

Abstract
Background:
Female athletes have a higher rate of anterior cruciate ligament (ACL) injuries than male athletes; however, the role of age in mediating this injury risk has not been explored. The purpose of this study was to characterize the relationship between age and sex in predicting ACL injury in the pediatric population.
Hypothesis:
Prepubescent boys are more likely to sustain an ACL injury than prepubescent girls.
Study Design:
Descriptive epidemiological study.
Level of Evidence:
Level 4.
Methods:
Data were collected from the Statewide Planning and Research Cooperative System database for the state of New York from 1996 to 2016. The database was queried for patients aged ≤19 years who had been diagnosed with an ACL tear using the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) code 844.2 or the ICD-10 (10th Revision) codes S83.512A/S83.511A/S83.519A. Patient age and sex at time of ACL injury diagnosis were recorded. Chi-square analysis was used to compare the frequency of ACL injury between groups, with statistical significance set atP < 0.05.
Results:
A total of 20,128 patients aged ≤19 years were diagnosed with an ACL tear (10,830 males, 9298 females; male:female, 1.16:1). In all, 129 patients aged <12 years sustained an ACL tear (85 boys, 44 girls; male:female, 1.93:1), and 19,999 of those patients were aged 12 to 19 years (10,745 males, 9254 females; male:female, 1.16:1). Chi-square analysis demonstrated a significant relationship between sex and age group (P < 0.006). Additional analysis revealed that female athletes were most at risk for ACL injury from ages 12 to 16 years, with 4025 male and 5095 female athletes sustaining ACL injuries in this group (male:female, 1:1.27; P < 0.0001).
Conclusion:
Prepubescent boys (aged <12 years) are more likely to sustain an ACL injury than same-aged female peers.
Clinical Relevance:
This study demonstrates that the risk of ACL injury varies with age and sex throughout childhood and adolescence, further guiding treatment and prevention for these pediatric athletes.
Keywords: pediatrics, ACL, anterior cruciate ligament, incidence, orthopaedics
Knee injuries represent the majority of sports injuries requiring surgical intervention in young athletes. Anterior cruciate ligament (ACL) tears represent half of these injuries, with almost 200,000 arthroscopic ACL reconstructions performed each year.17 ACL injuries are rare, yet severe, among skeletally immature patients.
Despite their relative rarity, the incidence of these injuries has been steadily increasing in recent years.3 The reason for this is likely due to the increased and early participation in organized sports.18 The incidence of ACL tears in this population appears to be increasing, with patients presenting at younger ages.1,13,28 This is thought to involve early sports participation and specialization, as more young athletes are playing just 1 sport for the majority of the year.7,8
Female athletes are at a higher risk of ACL injury than their male counterparts.2,15 This relationship has been studied in many populations and at many levels of play.20 Previous literature, some of which has utilized the Statewide Planning and Research Cooperative System (SPARCS) database, has documented a rising rate of ACL reconstruction among the pediatric population.6 However, there is a paucity of research regarding the effect of age on sex-based differences in ACL injury incidence.
The purpose of this article was to characterize the effects of age and sex in predicting the prevalence of ACL injuries in a pediatric population. We hypothesized that prepubescent boys were more likely to sustain an ACL injury than their same-aged female peers.
Methods
A retrospective review of a Health Insurance Portability and Accountability Act–compliant database was conducted using the SPARCS database for the state of New York from 1996 to 2016, which did not require institutional review board approval. This database was then queried according to the following inclusion criteria: patients aged ≤19 years who had been diagnosed with an ACL tear, as determined by the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9 CM) code 844.2 or the ICD-10 (10th Revision) codes S83.512A/S83.511A/S83.519A. We then recorded each patient’s sex and age at the time of ACL diagnosis for statistical analysis.
The SPARCS database allowed us to determine the relative incidence of ACL injury between male and female patients. This database, unfortunately, does not allow for demonstration of primary versus reinjury, nor can it give specific historical information, such as injury mechanism. To investigate age-based differences in the incidence of ACL injury, patients were grouped to reflect standard stages of physical development. Prepubertal patients were defined as 11 years of age and younger, ages 12 to 16 years were defined as pubertal, and ages 17 to 19 years were defined as late puberty/postpuberty. These groups were then analyzed as described below.
We utilized GraphPad Prism 8.0 (GraphPad Software) to conduct our statistical analysis. Chi-square analysis was used to compare the incidence of ACL injury for the categorical variables: age and sex. Statistical significance was set at P < 0.05.
