

This cohort study identifies patient characteristics associated with use of parathyroidectomy for the management of primary hyperparathyroidism in older adults.
Key Points
Question
What patient characteristics are associated with the use of parathyroidectomy for the treatment of older adults with primary hyperparathyroidism (PHPT)?
Findings
In this population-based cohort study of 210 206 Medicare beneficiaries diagnosed with PHPT from 2006 to 2016, 30.0% of patients were treated with parathyroidectomy. Increasing age, comorbidity, and frailty were associated with decreased odds of parathyroidectomy.
Meaning
These findings suggest that most older adults with PHPT do not receive definitive treatment with parathyroidectomy, with age, multimorbidity, and frailty influencing treatment decisions more than consensus guidelines; further research should identify barriers to appropriate surgical cure and develop tools to target parathyroidectomy to older adults most likely to benefit.
Abstract
Importance
Parathyroidectomy provides definitive management for primary hyperparathyroidism (PHPT), reducing the risk of subsequent fracture, nephrolithiasis, and chronic kidney disease (CKD), but its use among older adults in the US is unknown.
Objective
To identify patient characteristics associated with the use of parathyroidectomy for the management of PHPT in older adults.
Design, Setting, and Participants
This population-based, retrospective cohort study used 100% Medicare claims from beneficiaries with an initial diagnosis of PHPT from January 1, 2006, to December 31, 2016. Patients were considered to meet consensus guideline criteria for parathyroidectomy based on diagnosis codes indicating osteoporosis, nephrolithiasis, or stage 3 CKD. Multivariable logistic regression was used to identify patient characteristics associated with parathyroidectomy. Data were analyzed from February 11, 2020, to October 8, 2020.
Main Outcomes and Measures
The primary outcome was parathyroidectomy within 1 year of diagnosis.
Results
Among 210 206 beneficiaries with an incident diagnosis of PHPT (78.8% women; mean [SD] age, 75.3 [6.8] years), 63 136 (30.0%) underwent parathyroidectomy within 1 year of diagnosis. Among the subset of patients who met consensus guideline criteria for operative management (n = 131 723), 38 983 (29.6%) were treated with parathyroidectomy. Patients treated operatively were younger (mean [SD] age, 73.5 [5.7] vs 76.0 [7.1] years) and more likely to be White (90.1% vs 86.0%), to be robust or prefrail (92.1% vs 85.7%), and to have fewer comorbidities (Charlson Comorbidity Index score of 0 or 1, 54.6% vs 44.1%), in addition to being more likely to live in socioeconomically disadvantaged (46.9% vs 40.3%) and rural (18.1% vs 13.6%) areas (all P < .001). On multivariable analysis, increasing age had a strong inverse association with parathyroidectomy among patients aged 76 to 85 years (unadjusted rate, 25.9%; odds ratio [OR], 0.68 [95% CI, 0.67-0.70]) and older than 85 years (unadjusted rate, 11.2%; OR, 0.27 [95% CI, 0.26-0.29]) compared with those aged 66 to 75 years (unadjusted rate, 35.6%), as did patients with moderate to severe frailty (unadjusted rate, 18.9%; OR, 0.60 [95% CI, 0.56-0.64]) compared with robust patients (unadjusted rate, 36.1%) and those with a Charlson Comorbidity Index score of 2 or greater (unadjusted rate, 25.9%; OR, 0.77 [95% CI, 0.75-0.79]) compared with a Charlson Comorbidity Index score of 0 (unadjusted rate, 37.0%). With regard to operative guidelines, a history of nephrolithiasis increased the odds of parathyroidectomy (OR, 1.43 [95% CI, 1.39-1.47]); stage 3 CKD decreased the odds of parathyroidectomy (OR, 0.71 [95% CI, 0.68-0.74]); and osteoporosis showed no association (OR, 1.01 [95% CI, 0.99-1.03]).
Conclusions and Relevance
In this cohort study, most older adults with PHPT did not receive definitive treatment with parathyroidectomy. Older age, frailty, and multimorbidity were associated with nonoperative management, and guideline recommendations had minimal effect on treatment decisions. Further research is needed to identify barriers to surgical care and develop tools to target parathyroidectomy to older adults most likely to benefit.
Introduction
Primary hyperparathyroidism (PHPT) is a common endocrine disorder that has tripled in prevalence in the past 20 years and primarily affects those 65 years and older.1 Primary hyperparathyroidism is associated with an increased risk of osteoporotic fractures,2 nephrolithiasis,3 and chronic kidney disease (CKD),4 in addition to neurocognitive impairment5 and cardiovascular disease.6 Parathyroidectomy is the only definitive treatment for PHPT. Evidence-based criteria for the operative management of PHPT have expanded significantly since the first consensus guidelines were published in 1991.7 However, despite more inclusive surgical guidelines and evidence that operative cure results in benefits across multiple dimensions, including a reduced risk of fractures2 and symptomatic nephrolithiasis3 and improved quality of life,5,8 rates of parathyroidectomy for the management of PHPT are low and have been declining over time.9,10
Older adults have a higher absolute risk of morbidity from fractures, nephrolithiasis, and CKD, which suggests they have the greatest potential to benefit from parathyroidectomy in the management of PHPT. However, small studies11,12 suggest that increasing age is independently associated with delays in surgical referral and decreased likelihood of parathyroidectomy, regardless of the severity of disease or whether consensus guideline criteria are met. Multimorbidity further reduces the odds of surgical management, suggesting nonoperative management is favored owing to concern that the operative risk of older patients with comorbid conditions outweighs any potential benefit.10 However, no population-based, national data are available that describe the management of PHPT among older adults in the US, limiting our ability to identify barriers to definitive treatment.
