

Abstract
Introduction
Hand amputation significantly challenges one's independence in carrying out daily activities. With the UK and Italy recoding circa 5200 and 3500 upper limb (UL) amputations (ULAs) yearly, respectively, and about 541,000 Americans losing ULs in 2005, incidence victims constitute a considerable proportion of our population and should be adequately supported. The use of upper limb prosthesis (ULP) offers amputees a new opportunity of living a quality life - but poses challenges on the physically and psychologically traumatised. With reports that up to 20% of adult UL amputees choose not to use a prosthesis, roughly 26% of adults and 45% of children and adolescents are dissatisfied with their devices and abandon them with reasons of poor solution to basic needs, a review of ULP for suitability has become crucial.
Objectives
These include, to review UL prosthetic technology (PT), the materials used in the manufacturing of ULP, challenges in research and development of ULP, and to advise on the suitability of different devices to the needs of amputees.
Methods
They involve an extensive review of relevant literature and application of statistics to analyse data obtained from literature.
Results
ULAs are characterised to show affected bones in seven types of amputations. The characterisation depicts key causes of incidences that lead to amputations while advising on device suitability. PT is classified in terms of cost, nature, functions/operations of each type of device while providing the design challenges. Users’ opinions on PT materials are analysed and used to suggest new materials for the next generation of the devices. R&D challenges hindering future developments of PT is reviewed and results used to identify characteristics for the next generation of the technology.
Conclusions
To increase user satisfaction and reduce device abandonment, amputees need useful information on the trend in PT and engineers need information about device field performance for improvements. The use of better performing ULP will improve users’ everyday lives.
Keywords: Upper limb prosthesis, Users, Amputees, Biomechanical energy harvesting, Technology, Upper limb bones
1. Introduction
A prosthesis is a useful, artificial medical device that replaces a missing body part. It offers amputees a fresh opportunity of being able to perform the function which would have been performed by the missing body part. Amputees therefore find prostheses integral to restoring the activities of their challenged life to normalcy and achieving quality life. To deliver this expectation, the prostheses therefore should be fit for purpose in supporting the amputees Fig. 11.
Fig. 11.

Anterior view of transhumeral socket (lake, 2008).69
Upper limb prosthesis (ULP) is the special device which supports amputees with lost hand(s). For the device to be successful, its design must meet the expectation and the operations address the needs of the users. There are several cases of device disuse and abandonment resulting from issues around functionality, reliability, appearance, comfortability, and usability. Some prosthetic devices have poor motor control while others are not durable enough. In many scenarios, the users of the devices are not quite happy with the appearance and some types of devices do not have sensory touch function in addition to being inordinately heavy. Other desirable qualities found wanting in current prosthetic devices include lack of warmth and humanness.
To achieve an effective design of prosthesis, the design engineers and medical experts involve in its development ought to design for the issues states earlier. A better understanding of upper limb anatomy and possible sections of hand amputation and general effect of prosthetics on users will be helpful in realising the objective.
The skeletal anatomy of the upper extremity is shown in Fig. 1. It consists of eight principal types of bone: clavicle, scapula, humerus, ulna, radius, carpals, metacarpals and phalanges. The key regions can be classified into six: shoulder girdle, arm, elbow, forearm, carpus and hand.1 The shoulder contains the clavicle and scapula and articulates with the proximal humerus. Based on the interconnection and function of the bones, seven possible sections of amputation can be made. The sections are shown in Fig. 2 and are known as transcarpal, wrist disarticulation, transradial, elbow disarticulation, transhumeral, shoulder disarticulation and forequater.2 The plethora of devices utilised at these extents of the amputation is called upper extremity prostheses and are thus classified as such. However, there are simple classification of: prosthetic wrist, prosthetic elbow, prosthetic shoulder, prosthetic arm and terminal device. Currently, there are primarily passive and active prostheses for support to upper extremity amputees. Active prostheses can be further classified into myoelectric and body-powered.3 Both variations possess advantages and disadvantages.
Fig. 1.
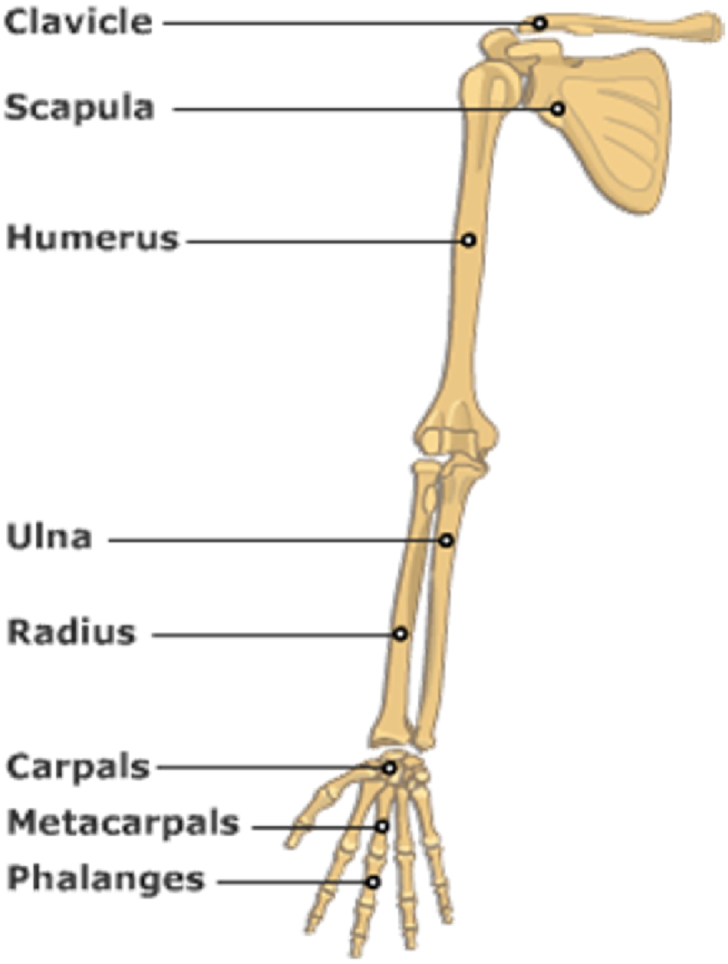
Upper limb bones. 2000 graphic71
Fig. 2.
