

Summary:
Tongue cancer is the most common malignant neoplasm of the oral cavity. Occurrence in the tip of the tongue (TOT) is rare. We describe a case report of a TOT tumor excision and reconstruction with a prelaminated fasciomucosal radial forearm free flap. A 41-year-old white man was referred to our department for a squamous cell carcinoma of the tip of the tongue. The patient worked as an air traffic control official; therefore, conservation of speech intelligibility, both in Italian and English language, was of paramount importance. A transoral excision of TOT, bilateral selective neck dissection, and reconstruction with prelaminated fasciomucosal radial forearm free flap were performed. Adjuvant radiotherapy was necessary. The patient was completely re-established as an air traffic control officer. Successful tongue reconstruction of smaller defects depends on thinness, pliability of flap, and conservation of tongue mobility. Surgical options for TOT reconstruction are facial artery muscolomucosa flap, Zhao flap, radial forearm free flap, or primary suture. In the authors’ opinion, a fasciomucosal prelaminated RFFF offers a series of advantages for TOT reconstruction. The absence of subcutaneous tissue makes the PFRFFF much thinner than fascio-cutaneous flaps. Compared with mucosal loco-regional flaps, prelaminated flaps allow the preservation of oral mucosa lining while providing adequate bulk and reduced scar formation for optimal func- tional recovery. In our case report, the fasciomucosal flap allowed an adequate reconstruction of TOT volume with good functional and aesthetic outcomes. The flap’s added bulk and its minimal scar retraction granted free tongue movement and optimal speech intelligibility.
Tongue cancer is the most common malignant neoplasm of the oral cavity and its incidence has increased over the past 30 years.1,2 While most tumors originate in the lateral border, occurrence in the tip of the tongue (TOT) is rare.3 The tongue is crucial for articulation, speech, swallowing, and mastication.4 Radical resections of tongue cancer often result in large defects and function impairment, with a great impact on post-operative quality of life.5,6 Thus, reconstruction following tongue cancer resection remains