

Abstract
Epidemiology, prevention, early management of cervical spine trauma and it's reduction are the objectives of this review paper. A PubMed and MEDLINE search between 2009 and 2019 were conducted using keywords. Case reports, experimental studies, papers other than English language and and unrelated studies were excluded. Up-to-date information on epidemiology of spine trauma, prevention, early emergency management, transportation, and closed reduction were reviewed and statements were produced to reach a consensus in 2 separate consensus meeting of World Federation of Neurosurgical Societies (WFNS) Spine Committee. The statements were voted and reached a positive or negative consensus using Delphi method. Global incidence of traumatic spinal injury is higher in low- and middle-income countries. The most frequent reasons are road traffic accidents and falls. The incidence from low falls in the elderly are increasing in high-income countries due to ageing populations. Prevention needs legislative, engineering, educational, and social efforts that need common efforts of all society. Emergency care of the trauma patient, transportation, and in-hospital acute management should be planned by implementing detailed protocols to prevent further damage to the spinal cord. This review summarizes the WFNS Spine Committee recommendations on epidemiology, prevention, and early management of cervical spine injuries.
Keywords: Spine trauma, Cervical spine injury, Spinal immobilization, Patient transportation, Closed reduction, Cervical facet dislocation
INTRODUCTION
Spinal cord trauma includes several types of spinal cord injury (SCI), spinal nerves, bone, and disco-ligamentous structures of the spine. The injuries may be secondary to closed trauma or penetrating trauma and may involve high and low energy mechanisms. Spinal injuries can lead to instability, pain and impaired mobility, and neurological damage often results in complete or partial paralysis.
Cervical spine and SCI are relatively rare conditions. However, the repercussion of traumatic SCI may be drastic and lead to substantial handicap [1]. SCI can be a severe pathology that results in motor and sensitive involvement and generates a significant impact on the patient’s psychosocial, mental, and social life. Learning epidemiology, reasons of trauma would lead to prepare preventive measures. Prevention needs legislative, engineering, educational, and social efforts that need common efforts of all society. Other than this, emergency care of the trauma patient, transportation, and acute in-hospital management should be planned by implementing detailed protocols to prevent further damage to the spinal cord and roots.
METHODS
A search in PubMed/MEDLINE carried out this review. All papers published during the last 10 years (2009 and 2019) were considered for inclusion. The literature search was done separately using keywords “spinal cord injury epidemiology,” “spinal cord injury prevention,” “spinal cord injury transportation,” “spinal cord injury emergency care,” “cervical closed reduction.” Subsequently, full-text articles were screened for eligibility. Case reports, experimental studies, papers other than English language, and papers older than 10 years were excluded.
Using the keywords “cervical spine fracture and closed reduction” we found 140 papers. After extracting documents before 2010, papers in languages other than English, and unrelated papers, 17 articles remained and evaluated.
The authors (MZ, EOF, NK) independently identified the relevant studies based on the title and abstract. The first consensus meeting was done on June 1, 2019, in Moscow. A re-evaluatiıon meeting was done in November 13, 2019 in Peshawar, Pakistan. The authors prepared statements covering different aspects of the SCI and cervical spine trauma based on the literature review. A presentation based on the literature review and the prepared statements was subjected to discussions, followed by the voting process by the WFNS Spine Committee members using the Delphi method. Answering to the questionnaire each expert voted for all of the statements grading every item on a 5-point scale according to Delphi method: 1 = total disagreement, 2 = disagreement, 3 = agreement, 4 = more than agreement, 5= total agreement. Consensus is reached when the sum of items “1”+“2” or “3”+“4”+“5” exceeds 66%. We called a negative consensus if 1–2> 66%, positive consensus= 3–4–5> 66%, nonconsensus= 1–2 or 3–4–5< 66%. The recommendations were prepared from those statements after a consensus meeting.
1. Epidemiology of Spine Trauma
The world’s incidence has an increasing trend with an estimated annual rate in 10.4–130.6 cases per million despite existing prevention measures. The incidence of SCI varies between 20.7 to 80.0 cases in the United States and 8.0 to 130.6 cases in Europe per million a year [2]. Studies have shown annual costs of up to 2.67 billion dollars [2]. This pathology’s economic burden includes rehabilitation services, personal assistance, loss of productivity due to disability, and social isolation.
Epidemiological data shows great variations in different areas of the world. Data in Latin America comes mainly from Brazil, with a reported incidence of 12.6 per-100,000 inhabitants [3]. The average age in patients with SCI was 39.8 years. They tend to be older in the western pacific region and younger in the United States and Canada. Men are the most affected with a ratio of men/women of 3.37.
Injuries are more frequent in the cervical spine (46.02%) and less prevalent in the lumbosacral spine (24%). Milby et al. [4] have performed a meta-analysis of 65 reports with a total of 281,864 subjects. Their analysis showed an overall prevalence of cervical spine injury (CSI) in all trauma patients as 3.7% (209,320 patients) [4].
Traffic accidents are the most common (39.5%) mechanism, followed by falls (38%). However, there are differences between different regions. For example, falls are the most common mechanism in low-income countries (54%), and sports-related injuries are rare in middle-income countries (2.1%) [3]. Fredø et al. [5] have performed an observational cohort study, analyzing the incidence of traumatic cervical spine fractures in the general population. They reported a rate of 12 cases per 100,000 residents per year with a male predominance and injury due to falls (60%) as the most common trauma mechanism. The next most common mechanism of injury is motor vehicle accidents at 21%. They observed SCI in 10% of cases [5].
A global data survey by Wyndaele and Wyndaele [6] reported a SCI incidence of 10.4 to 83.0 and a prevalence of 233 to 755 per 1 million populations. The authors conclude that most patients with SCI are young males in their thirties with severe neurologic deficits, commonly complete or incomplete paraplegia [6]. O’Connor [7] predicted a 143% increase in SCI cases with incomplete tetraplegia, from 88 cases per year in 1997 to 214 cases per year in 2021 [7].
Reported mortality attributed to SCI is between 0% and 60% [3]. The average in high-income countries is 15.4% unlike 3.8% in middle-income countries. The number of patients requiring surgical intervention is between 36.4% and 59% in the different regions of the world (Fig. 1) [3].
Fig. 1.

Annual incidence of traumatic spinal injury is illustrated by World Health Organization (WHO) region on the left. The burden of traumatic spinal injury is shown by WHO region and income region on the right. Reprinted from Kumar et al. World Neurosurg 2018;113:e345-63, with permission of Elsevier [3].
Mortality is also higher in SCI patients due to traffic accidents 2:1. SCI related to falls in high-income countries tends to be related to falls in the elderly, while in low-income countries, it falls at work. For example, in reports from Pakistan and Nepal, the vast majority of SCI for falls occurred in people working on trees, roofs, or balconies.