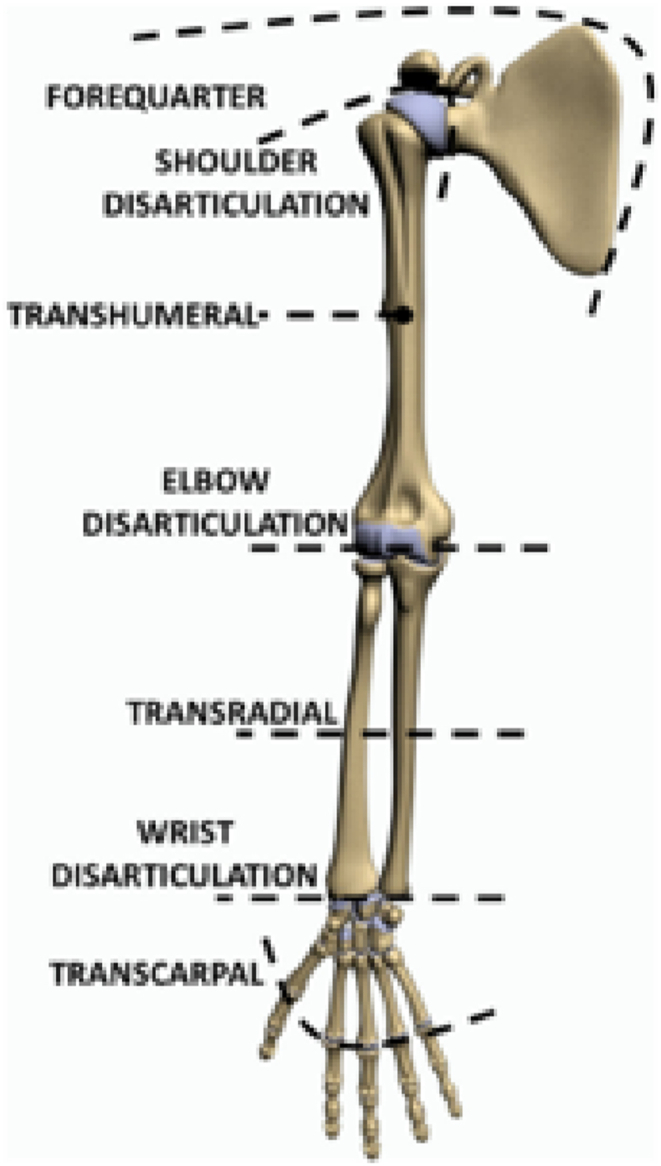
Classification of Upper Limb Amputation (Cordella et al., 2016).2
The current market, the forecast and prevalent of ULPs across continents determine their future. The report4 that ULP market size was valued at USD 1077.8 million in 2018 and is expected to witness more than 11% CAGR from 2019 to 2025 justifies the need to invest more resources in the technology to improve the quality and performance of the product.
Fig. 3 shows the industry share of the market to be $1 B N in 2018 and is expected to be $2.3 B N by 2025. The regional landscape of the market predicts India's industry CAGR from 2019 to 2025 to be 15.4% while U.S. is valued at about $544.1 MN. Fig. 4 presents the statistics of market share distribution of ULP components in Germany. Prosthetic wrist dominates the share while prosthetic shoulder is the least prevalent. In the United Kingdom, approximately 5200 upper limb amputations (ULAs) are performed annually. Most of the upper limb absence are classified as transcarpal at 61%. Transhumeral and forequarter amputations account for 16% and 2% of upper limb loss in the UK, respectively.2 The statistics are represented in Fig. 5. In the United States, it is estimated that there are 2.2 million amputees, with approximately a quarter suffering from a degree of upper limb loss.5 Fig. 6 presents a chart of projected upper limb prosthesis market share in key countries in Europe for 2025. Germany has the highest market share followed by France.
Fig. 3.

Industry share and regional landscape of upper limb prosthesis market.
Fig. 4.

Upper limb prosthetic market in Germany by component, 2018 (units) (Ankika et al., 2018).4
Fig. 5.

Severity in Upper Limb Amputation in the United Kingdom (Cordella et al., 2016).2
Fig. 6.

Upper limb prosthetic market in Europe 2025 (Units) (Ankika et al., 2018).4
The use of prostheses, combined with the emotional trauma commonly associated with the amputation, can have numerous negative effects on the user. Research on human perception alteration using an upper extremity prosthesis is sparse.6 Abandonment levels of ULPs are high.6,7 An independent survey was conducted where 20% of the participants involved had some extent of abandonment with their prosthesis.7 Published literature indicates that the actual abandonment value is much higher, dependant on the severity of the amputation among other contributing factors. It is reported that 60% of users with a shoulder disarticulation abandon their device – reasons include inadequate training and high cost of repairs.8
Numerous works have been published detailing the history and progression of upper limb prosthetic devices. A review on the advancements of prostheses was published by Das, Nagpal and Bankura,9 focusing on the technological improvements seen. Cordella et al.,2 Trent et al.,10 and Gaine, Smart and Bransby-Zachary11 all conducted reviews of upper limb prosthetics. This review article differs from the aforementioned documents as it aims to discuss the R&D challenges that face the industry and identify possible areas of development for upper limb devices.
It can be understood that the human hand is one of the more complicated anatomies with 19° of freedom and an opposing thumb which differentiates it from other primates.12 The entirety of the upper extremity is a decidedly complex limb with ‘neurovascular bundles, lymphatics, muscles and bones’ that coordinate to establish a functional limb, utilised for a multitude of activities and tasks.13 These complexities have accounted for the enormous difficulty faced in the design of improved ULPs - leading to the frustration faced by the users who are in demand of better performing device.
To provide the users hope in the form of trend on advancement in the technology in addition to furnish the technology developers information and data which will aid the design and manufacture of better performing ULP that will provide increased satisfaction to the users, this review is conducted. It is the objectives of the review to:
-
⁃
Evaluate the state of the technology and materials to identify shortcomings.
