

Abstract
Background
Lateral ankle sprains are common in indoor sports. High shoe–surface friction is considered a risk factor for non-contact lateral ankle sprains. Spraino is a novel low-friction patch that can be attached to the outside of sports shoes to minimise friction at the lateral edge, which could mitigate the risk of such injury. We aimed to determine preliminary effectiveness (incidence rate and severity) and safety (harms) of Spraino to prevent lateral ankle sprains among indoor sport athletes.
Methods
In this exploratory, parallel-group, two-arm pilot randomised controlled trial, 510 subelite indoor sport athletes with a previous lateral ankle sprain were randomly allocated (1:1) to Spraino or ‘do-as-usual’. Allocation was concealed and the trial was outcome assessor blinded. Match and training exposure, number of injuries and associated time loss were captured weekly via text messages. Information on harms, fear-of-injury and ankle pain was also documented.
Results
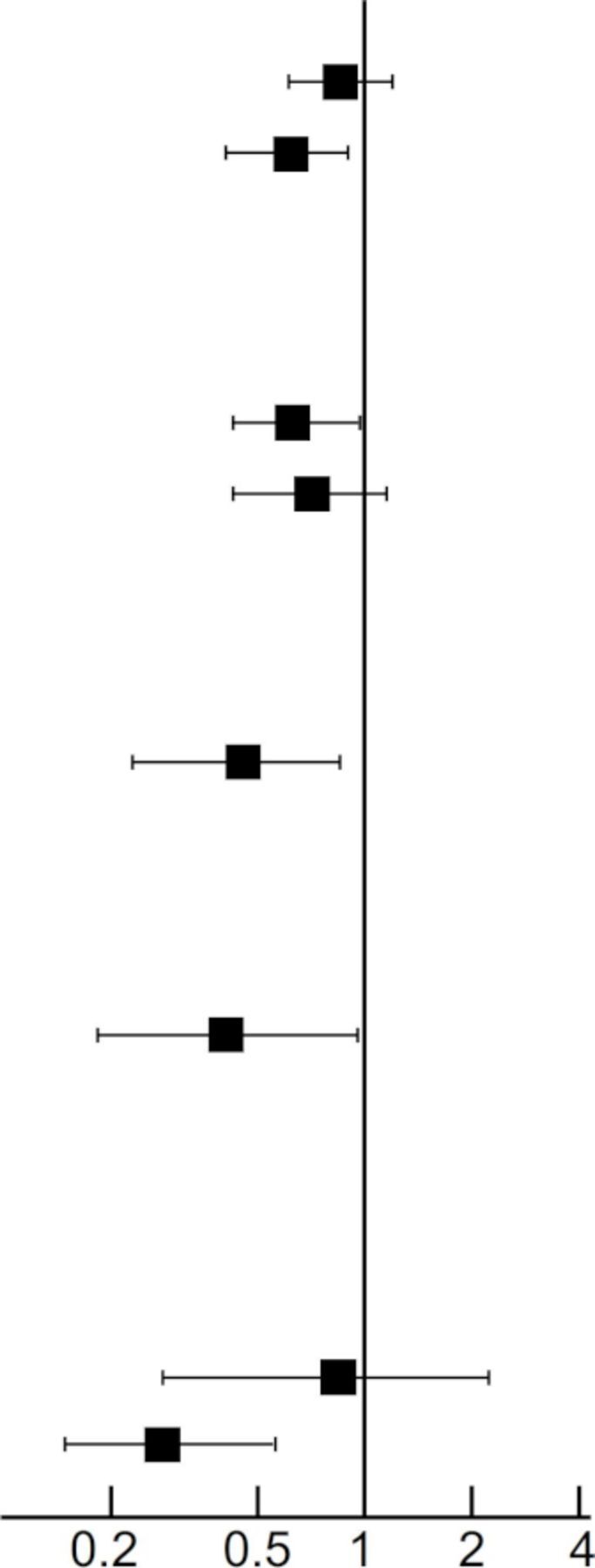
480 participants completed the trial. They reported a total of 151 lateral ankle sprains, of which 96 were categorised as non-contact, and 50 as severe. All outcomes favoured Spraino with incidence rate ratios of 0.87 (95% CI 0.62 to 1.23) for all lateral ankle sprains; 0.64 (95% CI 0.42 to 0.98) for non-contact lateral ankle sprains; and 0.47 (95% CI 0.25 to 0.88) for severe lateral ankle sprains. Time loss per injury was also lower in the Spraino group (1.8 vs 2.8 weeks, p=0.014). Six participants reported minor harms because of Spraino.
Conclusion
Compared with usual care, athletes allocated to Spraino had a lower risk of lateral ankle sprains and less time loss, with only few reported minor harms.
Trial registration number
Keywords: sports, ankle, sprain, randomised controlled trial, injury prevention
Video Abstract.