To better understand factors influencing treatment decisions for older adults with PHPT, this study evaluated patient characteristics associated with parathyroidectomy in the management of all Medicare beneficiaries diagnosed with PHPT from 2006 to 2016. We hypothesized that increasing patient age, frailty, and comorbidity burden would be inversely associated with parathyroidectomy and that meeting consensus criteria would have minimal influence on surgical decision-making for PHPT.
Methods
Data Source
We performed a retrospective cohort study of all beneficiaries with an incident diagnosis of PHPT within 100% of Medicare fee-for-service claims from January 1, 2006, to December 31, 2016. The study population was identified using outpatient claims, carrier claims, and Medicare Payment Advisory Commission and Master Beneficiary Summary files. Claims and enrollment data were accessed through the Virtual Research Data Center housed on a secure Centers for Medicare & Medicaid Services server. The institutional review board at Stanford University, Stanford, California, approved this study and waived the need for informed consent owing to research involving minimal risk to participants that could not be carried out practicably without the waiver. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Population
We identified a cohort of patients older than 65 years with a first diagnosis of PHPT based on International Classification of Diseases, Ninth Revision (ICD-9) or International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10), diagnosis codes for PHPT (252.01 and E21.0) on any claim during the study period. Beneficiaries were excluded if they had a history of stage 4 or 5 CKD, were receiving dialysis, or had a history of kidney transplant to prevent inclusion of patients with possible secondary or tertiary hyperparathyroidism (n = 63 782). We also excluded patients who had undergone prior parathyroidectomy (n = 4047), those with missing demographic information (age, sex, or race/ethnicity [n = 7641]), and those with mailing zip codes unavailable in US Census or Area Deprivation Index (ADI) data (n = 1532), including those with primary mailing addresses outside the US (Figure 1). Patients were required to have at least 12 months of continuous Medicare Part A and B enrollment (without Part C Medicare Advantage enrollment) before and after PHPT diagnosis (n = 41 387 excluded) to allow adequate time to identify preexisting medical comorbidities and preexisting diagnosis of PHPT and to observe the rate of initial operative management with comprehensive claims data.
Figure 1. Cohort Enrollment Criteria.

CKD indicates chronic kidney disease; ICD-9/10, International Classification of Diseases, Ninth Revision/International Statistical Classification of Diseases and Related Health Problems, Tenth Revision; PHPT, primary hyperparathyroidism.
aThe sum of subcategory totals exceeds the number of total exclusions because some patients met multiple exclusion criteria.
bPatients were excluded if age, sex, race/ethnicity, Area Deprivation Index, or urban or rural inhabitance were unknown.
Covariates
Patient characteristics collected included age, sex, and race/ethnicity. Patient comorbidity was assessed using the Charlson Deyo Comorbidity Index.13,14 The ADI is a validated measure of neighborhood disadvantage in the United States.15,16 Beneficiary mailing zip code was used to identify the corresponding ADI score to serve as a measure of each patient’s socioeconomic disadvantage. Mailing zip code was also used to construct urban vs rural inhabitance. Specifically, urban and rural population sizes were obtained from the Census Bureau 2010 Decennial survey for all zip codes.17 If more than 50% of the population in a zip code resided in a rural area, the zip code was designated as rural; otherwise, the zip code was designated as urban. A validated claims-based frailty index with strong evidence of validity in Medicare beneficiaries was used to classify patients as robust, prefrail, mildly frail, or moderately to severely frail.18 This index uses the deficit accumulation model to assess frailty, identifying older adults least likely to recover from physiological stressors. Patients were considered to meet consensus guideline criteria for parathyroidectomy if they had an ICD-9 or ICD-10 diagnosis code indicating a history of osteoporosis, nephrolithiasis, or stage 3 CKD.7 We were unable to assess whether patients met guideline criteria based on biochemical parameters (ie, serum calcium level >1.0 mg/dL greater than the upper limit of the reference range [to convert to mmol/L, multiply by 0.25] or 24-hour urinary calcium level of >400 mg/d). Patients who received endocrinologist care 6 months before or after PHPT diagnosis were identified by at least 1 outpatient or carrier claim with a Centers for Medicare & Medicaid Services provider specialty code indicating subspecialty training in endocrinology and a diagnosis code for PHPT or its related sequelae (ie, hypercalcemia, osteoporosis, and nephrolithiasis). The use of cinacalcet hydrochloride, a calcimimetic that reduces serum calcium levels but has not been shown to reduce end-organ damage in PHPT,19 was based on pharmacy claims during follow-up.
Outcomes
Patients who were managed with parathyroidectomy within 1 year of diagnosis were identified based on ICD-9/ICD-10 procedure codes (ICD-9: 0681, 0689, and 0699; ICD-10: 0GBLxxx, 0GBMxxx, 0GBNxxx, 0GBPxxx, 0GBQxxx, and 0GBRxxx) and Current Procedural Terminology codes 60500, 60502, and 60505 from all settings of claims. Beneficiaries were considered to have had a consultation for possible parathyroidectomy based on undergoing surgery within 1 year and/or having at least 1 outpatient or carrier claim with both a Centers for Medicare & Medicaid Services provider specialty code for a surgeon likely to perform parathyroidectomy (including endocrine surgeon, surgical oncologist, general surgeon, or otolaryngologist) and an ICD-9/ICD-10 diagnosis code for PHPT or related sequelae 6 months before or after PHPT diagnosis.