SCI can be devastating and associated with an increase in the length of stay, need for continued care after discharge, and mortality compared to patients without this injury.
Although there was a somewhat increased risk for patients involved in motor vehicle crashes, falls, and age older than 40, there was no greater independent risk for patients with head injuries or facial fractures [8]. The pelvic fracture was a significant independent risk factor that increased the risk of CSI 9 times. The combinations of risk factors such as the fall and pelvic fracture, head injury, and pelvic fracture resulted in a 15-fold higher risk of CSI. Patients with these predictor combinations have a high risk of CSI and merit further monitoring. These combinations of risk factors could also be used to improve pre-test probabilities to use diagnostic tools better and improve diagnostic performance [8].
2. Etiology of Spine Trauma
Based on current evidence, the 3 most common mechanisms are traffic accidents, falls, and violence. In Brazil, South Africa, and the United States, SCI incidents due to violence are 42%, 25%, and 11.7%, respectively, mainly due to penetrating trauma from a firearm projectile. Some countries such as Norway, Australia, and Canada reported less than 2% of SCI associated with firearm trauma. In countries such as Finland and Israel, SCI associated with suicide occurs up to 10%. The United States and Canada report the highest rate in SCI associated with sports with 8% [8].
SCI related to occupational accidents is reported in at least 15% of all SCI cases. The use of alcohol or drugs has been identified as an associated factor in 34% of all SCI cases associated with traffic accidents [3].
3. Prevention of Spinal Cord Trauma
Prevention must be the first aim since disability resulting from SCI can be devastating for both patients and society. Some of the data below for the prevention of SCI are taken from the World Health Organization recommendations and the International Spinal Cord Society published in 2013 [9].
1) Road traffic accidents
Certain conditions risk road traffic accidents. Prevention should start with different accident levels such as crash prevention, injury prevention during the crash, and postcrash life-sustaining (Table 1). The impact of traffic accidents can be reduced by measures below [9]:
Table 1.
The Haddon matrix applied to road traffic injury prevention
| Phase | Factors |
|||
|---|---|---|---|---|
| Human | Vehicles and equipment | Environment | ||
| Precrash | Crash prevention | Information | Roadworthiness | Road design and road layout |
| Attitudes | Lighting | Speed limit | ||
| Impairment | Braking | Pedestrian facilities | ||
| Police enforcement | Handling | |||
| Speed management | ||||
| Crash | Injury prevention during the crash | Use of restraints | Occupant restraints | Crash-protective roadside objects |
| Impairment | Other safety devices | |||
| Crash-protective design | ||||
| Postcrash | Life-sustaining | First-aid skills | Ease of access | Rescue facilities |
| Access to medics | Fire risk | Congestion | ||
Adapted from Haddon W Jr. Public Health Rep 1980;95:411-21 [52].
• Enforcing appropriate laws for drink-driving, fatigue, speeding, seat-belt, and helmet use.
• Correctly used 3-point seat-belt systems prevent severe head strikes against interior vehicle structures, which are associated with tension-flexion injuries, avoid ejection from the vehicle, and effectively reduce thoracolumbar injuries.
• Enforcement, coupled with behavioral interventions such as seat-belt reminder systems, has been shown to ensure high seat-belt use levels.
• Child restraint systems according to the child's age and weight are essential in decreasing the risk of injury to infants and children. They are preferable to 2-point lap-belts, which have been associated with thoracolumbar and abdominal injuries.
• Engineering safety measures, such as airbags, restraint systems, and road design. Electronic stability control within cars, i.e., a computerized technology that improves the safety of a vehicle’s stability by detecting and reducing skidding.
• Standards for the design of vehicle seating that specify height requirements for head restraints, as well as high-level seat design, can lessen the probability of cervical spine soft-tissue sprains, i.e., whiplash-type injuries.
• Motorcycle helmets can prevent traumatic brain injury (TBI). But, their role in preventing cervical spinal cord injuries is unclear.
• Educating the public about road safety.
• Barrier systems and road shoulder sealing inroads to promote safe road edges.
2) Falls
The second most common reason for SCI is the falls. Four patterns resulting in SCI have been recognized: (1) falls from the same height, such as playing sports, stumbling over a carpet, (2) falls from less than one-meter heights, such as falling downstairs, falling off a short wall; (3) falls from a meter high or more, for instance, falling from a building or a horse; (4) being hit or crushed by a falling object, for example, cranes, scaffolding, stairs. Many serious falls occur while working or playing a sport, or in unsafe homes or residences. In homes, falls can occur on the stairs. Fall from stairs is principally frequent amongst the elderly and the children.
Preventing falls can be enhanced by adjustments to older people’s living environments, such as the removal of clutter, loose rugs and bumpy surfaces, and the provision of good lighting, railings and appropriate level seats, toilets, and beds. Programs to evaluate balance can detect those at risk and lead to the application of procedures to enhance stability and prevent falls, such as exercise classes. Provision of suitable aiding devices, such as walkers, and training users in its use and maintenance are also helpful [9].
Fall prevention involves adapting the environment, placing laws and regulations, teaching the population about risks, and providing immediate postfall treatment.
3) Violence
One of the most common causes of spinal cord injuries is firearms, either for assaults, self-harm, or involuntary shooting. SubSaharan Africa has the highest reported amount of SCI related to violence in the world (38% of all cases of SCI). Other than firearms, knives and other sharp objects can be used. Bomb explosions can also cause spinal cord injuries [9].
Restricting firearms legislation and lesser firearms ownership tend to have lower levels of gun violence. In countries such as Australia, Austria, Brazil, and New Zealand, restricting firearm, licensing, and bans, the minimum age for purchasing, background checks, have been policies that seem to be effective. Findings in Colombia and El Salvador indicate that the prohibition of carrying firearms in public could reduce homicide rates. Besides, multidimensional strategies are needed to reduce demand for guns, such as dissuading vulnerable youth from gang membership [9].
4) Sport and recreation-related injuries
Several sports and recreational activities have caused SCI. According to research, sports injuries worldwide account for between 7%–18% of all SCI [9].
Diving can cause neurological complications, which results in tetraplegia, and an injury at the level of C4 represents the most common form of diving injury. Diving-related SCI is connected to a lack of diver awareness and education, jumping into shallow water (1.5 m or less), lack of strong indicators and safety regulations, characteristics of the upslope in swimming pools, and alcohol consumption. For example, 63% of SCI in-ground pools in Canada resulted from the diver striking the upslope between the deep and shallow ends of the pool [9]. Some suggestions to reduce the SCI related to diving are: (1) Establish guidelines for private and public pools to promote diving safety; (2) Pool safety emphasizing the dangers of diving and head-first entry into shallow water; (3) Individuals in schools and communities should be educated with evidence and a broad approach about water safety [9].