-
⁃
Highlight the opinions of the users on materials used to manufacture ULPs and suggest possible new materials.
-
⁃
Provide design considerations and recommend critical design areas for future research and development.
-
⁃
Discuss R&D challenges hindering future developments of the technology.
2. Technology of prosthesis
The existing technology can be classified into three main categories. These are the passive, active and hybrid prosthetic devices. They are discussed further for an insight into their capabilities and shortcomings.
2.1. Passive prostheses
The passive prosthetic devices (PPD) are employed when physical appearance and comfort are of the utmost priority.14 Fig. 7 presents an exploded diagram of a passive arm prosthetic device with the key components. The lifelike appearance is apparent.
Fig. 7.

Exploded diagram of a passive arm prosthetic device. Showing its components of a (Passive arm prostheses, 2019).70
Passive devices remain a popular choice for users despite their functional limitations. They are relatively inexpensive and have an aesthetically pleasing cosmetic appearance. The functionality of PPD is limited to primitive actions such as pushing, pulling and carrying objects.15 However, they are commonly worn in social situations as they increase the confidence of the user. Approximately one in three amputees use a passive prosthesis in some capacity.14 The device is usually recommended for patients who have recently undergone amputation. On familiarisation with it, users typically advance onto using active prostheses.
2.2. Active prostheses
The primary distinction between active and passive prosthetic devices is that active devices can generate power.16 Active prostheses can be further classified into body powered and myoelectric devices. Each presents advantages and disadvantages. Owing to complementary nature of passive and active devices in meeting the needs of amputees, a combination of passive and active prosthetic devices is advised. In shoulder disarticulation amputations, patients are routinely fitted with a passive shoulder joint and an active myoelectric elbow wrist and hand.17 The body powered and myoelectric devices are discussed thus:
2.2.1. Body powered devices (BPD)
Body powered upper extremity prostheses are controlled using a harness which is connected via a cable to elsewhere on the patient's body, such as the healthy shoulder.18 The working shoulder is manoeuvred in distinct movements to control the prosthesis.19 A standard body powered upper extremity prosthesis features a socket, wrist, control cable, harness and a terminal device.20 An illustration of BPD is shown in Fig. 8. A major advantage of this is that the hooks are highly practical for a wide variety of activities. They are suitable for extensive, heavy-duty activities when compared to myoelectric prostheses because they are less susceptible to damage in volatile conditions such as corrosive and wet environments. This is due to their exclusion of batteries or an alternative power source.21 In addition to this, body powered devices offer ‘intuitive control of the prosthetic device as well as force feedback via the cable tensioning’.22 Another advantageous aspect is that the cost to the user is relatively low in comparison to myoelectric devices.2 In the USA, a body powered upper extremity prosthesis can cost approximately $10,000, whereas myoelectric devices range from $20,000 to $100,000.23
Fig. 8.

A typical body powered upper limb prosthesis (Hussain, Shams and Jawaid Khan, 2019)20
Despite these positive aspects, body powered devices present several issues. The activation forces required are often large and can be physically overwhelming for some users, leading to issues such as fatigue and discomfort.24 If a hand is utilised as the terminal device, the prosthesis is generally mechanically inefficient, as they are relatively heavy, and most hands do not provide enough pinch force to complete mundane tasks.21 Many users prefer the terminal device to be a hook when using a body powered prosthesis due to their improved functionality and ease of use.25 Despite this, hooks do not provide the user with an authentic appearance and therefore are not satisfactory for a large percentage of users.21
Body powered prostheses remain a popular option among users due to their low cost and substantial functionality.
The response of users in an independent survey conducted in 1986 is presented in Fig. 9. It is found that 68% of users opted for the body powered hook, 20% indicated use of the cable operated hand and 12% are indifferent.26 In a study conducted in 2012, it was found that the use of BPD has reduced over time - 30% of those interviewed used a body powered device, with myoelectric being the most prevalent prosthesis among adult amputees27 Fig. 10.
Fig. 9.

Variance in the Usage of Body Powered Prostheses in an independent survey (Millstein, Heger and Hunter, 1986)26
Fig. 10.

Diagram of myoelectric prosthetic arm (Paul, 2015).68
2.2.2. Myoelectric devices
Myoelectric upper extremity prostheses are powered through the use of electric motors with an external power source. The movement of the joint is controlled through muscle activity from the remaining limb. ‘Electromyographic (EMG) signals from the limb stump are detected by surface electrodes, amplified and then processed by a controller to drive battery-powered motors that move the hand, wrist or elbow’.28
A myoelectric upper extremity prosthesis aims to ameliorate the cosmesis of the device, a deciding factor for many users on which device they wish to use.3 Losing a limb is a severely traumatic event for a patient and consequently, the individuals social-psychological requirements are of top priority. Devices that do not restore a lifelike appearance for the user are commonly rejected.29 As a result of this, myoelectric prostheses are the standard for Western countries, with around 90% of patients using it as their primary device.30 Another benefit of myoelectric devices is that they operate in a physiologically natural manner. When a transradial prosthesis is employed, the muscles which are used to open and close the myoelectric hand are identical to the muscles used in the natural hand.21 Moreover, the grip strength of the myoelectric device is typically several times larger than that of a body-powered prosthesis. This is achieved with practically no additional force required as only minute muscle contractions are necessitated to achieve the maximum grip force.21
Despite the functional and cosmetic advancements when compared to passive and body powered prostheses, the cost of myoelectric devices is a barrier that limits users access. This is especially prevalent in countries without a robust healthcare system. In countries such as the USA, an advanced myoelectric upper prosthesis with a functional terminal device can cost around $75,000.31 This restricts users with a lower income from accessing the optimal level of healthcare – numerous technologies are being investigated to assess whether the cost of myoelectric prostheses could be lowered. Another negative aspect of myoelectric devices is that their battery needs to be recharged daily. The battery can become damaged from environmental factors such as water and dirt; maintenance and repair costs for the devices are generally higher than alternatives.21
2.3. Hybrid devices
The aforementioned devices are the primary options available to amputees. However, a less commonly used prosthetic device is a hybrid device. A hybrid upper extremity prosthetic device combines body powered and myoelectric components to construct a functional device which incorporates the benefits from the individual devices. At the transradial level, hybrid designs are typically not utilised as there are limited devices available with suitable technology.21 However, for over 25 years, Europe has achieved significant success with a transhumeral prosthesis, utilising a ‘cable-operated, body-powered elbow with myoelectric control from the biceps (closing) and triceps (opening)’.32 Some hybrid controls offer simultaneous sequential control of the prosthetic elbow and hand, but harnessing can be inconvenient and strenuous, most notably at the short transhumeral level as the user may not possess adequate force to operate the elbow.21
2.4. Characterisation of upper limb amputation and technology
Having introduced and discussed the technology, an attempt is made to characterise it. The characterisation is presented in Table 1, Table 2. Table 1 presents characterisation of upper limb amputation and prosthetic technology while Table 2 depicts characterisation of the technology and recommendation. Table 1 shows affected bones in seven types of amputations. The key causes of the amputation as well as the suitable technology are outlined. Understanding the causes would provide knowledge to set up prevent measures and control. These would inadvertently reduce incidences. Table 2 classified the technology in terms of body powered, myoelectric, cable operated and not available (N/A). It also presents the key functions and operations of each type. The cost range, estimated production in the UK as well as recommendation based on the income class of the amputee are stated. The knowledge of the key functions/operations of the devices and the cost range could assist new amputees in making an initial decision of technology to choose. The decision ought to be made in conjunction with the advice of a qualified medical personnel. The estimated production in the UK may guide the business stakeholders on viability of each device.