Statistical Analysis
Data were analyzed from February 11, 2020, to October 8, 2020. Our analytic approach sought to identify patient characteristics independently associated with the treatment of older adults with parathyroidectomy within 1 year of PHPT diagnosis. Univariate comparisons were performed using the χ2 and unpaired t tests. A multivariable logistic regression model was calculated to determine associations between patient characteristics and parathyroidectomy. Based on clinical relevance, we adjusted for age, sex, race/ethnicity, ADI, urban or rural inhabitance, frailty, Charlson Comorbidity Index score, history of osteoporosis, stage 3 CKD or nephrolithiasis, and endocrinologist care 6 months before or after diagnosis. Adjusted odds ratios (ORs) and 95% CIs were calculated. A Cochran-Armitage trend test was used to determine whether rates of parathyroidectomy changed consistently over time. We performed a priori planned sensitivity analyses to determine whether the results were substantively changed under 2 conditions: (1) when cohort enrollment was limited to patients 67 years or older (to ensure we were identifying incident diagnoses of PHPT as opposed to first recorded diagnosis code after enrollment in Medicare), and (2) when the primary outcome was defined as parathyroidectomy at any time after diagnosis (to evaluate the effect of the time horizon chosen for treatment decisions on our study findings). We performed additional sensitivity analyses to determine whether the rate of parathyroidectomy was substantively different when eliminating the continuous enrollment criteria or restricting the cohort to patients who survived more than 5 years after PHPT diagnosis. The significance level for all comparisons was P < .05, and tests were 2 tailed. Analyses were performed using SAS statistical software, version 9.4 (SAS Institute, Inc).
Results
We identified 210 206 Medicare beneficiaries diagnosed with PHPT from January 1, 2006, to December 31, 2016 (Figure 1). Demographic characteristics of this cohort are presented in Table 1, with a mean (SD) age of 75.3 (6.8) years, 78.8% women and 21.2% men, and 87.3% White participants. Among these older adults with PHPT, 63 136 (30.0%) underwent parathyroidectomy within 1 year of diagnosis. Patients treated with parathyroidectomy were younger (mean [SD] age, 73.5 [5.7] vs 76.0 [7.1] years; P < .001) and more likely to be White (90.1% vs 86.0%), to be robust or prefrail (92.1% vs 85.7%), and to have a lower comorbidity burden (Charlson Comorbidity Index score of 0 or 1, 54.6% vs 44.1%) compared with the nonoperative group (Table 1). Patients undergoing operative management were also more likely to live in disadvantaged neighborhoods (46.9% vs 40.3%) and rural geographic locations (18.1% vs 13.6%) (all P < .001). A total of 131 723 patients (62.7%) met at least 1 consensus guideline criteria for surgical management, and 38 983 of these patients (29.6%) were treated with parathyroidectomy within 1 year of diagnosis.
Table 1. Baseline Characteristics of Medicare Beneficiaries Diagnosed With PHPT, 2006-2016.
| Characteristic | Patient group, No. (%)a | ||
|---|---|---|---|
| Overall (n = 210 206) | Parathyroidectomy (n = 63 136) | Nonoperative management (n = 147 070) | |
| Sex | |||
| Male | 44 569 (21.2) | 13 684 (21.7) | 30 885 (21.0) |
| Female | 165 637 (78.8) | 49 452 (78.3) | 116 185 (79.0) |
| Age, y | |||
| 66-75 | 117 960 (56.1) | 42 024 (66.6) | 75 936 (51.6) |
| 76-85 | 73 491 (35.0) | 19 010 (30.1) | 54 481 (37.0) |
| ≥86 | 18 755 (8.9) | 2102 (3.3) | 16 653 (11.3) |
| Race/ethnicity | |||
| White | 183 433 (87.3) | 56 888 (90.1) | 126 545 (86.0) |
| Black | 19 797 (9.4) | 4741 (7.5) | 15 056 (10.2) |
| Asian | 1953 (0.9) | 390 (0.6) | 1563 (1.1) |
| Hispanic | 2280 (1.1) | 480 (0.8) | 1800 (1.2) |
| American Native | 453 (0.2) | 150 (0.2) | 303 (0.2) |
| Other | 2290 (1.1) | 487 (0.8) | 1803 (1.2) |
| ADI groupb | |||
| Advantaged | |||
| Most | 52 899 (25.2) | 12 717 (20.1) | 40 182 (27.3) |
| Slightly | 68 471 (32.6) | 20 784 (32.9) | 47 687 (32.4) |
| Disadvantaged | |||
| Slightly | 65 887 (31.3) | 22 093 (35.0) | 43 794 (29.8) |
| Most | 22 949 (10.9) | 7542 (11.9) | 15 407 (10.5) |
| Geography | |||
| Urban | 178 718 (85.0) | 51 689 (81.9) | 127 029 (86.4) |
| Rural | 31 488 (15.0) | 11 447 (18.1) | 20 041 (13.6) |
| Region | |||
| Midwest | 43 340 (20.6) | 15 031 (23.8) | 28 309 (19.2) |
| Northeast | 51 574 (24.5) | 9720 (15.4) | 41 854 (28.5) |
| South | 78 235 (37.2) | 26 629 (42.2) | 51 606 (35.1) |
| West | 37 057 (17.6) | 11 756 (18.6) | 25 301 (17.2) |
| Frailtyc | |||
| Robust | 76 954 (36.6) | 27 759 (44.0) | 49 195 (33.5) |
| Prefrail | 107 248 (51.0) | 30 394 (48.1) | 76 854 (52.3) |
| Mild | 18 316 (8.7) | 3531 (5.6) | 14 785 (10.1) |
| Moderate to severe | 7688 (3.7) | 1452 (2.3) | 6236 (4.2) |
| Charlson Comorbidity Index score | |||
| 0 | 51 534 (24.5) | 19 069 (30.2) | 32 465 (22.1) |
| 1 | 47 758 (22.7) | 15 372 (24.3) | 32 386 (22.0) |
| ≥2 | 110 914 (52.8) | 28 695 (45.4) | 82 219 (55.9) |
| Consensus guideline criteria | |||
| History | |||
| Stage 3 CKD | 17 566 (8.4) | 3565 (5.6) | 14 001 (9.5) |
| Nephrolithiasis | 28 239 (13.4) | 10 241 (16.2) | 17 998 (12.2) |
| Osteoporosis | 110 314 (52.5) | 32 067 (50.8) | 78 247 (53.2) |
| Endocrinologist care | 98 660 (46.9) | 34 142 (54.1) | 64 518 (43.9) |
Abbreviations: ADI, Area Deprivation Index; CKD, chronic kidney disease; PHPT, primary hyperparathyroidism.