4. Transportation and Immobilization of Patients With Cervical Spine Trauma
Prehospital immobilization of the cervical spine is commonplace in modern spinal injury management and has largely been unchanged for the last decades. It is a standard procedure and is highly recommended in the overwhelming majority of national and international trauma care guidelines and emergency medical service (EMS) protocols [10-13].
The primary concern during initial EMS management in cases of potential cervical spine trauma is to prevent secondary injury due to possible pathologic motion of the injured spine during patient transportation and medical treatment. About 3%–25% of secondary spinal cord injuries occur either during transit or early management [1,14].
The idea of reducing the risk of neurologic deterioration by immobilizing the patients using a rigid cervical collar and a hard backboard was first postulated in the 1960s. Since then, this strategy was implemented and remained an integral part of many EMS worldwide [1,11].
Prehospital spinal immobilization is a prioritized procedure in the Advanced Trauma Life Support (ATLS) guidelines from the American College of Surgeons [15] and in the Prehospital Trauma Life Support (PHTLS®) guidelines from the National Association of Emergency Medical Technicians [16]. These guidelines dominate the field of EMS care, and are utilized in almost 60 countries [11].
The updated Guidelines for the Management of Acute Cervical Spine and Spinal Cord Injury published in 2013 by the American Association for Neurological Surgeons (AANS) and the Congress of Neurological Surgeons (CNS) Joint Guidelines Committee [17] provided 112 evidence-based diagnostic and treatment recommendations (77 level III, 16 level II, and 19 level I recommendations). The majority of these recommendations are level III [11].
Although spinal immobilization and motion restriction is performed ubiquitously by EMS practitioners and millions of patients with cervical spine trauma are outfitted with a collar, in recent years a growing body of evidence indicates a need to reconsider the routine use of cervical collars and rigid backboards in prehospital trauma care [1,11-13].
1) Cervical spine immobilization
The ATLS and PHTLS guidelines recommend considering CSI or SCI in all patients with multiple injuries and limiting these patients’ spinal motion to protect the spine from further damage until spine injury has been ruled out. It is also essential to have in mind that not all patients need immobilization and that excessive manipulation and inadequate restriction of spinal motion can cause additional neurological damage and worsen the patient’s outcome [15,16].
Exclusion of spinal trauma can be straightforward in patients without neurological deficit, pain, or tenderness along the spine. If there is no evidence of intoxication or additional painful injuries, this virtually excludes significant spinal injury. The possibility of cervical spine injuries may be eliminated special triaging tools, lite the National Emergency X-radiography Utilization Study (NEXUS) tool or the Canadian C-Spine Rule (CCR) which will be discussed later [15].
Evaluation of patients with various degrees of depressed level of consciousness is more complicated and requires appropriate radiographic imaging to exclude spinal injury. If the images are inconclusive, the spine's motion restriction is performed until further testing can be done. It is worth noting that the presence of a cervical collar and backboard can provide a false sense of security. If the patient is not appropriately immobilized, spinal motion is still possible [15].
The 2 most commonly used triaging tools are the NEXUS tool or the CCR. Both the NEXUS and the CCR originally were developed to decide if a trauma patient needs radiographic imaging to diagnose spinal injuries in the hospital setting [1]. In 2011, the CCR was revised and updated for the prehospital settings to decide if a patient needs cervical immobilization [11]. Both tools are commended by the ALTS and PHTLS guidelines [15,16].
Stiell et al. [18] performed a multicenter prospective analysis of the use of the CCR and reported that it is an accurate and reliable tool and can prevent prolonged and uncomfortable immobilization for many trauma patients.
In 2019, Maschmann et al. [1] modified the above-mentioned triaging tools. To reduce overtriage and unnecessary spinal immobilization, they proposed dividing trauma patients into 3 groups: group 1, with no need for stabilization; group 2, with stabilization on a vacuum mattress; and group 3, in need of timecritical stabilization. The authors suggested their spinal trauma decision algorithm based on clinical findings [1].
Studies published in recent years report various associated risks and hazardous effects related to spinal immobilization and call to end this routine practice. The reported risks include pain, increased intracranial pressure, the formation of pressure ulcers, increased difficulty of clinical examination, prolonged prehospital on-scene time, difficulty in performing vital procedures like endotracheal intubation, incorrect placement of cervical collars, and risk of fracture displacement in the elderly [1,12,13].
Chendrasekhar et al. [19] reported that pressure-related ulcers after cervical collar placement correlate with the duration of cervical immobilization. Kolb et al. [20] said an association between cervical spine immobilization using rigid collars and elevated ICP, noting a modest to a significant rise in intracranial pressure (ICP) which should be considered in patients with associated TBI. It should always be kept in mind when assessing the need for a cervical collar, that approximately 5% of patients with TBI have an associated spinal injury, and about 25% of patients with spinal injury have at least a mild TBI [14,15,21].
The AANS/CNS Guidelines for the Management of Acute Cervical Spine and Spinal Cord Injury list clinical criteria to select appropriate patients for spinal immobilization [14]: (1) spinal pain or tenderness, including any neck pain with a history of trauma, (2) significant multiple system trauma, (3) severe head or facial trauma, (4) numbness or weakness in any extremity after trauma, (5) loss of consciousness caused by trauma, (5) If the mental status is altered (including drugs, alcohol, trauma) and no history is available, or the patient is found in a setting of possible trauma (e.g., lying at the bottom of stairs or in the street); or the patient experienced near-drowning with a history or probability of diving, and (6) any significant distracting injury.
Gather et al. [22] reported that the overwhelming majority of German national level I trauma centers (around 98%) immobilize the cervical spine using a cervical collar.
The general recommendations for cervical immobilization are: all patients with suspected SCI should be immobilized, and patient triage on the scene should be performed by trained emergency medical personnel. In patients with no signs of cervical trauma, immobilization is generally not recommended. Spinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitation. The cervical collar should not be removed before a neurologic assessment of the cervical spine, including palpation with voluntary movement in all planes, have been performed and found to be not related to injury [14]. Patients should be immobilized with a combination of a rigid cervical collar and supportive blocks on a backboard with straps [14].
2) Patient transportation
Transportation of a patient with suspected cervical trauma can be a genuinely challenging task. The EMS has various medical devices like the long spine board, vacuum mattress, soft stretcher, trauma mattress, and the Pharaoh mattress. The advantages and disadvantages of one over another continue to be a topic of debate [22,23].
The ATLS, PHTLS, and AANS/CNS guidelines recommend using the spine board with supportive blocks and straps as an effective patient transportation method. Immobilization with sandbags and tape is not recommended [15-17].