Table 1.
Characterisation of upper limb amputation and prosthetic technology.
| S/No | Amputation classification | Affected bones | Amputation Causes | Suitable Technology |
|---|---|---|---|---|
| 1 | Transcarpal | Phalanges and Metacarpals | Accidental trauma - power tools, trapped in door 33 | Prosthetic wrist |
| 2 | Wrist disarticulation | Carpals, Radius and Ulna | Severe peripheral vascular disease, electric and thermal injury, frostbite, sepsis 34 | Prosthetic wrist |
| 3 | Transradial | Radius and Ulna | Trauma to the hand and arm most common. Tumour and birth defects also 35 | Terminal devices |
| 4 | Elbow disarticulation | Radius, Ulna and Humerus | Trauma, cancer, bone infection 36 | Prosthetic elbow |
| 5 | Transhumeral | Humerus | Trauma, tumour control 37 | Terminal devices |
| 6 | Shoulder disarticulation | Humerus, Clavicle and Scapula | Not common, traumatic injury to entire arm, congenital abnormality, tumour 38 | Prosthetic shoulder |
| 7 | Forequarter | Clavicle and Scapula | Malignant tumours, severe trauma 13 | Prosthetic Arm |
Table 2.
Upper limb prosthetic technology characterisation and recommendation.
| S/No | Technology | Type/Classification | Key functions/operations | Cost range | Estimated Prosthetic Production in the UK* | Recommendation |
|---|---|---|---|---|---|---|
| 1a | Passive Prosthetic Wrist | N/A | Enable reorientation of terminal device relative to the forearm manually 39 | Exact Data not Available | 28 | N/A |
| 1b | Active Prosthetic Wrist | Body Powered & Myoelectric | Enable reorientation of terminal device relative to the forearm, through cables or motors 39 | ~$18,000 40 | Middle income class | |
| 2a | Passive Prosthetic Elbow | N/A | To provide cosmetic improvement - fairly non-functional 41 | Exact Data not Available | 14 | N/A |
| 2b | Active Prosthetic Elbow | Body Powered & Myoelectric | To flex and straighten the arm through a harness or motor 41 | $60,000+ 40 | High Income class | |
| 3a | Passive Prosthetic Shoulder | N/A | To provide cosmetic improvement | Exact Data not Available | 70 | N/A |
| 3b | Active Prosthetic Shoulder | Body Powered & Myoelectric | Used to provide pain relief and restore mobility to the shoulder joint 42 | $61,000+ 40 | High income class | |
| 4a | Passive Prosthetic Arm | N/A | Cosmetic improvement, can be used for carrying and stabilization 43 | $10,000 40 | 350 | Low income class |
| 4b | Active Prosthetic Arm | Body Powered & Myoelectric | Enables opening, closing, rotation with varying strengths and speeds 43 | $60,000 - $100,000 40 | High Income class | |
| 5a | Passive Terminal Devices | N/A | Allows for pushing, pulling and carrying; used for cosmetic purposes mainly 14 | Exact Data not Available | 854 | N/A |
| 5b | Active Terminal Devices | Cable Operated & Myoelectric | Allows for opening and closing of the hand and rotation of the wrist 44 | £25,000 - £60,000 per hand 12 | Middle income class |
3. Materials
The materials that have been utilised to construct upper extremity prosthetic limbs have evolved throughout time. Initially, wood was used to replace a lost limb; however, as technology has advanced, the materials used in prosthetic limbs has improved significantly.45
3.1. Biocompatibility
Shackelford46 stated that biomaterials are ‘engineered materials created for applications in biology and medicine.’ Depending on the part, materials used in prosthetics need to be biocompatible to ensure that they do not cause any harm to living tissue. A wide range of mechanical, physical and material properties are also considered when selecting which materials would be suitable for prosthetic use, including wear resistance, yield strength and ductility.47
3.2. Metals
The most commonly used metals in the skeletal design of upper extremity prostheses are titanium and aluminium. Other metals utilised in some scope include copper, iron, magnesium and steel. Titanium is widely employed due to its favourable properties that make it suitable for biomedical purposes, such as excellent resistance to corrosion, light weight and a good strength to weight ratio.28 In addition to this, it is also alloyed with certain other metals such as aluminium and vanadium to improve mechanical properties. Moreover, the low modulus of elasticity of titanium means that it is similar to human bone. The benefit of this is that the skeletal load of the user will be distributed more uniformly between the implant and the bone. This results in an improved gait for the user.28 However, despite the advantageous aspects of titanium as a biomaterial, it is costly and can limit access in countries without a comprehensive healthcare system.48
3.3. Polymers
The socket is the connecting part of the prosthesis and is precisely moulded around a cast of the residual limb so that it accurately fits the user. It is crucial that sockets are custom-made and fitted by an experienced prosthetist.49
The structure of the socket is typically composed of thermoplastics, such as a polyester resin or an acrylic resin.48 Other polymers that are utilised are nylon and acrylics – they are both commonly used for prosthetic socks which cover the prosthesis. In addition to this, polyurethane foam is extensively used in ‘both soft, cosmetic foam covers and rigid structural sections’.50
3.4. Silicone
Silicone has been regarded as ‘the most significant advancement in materials for prosthetic interfaces’.51 Room temperature vulcanized silicone is cushioned and comfortable to touch. High temperature vulcanized silicone has advantageous strength properties and is highly durable. Silicone is ideal for use in prosthetics as it is biocompatible; it is commonly used in sockets or liners. The material is dynamic, meaning it moves with the body and provides an enhanced grip for the user. Moreover, it has been found to encourage the growth of new skin when it is contact with the residual limb.51 Silicone is also utilised for the casting process as it retains a high accuracy for the shape and size of the prosthesis.52
3.5. Other materials
Carbon fiber is frequently used in the pylon design due to its high strength and light weight; it also possesses high chemical and temperature resistance, high stiffness and low thermal expansion. The specific modulus of carbon fiber is approximately three times higher than that of magnesium and titanium.28 However, the cost can be high when compared to materials with similar mechanical properties.