Introduction
A 2014 systematic review on incidence and prevalence of lateral ankle sprain injuries identified indoor sports as ‘high risk’ sports, reporting a pooled injury incidence rate of 7 sprains per 1000 exposures.1 This conspicuously high incidence rate was highlighted in an evidence review from the International Ankle Consortium,2 as well as in a 2018 clinical guideline.3
High friction between shoe and surface is a posited risk factor for non-contact lower limb injuries across various sports,4–7 and shoe–surface friction is generally high in indoor sports.5 The majority of lateral ankle sprains occur via a ‘non-contact’ injury mechanism,1 2 8 in which the shoe is only in contact with the floor, indicating that high shoe–surface friction is an important part of the injury mechanism.
Spraino is a new low-friction patch (figure 1) designed to prevent these ‘friction-related’ sprains in indoor sports by minimising friction at the lateral edge of the shoe sole and thus removes the anchoring point between shoe and floor, around which non-contact lateral ankle sprains typically occur.9 Removing that anchor reorients the vector of the ground reaction force (figure 2) allows the foot to realign more easily and prevents the rapid excessive inversion and internal rotation associated with lateral ankle sprains10 (online supplementary video). The first natural step following promising laboratory testing is to establish ‘proof-of-principle’,11 preliminary evidence of effectiveness, on clinically relevant endpoints. At present, it is unknown how Spraino might affect important clinical outcomes.
Figure 1.

Indoor sports shoe with Spraino low-friction patches attached on the outside.
Figure 2.

Preventive mechanism of Spraino: in case of a bad landing, Spraino minimises the otherwise high shoe–surface friction at the lateral edge of the shoe. This minimises the horizontal ground reaction forces (GRFs), thereby bringing the GRF vector closer towards the joint centre which serves to prevent excessive ankle inversion and internal rotation.
bjsports-2019-101767supp001.mp4 (19.5MB, mp4)
Therefore, the aims of this exploratory pilot trial were to determine preliminary effectiveness and safety of using Spraino to prevent lateral ankle sprains among subelite indoor sport athletes with a previous lateral ankle sprain, when compared with a ‘do-as-usual’ control group.
Methods
Design
We designed and conducted a two-arm, parallel-group, exploratory pilot randomised controlled trial to assess proof-of-principle for Spraino, being preliminary effectiveness and safety in lateral ankle sprain injury prevention among high risk indoor sport athletes. Participants were randomly allocated (1:1) to an intervention (Spraino) group or a control (do-as-usual) group. The trial was registered at ClinicalTrials.gov (NCT03311490) on 17 October 2017 and enrolment was conducted between 19 October 2017 and 28 February 2018. The trial protocol (online supplementary appendix S6) was developed using the PREPARE trial guide12 and Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) checklist.13 We report the trial using the Consolidated Standards of Reporting Trials (CONSORT) 2010 extension for pilot and feasibility trials.14
bjsports-2019-101767supp002.pdf (1.2MB, pdf)
Participants
Participants were recruited from 91 indoor sports teams (handball, basketball and badminton) competing at divisional or league level in Denmark. Participants were eligible for inclusion if they: (1) were aged 18 years or older; (2) could read, speak and understand Danish; (3) could receive and reply to text messages using Short Message Services (SMS); (4) performed indoor sport in a subelite level team with at least 2 weekly practice sessions; (5) had incurred at least one lateral ankle sprain in the preceding 24 months; and (6) had returned to play at the commencement of our trial.
We included athletes with a previous lateral ankle sprain as they are at particularly ‘high risk’ of new injury,15 16 making injury risk mitigation pertinent. At the time of recruitment, all athletes were participating fully in their sport and reported no acute injury symptoms.
Sample size
The sample size was determined by the formula where n is the number of participants in each arm, T the observation time, and θ0 and θ1 the incidence rates in the control and intervention group.17 We anticipated an incidence rate of 4.9 ankle sprains per 1000 hours of exposure1 without Spraino, and an incidence rate of 2.94 per 1000 hours in participants randomised to Spraino (40% lower). With a power of 80% and an α of 5%, an exposure time of ~15 350 hours would be needed in each arm. Assuming an average exposure of 3 hours of court activities per week per participant (including off-season), 250 participants would be needed to be observed for 20 weeks. Assuming a dropout rate of 15%, the 250 participants should be observed for at least 23 weeks.
Randomisation
Randomisation was performed after the included participants had provided written consent and the completed baseline questionnaires had been collected. We generated the two comparison groups using balanced block randomisation. The random component in the sequence generation process was a drawing of lots. Block sizes were determined by the number of enrolled participants within a given team, with an equal amount of lots representing allocation for intervention and control being used to assure a 1:1 allocation ratio (ie, if a team had 9 enrolled players, then 10 lots, 5 representing each group (intervention and control), were included). The lots (wooden beads) were identical in appearance and drawn from an opaque bag. It was ensured that allocation was concealed for participants and investigators enrolling participants.
Intervention
Spraino was given to the intervention group with the purpose of mitigating the risk of lateral ankle sprain, while the control group was a do-as-usual comparator. Spraino comprises a set of adhesive patches, which are attached along the lateral edge of the shoe (figure 1). The front patch covers 2–4 mm of the shoe sole while the rear patch does not cover the edge (online supplementary video). Spraino is intended for use in indoor sports and has a reported durability of 20–40 hours of activity.18
The intervention group received Spraino and application instructions on the same day of inclusion, along with a leaflet (online supplementary appendix S5) containing information on how to order new patches and how to report adverse events associated with its use. They were encouraged to use Spraino during all indoor sport activities. Participants of both groups were also permitted to use (or keep using) any other injury preventive measure of their choice.