Although the dangers of excessive spinal motion have been well researched, prolonged immobilization of patients on a spine board can be hazardous, causing severe pain and discomfort in conscious patients, possible severe decubitus ulcers, and respiratory compromise. It is recommended that long spine boards be used only during patient transportation, and every effort should be made to remove patients from spine boards without unnecessary delay [15].
Nolte et al. [24] conducted a biomechanical analysis of immobilization techniques performed in a standardized setting. The authors’ primary analysis endpoint was the cervical range of motion of a participant immobilized using a spine board with or without a cervical collar, a vacuum mattress with or without a cervical collar, and a minimal immobilization technique using an ambulance cot and pillows. The vacuum mattress was analyzed in 2 settings -straight and inclined (30°). Nolte et al. [24] concluded that the best spinal motion restriction during transportation is achieved using the spine board, and it should be used if the distance to the trauma center is short. The patient is better transported on a vacuum mattress with a cervical collar and head blocks to avoid pain and possible ulcers when longer. If the patient is suspected of having TBI, the vacuum mattress should be elevated to 30°, and cervical collar should be avoided. Minimal immobilization is recommended only if the patient is unstable (e.g., shock) [24].
Similar data were reported by Rahmatalla et al. [25] noting the long spine board and vacuum matters combined with the cervical collar as the most effective.
Gather et al. [22] performed a survey-based analysis of currently used spinal immobilization in 107 level I trauma centers in Germany. Approximately 39% of the time, patients in the acute phase were transferred to a soft stretcher. The transfer was most often done using the log-roll technique with the aid of a sliding or rolling board. However, this could cause significant movement of the spine. The use of the recommended lift-and-slide method is, however, much more difficult. The respondents rated the soft stretcher as the worst spinal immobilization device [22]. Respondents were most satisfied with the use of a spine board. As described in the literature, the disadvantages of using the spine board did not justify ruling it out in the initial phase of acute treatment. It must be ensured that the patient's time-consuming immobilization on the spine board does not lead to relevant delays in subsequent diagnostics and therapy [22].
The general recommendations for patient transportation are using a long spine board as the most effective method of restricting spinal motion during transportation.
A group of German authors have produced a spinal immobilization protocol in adult trauma patients and searched for its applicability in emergency care providers [26]. They have called it the Emergency Medicine Spinal Immobilization Protocol (E.M.S. IMMO Protocol) (Fig. 2).
Fig. 2.
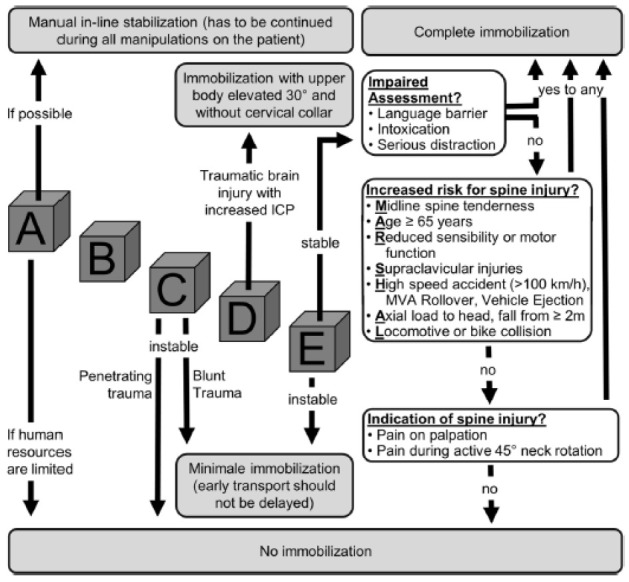
Emergency Medicine Spinal Immobilization Protocol (E.M.S. IMMO Protocol). Reprinted from Kreinest et al. Scand J Trauma Resusc Emerg Med 2016;24:71, under the terms of Open Access [26].
Prehospital immobilization in children with potential acute SCI can show significant variability. Kim et al. [27] have investigated the type of immobilization in children in different age groups. They reported that full spinal immobilization could be applied to older children more uniformly. It was not that easy at younger ages, and one-quarter of the children younger than 2 years were not immobilized at all.
5. Early Reduction of Cervical Spinal Dislocations
Dislocation of cervical facets after trauma commonly cause spinal canal narrowing and neurologic deficits [28]. The incidence of neurological deficits is higher if there is bilateral facet dislocation [29,30]. The most common levels of dislocation are C5–6 and C6–7 [31,32]. If the reduction and decompression of the spinal canal are not provided, ischemia, edema, and production of free radicals will cause secondary injury resulting in permanent deficits of the patient [33,34].
There is no doubt that immobilization of the cervical spine must be provided as soon as possible, as well as normal alignment must be provided either with closed or open (surgical) reduction techniques.
Closed reduction of the cervical spine using head traction has been used for many years and reported as an effective treatment for many cervical facet dislocations [33,35]. Closed reduction using skull tongs can cause a spinal cord decompression and achieve a normal alignment of the spine [36]. There are also some reports that if the reduction is achieved early enough, the neurological improvement will be more [37].
However, many papers report that closed reduction attempts cannot be successful in all cases. Besides, even after a closed reduction, open surgery with stabilization of the dislocated level is necessary. Since closed reduction requires close neurologic monitoring, imaging to monitor progress is not always feasible [36]. Some surgeons prefer to make an open reduction and stabilization surgery at the same sitting for those reasons. There is still a controversy about performing a closed reduction compared with open surgical reduction and fixation [38].
Reduction after cervical trauma is necessary in case of dislocated facets. Two techniques can achieve it:
1) Closed reduction
It should better be done under fluoroscopy in the operating room by an experienced spine surgeon. Patient relaxation is recommended. Obtunded patients and patients having problems communicating should better not go to closed reduction. Closed reduction should be performed as early as possible. Most surgeons perform a closed reduction just before the surgery.
Closed reduction using axial traction with tongs may have 2 consequences: If the reduction occurs with lower weights, it means the facets are fractured, and good alignment will be achieved easily. However, if too many weights are necessary, a reduction is severe, we must predict for locked facets, at least one facet is locked (Fig. 3). If the trauma is not acute, the closed reduction is also difficult.
Fig. 3.
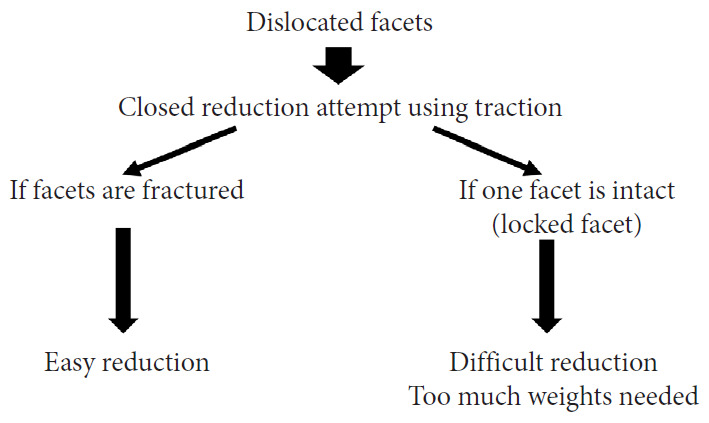
Cervical traction and condition of the facets.