one of the most challenging problems in head and neck oncology.7 With the advances in microsurgical techniques, tongue reconstruction must be aimed not only toward the replacement of deficient tissue, but also toward the recovery of its functions.8 TOT plays a major role in speech intelligibility and serves as an indicator for subjective and objective speech outcome.6 Tumor involving TOT can result in a distorted contact with the alveolar ridge or palate, thus intensifying speech disorders.2,9 Although postoperative function is influenced by multiple factors, restoration of the tongue’s bulk and mobility is essential to achieve optimal outcomes.7 However, there is no consensus regarding the most appropriate reconstructive method in partial glossectomies.5 We describe a case report of a TOT tumor excision and reconstruction with a prelaminated fasciomucosal radial forearm free flap (PFRFFF).
CASE REPORT
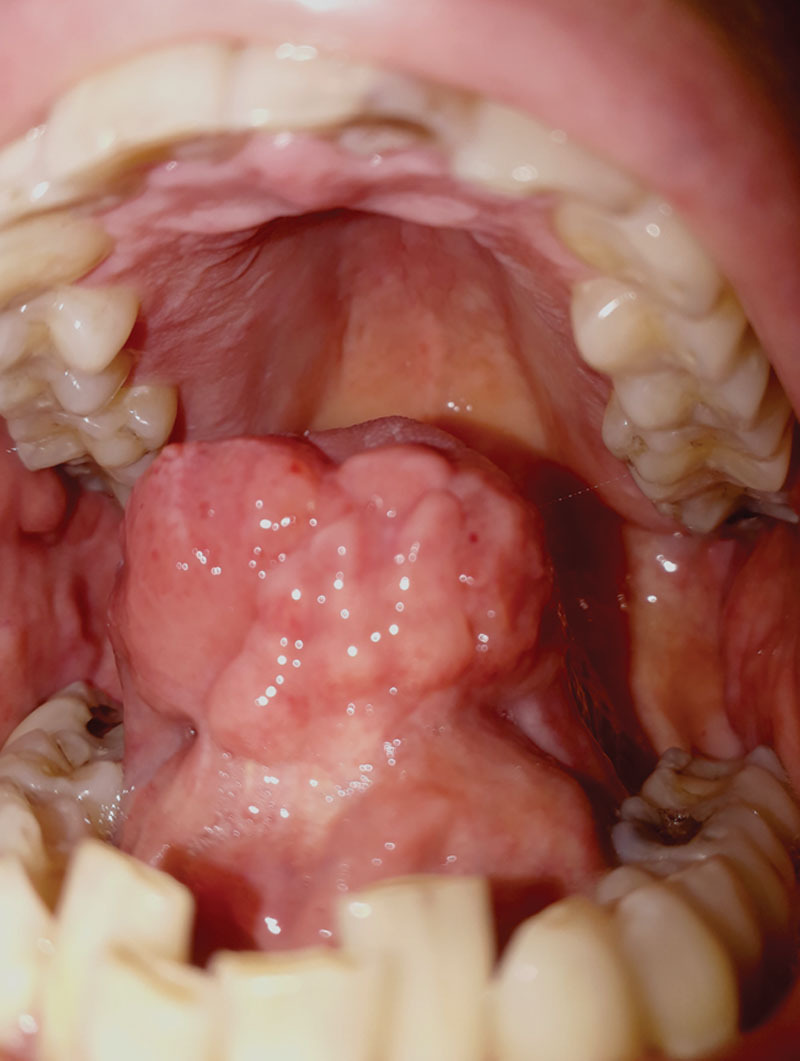
A 41-year-old white man was referred to our department for a painless ulcerated TOT lesion that had been growing for over a year (Fig. 1). The patient had a silent medical history and presented no risk factors for oral cancer. A biopsy of the lesion was performed as well as a neck contrast enhanced MRI and chest CT scan. The patient was diagnosed with a squamous cell carcinoma G3 HPV of the tip of the tongue (cT2cN0cM0). The patient worked as an air traffic control official; therefore, conservation of speech intelligibility, both in Italian and English language, was of paramount importance. A transoral excision of TOT, bilateral selective neck dissection, and reconstruction with PFRFFF were proposed.
Fig. 1.

Ulcerated lesion of the tip of the tongue upon the patient’s referral.
A mucosal island flap of 4 × 3 cm was harvested from the right cheek and morselized into smaller pieces, which were individually disposed over the left antibrachialis fascia (right hand dominant) (Figs. 2, 3). A silicone sheet was placed over the grafts between mucosa and subcutaneous tissue to maintain a cleavage plane, control cellular growth on the horizontal line, and prevent adhesion.
Fig. 2.
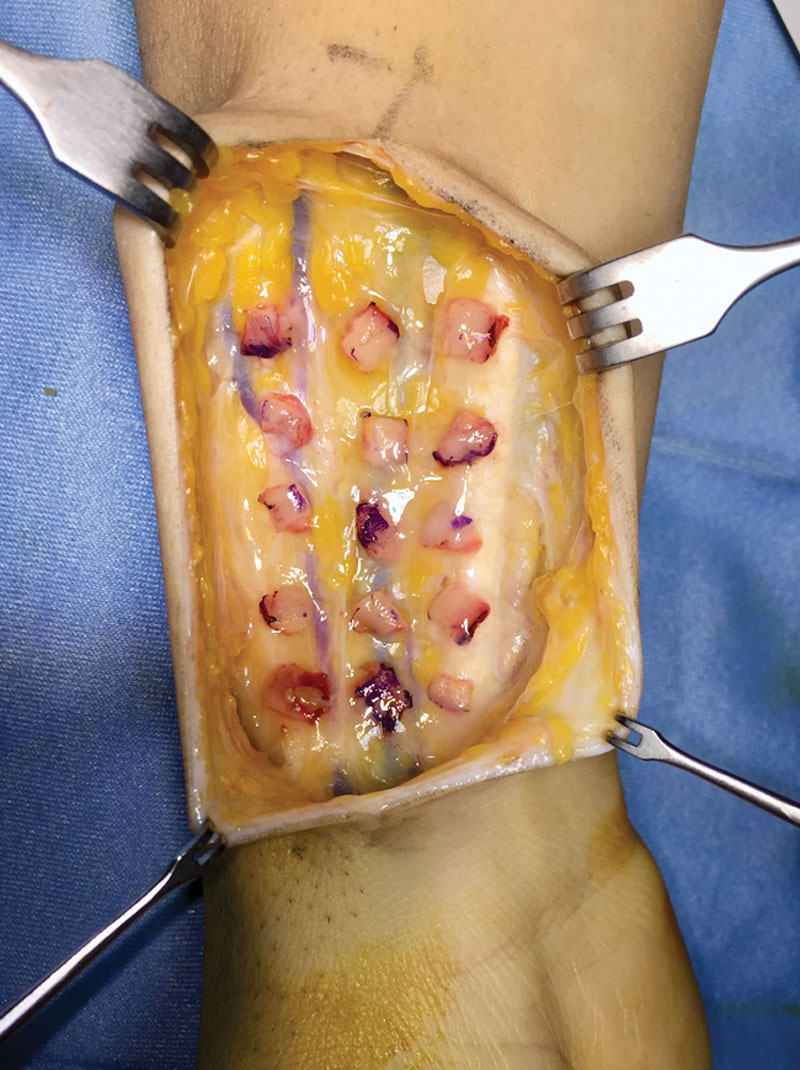
Morselized buccal mucosa grafts placed over the left antibrachialis fascia.