Percentages have been rounded and may not total 100.
Determined based on mailing zip code of beneficiary according to the Neighborhood Atlas.15
Determined based on the validated claims-based frailty index.18
Overall, differences in the rate of parathyroidectomy were more pronounced by age group, comorbidity, and frailty status than by consensus guideline criteria (Figure 2). Although the rate of parathyroidectomy decreased with increasing age (absolute risk difference, 24.4% for 66-75 vs ≥86 years), Charlson Comorbidity Index score (absolute risk difference, 11.1% for Charlson Comorbidity Index score 0 vs ≥2), and frailty status (absolute risk difference, 17.2% for robust vs moderate to severe frailty), there was no clinically meaningful difference in the rate of parathyroidectomy based on meeting consensus guideline criteria within each age, Charlson Comorbidity Index score, or frailty group (absolute risk differences ≤3%).
Figure 2. Rate of Parathyroidectomy Among Patients Who Did and Did Not Meet Consensus Guideline Criteria for Surgical Management.
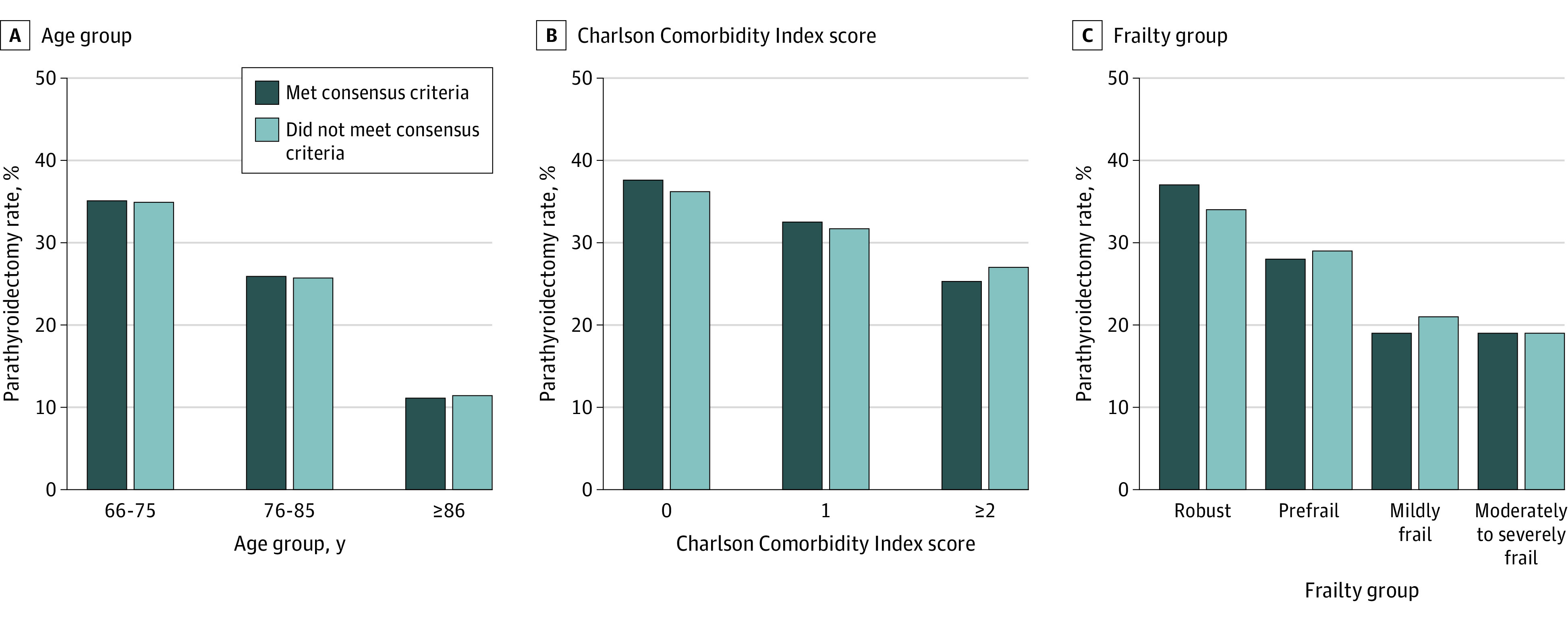
Data are stratified by age, comorbidity burden, and frailty. Meeting consensus criteria for parathyroidectomy was defined based on a documented diagnosis of osteoporosis, nephrolithiasis, or stage 3 chronic kidney disease.