2) Open reduction
Some surgeons prefer it as the first procedure. Some others apply an open reduction in case a closed reduction is not possible. Then a decision for 2 options must be made: anterior or posterior reduction and fixation.
In acute trauma cases, immediate anterior decompression is preferred by most spine surgeons. An anterior open reduction with a distractor is performed. Caspar vertebral body pins and distractor is a useful adjunct at this point. The reduction can be achieved with this technique in most of the locked facets. If an anterior open reduction may not be achieved in rare instances, a posterior open reduction must be followed.
If the surgeon prefers primary open posterior reduction, a preoperative magnetic resonance imaging (MRI) is necessary to exclude herniated disc material.
3) Closed vs. open reduction
The decision to perform an open or closed reduction is mostly dependent on 2 factors [38].
(1) Safety
Patient monitoring during a closed reduction process is necessary, since overtraction or other pathologies may cause further neurologic deficits. After a closed reduction in awake patients, the incidence of permanent neurological complications is approximately 1%, transient injury 2%–4% [28].
Closed reduction in an awake and alert patient can be considered as a safe procedure. A closed reduction attempt is not safe in an obtunded or intubated patient. The case report by Eismont et al. [39] suggests that closed reduction is unsafe in a patient with a decreased conscious level.
Prereduction MRI has been recommended by some authors to exclude a significant anterior space-occupying lesion. However, the exact definition of a critical anterior mass or disc fragment is lacking. Besides, performing a magnetic resonance image in an acute cervical trauma patient after a computed tomography (CT) scan may not be feasible in an emergency setting. Moreover, multiple transfers of the patient in radiology departments without skull traction may cause more risks.
If a closed reduction fails, it should be followed with an open reduction. An open reduction with or without a decompression should be considered. If the surgeon's choice is a posterior open reduction, it should better be done after an MRI is obtained.
(2) Feasibility of a closed reduction
The CT scans can nicely show if there are fracture(s) of facets and the facets' locked position. As mentioned before, closed reduction will be difficult, even impossible in case of at least one locked facet and no fracture. In fact, closed reduction in facet dislocations has been successful in approximately 50% of the patients [40,41].
There have been 2 recommendation efforts for closed reduction of cervical dislocations. One of them is the “Guidelines of Joint Section on Disorders of the Spine and Peripheral Nerves of AANS and CNS” and published in 2013 [28]. They recommend an early closed reduction of cervical spinal fracture-dislocations with traction. But, for the patients with an additional rostral injury, closed reduction should not be applied. In case the patient’s mental status is altered or if the closed reduction has failed, before any open surgical reduction MRI is recommended.
The other recommendations come from the “Spine Section of the German Society for Orthopedics and Trauma” and published in 2018 [42]. They have defined the treatment option of cervical spine injuries according to AOSpine classification [43]. Facet injuries have 4 grades. F4-Injuries (Subluxation or Perched/Dislocated Facet) also contain unilateral or bilateral locked facets that require a safe reduction without neurological deficits. They also recommend a closed reduction under fluoroscopy by an experienced spine surgeon in the operating room as early as possible. Patient relaxation can facilitate reduction. In case a closed reduction cannot be achieved, immediate anterior decompression and an open reduction attempt with a distractor should be done. If an anterior open reduction is not successful, it must be followed by an open posterior approach. If the surgeon's preference is to make an open dorsal reduction, a preoperative MRI must be taken to see if there is a herniated disc [42].
(3) Publications defending closed reduction
In a retrospective study [41] examining 15 patients with a cervical fracture-dislocation performing immediate closed reduction without obtaining a prereduction MRI, there were 6 failures (43%) that have gone open surgical reduction and stabilization. They have done 3 anterior only, 3 posterior only, and 9 combined anteriorposterior approaches after reduction attempts. They report that in 57% of patients placed in traction, the reduction was possible.
In another retrospective study involving 110 cases with facet fractures [40], closed reduction after analgesic and anxiolytic medications were attempted. Lateral radiographs were taken with every increment of weight, starting with 4.5 kg. In awake patients, they have monitored physical examinations; in obtunded patients, they have monitored somatosensory evoked potentials (SEPs).
Increments were increased until a maximum of 23 kg of traction. If 50 lb failed, they have transitioned to open reduction. In cases with facet fractures without jumped facets (65 cases, 60%), they have not attempted a closed reduction. The authors report that the rate of successful closed reduction was significantly higher in incomplete motor deficits (5 of 5) than complete motor deficits (2 of 11). They have concluded that closed reduction should be attempted in patients with good motor examinations; however, those with significant deficits may benefit from earlier surgical intervention [40].
Miao et al. [44] have preferred closed reduction under general anesthesia with monitoring and fluoroscopic guidance in 24 patients; 16 unilateral, 8 bilateral facet dislocation. They have started with 5-kg weight, increased at a rate of 1 kg per 10 minutes until they reach a maximum of 15 kg. Then, they have done an immediate anterior and posterior stabilization.
A report from Stoke Mandeville Hospital in the United Kingdom [45] has used the so-called rapid incremental closed traction reduction for cervical facet dislocation and SCI patients. Among 16 patients, the success rate of the closed reduction was about 44%.
Some surgeons have used different closed reduction techniques. A study by Wang et al. [46] describing a reduction technique for treating unilateral locked facets is using a Z-shape elevatingpulling reduction through a halo-vest and awake condition. After reduction, only anterior cervical decompression and internal fixation were performed. The same authors have then performed a multicenter study in 63 patients with locked facets [47]. Z-shape elevating-pulling reduction (n = 20) or traditional skull traction reduction (n = 43). The success rates were significantly better in the Z-shape elevating group (87.5%) than in the skull traction group (35.3%) for unilateral locked facet reduction.
(4) Publications defending open reduction
Gattozzi et al. [48] have used early ventral surgery without traction in all cases with facet dislocation. In 36 patients who have gone early (24 hours) surgery, traction was done after anesthesia induction, then under fluoroscopy, if not reduced, a Cobb elevator placed in disc space used for anterior open reduction. Then, an anterior graft and plate were placed.
Zhou et al. [49] have reported 2 cases that unilateral locked facets could not be reduced by closed traction, and they have done a posterior, anterior surgery.
Shimizu et al. [50] have described a method to reduce the unilateral locked facet by a percutaneous technique under fluoroscopy, then immediate anterior fusion and plating. This approach’s aim was explained to save the extensive posterior muscle dissection and reduce postoperative axial pain.