Patient and public involvement
Questionnaires and SMS questions were piloted and redesigned with help from 25 athletes. Twenty intervention group participants gave post-trial feedback on both the intervention and study design and conduct. The National Olympic Committee created awareness and helped recruit participating teams.
Injury registration and data collection
The participants completed a baseline questionnaire19 (online supplementary table S2), from which mobile phone numbers were obtained to prospectively collect data in SMS-Track20 21 through answers to 6 weekly standardised questions (online supplementary figure S3).
When replying to the SMS questions, participants were required to report: (Q1, Q2) their weekly training and match exposure; (Q3) whether they had incurred a lateral ankle sprain; (Q4) whether their participation was restricted due to a lateral ankle sprain; (Q5) whether they used any ankle injury prevention measure; (Q6) whether they adhered to the intervention. Reminder messages were sent out after 48 hours if an answer to a text message had not been collected. They received a reminder phone call if answers had not been received for two consecutive weeks.
If a lateral ankle sprain, or a participation restriction due to an ankle-related problem, was reported via the SMS system, a follow-up telephone interview was conducted by a member of the research team (online supplementary figure S3). If a lateral ankle sprain was incurred, a detailed injury registration form was completed (online supplementary table S4).
The occurrence of adverse events related to the use of Spraino was closely monitored by a member of the research team.
Outcome measures
Being exploratory, our trial was designed without a predetermined hierarchy among outcome measures. Data on contact and non-contact lateral ankle sprains, as well as in-trial first-time injuries and injury recurrences were documented. A contact sprain was defined as an injury incurred by stepping/landing directly onto an object (ie, opponent’s foot). A non-contact sprain was defined as an injury incurred without stepping onto something (other than the floor), regardless of any player-to-player interaction prior to the event. A recurrent sprain was defined as a subsequent sprain to the same ankle previously injured within the trial period.22 23
Time-loss following a sprain was defined as number of calendar weeks with time lost from unrestricted participation due to injury-associated symptoms,24 and was based on the response to Q4 (online supplementary figure S3). As such, an ankle sprain resulted in time-loss if: (Q4=1) the participant had reduced their participation in their primary sport; or (Q4=2) the participant was affected but still participated. A sprain was considered ‘severe’ if the participant experienced time-loss for more than 3 weeks.25 Time-loss recordings for each injury was stopped on the first day of a consecutive 3 week period during which the participant could participate unrestricted in his/her primary sport to assure a causal link between injury and acute time-loss.
Additional outcomes included pain in the ankle joint during sport (NRS: 0–10)26 and fear of injury (NRS: 0–100)27 assessed at baseline and follow-up using numeric rating scales (NRS). The intervention group were instructed to report adverse events they associated with Spraino.
Statistical analysis
Lateral ankle sprain incidence rates per 1000 hours of exposure, differences and incidence rate ratios (IRRs, Spraino vs control) were estimated using Poisson regression with the sum of match play and practice hours as exposure. The effectiveness estimates were adjusted for sex, age, type of sport and level of play. Injury recurrence was estimated similarly but only containing exposure from in-trial injured participants. Mean time loss for participants who sustained an ankle sprain was calculated using negative binomial regression. Robust standard errors were calculated to adjust for the repeated nature of measurements (within-participant correlation).
Change in fear of sustaining an ankle sprain, and change in ankle pain, from baseline to follow-up, were calculated using negative binomial regression, adjusting for the values reported at baseline.28 Multiple imputations by chained equations were performed to account for missing values.29 The imputation procedure included variables (age, sex, group allocation and type of sport) prehypothesised to potentially predict missing information. Data were analysed using the mi estimate command in Stata (20 imputations) which first runs the estimation command on each imputation separately and then combines results using Rubin’s rule.30 Analyses were also conducted for participants with full information only (available case analysis).
Statistical analyses were conducted in Stata/IS V.13.1 and performed as intention to treat using inverse probability-of-censoring weighting to account for participant dropout.28 31 Adhering to the intention-to-treat principle, Spraino adherence and cointerventions were not taken into account in the analysis. The outcome assessor was blinded to group allocation.
Deviations from registration
Five outcomes were not prespecified in the ClinicalTrials.gov registration. First-time and in-trial recurrent events were combined to investigate (1) the overall effectiveness on injury severity (time-loss), (2, 3) injury mechanism (non-contact sprains and associated time loss), (4) rate of severe ankle sprains and (5) time loss for in-trial recurrences. These measures were missed in oversight during the registration process but added to the analysis plan (4 December 2018) before the trial was analysed and unblinded (26 December 2018). The full trial protocol is available as online supplementary appendix S6 and results of all prespecified outcomes are found in online supplementary table S1.