On multivariable analysis, increasing age was inversely associated with parathyroidectomy among those aged 76 to 85 years (unadjusted rate, 25.9%; OR, 0.68 [95% CI, 0.67-0.70]) and 86 years or older (unadjusted rate, 11.2%; OR, 0.27 [95% CI, 0.26-0.29]) compared with ages 66 to 75 years (unadjusted rate, 35.6%), as were moderate to severe frailty (unadjusted rate, 18.9%; OR, 0.60 [95% CI, 0.56-0.64]) compared with being robust (unadjusted rate, 36.1%) and a Charlson Comorbidity Index score of at least 2 (unadjusted rate, 25.9%; OR, 0.77 [95% CI, 0.75-0.79]) compared with a Charlson Comorbidity Index score of 0 (unadjusted rate, 37.0%) (Table 2). Patients living in the most disadvantaged neighborhoods (OR, 1.66 [95% CI, 1.60-1.72] vs most advantaged) and rural areas (OR, 1.18 [95% CI, 1.15-1.22] vs urban areas) were more likely to be treated with parathyroidectomy. With regard to operative guideline consensus criteria, a history of nephrolithiasis increased the odds of parathyroidectomy (OR, 1.43 [95% CI, 1.39-1.47]); stage 3 CKD decreased the odds of parathyroidectomy (OR, 0.71 [95% CI, 0.68-0.74]); and having a history of osteoporosis showed no association (OR, 1.01 [95% CI, 0.99-1.03]).
Table 2. Patient Characteristics Associated With Parathyroidectomy Among Medicare Beneficiaries With PHPT Based on Multivariable Logistic Regression.
| Characteristic | Unadjusted rate of parathyroidectomy, No./total No. (%) | Adjusted OR (95% CI) |
|---|---|---|
| Sex | ||
| Female | 13 684/44 569 (30.7) | 1 [Reference] |
| Male | 49 453/165 637 (29.9) | 1.00 (0.98-1.03) |
| Age, y | ||
| 66-75 | 42 024/117 960 (35.6) | 1 [Reference] |
| 76-85 | 19 010/73 491 (25.9) | 0.68 (0.67-0.70) |
| ≥86 | 2102/18 755 (11.2) | 0.27 (0.26-0.29) |
| Race | ||
| White | 56 888/183 433 (31.0) | 1 [Reference] |
| Black | 4741/19 797 (23.9) | 0.67 (0.65-0.70) |
| Asian | 390/1953 (20.0) | 0.64 (0.57-0.72) |
| Hispanic | 480/2280 (21.1) | 0.66 (0.60-0.74) |
| American Native | 150/453 (33.1) | 0.97 (0.80-1.19) |
| Other | 487/2290 (21.3) | 0.62 (0.56-0.69) |
| ADI groupa | ||
| Advantaged | ||
| Most | 12 717/52 899 (24.0) | 1 [Reference] |
| Slightly | 20 784/68 471 (30.4) | 1.39 (1.35-1.43) |
| Disadvantaged | ||
| Slightly | 22 093/65 887 (33.5) | 1.61 (1.57-1.66) |
| Most | 7542/22 949 (32.9) | 1.66 (1.60-1.72) |
| Geography | ||
| Urban | 51 689/178 718 (28.9) | 1 [Reference] |
| Rural | 11 447/31 488 (36.4) | 1.18 (1.15-1.22) |
| Frailtyb | ||
| Robust | 27 759/76 954 (36.1) | 1 [Reference] |
| Prefrail | 30 394/107 248 (28.3) | 0.84 (0.82-0.86) |
| Mild | 3531/18 316 (19.3) | 0.61 (0.58-0.64) |
| Moderate to severe | 1452/7688 (18.9) | 0.60 (0.56-0.64) |
| Charlson Comorbidity Index score | ||
| 0 | 19 069/51 534 (37.0) | 1 [Reference] |
| 1 | 15 372/47 758 (32.2) | 0.88 (0.86-0.91) |
| ≥2 | 28 695/110 914 (25.9) | 0.77 (0.75-0.79) |
| Consensus guideline criteria | ||
| History | ||
| Nephrolithiasis | 10 241/28 239 (36.3) | 1.43 (1.39-1.47) |
| Osteoporosis | 32 067/110 314 (29.1) | 1.01 (0.99-1.03) |
| Stage 3 CKD | 3565/17 566 (20.3) | 0.71 (0.68-0.74) |
| Endocrinologist care | 34 142/98 660 (34.6) | 1.42 (1.40-1.45) |
Among all patients with PHPT, those living in the most advantaged neighborhoods (29.3%) and urban areas (35.1%) were least likely to undergo evaluation by a surgeon compared with those living in disadvantaged neighborhoods (40.6% for slightly and 40.3% for most disadvantaged) or rural areas (44.0%) (Table 3). There was no clinically significant difference in the rate of parathyroidectomy among patients evaluated by a surgeon within each ADI category or urban vs rural inhabitance, which ranged from 81.6% for most disadvantaged areas to 82.7% for slightly advantaged areas. Among the 131 723 patients who met consensus guideline criteria, 47 393 (36.0%) were evaluated by a surgeon and 38 983 of those (82.3%) underwent parathyroidectomy within 1 year. Among all 147 070 patients who underwent nonoperative management, 13 484 (9.2%) had an outpatient visit with a surgeon, suggesting possible evaluation for parathyroidectomy, and 7849 (5.3%) were treated with cinacalcet.
Table 3. Proportion of Patients With PHPT Evaluated by a Surgeon for Parathyroidectomy According to ADI and Urban or Rural Inhabitance.
| Variable | Total No. of patients | No. (%) of patients | |
|---|---|---|---|
| Evaluated by a surgeon | Treated with parathyroidectomy within 1 y | ||
| ADI categorya | |||
| Advantaged | |||
| Most | 52 899 | 15 491 (29.3) | 12 717 (82.1) |
| Slightly | 68 471 | 25 117 (36.7) | 20 784 (82.7) |
| Disadvantaged | |||
| Slightly | 65 887 | 26 774 (40.6) | 22 093 (82.5) |
| Most | 22 949 | 9238 (40.3) | 7542 (81.6) |
| Geography | |||
| Urban | 178 718 | 62 766 (35.1) | 51 689 (82.4) |
| Rural | 31 488 | 13 854 (44.0) | 11 447 (82.6) |
Abbreviation: ADI, Area Deprivation Index; PHPT, primary hyperparathyroidism.