Another issue is the success rate of closed reduction, which has been reported approximately 50% [40,41,45]. In a meta-analysis by Kepler et al. [51] for cervical facet fractures involving 11 studies and 368 patients, closed reduction was successful in 56.4% of patients. However, an open reduction was successful in 94.9% of patients. Anterior versus posterior surgery success rates were also compared, and anterior approaches had a 90.5% rate of maintenance of reduction, while it was 75.6% rate for the posterior approach.
An algorithm for the surgeon’s choice of closed or open reduction options is given in Fig. 4.
Fig. 4.
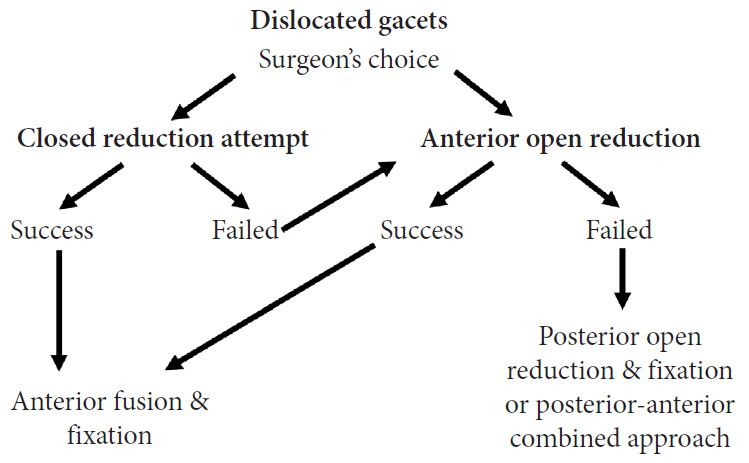
An algorithm for the surgeon’s choice of closed or open reduction options.
CONCLUSION
Traumatic spinal injury is a major source of morbidity and mortality throughout the world. It is estimated that 780,000 people have a traumatic spinal injury each year. Compared with high-income countries, the proportion of patients with a traumatic spinal injury with SCI is higher in low-and-middle-income countries. Partly preventable mechanisms, including road traffic accidents and falls, are the leading causes of traumatic spinal injury globally.
The optimal technique for immobilizing and transporting patients with cervical spine trauma continues to be a problem. Although there is a tendency in current literature to question the traditional methods, they are an effective and time-tested practice to prevent secondary SCI. They are supported by years of cumulative clinical experience. The practice of using a cervical collar and long spine board is effective and offers the best motion restriction, but should be used only when indicated and not routinely. All the benefits and risks of immobilization should be considered in every individual situation.
RECOMMENDATIONS
Recommendations for Epidemiology of Spinal Trauma
*Global incidence of traumatic spinal injury is 10.5 cases per 100,000 persons in new cases annually. The incidence is higher in low- and middle-income countries. The most frequent reasons are road traffic accidents and falls.
*The incidence of traumatic SCI from land transport increases in low-income countries due to transition to motorized transport, inadequate infrastructure, and regulatory challenges.
*The incidence from low falls in the elderly is increasing in high-income countries due to ageing populations.
Recommendations for Prevention of Spine Trauma
*The best intervention for the prevention of SCI associated with road traffic crashes comprise:
• Legislating and enforcing drink-driving laws (including a blood alcohol concentration limit of 0.05 g/dL for all road users
• Use of head restraints
• Use of seat-belts and use of child passenger restraints
• Setting and enforcing speed limits
*The best intervention for preventing SCI associated with road traffic crashes of 2-wheelers comprises:
• Motorcycle helmets
• Daytime running lights for motorcycles
• Road designs that separate pedestrians and two-wheelers from cars and heavier vehicles. Area-wide traffic calming measures
• Graduated driver licensing systems
*The prevention of SCI related to falls comprise the following interventions:
• Floor clear of clutter and loose rugs, provision of good lighting, hand-rails and appropriate level furniture, window guards in high-rise buildings, barriers on roofs
• Safe harvest equipment. Use wheelbarrows instead of carrying loads on the head.
*The prevention of SCI related to sports injuries comprise the following interventions:
• Mandatory safety training for coaches and referees
• Legislation and enforcement of safe pool design, e.g., depth, lighting, diving board height, and elasticity, prohibiting use of alcohol around water sports.
• Playground standards for the depth of appropriate surface material, the height of equipment, and maintenance
• Early access to decompression chambers
Recommendations for Transportation and Immobilization of Patients With Cervical Spine Trauma
*Immobilization patients over the age of 12 years with high-risk SCI during the prehospital setting should include a hardcervical collar, spinal backboard with tape/straps to immobilize the entire patient
*In case of limited human resources, alert patients with minimal blunt trauma without penetrating trauma and any spinal pain can be transported without immobilization
*Transport of patients with acute traumatic SCI to the definitive hospital center for SCI care should occur as soon as possible and not later than 24 hours of injury
*After arriving to the hospital, collar immobilization may be discontinued in the alert asymptomatic patients, following normal MRI obtained within 48 hours of injury. Dynamic x-ray can be excluded from the list of options for investigation. In the obtunded patient, collar immobilization may be discontinued after a negative high-quality C-spine CT scan. Symptomatic patients with normal CT scans should proceed to MRI.
*There is a big variability in spinal immobilization of children. Children younger than 2 years have more difficulties for immobilization. There is no consensus if the children should have different immobilization measures.
Recommendations for Closed Reduction of Cervical Dislocations
*There is no evidence that closed reduction of cervical locked facets has more benefits to open reduction.
*If a closed reduction is attempted, awake patients with incomplete injuries are better candidates.
*If a reduction in patients with decreased consciousness is attempted, prereduction MRI and open reduction should be preferred.
*If a closed reduction attempt fails, immediate anterior decompression and surgical reduction are better options.
*Best time for a closed reduction is not well known, although most papers suggest it should be as soon as possible.
*All patients after closed reduction should be operated for stabilization and fusion. This surgery can be with an anterior, posterior or combined anterior and posterior approach.