Results
Recruitment and trial completion
Five hundred and ten participants were recruited and randomised from 1339 approached athletes of which 576 were eligible for inclusion (figure 3). Four hundred and eighty participants completed the trial: 246 in the intervention (Spraino) group and 234 in the control (do-as-usual) group. Completion was defined as having responded at least once to the weekly text messages. Our prospective registration of injuries was originally specified to be conducted over a 52-week period. However, as the number of events required for statistical analyses was achieved sooner than anticipated, the trial was halted on 5 October 2018 (9 months average follow-up). The mean number of participating weeks was slightly higher in the intervention group compared with the control group (20.7 vs 18.2 weeks).
Figure 3.

Consolidated Standards of Reporting Trials flow diagram.
Trial population
The mean age of participants was 22.7 years, 57% were men and the majority were handball players. No clinically relevant between-group differences appeared present (table 1) and no baseline hypothesis testing was undertaken, as suggested by the CONSORT group.14 32
Table 1.
Baseline characteristics
| Spraino | Control | Total | |
| Participants, n | 256 | 254 | 510 |
| Male, n (%) | 146 (57) | 146 (57) | 292 (57) |
| Age, mean (SD) | 22.3 (4.0) | 23.0 (4.5) | 22.7 (4.3) |
| Height (cm), mean (SD) | 181 (10) | 182 (11) | 182 (11) |
| Body mass (kg), mean (SD) | 80.8 (14) | 80.3 (14) | 80.5 (14) |
| Fear*, median (IQR) | 70 (40–90) | 70 (50–90) | 70 (40–90) |
| Pain†, median (IQR) | 2 (0–3) | 1 (0–2) | 1 (0–3) |
| Sport, n (%) | |||
| Handball | 204 (80) | 205 (81) | 409 (80) |
| Basketball | 26 (10) | 31 (12) | 57 (11) |
| Badminton | 26 (10) | 18 (7) | 44 (9) |
| Weekly practice (hours), mean (SD) | 6.1 (3.1) | 6.1 (3.0) | 6.1 (3.0) |
| Level of play, n (%) | |||
| League | 10 (4) | 12 (5) | 22 (4) |
| First division | 80 (31) | 78 (31) | 158 (31) |
| Second division | 64 (25) | 70 (28) | 134 (26) |
| Third division | 102 (40) | 94 (37) | 196 (38) |
*Fear of ankle sprain during primary sport (100=no fear, 0=highest fear imaginable).
†Pain in ankle joint during primary sport (0=no pain, 10=highest pain imaginable).
Intervention effectiveness on incidence rates and incidence-related time loss
A total of 151 lateral ankle sprains were sustained during the trial, of which 96 were categorised as non-contact injuries. Fifty injuries were categorised as severe. The injury incidence rate (sprains per 1000 hours of exposure) was lower in the intervention (Spraino) group compared with the control (do-as-usual) group for all collected outcomes (table 2; online supplementary table S1).
Table 2.
Incidence rates, event-related time loss and effectiveness estimates (Spraino vs control)
| Spraino (n=256) |
Control (n=254) |
Spraino versus Control | |||
| Difference | Ratio* | ||||
| Total exposure (hours) | 18 803 | 14 185 | |||
| Events (151) | |||||
| Number | 81 | 70 |
|
||
| Incidence rate† | 4.30 (3.30 to 5.30) | 4.93 (3.68 to 6.18) | −0.62 (−2.24 to 0.99) | 0.87 (0.62 to 1.23) | |
| Time loss (weeks) | 1.8 (1.3 to 2.3) | 2.8 (2.2 to 3.4) | −1.0 (−1.8 to −0.2) | 0.63 (0.44 to 0.92) | |
| Non-contact events (96) | |||||
| Number | 44 | 52 | |||
| Incidence rate† | 2.33 (1.67 to 3.00) | 3.67 (2.54 to 4.77) | −1.38 (−2.74 to −0.02) | 0.64 (0.42 to 0.98) | |
| Time loss (weeks) | 1.9 (1.1 to 2.7) | 2.7 (2.0 to 3.4) | −0.9 (−2.0 to 0.2) | 0.67 (0.41 to 1.10) | |
| Severe events (50) | |||||
| Number | 19 | 31 | |||
| Incidence rate† | 1.01 (0.51 to 1.50) | 2.20 (1.36 to 3.04) | −1.17 (−2.13 to −0.20) | 0.47 (0.25 to 0.88) | |
| Non-contact severe events (34) | |||||
| Number | 12 | 22 | |||
| Incidence rate† | 0.63 (0.25 to 1.02) | 1.56 (0.82 to 2.30) | −0.89 (−1.74 to −0.04) | 0.43 (0.19 to 0.97) | |
| In-trial recurrent events (19) | |||||
| Total exposure (hours) | 1889 | 1428 | |||
| Number | 10 | 9 | |||
| Incidence rate† | 5.27 (1.68 to 8.85) | 6.29 (1.81 to 10.8) | −0.99 (−6.81 to 4.84) | 0.85 (0.32 to 2.24) | |
| Time loss (weeks) | 1.1 (0.5 to 1.7) | 3.5 (2.1 to 4.86) | −2.3 (−3.7 to −0.9) | 0.33 (0.15 to 0.72) | |
Numbers in parenthesis represent 95% CIs.
Spraino versus control, ratio <1 indicates preventive effect.