The pylon is typically covered with flesh coloured foam or plastic.49 Comfort is the primary motivation for the use of foam.
4. R&D challenges
Upper extremity prosthetic devices are rapidly advancing with major improvements having been made in recent years.53 Despite this, there are a wide variety of research and development challenges that bioengineers encounter.
4.1. Sensory inputs
The sense of touch is a crucial ability in order to dextrously control objects – it relies on sensory signals that stem from the hand.54 Sensory inputs are necessary in order to generate precise movements that incorporate force sensing. However, currently a system has not been fully developed that allows a patient to experience the sensation of touch with their prosthetic limb.55 This remains a challenging development issue in the field of robotics. Nonetheless, recently research has advanced in this area. After a development period of 15 years, the LUKE arm has been created by researchers at the University of Utah. The test subject can distinguish 119 varying touch sensations, differentiating between soft and hard objects. The state-of-the-art technology operates through microelectrodes which are embedded in the patients forearm and then connected to a computer. This conveys touch signals from the prosthetic arm, to the computer then to the brain.56 Despite this, the advanced technology only operates functionally when connected to an external computer. The major challenge that the researchers must address is a portable version to provide maximum practicality. The engineers behind this estimate that testing may be available as early as 2021.56
4.2. Other R&D challenges
There are numerous other research and development challenges. The vast majority of the actuators that are currently used are cumbersome and heavy for the patient; the devices which are lighter in weight generally do not provide enough power for the amputee to maintain a high level of functionality.55 As a result of this, research needs to be conducted into developing a much more lightweight option for the patient to provide maximum comfort whilst retaining high levels of performance. Furthermore, common issues that are reported by patients using upper extremity prosthetic devices are that an incorrectly fitted socket can result in pressure on the residual limb. As the socket is precisely designed to apportion forces over as great a surface area as possible to reduce pain, an awkwardly fitting socket can give rise to issues such as consistent pain and dermatologic complications, including contact dermatitis and excessive sweating.57 As a result, further development needs to be centralised around these issues so that adherence and patient satisfaction are maintained to a high level.
5. Future development
It is recognised that having to design and engineer a device that will have to replace a missing limb is one of the most difficult aspects in engineering. This is due to the complex nature of the natural processes that the devices have to mimic.58 To further improve the current technology available, there are numerous innovations at the forefront of engineering, designed to enhance the functionality for the user.
5.1. 3D printing
Over the past decade, 3D printing has seen substantial advancements in the technology available. Initially utilised to overcome the high cost of upper extremity prostheses, the first widely available 3D printed device was the Robohand. Developed in 2011, it costs approximately £1600 for a fully assembled device; alternatively, users with access to a 3D printer can print the parts individually and assemble it themselves.59 Whilst possessing advantageous aspects such as dramatically reduced cost and its relative light weight, it is only suitable for patients who have a functioning wrist. Moreover, the fingers of the device cannot be opened and closed independently from one another, limiting the practicality of the prosthesis.59
The technology is still constantly evolving but is not yet utilised by professional bodies around the world. Despite this, the majority of devices that are manufactured in this method are for children. The growth of children means that new devices need to be created so that it will securely fit the patient. A major benefit of 3D printing for upper extremity prostheses is that the parts can be conveniently personalised to suit the patient's aesthetic and functional requirements.60 Moreover, the aforementioned production costs are greatly reduced, a major benefit for patients who struggle to access conventional options. However, the functionality of these devices is currently lacking. Consequently, further development into this sector is required.
5.2. Movement based control
Despite being the most widely used method of power available in upper extremity prosthetic devices, myoelectric control presents numerous limitations such as difficulty when managing simultaneous movements and few degrees of freedom.61 As a result of this, there is a revived interested in movement-based control. This method utilises residual limb movements, compared to muscular activity as the command input.62 Numerous independent studies have been conducted to verify the practicality of this system. One study was based around a simplistic electric device which relied on an inertial measurement unit – it translated predesignated movements into control signals which produced a noticeably more intuitive and natural experience for the user.63 The research on this topic is fairly limited, therefore further experimentation is required to understand whether this would be a viable alternative to myoelectric control.
5.3. Biomechanical energy harvesting
Myoelectric prosthetic devices require a battery to operate. This typically needs to be recharged daily and is a major drawback as it reduces the practicality and ease of use of the device.64 A theoretical concept that aims to offset this disadvantage is the harvesting of biomechanical energy from human motion. The mechanical efficiency of the human body is approximated to be 15–30%; this indicates that the majority of energy digested as food is discharged into the atmosphere in the form of heat.65 This could theoretically be converted into electrical energy to power a device. A variety of methods have been proposed. A piezoelectric material was initially suggested but due to unsatisfactory results, this idea was abandoned.66
Numerous studies have been conducted to determine if a device could effectively power a prosthetic limb. The majority of power generation devices utilise walking as the method of generation. A 2009 study by Li, Naing and Donelan67 suggested that fairly substantial amounts of power could be produced through a lightweight device harvesting energy from the motion of walking.67 However, most of the devices focus on lower limb prostheses. As a result of this, further research is needed to fully understand whether biomechanical energy could be harvested for an upper limb prosthetic device.