Fig. 3.

Morselized buccal mucosa grafts after 3 weeks.
The donor site was closed primarily with an absorbable suture. After 21 days the patient underwent an anterior glossectomy with total removal of TOT, bilateral selective neck dissection of levels I–III, and TOT reconstruction with fasciomucosal PFRFFF. Final stage pT2 pN1 (1/66, ECS-) cM0.
Post-operative course was uneventful. The donor site healed completely without the need of further intervention. Nasogastric feeding tube was removed in postoperative day 6. The patient was dismissed 10 days after surgery, with a normal diet. Due to disease stage and lymph node involvement, adjuvant radiotherapy was performed. Speech rehabilitation was initiated 3 weeks after surgery.
Six months after the end of adjuvant treatment, the reconstruction appeared well stabilized with an optimal mucosal lining apposition between flap and residual tongue (Fig. 4). The patient passed the examination test by the Italian Civil Aviation Authority and was completely re-established as an air traffic control officer. At 30 months after surgery, the patient maintains no evidence of disease status.
Fig. 4.
PRFFF outcome 1 year after surgery.
DISCUSSION
The tip of the tongue has a major role in consonant production. Dental consonants require TOT-teeth contact, and alveolar consonants are produced with short distances between the TOT and alveolar ridge.9,10 Patients with TOT preservation show significantly less decline in intelligibility than those with resection of the tip.7 Successful tongue reconstruction of smaller defects depends on thinness, pliability of flap and conservation of tongue mobility. Several authors have demonstrated that radial forearm free flap (RFFF) can be a viable first choice for small to hemiglossectomy defect reconstruction.5,8,11,12 An ideal reconstruction should replace the deficient tissue with one of similar size, volume and texture. The challenge of TOT reconstruction lies in the perfecting of cosmesis and function and not the only replacement of deficient tissue.12
Prelaminated oral mucosa has been implemented in oral cavity and facial defect reconstruction.13–17 Due to a high cell renewal rate, morselized buccal mucosa grafts can spread over a vascularized fascial bed and become functional in 3 weeks.13 Alternative surgical options for TOT reconstruction could be FAMM (facial artery muscolomucosal) flap, Zhao flap, RFFF, or primary suture.4,18–20 In the authors’ opinion, a fasciomucosal prelaminated RFFF offers a series of advantages for TOT reconstruction. It is a thin and pliable flap that preserves the physiology and lubrification of the oral mucosa. The absence of subcutaneous tissue makes the PFRFFF much thinner than fascio-cutaneous flaps.14 Compared with mucosal loco-regional flaps, prelaminated flaps allow the preservation of oral mucosa lining while providing adequate bulk and reduced scar formation for optimal functional recovery.13 Because only a thin oral mucosal sheet is harvested, while keeping a 1-cm safety distance from Stensen duct, donor site morbidity is minimal and no further intervention is needed. Prelamination resolves the necessity for skin grafting in the forearm, one of RFFF’s major disadvantages.12
In our case report, the fasciomucosal flap allowed an adequate reconstruction of TOT volume with good functional and aesthetic outcomes. Because the resection involved TOT exclusively, taste perception from the remaining tongue and oral cavity was unaltered and the patient did not complain any dysgeusia. The flap’s added bulk and its minimal scar retraction granted free tongue movement and optimal speech intelligibility. In choosing the PFRFFF, as with all prelaminated free flaps, long-term volume reduction of up to 50% should be considered while preparing the flap.13,15
The major drawback of PFRFFF is the necessity for a 3-week wait interval between the morselization of buccal mucosa grafts and reconstruction. Nonetheless, this time period can be utilized for preoperative radiotherapy or chemotherapy.16,17
CONCLUSIONS
In the authors’ opinion, fasciomucosal PFRFFF is a valid TOT reconstructive option especially in selected cases where speech intelligibility and articulation are of the uttermost importance. To our knowledge, no cases of tip of the tongue reconstruction with prelaminated flaps have been reported.