*Incidence rate ratio or relative time-loss duration.
†Per 1000 hours of participation in primary sport.
The IRR was 0.87 (95% CI 0.62 to 1.23) for any type of lateral ankle sprain, with a mean time loss of 1.8 weeks (95% CI 1.3 to 2.3) in the intervention (Spraino) group and 2.8 weeks (95% CI 2.2 to 3.4) in the control (do-as-usual) group, resulting in a time-loss difference of 1 week (95% CI −1.8 to −0.2; table 2). The 96 non-contact sprains occurred at a lower rate in the intervention group compared with the control group (IRR of 0.64; 95% CI 0.42 to 0.98) with a time-loss difference per non-contact sprain of 0.9 weeks (95% CI −2.0 to 0.2). For all severe lateral ankle sprains, the IRR was 0.47 (95% CI 0.25 to 0.88) and for severe non-contact sprains the IRR was 0.43 (95% CI 0.19 to 0.97), both favouring the intervention group.
The 19 in-trial injury recurrences occurred at similar rate in the two groups (IRR of 0.85; 95% CI 0.31 to 2.34), with 2.3 weeks (95% CI −3.7 to −0.9) less event-related time loss in the intervention (Spraino) group (table 2).
Intervention effectiveness on fear and pain during sport
Four hundred and fifty-five participants provided full information on fear and pain at baseline, while 281 provided full information at follow-up. The mean fear of sustaining an ankle sprain during sport decreased in both groups. A between-group difference of 13.7 points (95% CI 9.2 to 18.3) was observed (table 3). The mean level of pain in the ankle decreased in the intervention group while it increased in the control group. A between-group difference of −1.2 points (95% CI −1.5 to −0.9) was observed (table 3).
Table 3.
Fear of new ankle sprain* and pain in the ankle† at baseline and follow-up, and between-group difference for change adjusted for baseline values (Spraino vs control)
| Mean (95% CI) | Between-group difference for change | ||
| Spraino | Control | ||
| Fear*, intention to treat (n) | 254 | 256 | |
| Baseline | 62.9 (59.1 to 66.6) | 66.6 (63.1 to 70.1) | 13.7 (9.2 to 18.3) |
| Follow-up | 84.7 (82.2 to 87.2) | 70.9 (67.2 to 74.7) | |
| Fear*, available case (n) | 146 | 122 | |
| Baseline | 62.9 (59.1 to 66.6) | 66.6 (63.1 to 70.1) | 15.4 (10.2 to 20.7) |
| Follow-up | 85.0 (82.4 to 87.5) | 69.5 (65.2 to 73.9) | |
| Pain†, intention to treat (n) | 254 | 256 | |
| Baseline | 1.9 (1.7 to 2.1) | 1.6 (1.4 to 1.8) | −1.2 (–1.5 to –0.9) |
| Follow-up | 0.6 (0.5 to 0.7) | 1.8 (1.6 to 2.0) | |
| Pain†, available case (n) | 152 | 127 | |
| Baseline | 1.9 (1.7 to 2.1) | 1.6 (1.4 to 1.8) | −1.3 (–1.6 to –1.0) |
| Follow-up | 0.6 (0.4 to 0.7) | 1.9 (1.6 to 2.2) | |
Numbers in parenthesis represent 95% CIs.
*Fear of sustaining a new ankle sprain during sport was measured on a scale from 100 representing no fear to 0 representing maximum fear. A change of >0 reflects less fear at follow-up as compared with baseline.
†Pain in the ankle during sport was measured on a scale from 0 representing no pain to 10 representing worst pain imaginable. A change of <0 reflects less pain at follow-up as compared with baseline.
Adherence
Full adherence in the intervention group was defined as having reported to use Spraino for at least 75% of the week, during all weeks of participation. This was observed in 31 (13%) participants, while 49 (20%) reported not to have used Spraino at all. The 80% of the intervention group participants, who reported to have used Spraino, were adherent for 68% of the participating weeks. Treatment contamination was observed whereby 5 (3%) participants in the control group reported use of Spraino.
Harms
Six participants reported eight adverse events leading to minor harms during the trial (table 4). Of these, four participants experienced harm in the form of an ankle sprain.
Table 4.
Intervention-related adverse events leading to harm
| Participant info | Event report to hotline |
| Handball player, female 19 years | ‘I rolled over due to the tape. Maybe it was placed wrong.’ (Reported as having occurred twice) |
| Handball player, female 20 years | ‘Had a slipping incident (due to Spraino) at training where I fell and got some bruises. Nothing serious though.’ |
| Handball player, male 22 years | ‘I had an existing groin injury that I felt got worsened through an outwards rotation due to the tape.’ |
| Badminton player, male 23 years | ‘Rolled over twice and (I am) 100% certain it is due to the tape. Jumping towards my right when my foot slides underneath me.’ (Reported as having occurred twice) |
| Handball player, male 29 years | ‘I felt that it was the tape that made me twist my ankle. Took it off afterwards.’ |
| Badminton player, male 20 years | ‘Made a lunge with my left leg and twisted my ankle. Felt like the tape increased the twist.’ |
Discussion
This trial was designed to assess proof-of-principle of Spraino by determining preliminary effectiveness and safety in lateral ankle sprain injury prevention, when added to do-as-usual injury prevention among subelite indoor sport athletes with a previous sprain injury. In general, we found that Spraino had a protective effect across outcome measures, as the incidence rate of non-contact sprains and severe sprains was lower for those randomised to Spraino than those randomised to usual care.