To better characterize the rates of ACL injury, rather than simply ACL injury incidence, we utilized age- and sex-matched New York State census data to calculate the rate of ACL injury per 100,000 people for each year of the study period. The Student t test was then used to analyze the rate of ACL injury as a function of age and sex, with statistical significance set at P < 0.05.
Results
The SPARCS database yielded 20,137 patients; 9 of these had to be excluded because of incomplete demographic information. Ultimately, 20,128 patients met the inclusion criteria for this study, 10,830 of whom were male and 9298 of whom were female. This represents an overall male to female ratio of 1.16:1. Average age at the time of diagnosis for all patients was 16.55 ± 1.70 years (range, <1-19 years). Average age at diagnosis for female athletes was 16.23 ± 1.68 years (range, <1-19 years), while male patients were diagnosed at an average age of 16.83 ± 1.67 years (range, <1-19 years) (P < 0.0001). The distribution of ACL tears as a function of age and sex is depicted in Figure 1.
Figure 1.
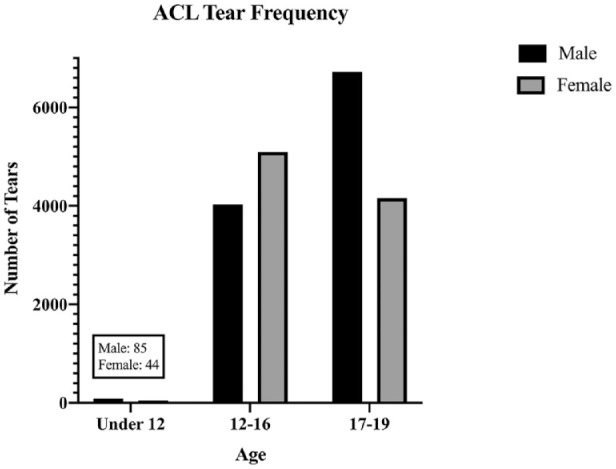
Incidence of anterior cruciate ligament (ACL) tear separated by 3 age cohorts.
A total of 129 patients were younger than 12 years of age. Among this group, 85 male and 44 female athletes were diagnosed with an ACL injury, representing a male:female ratio of 1.93:1. In all, 19,999 patients with an ACL injury between the ages of 12 and 19 years were identified. This group had 10,745 male and 9254 female athletes, representing a male:female ratio of 1.16:1. Chi-square analysis demonstrated a statistically significant difference in incidence by sex between the 2 age groups (P < 0.006). Athletes younger than 12 years of age with an ACL tear were significantly more likely to be male.
Conversely, there was a higher incidence of ACL injury reported in girls between the ages of 12 and 16 years compared with their male counterparts. A total of 4025 boys and 5095 girls were treated for an ACL injury in this age range (male:female, 1:1.27; P < 0.0001). There were 6720 male and 4159 female athletes between 17 and 19 years of age at the time of diagnosis in this cohort, representing a ratio of 1.61:1 (P < 0.0001). These data are represented in Figure 2.
Figure 2.
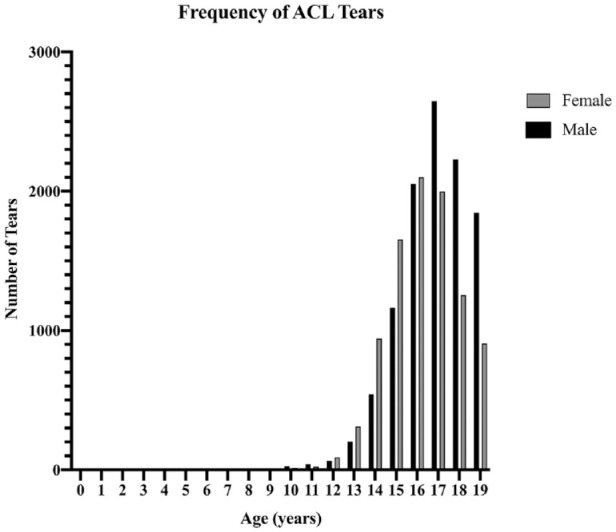
Incidence of anterior cruciate ligament (ACL) tear by sex and age at diagnosis.
Using age- and sex-matched New York State census data, an average annual rate was calculated or ACL injury in male adolescents <12 years of age to be 5.0 ± 2.9 per 100,000; this rate was significantly greater than that calculated for female athletes younger than 12 years of age, which was 2.8 ± 2.1 per 100,000 (P = 0.042). The current study reports a calculated average annual rate of ACL injury in boys 12 to 16 years old to be 243 ± 63 per 100,000, significantly lower than 322 ± 66 per 100,000, the rate for similarly aged girls (P = 0.006). Last, the calculated average yearly rate of ACL injury in male adolescents aged 17 to 19 years was 399 ± 98 per 100,000. This number was significantly greater than the 260 ± 58 per 10,000 rate calculated for 17- to 19-year-old female adolescents (P < 0.001). These findings are depicted in Figure 3.