Determined based on mailing zip code of beneficiary according to the Neighborhood Atlas.15
There were no qualitative differences in our study results in planned sensitivity analyses limiting cohort enrollment to those 67 years or older or defining the primary outcome as parathyroidectomy at any time during follow-up (eTables 1-4 in the Supplement). Median follow-up for the overall cohort was 55 (interquartile range, 31-86) months, and 5225 patients (35.8%) underwent parathyroidectomy at any point during follow-up. The rate of parathyroidectomy within 1 year of diagnosis was similar to that of the primary analysis if we did not apply continuous enrollment criteria (28.6%) or if we restricted the cohort to patients who survived more than 5 years after PHPT diagnosis (31.8%). There was an inconsistent but overall decreasing trend in the rate of parathyroidectomy in patients diagnosed with PHPT during the study period (32.0% in 2006; 28.2% in 2016; P < .001) and in the subgroup of patients who met at least 1 of the consensus guideline criteria (33.9% in 2006; 30.2% in 2016; P < .001) (eFigure in the Supplement).
Discussion
In this large, nationally representative cohort of older adults with PHPT, most patients underwent nonoperative management, with only 30.0% undergoing parathyroidectomy within 1 year of diagnosis. Patient characteristics independently associated with nonoperative management included older age, non-White race/ethnicity, frailty, and increased comorbidity burden. Beneficiaries living in rural and disadvantaged neighborhoods were more likely to be evaluated by a surgeon and treated with parathyroidectomy. Meeting consensus guideline criteria had an inconsistent association with treatment, with a history of nephrolithiasis conferring increased likelihood of parathyroidectomy, osteoporosis having no association, and stage 3 CKD decreasing the likelihood of surgical management. The rate of parathyroidectomy has decreased over time in patients overall and those who meet consensus guideline criteria. These findings suggest that definitive cure with parathyroidectomy is not readily used for the management of PHPT in older adults, and guideline recommendations appear to have minimal effect on treatment decisions, especially among frail patients with a high comorbidity burden.
Our study is, to our knowledge, the first national, population-based analysis to demonstrate low rates of use of parathyroidectomy in older adults with PHPT in the US and document that patient age, frailty, and comorbidity influence treatment decisions more than multidisciplinary guidelines. In a previous study looking at patients with commercial insurance or Medicare Advantage coverage diagnosed with PHPT (2004-2016), Seib et al10 found a similar rate of operative management among adults older than 65 years (30.1%), suggesting our present findings represent an accurate picture of the treatment of older adults diagnosed with PHPT in the US. Infrequent use of surgery and poor adherence to management guidelines for PHPT have also been documented in smaller regional, single-center, and Veterans Affairs studies.9,11,12 This study confirms that poor adherence to guidelines is national in scope, preferentially affecting older adults.
Prior studies have documented that age and comorbidity are inversely associated with surgical management of PHPT,11,12 but our finding that older age remains strongly and independently associated with nonoperative management after accounting for patient frailty in a large, insured patient population suggests that we are not using parathyroidectomy appropriately to prevent morbidity in older adults who are likely to benefit. This may be due to widespread unfamiliarity with guideline recommendations or, alternatively, provider concerns that guidelines do not apply to older, multimorbid patients. Existing guidelines for the surgical management of PHPT are based in large part on observational studies in which the median ages of surgically managed cohorts are substantially younger than those managed with observation and medical therapy.7,20 While the absolute risk of major complications from parathyroidectomy is low (1.1%), surgical risk increases among patients older than 75 years and those with frailty.21 Therefore, the absence of generalizable data on outcomes for older patients with PHPT may lead clinicians to question whether the short-term risks of parathyroidectomy outweigh long-term risk reduction for fractures, nephrolithiasis, and CKD in this vulnerable group. Although nonoperative management may represent appropriate clinical decision-making in some older, frail patients with limited life expectancy, the low rate of surgery in robust patients with PHPT suggests room for improvement. With the national scope of guideline nonadherence and nonoperative management now evident, a renewed focus should be placed on high-quality research to determine whether the benefits of parathyroidectomy exceed the risk of surgery in older adults, including those with multimorbidity and frailty.
It is notable that decreased use of parathyroidectomy for the management of PHPT over time occurred concurrently with expansion of published, multidisciplinary consensus criteria for operative management in 200922 and 2014.7 Prior studies suggest that increased routine calcium testing and expanded screening guidelines for osteoporosis have likely contributed to increased diagnosis of PHPT in patients with mild disease.1,23 Therefore, it is possible that increased detection of mild disease in an expanding older patient population accounts for the trend toward decreased use of parathyroidectomy over time. Long-term studies are needed to quantify the morbidity that results from the increasing burden of prevalent disease due to nonoperative management in older adults.
Specialist care by nephrologists and urologists has been associated with increased odds of evaluation for PHPT in patients with hypercalcemia and kidney stones.24 Therefore, a history of nephrolithiasis may be associated with increased odds of parathyroidectomy owing to exposure to specialists who are attuned to the indications for surgical treatment. In contrast, our finding that living in a disadvantaged neighborhood or a rural area was independently associated with increased odds of surgical management was contrary to our expectation that these patients may have decreased access to an endocrinologist or specialized surgical care and therefore more often are treated nonoperatively. Lower socioeconomic status and rural inhabitance have been associated with parathyroidectomy by low-volume surgeons25,26 but, to our knowledge, no prior population-based studies have evaluated the effect of these factors on treatment decisions. A possible explanation for our findings is that patients in disadvantaged or rural neighborhoods are more likely to have severe biochemical disease owing to delayed diagnosis in patients with poor access to care. We do not have biochemical data from this cohort to test this hypothesis. Another possibility is that the difference in management was related to patient preference or clinician referral patterns. This possibility is supported by our finding that patients were less likely to be evaluated by a surgeon if they lived in urban or advantaged neighborhoods. Further studies are needed to understand patient preferences and determine the role that severity of biochemical disease plays in treatment decisions.
