P, Miccinesi G, Ricciuti M, Cifarelli W, et al. Evaluation of social support, quality of life, and body image in women with breast cancer. Breast Care. 2016;11:28–32. doi: 10.1159/000443493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Talepasand S, Pooragha F, Kazemi M. Resiliency and quality of life in patients with cancer: Moderating role of duration of awareness of cancer. Iran J Cancer Prev. 2013;6:222–6. [PMC free article] [PubMed] [Google Scholar]
- 31.Barg FK, Cronholm PF, Straton JB, Keddem S, Knott K, Grater J, et al. Unmet psychosocial needs of Pennsylvanians with cancer: 1986-2005. Cancer. 2007;110:631–9. doi: 10.1002/cncr.22820. [DOI] [PubMed] [Google Scholar]
- 32.Bartz JA, Hollander E. The neuroscience of affiliation: Forging links between basic and clinical research on neuropeptides and social behavior. Horm Behav. 2006;50:518–28. doi: 10.1016/j.yhbeh.2006.06.018. [DOI] [PubMed] [Google Scholar]
- 33.Ozbay F, Fitterling H, Charney D, Southwick S. Social support and resilience to stress across the life span: A neurobiologic framework. Curr Psychiatry Rep. 2008;10:304–10. doi: 10.1007/s11920-008-0049-7. [DOI] [PubMed] [Google Scholar]