Figure 3.
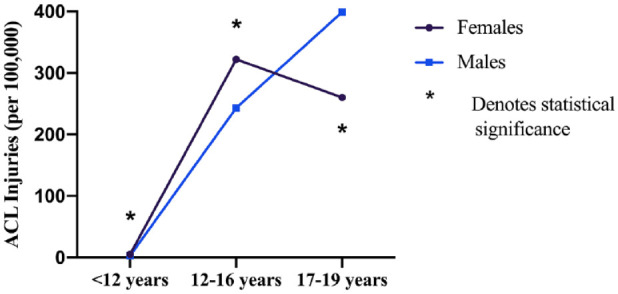
Rate of anterior cruciate ligament (ACL) tear by sex and age at diagnosis.
Discussion
The relationship between sex and age was characterized in predicting risk of ACL injury in pediatric athletes. Previous research has shown that young female athletes were at a greater risk of ACL injury than their male counterparts, but data were limited with regard to the effect of age on this relationship, particularly for the youngest athletes. We hypothesized that prepubescent boys were more likely to be treated for an ACL injury than similarly aged girls.
The data demonstrate that, among pediatric athletes aged <12 years, male athletes have almost twice the rate of ACL injuries as their female peers. This finding is reinforced by small-scale prospective studies investigating outcomes of prepubescent ACL reconstruction. Koch et al12 investigated epiphyseal reconstruction of torn ACLs in 12 athletes aged 10 to 13 years. Of note, postoperative outcomes among their cohort were generally good, and their study group was 83.3% (n = 10) male.12 Our findings were more similar to those from a systematic review by Kaeding et al,10 which analyzed surgical techniques and outcomes in 13 studies looking at ACL reconstruction among preadolescent athletes. In that systematic review, the authors found 73.2% (n = 137) of athletes were male, a similar number to our own study, which found that 65.9% (n = 85) of athletes were male.10 Of note, our findings report higher incidence of ACL injury per 100,000 people than a similar study by Dodwell et al,6 which examined rates of pediatric ACL reconstruction in New York State. This is likely due to a combination of 2 factors. First, this study period included 6 additional years of data, and a year-over-year increase in the rate of pediatric ACL reconstruction has been consistently reported; moreover, the overall rate of pediatric ACL reconstruction has likely increased since their findings were published. Second, it may still be the case that not every child who presents for treatment of an ACL injury is offered and/or elects to pursue surgical reconstruction.6
One explanation for the higher rate of ACL injury demonstrated in prepubescent male athletes is the observed variance in level of sport participation among young children of different sexes.22 This explanation is limited, as data from the Women’s Sports Foundation demonstrate that youth participation in sport is higher among boys throughout all levels of youth play.22 However, it is important to note that participation in organized sports has been shown to be a risk factor for ACL injury. Nationally, boys play organized sports at a higher rate than girls.11,27 This difference is especially pronounced in urban areas as well as in younger ages.23 Therefore, this increased risk is likely attributable, in part, to increased organized sport exposure.
Our data, demonstrating that the increased rate in female athletes begins around puberty, support many of these theories, especially the anatomic and biomechanical hypotheses. As girls typically reach their growth spurt before boys, it would make sense that the effects of this rapid growth period are first evident in girls.21,25 Rapid growth elongates both the tibia and the femur, increasing the torque on the knee.13,26 Additionally, increased height and body weight shifts the center of mass superiorly. All these factors combine to increase stress on the knee and decrease control of the center of mass, making the young athlete more prone to injury.13 During the male pubertal growth spurt, increase in muscle mass is protective against some of these effects.13 Increased muscle strength takes some of the strain off the static components of the joint, such as the ACL.16,19 Prior to puberty and a period of rapid growth, increased sports participation by young boys likely is the predominant factor in contributing to risk of injury; yet after this point, these other risk factors cause female athletes to be at greater risk.