Interpretation
Most of the injuries incurred in this trial occurred via a non-contact injury mechanism. This aligns with previously published literature2 8 33 and was the case for 74% (52 out of 70) of sprains in the control (do-as-usual) group and 54% (44 out of 81) in the intervention (Spraino) group. The lower incidence rate and proportion of non-contact sprains in the intervention group brings notion to the thought of excessive friction as an important risk factor for lower extremity injuries in sports.4–7 34
Average time loss was significantly 37% lower in the intervention (Spraino) group. They returned to sports participation without restriction 1 week faster following injury on average, than did controls. For in-trial recurrent events, event-related time loss was 67% lower in the intervention (Spraino) group (1.1 vs 3.5 weeks).
The additive effectiveness of Spraino on injury incidence rate found in this study is comparable to the effects of other preventive measures (ie, exercise and external prophylactic measures like bracing and taping) when these are compared with no measure.15 That Spraino was associated with lower injury severity contrasts directly with the results of previous studies, that investigated other prophylactic measures, who found no reduction in time-loss per injury.35 Our results support the premise that Spraino can mitigate the risk of sprain injuries among indoor sport athletes, and that its use is not associated with severe adverse consequences.
The intervention (Spraino) group had 21.8 points lower fear of ankle sprain injuries; the between-group difference of 13.7 points is less than minimal clinically important difference(MCID = 19.0)36 but could still be of some importance with persisting fear of injury being regarded as a major hindrance to sports activity.27 Pain is a frequent and debilitating problem following musculoskeletal injury. The between-group difference of 1.2 points (11 NRS) in ankle pain, favouring Spraino, may not be clinically relevant considering an MCID of 2 points.26 However, our findings related to fear and pain suggest that Spraino may have further beneficial effects, aside from injury prevention.
Implications
Considering the high risk of both initial and recurrent ankle sprains in indoor sports,1 33 and with 40% of the approached population being eligible due to having sustained an ankle sprain within 24 months prior to the trial, prevention seems relevant to a large population of indoor sport athletes. Clinicians should consider advising indoor sport athletes to use Spraino given its effectiveness in lowering the incidence rate of lateral ankle sprains, without any severe adverse consequences. Spraino may be particularly relevant for those athletes with subjective reporting of pain, fear of injury and ankle instability.37
Strengths and limitations
We acknowledge several limitations. First, not all presented outcomes were preregistered. These outcomes were however added before analysis and fit the overall pattern of Spraino effectiveness. Second, only passive surveillance of harms was used, which generally yields fewer adverse events than active monitoring.38 Third, participants were not blinded to the intervention. This is not regarded as a limitation to the objective outcomes: incidence rate and time loss. However, the risk of bias is high on the subjective outcomes (fear and pain).
We did not control for the use of other injury prevention strategies, since Spraino was introduced as an additional preventive measure. However, the combination of less than perfect adherence to Spraino, treatment contamination and do-as-usual injury prevention in the control group makes the effectiveness across all outcomes highly promising. The intervention mirrors real life use of Spraino as all athletes were responsible for applying and replacing the product.
What are the findings?
Spraino shows promising effects and appears safe when used to mitigate the risk of non-contact lateral ankle sprain injuries in indoor sport athletes.
Athletes randomised to Spraino had a 53% lower incidence rate of severe lateral ankle sprain injuries than did the control athletes.
Spraino seems to reduce ankle-related pain and fear of lateral ankle sprain injuries.
How might it impact on clinical practice in the future?
Clinicians might consider recommending that indoor sports athletes with a previous lateral ankle sprain injury use Spraino.
Spraino may be a relevant add-on for athletes in instances where previous preventive measures have been ineffective.
Acknowledgments
The authors wish to acknowledge Jonas Bak for stepping in during the final months of data collection, and The National Olympic Committee and Sports Confederation of Denmark (DIF), and the respective federations (DHF, DBBF and Badminton Denmark), for their valuable contribution in creating awareness and help in recruiting participating teams.
Footnotes
Twitter: @FilipGertz, @TBandholm, @MikkelBek, @EamonnDelahunt, @KThorborg
Contributors: TBG, FGL and UK conceived the study. KT, TB, ED, PBP and MBC designed the trial. TBG and UK were grant holders. SM managed the collection of data under the supervision of MBC. JST provided statistical and epidemiological expertise and conducted the statistical analyses. TB, KT and ED provided clinical scientific expertise throughout the study. KT supervised the study in its entirety. All authors contributed to refinement of the article and approved the final manuscript.
Funding: The trial was funded by Copenhagen Center for Health Technology (CACHET), grant number RFH-15-00013 and Innovation Fund Denmark, grant number 7038-00087A. Spraino ApS provided the low-friction shoe patches, worth approx. €19 000.