REFERENCES
- 1.Maschmann C, Jeppesen E, Rubin MA, et al. New clinical guidelines on the spinal stabilisation of adult trauma patients - consensus and evidence based. Scand J Trauma Resusc Emerg Med. 2019;27:77. doi: 10.1186/s13049-019-0655-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ning GZ, Wu Q, Li YL, et al. Epidemiology of traumatic spinal cord injury in Asia: a systematic review. J Spinal Cord Med. 2012;35:229–39. doi: 10.1179/2045772312Y.0000000021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kumar R, Lim J, Mekary RA, et al. Traumatic spinal injury: global epidemiology and worldwide volume. World Neurosurg. 2018;113:e345–63. doi: 10.1016/j.wneu.2018.02.033. [DOI] [PubMed] [Google Scholar]
- 4.Milby AH, Halpern CH, Guo W, et al. Prevalence of cervical spinal injury in trauma. Neurosurg Focus. 2008;25:E10. doi: 10.3171/FOC.2008.25.11.E10. [DOI] [PubMed] [Google Scholar]
- 5.Fredø HL, Rizvi SA, Lied B, et al. The epidemiology of traumatic cervical spine fractures: a prospective population study from Norway. Scand J Trauma Resusc Emerg Med. 2012;20:85. doi: 10.1186/1757-7241-20-85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wyndaele M, Wyndaele JJ. Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord. 2006;44:523–9. doi: 10.1038/sj.sc.3101893. [DOI] [PubMed] [Google Scholar]
- 7.O’Connor PJ. Forecasting of spinal cord injury annual case numbers in Australia. Arch Phys Med Rehabil. 2005;86:48–51. doi: 10.1016/j.apmr.2004.07.346. [DOI] [PubMed] [Google Scholar]
- 8.Clayton JL, Harris MB, Weintraub SL, et al. Risk factors for cervical spine injury. Injury. 2012;43:431–5. doi: 10.1016/j.injury.2011.06.022. [DOI] [PubMed] [Google Scholar]
- 9.Prevenntion of spinal cord injury . World Health Organization, The International Spinal Cord Society. International perspesctives on spinal cord injury. Geneva (Switzerland): World Health Organization; 2013. pp. 43–59. [Google Scholar]
- 10.Lukins TR, Ferch R, Balogh ZJ, et al. Cervical spine immobilization following blunt trauma: a systematic review of recent literature and proposed treatment algorithm. ANZ J Surg. 2015;85:917–22. doi: 10.1111/ans.13221. [DOI] [PubMed] [Google Scholar]
- 11.Sundstrøm T, Asbjørnsen H, Habiba S, et al. Prehospital use of cervical collars in trauma patients: a critical review. J Neurotrauma. 2014;31:531–40. doi: 10.1089/neu.2013.3094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kreinest M, Goller S, Rauch G, et al. Application of cervical collars - an analysis of practical skills of professional emergency medical care providers. PLoS One. 2015;10:e0143409. doi: 10.1371/journal.pone.0143409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Velopulos CG, Shihab HM, Lottenberg L, et al. Prehospital spine immobilization/spinal motion restriction in penetrating trauma: a practice management guideline from the Eastern Association for the Surgery of Trauma (EAST) J Trauma Acute Care Surg. 2018;84:736–44. doi: 10.1097/TA.0000000000001764. [DOI] [PubMed] [Google Scholar]
- 14.Theodore N, Hadley MN, Aarabi B, et al. Prehospital cervical spinal immobilization after trauma. Neurosurgery. 2013;72 Suppl 2:22–34. doi: 10.1227/NEU.0b013e318276edb1. [DOI] [PubMed] [Google Scholar]
- 15.ATLS Subcommittee; American College of Surgeons’ Committee on Trauma. International ATLS working group Advanced trauma life support (ATLS®): the ninth edition. J Trauma Acute Care Surg. 2013;74:1363–6. doi: 10.1097/TA.0b013e31828b82f5. [DOI] [PubMed] [Google Scholar]
- 16.National Association of Emergency Medical Technicians (U.S.) Prehospital Trauma Life Support Committee, A.C.o.S. C.o.T., Prehospital Trauma Life Support (PHTLS(R)) Prehospital trauma life support. St. Louis (MO): Mosby Jems/Elsevier; 2007. [Google Scholar]
- 17.Walters BC, Hadley MN, Hurlbert RJ, et al. Guidelines for the management of acute cervical spine and spinal cord injuries: 2013 update. Neurosurgery. 2013;60(CN_suppl_1):82–91. doi: 10.1227/01.neu.0000430319.32247.7f. [DOI] [PubMed] [Google Scholar]
- 18.Stiell IG, Clement CM, O'Connor A, et al. Multicentre prospective validation of use of the Canadian C-Spine Rule by triage nurses in the emergency department. CMAJ. 2010;182:1173–9. doi: 10.1503/cmaj.091430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chendrasekhar A, Moorman DW, Timberlake GA. An evaluation of the effects of semirigid cervical collars in patients with severe closed head injury. Am Surg. 1998;64:604–6. [PubMed] [Google Scholar]
- 20.Kolb JC, Summers RL, Galli RL. Cervical collar-induced changes in intracranial pressure. Am J Emerg Med. 1999;17:135–7. doi: 10.1016/s0735-6757(99)90044-x. [DOI] [PubMed] [Google Scholar]
- 21.Nakanishi T, Mitra B, Ackland H, et al. Time in collars and collar-related complications in older patients. World Neurosurg. 2019;129:e478–84. doi: 10.1016/j.wneu.2019.05.187. [DOI] [PubMed] [Google Scholar]
- 22.Gather A, Spancken E, Münzberg M, et al. Spinal immobilization in the trauma room - a survey-based analysis at german level I trauma centers. Z Orthop Unfall. 2020;158:597–603. doi: 10.1055/a-1007-2092. [DOI] [PubMed] [Google Scholar]
- 23.Holla M, Hannink G, Eggen TGE, et al. Restriction of cervical intervertebral movement with different types of external immobilizers: a cadaveric 3D analysis study. Spine (Phila Pa 1976) 2017;42:E1182–9. doi: 10.1097/BRS.0000000000002107. [DOI] [PubMed] [Google Scholar]
- 24.Nolte PC, Uzun DD, Häske D, et al. Analysis of cervical spine immobilization during patient transport in emergency medical services. Eur J Trauma Emerg Surg. 2019 Apr 27; doi: 10.1007/s00068-019-01143-z. [Epub]. [DOI] [PubMed] [Google Scholar]
- 25.Rahmatalla S, DeShaw J, Stilley J, et al. Comparing the efficacy of methods for immobilizing the cervical spine. Spine (Phila Pa 1976) 2019;44:32–40. doi: 10.1097/BRS.0000000000002749. [DOI] [PubMed] [Google Scholar]
- 26.Kreinest M, Gliwitzky B, Schüler S, et al. Development of a new Emergency Medicine Spinal Immobilization Protocol for trauma patients and a test of applicability by German emergency care providers. Scand J Trauma Resusc Emerg Med. 2016;24:71. doi: 10.1186/s13049-016-0267-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kim EG, Brown KM, Leonard JC, et al. Variability of prehospital spinal immobilization in children at risk for cervical spine injury. Pediatr Emerg Care. 2013;29:413–8. doi: 10.1097/PEC.0b013e318289d743. [DOI] [PubMed] [Google Scholar]