Interestingly, this relationship changes again after puberty, with male patients aged 17 to 19 years being more likely than female patients to sustain an injury to the ACL. This drop-off in the relative risks of ACL injury may be explained, at least in part, by the high rates of sport attrition that have been reported for postpubertal female athletes.14,24
Additionally, prior knee injury is associated with a greater risk of ACL injury.5,9 Pediatric patients undergoing ACL reconstruction have a high rate of both graft failure and contralateral ACL tear.5,9 Studies have shown that this often occurs before clearance to return to full activity and is likely caused by pediatric athletes’ high levels of activity and difficulty adhering to postoperative restriction from sports.4 It is important to ensure that pediatric athletes and their families are cognizant of and understand the importance of activity restrictions during recovery.
While many risks of ACL injury are not modifiable, research has shown promise in neuromuscular training to prevent ACL injury.20 These programs train athletes to avoid common motions and situations that make them prone to ACL injury as well as provide strength and balance training.18,20
These data demonstrate that the interactions between age, sex, and ACL injury risk are complex, with the incidence of ACL injury being higher in prepubertal boys and pubertal girls. Thus, rather than depicting an “epidemic” of ACL injuries in young female athletes, it appears that the risk of sustaining an ACL injury is variable throughout the pediatric and adolescent years, with both physiologic factors (eg, hormone levels and body composition) and sociologic factors (eg, rate and level of sport participation) likely contributing to a young athlete’s overall risk.
Limitations
This study has significant limitations. First, although the SPARCS database is a powerful tool for retrospectively conducted epidemiological studies such as this, there are inherent limitations associated with a retrospective analysis of a large database. Database studies are limited by the differences in recording and reporting of data between various hospitals, and the outcome measurements are also limited. Additionally, this study is based on the recorded date of diagnosis of ACL injury, but we have no way of knowing actual age of injury based on these data. That said, this study would not have been feasible with regard to scale if designed prospectively. Additionally, as noted above, this study looked at the simple incidence of ACL injury and calculated the rate of injury within the population of New York State, rather than the rate of ACL injury as a function of athletic exposures, which is more commonly reported in the sports literature. Last, these data were collected from 1996 to 2016, and as such, may be of somewhat limited use at present.
Conclusion
While pubertal female athletes in New York State do have a greater overall rate of ACL injury than age-matched male athletes, prepubescent males have a significantly higher rate of ACL injury than their same-aged female peers. This relationship may be due in part to differences in rates of youth sports participation between young boys and girls, although it is also likely that anatomic, biomechanical, and hormonal sex-based differences contribute to the increased risk of ACL injury observed in pubertal girls. Ultimately, the results of this study demonstrate a complex relationship between sex and stage of physiologic development, which underpins an individual’s risk for ACL injury. Understanding this should, in turn, allow us to better individualize ACL injury screening and prevention programs for all pediatric athletes.
Acknowledgments
We would like to acknowledge Debra Sala for her help with this project.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Ardern CL, Ekås G, Grindem H, et al. 2018 International Olympic Committee consensus statement on prevention, diagnosis and management of paediatric anterior cruciate ligament (ACL) injuries. Knee Surg Sports Traumatol Arthrosc. 2018;26:989-1010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. Am J Sports Med. 1995;23:694-701. [DOI] [PubMed] [Google Scholar]
- 3. Beck NA, Lawrence JTR, Nordin JD, DeFor TA, Tompkins M. ACL tears in school-aged children and adolescents over 20 years. Pediatrics. 2017;139:e20161877. [DOI] [PubMed] [Google Scholar]
- 4. DeFrancesco CJ, Storey EP, Flynn JM, Ganley TJ. Pediatric ACL reconstruction and return to the operating room: revision is less than half of the story. J Pediatr Orthop. 2019;39:516-520. [DOI] [PubMed] [Google Scholar]
- 5. Dekker TJ, Godin JA, Dale KM, Garrett WE, Taylor DC, Riboh JC. Return to sport after pediatric anterior cruciate ligament reconstruction and its effect on subsequent anterior cruciate ligament injury. J Bone Joint Surg Am. 2017;99:897-904. [DOI] [PubMed] [Google Scholar]