Competing interests: TBG is the founder of Spraino ApS. FGL is a paid employee in Spraino ApS. Spraino ApS was responsible for provision of Spraino. The conflict was accommodated by restricting Spraino ApS and authors FGL and TBG from having any deciding role in the design of the study, in the execution, analyses, interpretation of data, or decision to submit results. Statistical analyses were performed externally by JS who was blinded to group allocation. KT had full authority of the trial administration. The three senior clinical researchers (KT, TB and ED) had full authority in terms of submission for publication. Copenhagen Center for Health Technology (CACHET) and Innovation Fund Denmark had no scientific role in the trial. KT is an Associate Editor of the British Journal of Sports Medicine. ED is a Senior Associate Editor of the British Journal of Sports Medicine in the area of foot and ankle injuries.
Patient and public involvement: Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication: Not required.
Ethics approval: Ethics approval was obtained from The North Denmark Region Committee on Health Research Ethics on 5 July 2017.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data are available upon reasonable request.
References
- 1. Doherty C, Delahunt E, Caulfield B, et al. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med 2014;44:123–40. 10.1007/s40279-013-0102-5 [DOI] [PubMed] [Google Scholar]
- 2. Gribble PA, Bleakley CM, Caulfield BM, et al. Evidence review for the 2016 international ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med 2016;50:1496–505. 10.1136/bjsports-2016-096189 [DOI] [PubMed] [Google Scholar]
- 3. Vuurberg G, Hoorntje A, Wink LM, et al. Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline. Br J Sports Med 2018;52:956 10.1136/bjsports-2017-098106 [DOI] [PubMed] [Google Scholar]
- 4. Dragoo JL, Braun HJ. The effect of playing surface on injury rate: a review of the current literature. Sports Med 2010;40:981–90. 10.2165/11535910-000000000-00000 [DOI] [PubMed] [Google Scholar]
- 5. Olsen OE, Myklebust G, Engebretsen L, et al. Relationship between floor type and risk of ACL injury in team handball. Scand J Med Sci Sports 2003;13:299–304. 10.1034/j.1600-0838.2003.00329.x [DOI] [PubMed] [Google Scholar]
- 6. Pasanen K, Parkkari J, Rossi L, et al. Artificial playing surface increases the injury risk in pivoting indoor sports: a prospective one-season follow-up study in Finnish female floorball. Br J Sports Med 2008;42:194–7. 10.1136/bjsm.2007.038596 [DOI] [PubMed] [Google Scholar]
- 7. Wannop JW, Worobets JT, Stefanyshyn DJ. Footwear traction and lower extremity joint loading. Am J Sports Med 2010;38:1221–8. 10.1177/0363546509359065 [DOI] [PubMed] [Google Scholar]
- 8. Herzog MM, Mack CD, Dreyer NA, et al. Ankle Sprains in the National Basketball association, 2013-2014 through 2016-2017. Am J Sports Med 2019;47:2651–8. 10.1177/0363546519864678 [DOI] [PubMed] [Google Scholar]
- 9. Wright IC, Neptune RR, van den Bogert AJ, et al. The influence of foot positioning on ankle sprains. J Biomech 2000;33:513–9. 10.1016/S0021-9290(99)00218-3 [DOI] [PubMed] [Google Scholar]
- 10. Lysdal FG, Jakobsen L, Grønlykke TB, et al. A kinematic analysis of the Spraino ® realignment mechanism during simulated noncontact ankle sprain injuries. Footwear Sci 2019;11:S167–9. 10.1080/19424280.2019.1606309 [DOI] [Google Scholar]
- 11. Schmidt B. Proof of principle studies. Epilepsy Res 2006;68:48–52. 10.1016/j.eplepsyres.2005.09.019 [DOI] [PubMed] [Google Scholar]
- 12. Bandholm T, Christensen R, Thorborg K, et al. Preparing for what the reporting checklists will not tell you: the prepare trial guide for planning clinical research to avoid research waste. Br J Sports Med 2017;51:1494–501. 10.1136/bjsports-2017-097527 [DOI] [PubMed] [Google Scholar]
- 13. Chan A-W, Tetzlaff JM, Gøtzsche PC, et al. Spirit 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ 2013;346:e7586–42. 10.1136/bmj.e7586 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Eldridge SM, Chan CL, Campbell MJ, et al. Consort 2010 statement: extension to randomised pilot and feasibility trials. Pilot Feasibility Stud 2016;2:1–32. 10.1186/s40814-016-0105-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Verhagen EALM, Bay K. Optimising ankle sprain prevention: a critical review and practical appraisal of the literature. Br J Sports Med 2010;44:1082–8. 10.1136/bjsm.2010.076406 [DOI] [PubMed] [Google Scholar]
- 16. Tassignon B, Verschueren J, Delahunt E, et al. Criteria-based return to sport decision-making following lateral ankle sprain injury: a systematic review and narrative synthesis. Sports Med 2019;49:601–19. 10.1007/s40279-019-01071-3 [DOI] [PubMed] [Google Scholar]