6. Conclusions
This review presents the state-of-the-art in technologies and materials of the upper limb prosthetics (ULP) for user suitability and needs analyses. The review is critical because availability and use of better performing and thus suitable ULP will not only lower the rate of abandonment of the device but will lead to improvement in the quality of lives of the users.
The suitability of passive and active prostheses depends on the immediate need of the user. The passive prostheses seem suitable for users who are not bothered about supply of power to the device but whose interest is on appearance and comfort when wearing the device. Users who want power in the device is better off with active prostheses. Depending on their preferences in powering the device, body powered, or myoelectric devices suffice. Users who are comfortable to supply the power from elsewhere on their body with less concern on discomfort arising from the use of the device may adopt body powered devices. Amputees who have substantial economic power will find myoelectric prosthetic suitable as they will recreate the operation of the amputated limb in a physiological natural manner.
A system which fully gives the users of ULP the complete feeling of touch of objects has to be developed from the promising LUKE arm ULP that currently distinguishes 119 differing touch sensations. More and urgent research are needed in 3D printing of ULP to increase recognition and adoption by professional bodies as it is poised to be the cost-effective production method for ULP. Significant improvement on the emerging biomechanical energy harvesting technology would deliver ULP which functions without the need for a chargeable external power source. Thus, research focused on new sources of power to the ULP is indispensable.
Silicone is currently the most significant advancement in materials for prosthetic interfaces owing to its dynamic properties that allow it to move with the body. In addition, its biocompatibility characteristics is found to promote growth of new skin when in contact with the residual limb. Notwithstanding these favourable properties, metals remain the most utilised material in the pylon design of ULP devices. Aluminium and titanium are widely used because of their resistance to corrosion and satisfactory strength to weight ratio. Titanium also possesses low modulus of elasticity that makes it comparable to bone. Carbon fiber, foam and various polymers are also utilised in ULP manufacture.
Addressing the findings of the research will reduce the disparity between amputees and able-bodied people - satisfying the overall aim of prosthetic devices development and manufacture.
Declaration of competing interest
None.
Acknowledgements
We acknowledge the authors who's works are cited.
References
- 1.Doyle J., Botte M. Lippincott Williams & Wilkins; Philadelphia: 2002. Surgical Anatomy of the Hand and Upper Extremity; p. 3. [Google Scholar]
- 2.Cordella F., Ciancio A., Sacchetti R. Literature review on needs of upper limb prosthesis users. Front Neurosci. 2016;10:1–2. doi: 10.3389/fnins.2016.00209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Carey S., Lura D., Highsmith M. Differences in myoelectric and body-powered upper-limb prostheses: systematic literature review. J Rehabil Res Dev. 2015;52(3):247–262. doi: 10.1682/JRRD.2014.08.0192. [DOI] [PubMed] [Google Scholar]
- 4.Bhutani A., Swain R. 2018. Upper Limb Prosthetics Market Forecasts 2019-2025 Global Statistics.https://www.gminsights.com/industry-analysis/upper-limb-prosthetics-market [online] Global Market Insights, Inc. Available at: [Google Scholar]
- 5.Wheaton L. Neurorehabilitation in upper limb amputation: understanding how neurophysiological changes can affect functional rehabilitation. J NeuroEng Rehabil. 2017;14(1) doi: 10.1186/s12984-017-0256-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Buckingham G., Parr J., Wood G., Vine S., Dimitriou P., Day S. The impact of using an upper-limb prosthesis on the perception of real and illusory weight differences. Psychonomic Bull Rev. 2018;25(4):1507–1516. doi: 10.3758/s13423-017-1425-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Biddiss E., Chau T. Upper-limb prosthetics. Am J Phys Med Rehabil. 2007;86(12):977–987. doi: 10.1097/PHM.0b013e3181587f6c. [DOI] [PubMed] [Google Scholar]
- 8.Resnik L., Meucci M., Lieberman-Klinger S. Advanced upper limb prosthetic devices: implications for upper limb prosthetic rehabilitation. Arch Phys Med Rehabil. 2012;93(4):710–717. doi: 10.1016/j.apmr.2011.11.010. [DOI] [PubMed] [Google Scholar]
- 9.Das N., Nagpal N., Bankura S. A review on the advancements in the field of upper limb prosthesis. J Med Eng Technol. 2018;42(7):532–545. doi: 10.1080/03091902.2019.1576793. [DOI] [PubMed] [Google Scholar]
- 10.Trent L., Intintoli M., Prigge P. A narrative review: current upper limb prosthetic options and design. Disabil Rehabil Assist Technol. 2019;15(6):604–613. doi: 10.1080/17483107.2019.1594403. [DOI] [PubMed] [Google Scholar]
- 11.Gaine W., Smart C., Bransby-Zachary M. Upper limb traumatic amputees. J Hand Surg. 1997;22(1):73–76. doi: 10.1016/s0266-7681(97)80023-x. [DOI] [PubMed] [Google Scholar]
- 12.Hirt B., Seyhan H., Wagner M., Zumhasch R. 2016. Hand and Wrist Anatomy and Biomechanics; p. 2. [Google Scholar]
- 13.Maduri P., Akhondi H. StatPearls; 2019. Upper Limb Amputation. [PubMed] [Google Scholar]
- 14.Maat B., Smit G., Plettenburg D., Breedveld P. Passive prosthetic hands and tools: a literature review. Prosthet Orthot Int. 2017;42(1):66–74. doi: 10.1177/0309364617691622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ovadia S., Askari M. Upper extremity amputations and prosthetics. Semin Plast Surg. 2015;29(1) doi: 10.1055/s-0035-1544171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dabiri Y., Najarian S., Eslami M., Zahedi S., Farahpour H., Moradihaghighat R. ICBME); 2010. Comparison of Passive and Active Prosthetic Knee Joint Kinematics during Swing Phase of Gait. 2010 17th Iranian Conference Of Biomedical Engineering. [Google Scholar]
- 17.Salminger S., Roche A., Sturma A., Mayer J., Aszmann O. Hand transplantation versus hand prosthetics: pros and cons. Current Surgery Reports. 2016;4(2) doi: 10.1007/s40137-016-0128-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Huinink L., Bouwsema H., Plettenburg D., van der Sluis C., Bongers R. Learning to use a body-powered prosthesis: changes in functionality and kinematics. J NeuroEng Rehabil. 2016;13(1) doi: 10.1186/s12984-016-0197-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Clements I. 2008. How Prosthetic Limbs Work.https://science.howstuffworks.com/prosthetic-limb4.htm [online] HowStuffWorks. Available at: [Google Scholar]
- 20.Hussain S., Shams S., Jawaid Khan S. Biomechanical and Biomedical Engineering; 2019. Impact of Medical Advancement: Prostheses. Computer Architecture In Industrial. [Google Scholar]
- 21.Uellendahl J. Myoelectric versus body-powered upper-limb prostheses. Journal of Prosthetics and Orthotics. 2017;29:P25–P29. [Google Scholar]
- 22.Beckerle P., Willwacher S., Liarokapis M., Bowers M., Popovic M. 2019. Prosthetic Limbs; pp. 235–278. Biomechatronics. [Google Scholar]
- 23.Bioengineering Institute Center for Neuroprosthetics, n.d. Limb Prosthetics Services And Devices. Worcester Polytechnic Institution, p.10.