Strengths and Limitations
Strengths of our study include the large sample size and geographic diversity of a nationally representative population with PHPT. In addition, the use of validated measures of socioeconomic status and frailty as covariates in our multivariable models provide a more nuanced understanding of potential barriers to surgical management and guideline-concordant care than is documented in prior analyses. Limitations of our study are those inherent to research using administrative claims data. Prior studies using biochemical data9,27 have shown that PHPT is underdiagnosed. As a result, the use of ICD-9/ICD-10 codes to identify our cohort likely results in underidentification of those with biochemically evident PHPT that is not recognized or coded for by physicians and, therefore, an overestimation of the rate of parathyroidectomy in older adults with PHPT. However, the motivation for this study was to identify patient factors that influence initial PHPT treatment decisions by patients and clinicians; therefore, we chose to use criteria with high specificity to identify a nationally representative cohort with a recognized diagnosis of PHPT. The absence of clinical data such as calcium and parathyroid hormone levels, as well as diagnostic testing indicative of the severity of PHPT and its sequelae, such as bone mineral density and urinary calcium excretion, prevented us from including these factors in our models, despite their relevance as consensus guideline criteria for parathyroidectomy and their importance to clinicians. Owing to the retrospective nature of our analysis, there also may be unmeasured confounding of the association between patient characteristics and operative management. Last, as is common in analyses of Medicare claims, we excluded beneficiaries with Medicare Advantage plans to ensure we had complete ascertainment of claims. This and other exclusions to prevent cohort contamination from patients with secondary and tertiary hyperparathyroidism may have contributed to bias in cohort creation. However, the similarity of our current findings to those of our prior analysis, including older adults with PHPT and Medicare Advantage coverage,10 support the generalizability of our results to the overall Medicare population, which represents more than 90% of older adults in the US.
Conclusions
The findings of this cohort study suggest that most older adults with PHPT in the US do not receive definitive treatment with parathyroidectomy, and older age, frailty, and comorbidity are significantly associated with treatment decisions, whereas meeting consensus guideline criteria demonstrated inconsistent associations, in some cases against guideline recommendations. Further research is needed to identify barriers to appropriate surgical care and develop tools to target parathyroidectomy to older adults most likely to benefit.
eTable 1. Baseline Characteristics of Medicare Beneficiaries Diagnosed With PHPT (2006-2016) When Cohort Is Restricted to Patients 67 Years and Older
eTable 2. Baseline Characteristics of Medicare Beneficiaries Diagnosed With PHPT (2006-2016) When Parathyroidectomy at Any Time After Diagnosis Is Considered Primary Outcome
eTable 3. Patient Characteristics Associated With Parathyroidectomy for Beneficiaries With PHPT Based on Multivariable Logistic Regression When Cohort Is Restricted to Patients 67 Years and Older
eTable 4. Patient Characteristics Associated With Parathyroidectomy for Beneficiaries With PHPT Based on Multivariable Logistic Regression When Parathyroidectomy at Any Time After Diagnosis Is Considered
eFigure. Rate of Parathyroidectomy in Those Diagnosed With PHPT in Each Calendar Year (2006-2016) Among All Patients and Those Who Met Consensus Guideline Criteria for Operative Management
References
- 1.Yeh MW, Ituarte PHG, Zhou HC, et al. Incidence and prevalence of primary hyperparathyroidism in a racially mixed population. J Clin Endocrinol Metab. 2013;98(3):1122-1129. doi: 10.1210/jc.2012-4022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yeh MW, Zhou H, Adams AL, et al. The relationship of parathyroidectomy and bisphosphonates with fracture risk in primary hyperparathyroidism: an observational study. Ann Intern Med. 2016;164(11):715-723. doi: 10.7326/M15-1232 [DOI] [PubMed] [Google Scholar]
- 3.Mollerup CL, Vestergaard P, Frøkjaer VG, Mosekilde L, Christiansen P, Blichert-Toft M. Risk of renal stone events in primary hyperparathyroidism before and after parathyroid surgery: controlled retrospective follow up study. BMJ. 2002;325(7368):807. doi: 10.1136/bmj.325.7368.807 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Assadipour Y, Zhou H, Kuo EJ, Haigh PI, Adams AL, Yeh MW. End-organ effects of primary hyperparathyroidism: a population-based study. Surgery. 2019;165(1):99-104. doi: 10.1016/j.surg.2018.04.088 [DOI] [PubMed] [Google Scholar]
- 5.Coker LH, Rorie K, Cantley L, et al. Primary hyperparathyroidism, cognition, and health-related quality of life. Ann Surg. 2005;242(5):642-650. doi: 10.1097/01.sla.0000186337.83407.ec [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pepe J, Cipriani C, Sonato C, Raimo O, Biamonte F, Minisola S. Cardiovascular manifestations of primary hyperparathyroidism: a narrative review. Eur J Endocrinol. 2017;177(6):R297-R308. doi: 10.1530/EJE-17-0485 [DOI] [PubMed] [Google Scholar]
- 7.Bilezikian JP, Brandi ML, Eastell R, et al. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Fourth International Workshop. J Clin Endocrinol Metab. 2014;99(10):3561-3569. doi: 10.1210/jc.2014-1413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ambrogini E, Cetani F, Cianferotti L, et al. Surgery or surveillance for mild asymptomatic primary hyperparathyroidism: a prospective, randomized clinical trial. J Clin Endocrinol Metab. 2007;92(8):3114-3121. doi: 10.1210/jc.2007-0219 [DOI] [PubMed] [Google Scholar]