Footnotes
Published online 2 December 2020.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
REFERENCES
- 1.Süslü N, Hoşal AŞ, Aslan T, et al. Carcinoma of the oral tongue: a case series analysis of prognostic factors and surgical outcomes. J Oral Maxillofac Surg. 2013;71:1283–1290. [DOI] [PubMed] [Google Scholar]
- 2.Riemann M, Knipfer C, Rohde M, et al. Oral squamous cell carcinoma of the tongue: prospective and objective speech evaluation of patients undergoing surgical therapy. Head Neck. 2016;38:993–1001. [DOI] [PubMed] [Google Scholar]
- 3.Yamamoto H, Kawai M, Murakami KI. Pedunculated squamous cell carcinoma on the tip of the tongue. Oral Heal Case Rep. 2017;03:3–5. [Google Scholar]
- 4.Bokhari WA, Wang SJ. Tongue reconstruction: recent advances. Curr Opin Otolaryngol Head Neck Surg. 2007;15:202–207. [DOI] [PubMed] [Google Scholar]
- 5.Ji YB, Cho YH, Song CM, et al. Long-term functional outcomes after resection of tongue cancer: determining the optimal reconstruction method. Eur Arch Otorhinolaryngol. 2017;274:3751–3756. [DOI] [PubMed] [Google Scholar]
- 6.Matsui Y, Ohno K, Yamashita Y, et al. Factors influencing postoperative speech function of tongue cancer patients following reconstruction with fasciocutaneous/myocutaneous flaps-a multicenter study. Int J Oral Maxillofac Surg. 2007;36:601–609. [DOI] [PubMed] [Google Scholar]
- 7.Lam L, Samman N. Speech and swallowing following tongue cancer surgery and free flap reconstruction–a systematic review. Oral Oncol. 2013;49:507–524. [DOI] [PubMed] [Google Scholar]
- 8.Cai YC, Li C, Zeng DF, et al. Comparative analysis of radial forearm free flap and anterolateral thigh flap in tongue reconstruction after radical resection of tongue cancer. ORL J Otorhinolaryngol Relat Spec. 2019;81:252–264. [DOI] [PubMed] [Google Scholar]
- 9.Sun J, Weng Y, Li J, et al. Analysis of determinants on speech function after glossectomy. J Oral Maxillofac Surg. 2007;65:1944–1950. [DOI] [PubMed] [Google Scholar]
- 10.Wang J, Green JR, Samal A. Individual articulator’s contribution to phoneme production. Proc. IEEE Intl. Conf. on Acoustics, Speech, Signal Processing. 2013Vancouver, Canada; [Google Scholar]
- 11.Archontaki M, Athanasiou A, Stavrianos SD, et al. Functional results of speech and swallowing after oral microvascular free flap reconstruction. Eur Arch Otorhinolaryngol. 2010;267:1771–1777. [DOI] [PubMed] [Google Scholar]
- 12.Oh J, Lee TH, Lee JH, et al. Exclusive tongue tip reconstruction of hemiglossectomy defects using the underrated lateral arm free flap with bilobed design. Arch Craniofac Surg. 2019;20:37–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chiarini L, De Santis G, Bedogni A, et al. Lining the mouth floor with prelaminated fascio-mucosal free flaps: clinical experience. Microsurgery. 2002;22:177–186. [DOI] [PubMed] [Google Scholar]
- 14.Kim GG, Halvorson EG, Hang AX, et al. Prelamination of radial forearm free flap with buccal mucosa. Otolaryngol Head Neck Surg. 2013;148:341–343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Poeschl PW, Kermer C, Wagner A, et al. The radial free forearm flap - prelaminated versus non-prelaminated: a comparison of two methods. Int J Oral Maxillofac Surg. 2003;32:159–166. [DOI] [PubMed] [Google Scholar]
- 16.Rath T, Millesi W, Millesi-Schobel G, et al. Mucosal prelaminated flaps for physiological reconstruction of intraoral defects after tumour resection. Br J Plast Surg. 1997;50:303–307. [DOI] [PubMed] [Google Scholar]
- 17.Rath T, Millesi W, Lang S, et al. Mucosal prelamination of a radial forearm flap for intraoral reconstruction. Eur J Plast Surg. 1998;21:166–170. [DOI] [PubMed] [Google Scholar]
- 18.Zhao Z, Zhang Z, Li Y, et al. The buccinator musculomucosal island flap for partial tongue reconstruction. J Am Coll Surg. 2003;196:753–760. [DOI] [PubMed] [Google Scholar]
- 19.Moro A, Saponaro G, Doneddu P, et al. The arterialized facial artery musculo-mucosal island flap for post-oncological tongue reconstruction. J Craniofac Surg. 2018;29:2021–2025. [DOI] [PubMed] [Google Scholar]
- 20.Shivanand NB, Mohan MT, Joseph ST. Contralateral islanded facial artery myomucosal flap for the reconstruction of floor of the mouth defect. Craniomaxillofac Trauma Reconstr. 2018;11:157–160. [DOI] [PMC free article] [PubMed] [Google Scholar]