- 17. van Belle G. Statistical rules of thumb. 2nd ed New York: John Wiley & Sons, Inc, 2002. [Google Scholar]
- 18. Spraino ApS Produktinformation. Copenhagen: Spraino ApS, 2017. [Google Scholar]
- 19. Dick R, Agel J, Marshall SW. National collegiate athletic association injury surveillance system commentaries: introduction and methods. J Athl Train 2007;42:173–82. [PMC free article] [PubMed] [Google Scholar]
- 20. Møller M, Attermann J, Myklebust G, et al. Injury risk in Danish youth and senior elite handball using a new SMS text messages approach. Br J Sports Med 2012;46:531–7. 10.1136/bjsports-2012-091022 [DOI] [PubMed] [Google Scholar]
- 21. Møller M, Wedderkopp N, Myklebust G, et al. Validity of the SMS, phone, and medical staff examination sports injury surveillance system for time-loss and medical attention injuries in sports. Scand J Med Sci Sports 2018;28:252–9. 10.1111/sms.12869 [DOI] [PubMed] [Google Scholar]
- 22. Delahunt E, Coughlan GF, Caulfield B, et al. Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med Sci Sports Exerc 2010;42:2106–21. 10.1249/MSS.0b013e3181de7a8a [DOI] [PubMed] [Google Scholar]
- 23. Gribble PA, Delahunt E, Bleakley C, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the International ankle Consortium. Br J Sports Med 2014;48:1014–8. 10.1136/bjsports-2013-093175 [DOI] [PubMed] [Google Scholar]
- 24. Janssen KW, van Mechelen W, Verhagen EALM. Bracing superior to neuromuscular training for the prevention of self-reported recurrent ankle sprains: a three-arm randomised controlled trial. Br J Sports Med 2014;48:1235–9. 10.1136/bjsports-2013-092947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Roos KG, Kerr ZY, Mauntel TC, et al. The epidemiology of lateral ligament complex ankle sprains in national collegiate athletic association sports. Am J Sports Med 2017;45:201–9. 10.1177/0363546516660980 [DOI] [PubMed] [Google Scholar]
- 26. Salaffi F, Stancati A, Silvestri CA, et al. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J Pain 2004;8:283–91. 10.1016/j.ejpain.2003.09.004 [DOI] [PubMed] [Google Scholar]
- 27. Webster KE, Feller JA, Lambros C. Development and preliminary validation of a scale to measure the psychological impact of returning to sport following anterior cruciate ligament reconstruction surgery. Phys Ther Sport 2008;9:9–15. 10.1016/j.ptsp.2007.09.003 [DOI] [PubMed] [Google Scholar]
- 28. Mansournia MA, Altman DG. Invited commentary: methodological issues in the design and analysis of randomised trials. Br J Sports Med 2018;52:553–5. 10.1136/bjsports-2017-098245 [DOI] [PubMed] [Google Scholar]
- 29. Spratt M, Carpenter J, Sterne JAC, et al. Strategies for multiple imputation in longitudinal studies. Am J Epidemiol 2010;172:478–87. 10.1093/aje/kwq137 [DOI] [PubMed] [Google Scholar]
- 30. Rubin DB. Multiple imputation for nonresponse in surveys. Wiley-Interscience, 2004. [Google Scholar]
- 31. Mansournia MA, Altman DG. Inverse probability weighting. BMJ 2016;352:i189. 10.1136/bmj.i189 [DOI] [PubMed] [Google Scholar]
- 32. Schulz KF, Altman DG, Moher D, et al. Consort 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:c332 10.1136/bmj.c332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Fong DT-P, Hong Y, Chan L-K, et al. A systematic review on ankle injury and ankle sprain in sports. Sport Med 2007;37:73–94. 10.2165/00007256-200737010-00006 [DOI] [PubMed] [Google Scholar]
- 34. Orchard JW, Powell JW. Risk of knee and ankle sprains under various weather conditions in American football. Med Sci Sports Exerc 2003;35:1118–23. 10.1249/01.MSS.0000074563.61975.9B [DOI] [PubMed] [Google Scholar]
- 35. McGuine TA, Brooks A, Hetzel S. The effect of lace-up ankle braces on injury rates in high school basketball players. Am J Sports Med 2011;39:1840–8. 10.1177/0363546511406242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Zarzycki R, Failla M, Arundale AJH, et al. Athletes with a positive psychological response to return to sport training have better outcomes one and two years after ACL reconstruction. Orthop J Sport Med 2017;5:2325967117S0032 10.1177/2325967117S00324 [DOI] [Google Scholar]
- 37. Lentell G, Baas B, Lopez D, et al. The contributions of proprioceptive deficits, muscle function, and anatomic laxity to functional instability of the ankle. J Orthop Sports Phys Ther 1995;21:206–15. 10.2519/jospt.1995.21.4.206 [DOI] [PubMed] [Google Scholar]
- 38. Ioannidis JPA, Evans SJW, Gøtzsche PC, et al. Better reporting of harms in randomized trials: an extension of the CONSORT statement. Ann Intern Med 2004;141:781–8. 10.7326/0003-4819-141-10-200411160-00009 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bjsports-2019-101767supp001.mp4 (19.5MB, mp4)
bjsports-2019-101767supp002.pdf (1.2MB, pdf)