- 9.Alore EA, Suliburk JW, Ramsey DJ, et al. Diagnosis and management of primary hyperparathyroidism across the Veterans Affairs health care system. JAMA Intern Med. 2019;179(9):1220-1227. doi: 10.1001/jamainternmed.2019.1747 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Seib CD, Meng T, Suh I, et al. Undertreatment of primary hyperparathyroidism in a privately insured US population: decreasing utilization of parathyroidectomy despite expanding surgical guidelines. Surgery. Published online July 9, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wu B, Haigh PI, Hwang R, et al. Underutilization of parathyroidectomy in elderly patients with primary hyperparathyroidism. J Clin Endocrinol Metab. 2010;95(9):4324-4330. doi: 10.1210/jc.2009-2819 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kuo EJ, Al-Alusi MA, Du L, et al. Surgery for primary hyperparathyroidism: adherence to consensus guidelines in an academic health system. Ann Surg. 2019;269(1):158-162. doi: 10.1097/SLA.0000000000002474 [DOI] [PubMed] [Google Scholar]
- 13.Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613-619. doi: 10.1016/0895-4356(92)90133-8 [DOI] [PubMed] [Google Scholar]
- 14.Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130-1139. doi: 10.1097/01.mlr.0000182534.19832.83 [DOI] [PubMed] [Google Scholar]
- 15.Kind AJH, Buckingham WR. Making neighborhood-disadvantage metrics accessible—the Neighborhood Atlas. N Engl J Med. 2018;378(26):2456-2458. doi: 10.1056/NEJMp1802313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hu J, Kind AJH, Nerenz D. Area Deprivation Index predicts readmission risk at an urban teaching hospital. Am J Med Qual. 2018;33(5):493-501. doi: 10.1177/1062860617753063 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.US Census Bureau. 2010 Census Bureau Decennial Survey . Published January 2013. Accessed April 2, 2020. https://data.census.gov/cedsci/table?g=0100000US.860000&tid=DECENNIALSF12010.H2&hidePreview=true
- 18.Kim DH, Glynn RJ, Avorn J, et al. Validation of a claims-based frailty index against physical performance and adverse health outcomes in the Health and Retirement Study. J Gerontol A Biol Sci Med Sci. 2019;74(8):1271-1276. doi: 10.1093/gerona/gly197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Peacock M, Bolognese MA, Borofsky M, et al. Cinacalcet treatment of primary hyperparathyroidism: biochemical and bone densitometric outcomes in a five-year study. J Clin Endocrinol Metab. 2009;94(12):4860-4867. doi: 10.1210/jc.2009-1472 [DOI] [PubMed] [Google Scholar]
- 20.Wilhelm SM, Wang TS, Ruan DT, et al. The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. 2016;151(10):959-968. doi: 10.1001/jamasurg.2016.2310 [DOI] [PubMed] [Google Scholar]
- 21.Seib CD, Chomsky-Higgins K, Gosnell JE, et al. Patient frailty should be used to individualize treatment decisions in primary hyperparathyroidism. World J Surg. 2018;42(10):3215-3222. doi: 10.1007/s00268-018-4629-3 [DOI] [PubMed] [Google Scholar]
- 22.Bilezikian JP, Khan AA, Potts JT Jr; Third International Workshop on the Management of Asymptomatic Primary Hyperthyroidism . Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Third International Workshop. J Clin Endocrinol Metab. 2009;94(2):335-339. doi: 10.1210/jc.2008-1763 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Walker MD, Silverberg SJ. Primary hyperparathyroidism. Nat Rev Endocrinol. 2018;14(2):115-125. doi: 10.1038/nrendo.2017.104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ganesan C, Weia B, Thomas IC, et al. Analysis of primary hyperparathyroidism screening among US veterans with kidney stones. JAMA Surg. 2020;155(9):861-868. doi: 10.1001/jamasurg.2020.2423 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Al-Qurayshi Z, Hauch A, Srivastav S, Kandil E. Ethnic and economic disparities effect on management of hyperparathyroidism. Am J Surg. 2017;213(6):1134-1142. doi: 10.1016/j.amjsurg.2016.07.008 [DOI] [PubMed] [Google Scholar]
- 26.Sosa JA, Tuggle CT, Wang TS, et al. Clinical and economic outcomes of thyroid and parathyroid surgery in children. J Clin Endocrinol Metab. 2008;93(8):3058-3065. doi: 10.1210/jc.2008-0660 [DOI] [PubMed] [Google Scholar]
- 27.Press DM, Siperstein AE, Berber E, et al. The prevalence of undiagnosed and unrecognized primary hyperparathyroidism: a population-based analysis from the electronic medical record. Surgery. 2013;154(6):1232-1237. doi: 10.1016/j.surg.2013.06.051 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Baseline Characteristics of Medicare Beneficiaries Diagnosed With PHPT (2006-2016) When Cohort Is Restricted to Patients 67 Years and Older
eTable 2. Baseline Characteristics of Medicare Beneficiaries Diagnosed With PHPT (2006-2016) When Parathyroidectomy at Any Time After Diagnosis Is Considered Primary Outcome
eTable 3. Patient Characteristics Associated With Parathyroidectomy for Beneficiaries With PHPT Based on Multivariable Logistic Regression When Cohort Is Restricted to Patients 67 Years and Older
eTable 4. Patient Characteristics Associated With Parathyroidectomy for Beneficiaries With PHPT Based on Multivariable Logistic Regression When Parathyroidectomy at Any Time After Diagnosis Is Considered
eFigure. Rate of Parathyroidectomy in Those Diagnosed With PHPT in Each Calendar Year (2006-2016) Among All Patients and Those Who Met Consensus Guideline Criteria for Operative Management