- 6. Dodwell ER, LaMont LE, Green DW, Pan TJ, Marx RG, Lyman S. 20 Years of pediatric anterior cruciate ligament reconstruction in New York State. Am J Sports Med. 2014;42:675-680. [DOI] [PubMed] [Google Scholar]
- 7. Fabricant PD, Kocher MS. Anterior cruciate ligament injuries in children and adolescents. Orthop Clin North Am. 2016;47:777-788. [DOI] [PubMed] [Google Scholar]
- 8. Field AE, Tepolt FA, Yang DS, Kocher MS. Injury risk associated with sports specialization and activity volume in youth. Orthop J Sports Med. 2019;7:2325967119870124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Ho B, Edmonds EW, Chambers HG, Bastrom TP, Pennock AT. Risk factors for early ACL reconstruction failure in pediatric and adolescent patients: a review of 561 cases. J Pediatr Orthop. 2018;38:388-392. [DOI] [PubMed] [Google Scholar]
- 10. Kaeding CC, Flanigan D, Donaldson C. Surgical techniques and outcomes after anterior cruciate ligament reconstruction in preadolescent patients. Arthroscopy. 2010;26:1530-1538. [DOI] [PubMed] [Google Scholar]
- 11. Kanters MA, Bocarro JN, Edwards MB, Casper JM, Floyd MF. School sport participation under two school sport policies: comparisons by race/ethnicity, gender, and socioeconomic status. Ann Behav Med. 2012;45(suppl 1):S113-S121. [DOI] [PubMed] [Google Scholar]
- 12. Koch PP, Fucentese SF, Blatter SC. Complications after epiphyseal reconstruction of the anterior cruciate ligament in prepubescent children. Knee Surg Sports Traumatol Arthrosc. 2016;24:2736-2740. [DOI] [PubMed] [Google Scholar]
- 13. LaBella CR, Hennrikus W, Hewett TE. Anterior cruciate ligament injuries: diagnosis, treatment, and prevention. Pediatrics. 2014;133:e1437-e1450. [DOI] [PubMed] [Google Scholar]
- 14. Lin CY, Casey E, Herman DC, Katz N, Tenforde AS. Sex differences in common sports injuries. PM R. 2018;10:1073-1082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Lindenfeld TN, Schmitt DJ, Hendy MP, Mangine RE, Noyes FR. Incidence of injury in indoor soccer. Am J Sports Med. 1994;22:364-371. [DOI] [PubMed] [Google Scholar]
- 16. Lipps DB, Oh YK, Ashton-Miller JA, Wojtys EM. Morphologic characteristics help explain the gender difference in peak anterior cruciate ligament strain during a simulated pivot landing. Am J Sports Med. 2012;40:32-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Musahl V, Karlsson J. Anterior cruciate ligament tear. N Engl J Med. 2019;380:2341-2348. [DOI] [PubMed] [Google Scholar]
- 18. Myer GD, Sugimoto D, Thomas S, Hewett TE. The influence of age on the effectiveness of neuromuscular training to reduce anterior cruciate ligament injury in female athletes: a meta-analysis. Am J Sports Med. 2013;41:203-215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Nagano Y, Ida H, Akai M, Fukubayashi T. Gender differences in knee kinematics and muscle activity during single limb drop landing. Knee. 2007;14:218-223. [DOI] [PubMed] [Google Scholar]
- 20. Noyes FR, Barber-Westin SD. Neuromuscular retraining intervention programs: do they reduce noncontact anterior cruciate ligament injury rates in adolescent female athletes? Arthroscopy. 2014;30:245-255. [DOI] [PubMed] [Google Scholar]
- 21. Perry RJ, Farquharson C, Ahmed SF. The role of sex steroids in controlling pubertal growth. Clin Endocrinol (Oxf). 2008;68:4-15. [DOI] [PubMed] [Google Scholar]
- 22. Sabo D, Veliz P. Go Out and Play: Youth Sports in America. Women’s Sports Foundation; 2008. [Google Scholar]
- 23. Sabo D, Veliz P. Progress Without Equity: The Provision of High School Athletic Opportunity in the United States, by Gender 1993-94 Through 2005-06. Women’s Sports Foundation; 2011. [Google Scholar]
- 24. Senne JA. Examination of gender equity and female participation in sport. Sport J. 2016;19:1-9. [Google Scholar]
- 25. Soliman A, De Sanctis V, Elalaily R, Bedair S. Advances in pubertal growth and factors influencing it: can we increase pubertal growth? Indian J Endocrinol Metab. 2014;18(suppl 1):S53-S62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Stracciolini A, Stein CJ, Zurakowski D, Meehan WP, 3rd, Myer GD, Micheli LJ. Anterior cruciate ligament injuries in pediatric athletes presenting to sports medicine clinic: a comparison of males and females through growth and development. Sports Health. 2015;7:130-136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Veliz P, Shakib S. Gender, Academics and interscholastic sports participation at the school level: a gender-specific analysis of the relationship between interscholastic sports participation and AP enrollment. Sociol Focus. 2014;47:101-120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Werner BC, Yang S, Looney AM, Gwathmey FW., Jr. Trends in pediatric and adolescent anterior cruciate ligament injury and reconstruction. J Pediatr Orthop. 2016;36:447-452. [DOI] [PubMed] [Google Scholar]