- 28.Gelb DE, Hadley MN, Aarabi B, et al. Initial closed reduction of cervical spinal fracture-dislocation injuries. Neurosurgery. 2013;72 Suppl 2:73–83. doi: 10.1227/NEU.0b013e318276ee02. [DOI] [PubMed] [Google Scholar]
- 29.Ellenbogen RG, Abdulrauf SI, Sekhar LN. Principles of neurological surgery. 3rd ed. Philadelphia (PA): Elsevier/Saunders; 2012. [Google Scholar]
- 30.Hadley MN, Fitzpatrick BC, Sonntag VK, et al. Facet fracture-dislocation injuries of the cervical spine. Neurosurgery. 1992;30:661–6. [PubMed] [Google Scholar]
- 31.Goldberg W, Mueller C, Panacek E, et al. Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med. 2001;38:17–21. doi: 10.1067/mem.2001.116150. [DOI] [PubMed] [Google Scholar]
- 32.Greenbaum J, Walters N, Levy PD. An evidenced-based approach to radiographic assessment of cervical spine injuries in the emergency department. J Emerg Med. 2009;36:64–71. doi: 10.1016/j.jemermed.2008.01.014. [DOI] [PubMed] [Google Scholar]
- 33.Newton D, England M, Doll H, et al. The case for early treatment of dislocations of the cervical spine with cord involvement sustained playing rugby. J Bone Joint Surg Br. 2011;93:1646–52. doi: 10.1302/0301-620X.93B12.27048. [DOI] [PubMed] [Google Scholar]
- 34.Rowland JW, Hawryluk GW, Kwon B, et al. Current status of acute spinal cord injury pathophysiology and emerging therapies: promise on the horizon. Neurosurg Focus. 2008;25:E2. doi: 10.3171/FOC.2008.25.11.E2. [DOI] [PubMed] [Google Scholar]
- 35.Aarabi B, Mirvis S, Shanmuganathan K, et al. Comparative effectiveness of surgical versus nonoperative management of unilateral, nondisplaced, subaxial cervical spine facet fractures without evidence of spinal cord injury: clinical article. J Neurosurg Spine. 2014;20:270–7. doi: 10.3171/2013.11.SPINE13733. [DOI] [PubMed] [Google Scholar]
- 36.Khezri N, Ailon T, Kwon BK. Treatment of facet injuries in the cervical spine. Neurosurg Clin N Am. 2017;28:125–37. doi: 10.1016/j.nec.2016.07.005. [DOI] [PubMed] [Google Scholar]
- 37.Cotler JM, Herbison GJ, Nasuti JF, et al. Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine (Phila Pa 1976) 1993;18:386–90. doi: 10.1097/00007632-199303000-00015. [DOI] [PubMed] [Google Scholar]
- 38.Lee JY, Nassr A, Eck JC, et al. Controversies in the treatment of cervical spine dislocations. Spine J. 2009;9:418–23. doi: 10.1016/j.spinee.2009.01.005. [DOI] [PubMed] [Google Scholar]
- 39.Eismont FJ, Arena MJ, Green BA. Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. Case report. J Bone Joint Surg Am. 1991;73:1555–60. [PubMed] [Google Scholar]
- 40.Branche MJ, Ozturk AK, Ramayya AG, et al. Neurologic status on presentation as predictive measurement in success of closed reduction in traumatic cervical facet fractures. World Neurosurg. 2018;114:e344–9. doi: 10.1016/j.wneu.2018.03.001. [DOI] [PubMed] [Google Scholar]
- 41.Sribnick EA, Hoh DJ, Dhall SS. Traumatic high-grade cervical dislocation: treatment strategies and outcomes. World Neurosurg. 2014;82:1374–9. doi: 10.1016/j.wneu.2014.02.008. [DOI] [PubMed] [Google Scholar]
- 42.Schleicher P, Kobbe P, Kandziora F, et al. Treatment of injuries to the subaxial cervical spine: recommendations of the spine section of the German Society for Orthopaedics and Trauma (DGOU) Global Spine J. 2018;8(2 Suppl):25S–33S. doi: 10.1177/2192568217745062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Vaccaro AR, Koerner JD, Radcliff KE, et al. AOSpine subaxial cervical spine injury classification system. Eur Spine J. 2016;25:2173–84. doi: 10.1007/s00586-015-3831-3. [DOI] [PubMed] [Google Scholar]
- 44.Miao DC, Wang F, Shen Y. Immediate reduction under general anesthesia and combined anterior and posterior fusion in the treatment of distraction-flexion injury in the lower cervical spine. J Orthop Surg Res. 2018;13:126. doi: 10.1186/s13018-018-0842-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Ahmed WA, Naidoo A, Belci M. Rapid incremental closed traction reduction of cervical facet fracture dislocation: the Stoke Mandeville experience. Spinal Cord Ser Cases. 2018;4:86. doi: 10.1038/s41394-018-0109-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Wang X, Yao G, Chen Y, et al. New reduction technique for the treatment of unilateral locked facet joints of the lower cervical spine: a retrospective analysis of 12 cases. Orthopade. 2018;47:212–20. doi: 10.1007/s00132-017-3456-9. [DOI] [PubMed] [Google Scholar]
- 47.Wang X, An W, Wu Q, et al. Multicentre comparative study of Z-shape elevating-pulling reduction and skull traction reduction for treatment of lower cervical locked facets. Int Orthop. 2019;43:1255–62. doi: 10.1007/s00264-018-4041-5. [DOI] [PubMed] [Google Scholar]
- 48.Gattozzi DA, Yekzaman BR, Jack MM, et al. Early ventral surgical treatment without traction of acute traumatic subaxial cervical spine injuries. Surg Neurol Int. 2018;9:254. doi: 10.4103/sni.sni_352_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Zhou Y, Zhou Z, Liu L, et al. Management of irreducible unilateral facet joint dislocations in subaxial cervical spine: two case reports and a review of the literature. J Med Case Rep. 2018;12:74. doi: 10.1186/s13256-018-1609-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Shimizu T, Yoshioka K, Murakami H, et al. Fluoroscopy-assisted posterior percutaneous reduction for the management of unilateral cervical facet dislocations after unsuccessful closed reduction: a case report. Int J Surg Case Rep. 2019;58:212–5. doi: 10.1016/j.ijscr.2019.04.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kepler CK, Vaccaro AR, Chen E, et al. Treatment of isolated cervical facet fractures: a systematic review. J Neurosurg Spine. 2016;24:347–54. doi: 10.3171/2015.6.SPINE141260. [DOI] [PubMed] [Google Scholar]
- 52.Haddon W., Jr Advances in the epidemiology of injuries as a basis for public policy. Public Health Rep. 1980;95:411–21. [PMC free article] [PubMed] [Google Scholar]