- 24.Smit G., Plettenburg D. Efficiency of voluntary closing hand and hook prostheses. Prosthet Orthot Int. 2010;34(4):411–427. doi: 10.3109/03093646.2010.486390. [DOI] [PubMed] [Google Scholar]
- 25.Kejlaa G. Consumer concerns and the functional value of prostheses to upper limb amputees. Prosthet Orthot Int. 1993;17(3):157–163. doi: 10.3109/03093649309164376. [DOI] [PubMed] [Google Scholar]
- 26.Millstein S., Heger H., Hunter G. Prosthetic use in adult upper limb amputees: a comparison of the body powered and electrically powered prostheses. Prosthet Orthot Int. 1986;10(1):27–34. doi: 10.3109/03093648609103076. [DOI] [PubMed] [Google Scholar]
- 27.Østlie K., Lesjø I., Franklin R., Garfelt B., Skjeldal O., Magnus P. Prosthesis use in adult acquired major upper-limb amputees: patterns of wear, prosthetic skills and the actual use of prostheses in activities of daily life. Disabil Rehabil Assist Technol. 2012;7(6):479–493. doi: 10.3109/17483107.2011.653296. [DOI] [PubMed] [Google Scholar]
- 28.Mota A. California State Polytechnic University; Pomona: 2017. Materials of Prosthetic Limbs.https://www.bluecrossnc.com/sites/default/files/document/attachment/services/public/pdfs/medicalpolicy/myoelectric_prosthetic_components_for_the_upper_limb_6.pdf 2010. Myoelectric Prosthetic Components for The Upper Limb. [ebook] North Carolina: BlueCross BlueShield of North Carolina, pp.1–2. Available at: [Google Scholar]
- 29.Billock J. Upper limb prosthetic terminal devices: hands versus hooks. The American Academy of Orthotists and Prosthetists. 1986;10(2):57–65. [Google Scholar]
- 30.Kannenberg A. Active upper-limb prostheses. Journal of Prosthetics and Orthotics. 2017;29:P57–P62. [Google Scholar]
- 31.Ku I., Lee G., Park C., Lee J., Jeong E. Clinical outcomes of a low-cost single-channel myoelectric-interface three-dimensional hand prosthesis. Archives of Plastic Surgery. 2019;46(4):303–310. doi: 10.5999/aps.2018.01375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Childress, D., n.d. Upper-limb prosthetics: control of limb prostheses. In: Atlas of Limb Prosthetics, second ed.
- 33.Ishn.com. 2017. https://www.ishn.com/articles/105783-how-to-avoid-the-most-common-finger-loss-accidents [online] Available at: [Google Scholar]
- 34.Edwards S. Wrist and forearm amputations: background, indications, contraindications. 2019. https://emedicine.medscape.com/article/1245535-overview#a11 [online] Emedicine.medscape.com. Available at:
- 35.Human Technology Prosthetics. Orthotics n.d. What is A transradial prosthesis? – human technology prosthetics and orthotics. https://humantechpando.com/what-is-a-transradial-prosthesis/ [online] Available at:
- 36.Physio.co.UK. n.d. Above elbow amputation - amputees - what we treat - physio.Co.UK. https://www.physio.co.uk/what-we-treat/amputees/above-elbow-amputation/ [online] Available at:
- 37.McAuliffe J. Elbow disarticulation and transhumeral amputation: surgical principles. In: Bowker J., Michael J., editors. Atlas of Limb Prosthetics: Surgical and Prosthetic Principles. second ed. Mosby; 1992. [Google Scholar]
- 38.Autoaccident.com Management of shoulder amputations. 2020. https://www.autoaccident.com/management-of-shoulder-amputations.html [online] Available at:
- 39.Bajaj N., Spiers A., Dollar A. 2015. State of the Art in Prosthetic Wrists: Commercial and Research Devices.https://ieeexplore.ieee.org/document/7281221 [online] Ieeexplore.ieee.org. Available at: [Google Scholar]
- 40.Vandersea J. 2020. The Complete Guide to Arm & Hand Amputations and Prosthetics.https://mcopro.com/blog/resources/arm-hand-prosthetics/ MCOP. [online] MCOP Prosthetics. Available at: [Google Scholar]
- 41.Scheck & Siress . 2020. Above Elbow Prosthesis | Scheck & Siress.https://www.scheckandsiress.com/patient-information/care-and-use-of-your-device/above-elbow-prosthesis/ [online] Available at: [Google Scholar]
- 42.Hopkinsmedicine.org Reverse total shoulder replacement | johns hopkins shoulder and elbow surgery. 2020. https://www.hopkinsmedicine.org/orthopaedic-surgery/specialty-areas/shoulder/treatments-procedures/reverse-prosthesis.html#why_called [online] Available at:
- 43.Nevils-Karakeci R., Nevils-Karakeci R., McFadden C., Nevils-Karakeci R., Lang F. 2020. The Basics of Prosthetic Limbs and How They Work.https://interestingengineering.com/the-basics-of-prosthetic-limbs-and-how-they-work [online] Interestingengineering.com. Available at: [Google Scholar]
- 44.Scheck & Siress Terminal devices | scheck & siress. 2020. https://www.scheckandsiress.com/patient-information/care-and-use-of-your-device/terminal-devices/ [online] Available at:
- 45.Bellis M. 2006. The History of Prosthetics.http://theinventors.org/library/inventors/blprosthetic.htm [online] Theinventors.org. Available at: [Google Scholar]
- 46.Shackelford J. fifth ed. Prentice-Hall; Upper Saddle River, N.J.: 2000. Introduction to Materials Science for Engineers; p. 766. [Google Scholar]
- 47.Dos Santos V., Brandalise R., Savaris M. Springer International Publishing; Cham: 2017. Engineering of Biomaterials; p. 11. [Google Scholar]
- 48.Raghunath A. 2015. Materials in Prosthetics. [Google Scholar]
- 49.Woodford C. 2019. Prosthetics: A Simple Introduction to Artificial Limbs.https://www.explainthatstuff.com/prosthetic-artificial-limbs.html [online] Explain that Stuff. Available at: [Google Scholar]
- 50.Quigley, M., n.d. Prosthetic management: overview, methods, and materials. In: Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles, second ed.
- 51.Miguelez J., Lang M., Dodson R., Cameron M., Hays C. The O&P Edge; 2016. BUILDING A BETTER ARM: DESIGN AND FABRICATION IN UPPER-LIMB PROSTHETICS. [Google Scholar]
- 52.Cabibihan J., Abubasha M., Thakor N. A method for 3-D printing patient-specific prosthetic arms with high accuracy shape and size. IEEE Access. 2018;6:25029–25039. [Google Scholar]
- 53.Clement R., Bugler K., Oliver C. Bionic prosthetic hands: a review of present technology and future aspirations. Surgeon. 2011;9(6):336–340. doi: 10.1016/j.surge.2011.06.001. [DOI] [PubMed] [Google Scholar]
- 54.Tabot G., Dammann J., Berg J. Restoring the sense of touch with a prosthetic hand through a brain interface. Proc Natl Acad Sci Unit States Am. 2013;110(45):18279–18284. doi: 10.1073/pnas.1221113110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Bandara S., Gopura R., Hemapala K., Kiguchi K. The Seventeenth International Symposium on Artificial Life and Robotics 2012. Japan; 2012. Upper extremity prosthetics: current status, challenges and future directions. [Google Scholar]
- 56.Kent C. Touch sensitive prosthetic gives amputees A Sense of touch. 2019. https://www.medicaldevice-network.com/news/prosthetic-arm-gives-wearers-a-sense-of-touch/ [online] Verdict Medical Devices. Available at:
- 57.Steeper L.P.C. 2020. https://www.thelondonprosthetics.com/prosthetic-solutions/patient-information/after-care/common-problems/ Common Problems. [online] Available at:
- 58.Nathan S. 2018. Future Prosthetic: Towards the Bionic Human.https://www.theengineer.co.uk/future-prosthetic/ [online] The Engineer. Available at: [Google Scholar]
- 59.Gretsch K., Lather H., Peddada K., Deeken C., Wall L., Goldfarb C. Development of novel 3D-printed robotic prosthetic for transradial amputees. Prosthet Orthot Int. 2015;40(3):400–403. doi: 10.1177/0309364615579317. [DOI] [PubMed] [Google Scholar]
- 60.Kate J., Smit G., Breedveld P. 3D-printed upper limb prostheses: a review. Disabil Rehabil Assist Technol. 2017;12(3):300–314. doi: 10.1080/17483107.2016.1253117. [DOI] [PubMed] [Google Scholar]
- 61.Ning J., Dario F. Myoelectric control of upper limb prosthesis: current status, challenges and recent advances. Front Neuroeng. 2014;7 [Google Scholar]
- 62.Legrand M., Merad M., de Montalivet E., Roby-Brami A., Jarrassé N. Movement-based control for upper-limb prosthetics: is the regression technique the key to a robust and accurate control? Front Neurorob. 2018;12 doi: 10.3389/fnbot.2018.00041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Jarrasse N., Müller D., De Montalivet E. A simple movement-based control approach to ease the control of a myoelectric elbow prosthetics in transhumeral amputees. Annals of Physical and Rehabilitation Medicine. 2018;61 [Google Scholar]
- 64.Atzori M., Müller H. Control capabilities of myoelectric robotic prostheses by hand amputees: a scientific research and market overview. Front Syst Neurosci. 2015;9(162) doi: 10.3389/fnsys.2015.00162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Riemer R., Shapiro A. Biomechanical energy harvesting from human motion: theory, state of the art, design guidelines, and future directions. J NeuroEng Rehabil. 2011;8(1) doi: 10.1186/1743-0003-8-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Purwadi A., Parasuraman S., Khan M., Elamvazuthi I. Development of biomechanical energy harvesting device using heel strike. Procedia Computer Science. 2015;76:270–275. [Google Scholar]
- 67.Li Q., Naing V., Donelan J. Development of a biomechanical energy harvester. J NeuroEng Rehabil. 2009;6(1) doi: 10.1186/1743-0003-6-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Paul M. MSc. University of Salford; 2015. Sensory Feedback System for Prosthetic Arms. [Google Scholar]
- 69.Lake C. The evolution of upper limb prosthetic socket design. JPO J Prosthetics Orthot. 2008;20(3):85–92. [Google Scholar]
- 70.Ottobockus.com 2019. https://www.ottobockus.com/prosthetics/upper-limb-prosthetics/solution-overview/passive-arm-prostheses/ Passive Arm Prostheses. [online] Available at:
- 71.Sites.google.com Upper limb bones - the human skeletal system. 2000. https://sites.google.com/site/thehumanskeletalsystemiscool/structure/upper-limb-bones [online] Available at: