

Abstract
Introduction
Traumatic experiences and disordered sleep are strongly associated with drinking problems. We examined the effects of experiencing the Great East Japan Earthquake and subsequent nuclear power plant accident, and of sleep problems, on behavioral changes observed in non-drinkers.
Methods
This study examined cross-sectional data from the Mental Health and Lifestyle Survey conducted among residents in restricted areas of Fukushima in 2012. Participants were 21,454 evacuees aged 20 years or older at the time of disaster. People who did not drink before the disaster but became drinkers afterwards were compared with the rest of the cohort. We analyzed the association between behavioral changes in non-drinkers and potentially predictive variables, using logistic regression.
Results
The behavioral change of non-drinkers becoming drinkers (n=2,148) was significantly related to being male (OR=1.93, 95% CI: 1.74-2.15), being younger (21-49 yrs, OR=1.85, 95% CI: 1.60-2.13), having less educational attainment (up to high school graduate, OR=1.21, 95% CI: 1.09-1.35), smoking (OR=1.22, 95% CI: 1.08-1.38), losing family or relatives (OR=1.21, 95% CI: 1.07-1.37), change in employment (OR=1.19, 95% CI: 1.07-1.32), having severe sleep problems as measured by a Japanese version of the Athens Insomnia Scale (3-8, OR=1.45, 95% CI: 1.30-1.62), and severity of traumatic symptoms as measured by the PTSD Checklist Stressor-Specific (PCL-S) score (<44, OR=1.33, 95% CI: 1.17–1.51).
Conclusion
Having sleep problems and having more severe traumatic symptoms are significantly related to non-drinkers becoming drinkers.
Keywords: disaster, alcohol, trauma, sleep
Introduction
The Great East Japan Earthquake that occurred on March 11, 2011 caused a tsunami and an accident at the Fukushima Daiichi Nuclear Power Plant (hereinafter NPP). As evident from what happened in Chernobyl, there were great concerns about long-term psychological trauma among those who survived evacuation, arising from: fears about radiation exposure;loss of family, relatives, and/or property; and experience of other threats to life and livelihood.
Many studies have shown that disasters can have a significant impact on mental health. Experience of disaster could cause post-disaster mental distress among victims, including depression, post-traumatic stress disorder (PTSD), and suicidality1,2). Many victims showed increased symptoms of stress, difficulties caused by anxiety and sleep disturbance, and depressive symptoms or hopelessness after the Hanshin-Awaji Earthquake3). Disasters are experienced by many people and may result in a wide range of mental and physical health consequences4). Depression and anxiety are also commonly observed psychological problems in both natural disasters and terrorist attacks5,6). Severe psychological distress was likely to be found among those who experienced the earthquake, tsunami, and subsequent nuclear power plant accident7).
Associations between natural disasters and the use and abuse of alcohol are well established8). It can be imagined that people who have experienced a disaster consume alcohol to soothe their anxiety and help them fall asleep. Beaudoin reported that exposure to traumatic events increased alcohol consumption among evacuees after Hurricane Katrina9). Similarly, Cerda et al. found increased alcohol consumption after a disaster when compared with pre-disaster levels of consumption10). Keyes and Hatzenbuehler reviewed epidemiological studies and reported that escalation of alcohol use after a disaster may be most noticeable among those who already manifested drinking problems before the disaster11). Flory et al. described that survivors of Hurricane Katrina experienced alcohol consumption-related problems at a higher rate than expected as compared to pre-disaster prevalence data12). North et al. reviewed 10 disaster studies and recognized that while the post-disaster prevalence of alcohol use disorders was 19%, only 0.3% of the sample developed an acute new post-disaster alcohol use disorder, but they did not further discuss the profile of those who developed new alcohol use disorder13). Brower et al. pointed out that alcohol was also used as a way to deal with sleep problems among those with alcohol dependence14). Zhabenko discussed a correlation of alcohol dependence and insomnia among Polish patients using the Athens Insomnia Scale15).
In this context, the development of a drinking habit after a disaster could provoke mental health problems. For instance, Volpicelli et al. discussed a hypothesis that alcohol may relieve PTSD symptoms, such as anxiety, irritability, and depression because drinking compensates for deficiencies in endorphin activity following a traumatic experience16). In addition, a study conducted in the same population as this study revealed that changes of drinking style rather than level of individual consumption could significantly affect mental health conditions among affected people17). However, research has not yet fully explored whether disasters influence people who were non-drinkers before a disaster to become drinkers afterwards.
It seems highly likely that drinking behaviors would be considerably affected among those who have experienced a disaster, subsequent evacuation, and consequent suffering from traumatic stress reactions and sleep problems. A literature review showed that previous studies focused on those with preexisting alcohol problems and their other problems after a disaster8-12,14). However, the relationship between change in drinking behavior and disaster-related experience among those who did not drink before the disaster has not yet been examined.
After the Fukushima NPP accident, Fukushima Prefecture launched the Fukushima Health Management Survey, an extensive health survey to monitor the health status of evacuees and to arrange for those who are at risk of health problems to liaise with local resources18). Using baseline data from this survey, this study aimed to examine the relationship between changes in drinking behavior with sleep problems and traumatic symptoms, while controlling for disaster related-factors. The research question examined in this study was: What are the predictors of becoming a drinker ?
Methods
Study design
This study was a part of a longitudinal survey to monitor the mental health status of evacuees of the Fukushima NPP accident18,19). We used data from the Fukushima Health Management Survey, specifically, cross-sectional data from its Mental Health and Lifestyle Survey conducted in 2012, about one year after the accident.
This study was approved by the ethics review committee of Fukushima Medical University, which is guided by local policy, national law, and the World Medical Association Declaration of Helsinki.
Participants
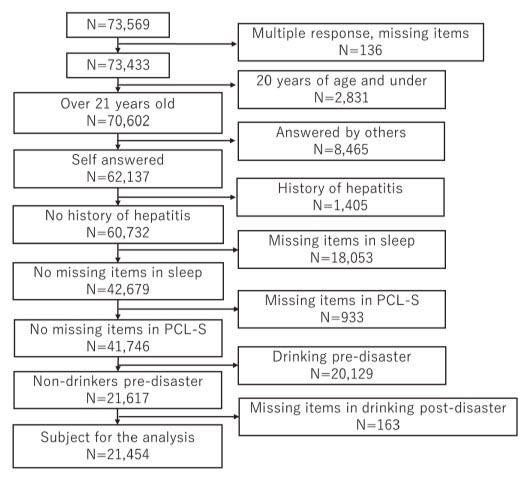
The target population of this survey was the entire population in the evacuation zone designated by Fukushima Prefecture due to the NPP accident (210,189 people). The survey items varied according to participants’ age range, with those who were 16 years or older at the time of the questionnaire using a self-administered PTSD Checklist Stressor-Specific Version (PCL-S)18). Hence, those who were aged 15 years or older as of March 11, 2011, (n=180,604) were the intended subjects of this study, and data on 73,569 participants were analyzed based on their valid responses (response rate: 40.7%)20).
In Japan, the legal drinking age is 20 years; therefore, we decided to exclude those aged less than 20 years at the time of the disaster. In order to do so, we excluded those who were aged less than 21 years at the time of the survey, which took place a year after the disaster. We also excluded those whose questionnaires were administered by others, those who had a history of chronic hepatitis, and those with missing items pertaining to sleep and PCL-S scores, so that the final sample size was n=21,454 (Figure 1).
Figure 1.
We divided the participants into three age groups, 21 to 49 years, 50 to 64 years, and 65 years and older, according to the previous study by Ueda et al. in which we had analyzed the same subjects17).
Measurements
Changes in drinking behavior
We asked about drinking patterns before the disaster by inquiring whether they used to drink less than once a month, and at the time when the questionnaire was administered by asking the average frequency and amount of alcohol consumed, and divided subjects into two groups: those who had been non-drinkers before the disaster and became drinkers post-disaster (hereinafter new drinkers), and those who had been non-drinkers before the disaster and remained non-drinkers post-disaster.
Those who had been diagnosed with chronic hepatitis were excluded from the data set since their alcohol consumption would be affected by their medical treatment.
Socioeconomic and other factors
For demographic and other variables, items were codified and examined as follows:
1) Socioeconomic variables included educational attainment: elementary school, junior high school, and high school as 0;vocational college, junior college, university (4 years), and graduate school as 1. This was in accord with a previous study by Ueda et al., in which we had analyzed the same subjects17) for analytical purposes. 2) Other factors included: subjective health status as very good, good, normal, poor, or very poor;smoking as yes or no;and exercise habits as almost every day, 2 to 4 times a week, once a week, or almost never.
Experience of disaster
Experience of disaster pertained to items that characterized the nature of disaster exposure, since individual experience differed significantly depending on where the person experienced disaster. Items describing exposure to the disaster included: experience of the tsunami as yes or no;and experience of the NPP accident – defined as hearing an explosion – as yes or no.
Disaster-related problems
Items describing secondary life stressors induced by the disaster included: experiencing damage to one’s house as yes for partial collapse, extensive collapse, or total collapse;and no for damage or partial damage;loss of family or relatives because of the disaster as yes or no;change in employment as yes or no;and change in living arrangements as 0 for a rental home, apartment, relative’s home, one’s own home or other;and 1 for evacuation shelter or temporary housing.
Sleep problems
A Japanese version of the Athens Insomnia Scale (AIS) was previously developed and validated21), and we used a simplified Japanese AIS, for which its psychometric properties were recently investigated for acceptable reliability (Cronbach alpha was 0.81)22). We asked eight questions regarding sleep problems, just as in the original AIS. In terms of satisfaction with sleep over the past month, we assigned 0 to “satisfied” and “slightly dissatisfied,” and 1 to “quite dissatisfied” and “very dissatisfied or have not slept at all.” For the other seven questions regarding experiences with sleep, we codified frequency of the problems as at least three times a week, instead of the original 4-point Likert scale (taking time to fall asleep, waking up in the middle of the night, waking up earlier than planned, not getting enough sleep, feeling depressed during the day, having reduced mental and physical activity, and feeling tired during the day). We allocated 1 to “yes,” and tallied the number of sleep problems.
Traumatic symptoms
Traumatic symptoms were assessed using the PTSD Checklist Stressor-Specific (PCL-S) scale. In the PCL-S scale, participants were asked to describe their experiences, in the past month, related to the earthquake and the subsequent power plant accident. Each question was rated on a 5-point Likert scale from one (not at all) to five (very much), with higher scores signifying more severe traumatic symptoms (range: 17-85). The original PCL was described by Blanchrd, EB et al. in 199623) and very recently, the reliability of a Japanese version was tested by Suzuki24), for the same population, which showed sufficient reliability (Cronbach’s Alpha was 0.92). In this study, we used the same cut-off threshold as the previous study17).
Statistical analysis
In order to explore the characteristics of new drinkers, we compared their basic characteristics and changes in drinking behavior using the chi-square test (Table 1). Disaster-related and socioeconomic variables were also compared between new drinkers and non-drinkers before and after the disaster using the chi-square test.
Table 1.
Characteristics of the non-drinkers and the new drinkers (n=21,617)
| Total | Non-drinkers | New drinkers | |||||||||
| n | % | n | % | n | % | χ2 | df | P values | |||
| Gender | n=21,454 | n=19,306 | n=2,148 | ||||||||
| Males | 5,943 | 27.7 | 5,063 | 26.2 | 880 | 41.0 | 209.788 | 1 | <0.001 | ||
| Age | n=21,454 | n=19,306 | n=2,148 | ||||||||
| 21-49 years old | 8,861 | 41.3 | 7,701 | 39.9 | 1,160 | 54.0 | 170.374 | 2 | <0.001 | ||
| 50-64 years old | 6,652 | 31.0 | 6,073 | 31.5 | 579 | 27.0 | |||||
| 65 years old and older | 5,941 | 27.7 | 5,532 | 28.7 | 409 | 19.0 | |||||
| Socioeconomic and other factors | |||||||||||
| Education attainment | n=20,923 | n=18,814 | n=2,109 | ||||||||
| Primary or middle school, or high school | 14,946 | 71.4 | 13,547 | 72.0 | 1,399 | 66.3 | 29.879 | 1 | <0.001 | ||
| Vocational college, junior college, university, or graduate school | 5,977 | 28.6 | 5,267 | 28.0 | 710 | 33.7 | |||||
| Subjective health status | n=21,139 | n=19,021 | n=2,118 | ||||||||
| Very good, good, or normal | 17,349 | 82.1 | 15,629 | 82.2 | 1,720 | 81.2 | 1.190 | 1 | 0.275 | ||
| Poor, or very poor | 3,790 | 17.9 | 3,392 | 17.8 | 398 | 18.8 | |||||
| Smoking | n=21,247 | n=19,126 | n=2,121 | ||||||||
| Current smoker | 3,531 | 16.6 | 2,997 | 15.7 | 534 | 25.2 | 124.534 | 1 | <0.001 | ||
| Exercise habit | n=21,234 | n=19,108 | n=2,126 | ||||||||
| Almost everyday | 2,729 | 12.9 | 2,492 | 13.0 | 237 | 11.1 | 24.055 | 3 | <0.001 | ||
| 2 to 4 times a week | 3,933 | 18.5 | 3,600 | 18.8 | 333 | 15.7 | |||||
| 1 a week | 2,763 | 13.0 | 2,483 | 13.0 | 280 | 13.2 | |||||
| Almost never | 11,809 | 55.6 | 10,533 | 55.1 | 1,276 | 60.0 | |||||
| Experience of disaster | |||||||||||
| Experience of tsunami | n=21,454 | n=19,306 | n=2,148 | ||||||||
| Yes | 3,836 | 17.9 | 3,379 | 17.5 | 457 | 21.3 | 18.743 | 1 | <0.001 | ||
| Experience of nuclear power plant accident | n=21,454 | n=19,306 | n=2,148 | ||||||||
| Yes | 10,802 | 50.3 | 9,651 | 50.0 | 1,151 | 53.6 | 9.994 | 1 | 0.002 | ||
| Disaster related problems | |||||||||||
| House damage | |||||||||||
| Partial-collapse and severer | n=20,114 | n=18,123 | n=1,991 | ||||||||
| Yes | 3,048 | 15.2 | 2,717 | 15.0 | 331 | 16.6 | 3.720 | 1 | 0.054 | ||
| Loss of family or relatives | n=21,170 | n=19,056 | n=2,114 | ||||||||
| Yes | 4,045 | 19.1 | 3,575 | 18.8 | 470 | 22.2 | 14.843 | 1 | <0.001 | ||
| Change in work | n=20,553 | n=18,454 | n=2,099 | ||||||||
| Yes | 10,985 | 53.4 | 9,693 | 52.5 | 1,292 | 61.6 | 61.735 | 1 | <0.001 | ||
| Living arrangement | n=17,376 | n=15,693 | n=1,683 | ||||||||
| Rental housing, apartment, relative’s home, own home or other | 15,259 | 87.8 | 13,765 | 87.7 | 1,494 | 88.8 | 1.584 | 1 | 0.208 | ||
| Evacuation shelter or temporary housing | 2,117 | 12.2 | 1,928 | 12.3 | 189 | 11.2 | |||||
| Psychiatric problems | |||||||||||
| Sleep problem | n=21,454 | n=19,306 | n=2,148 | ||||||||
| 0 | 3,821 | 17.8 | 3,526 | 18.3 | 295 | 13.7 | 96.841 | 8 | <0.001 | ||
| 1 | 3,082 | 14.4 | 2,826 | 14.6 | 256 | 11.9 | |||||
| 2 | 3,006 | 14.0 | 2,755 | 14.3 | 251 | 11.7 | |||||
| 3 | 2,776 | 12.9 | 2,505 | 13.0 | 271 | 12.6 | |||||
| 4 | 2,414 | 11.3 | 2,137 | 11.1 | 277 | 12.9 | |||||
| 5 | 2,028 | 9.5 | 1,786 | 9.3 | 242 | 11.3 | |||||
| 6 | 1,624 | 7.6 | 1,417 | 7.3 | 207 | 9.6 | |||||
| 7 | 1,427 | 6.7 | 1,255 | 6.5 | 172 | 8.0 | |||||
| 8 | 1,276 | 5.9 | 1,099 | 5.7 | 177 | 8.2 | |||||
| Traumatic symptoms (PCL) ≧44 | n=21,454 | n=19,306 | n=2,148 | ||||||||
| Yes | 4,610 | 21.5 | 4,025 | 20.8 | 585 | 27.2 | 46.728 | 1 | <0.001 | ||
We performed a logistic regression analysis adjusting for age and gender, then calculated adjusted odds ratios and 95% confidence intervals (CIs) using multiple logistic regression analyses by entering factors which were statistically significant in single logistic regression analysis (Table 2). These were performed to examine the association of changes in drinking behavior pre- and post-disaster with the following factors: basic characteristics and socioeconomic status, that is, educational attainment, subjective health status, smoking, and exercise habits; the experience of disaster, that is, experience of the tsunami, experience of the NPP accident; disaster related problems, that is, house damage, loss of family or relatives, changes in employment, and changes in living arrangements;sleep problems, using the total number of self-reported problems related to sleep (0 to 2 and 3 to 8) for exploratory effort, but not to see dose response, as a dependent variable;and traumatic symptoms, using the range of PCL-S ≧44 as a dependent variable. Significance was set at p<0.05.
Table 2.
The associations between potentially predictive variables and starting drinking
|
Statement drinking status before and after disaster
(Sex-Age adjusted model) |
Statement drinking status before and after disaster
(multivariable analysis) |
||||||||||
| New drinker | New drinker | ||||||||||
| Model | OR | (95%CI) | P value | OR | (95%CI) | P value | |||||
| n=21,454 | |||||||||||
| Gender (0 Females, 1 Males) | |||||||||||
| Males | 1.93 | 1.74-2.15 | <0.001 | ||||||||
| Age (0 65 years old and older) | |||||||||||
| 21-49 years old | 1.85 | 1.60-2.13 | 0.003 | ||||||||
| 50-64 years old | 1.24 | 1.07-1.44 | 0.004 | ||||||||
| Socioeconomic and other factors | |||||||||||
| Education attainment (0 less High school, 1 more Vocational college/Junior college) | 1.17 | 1.06-1.29 | 0.002 | 1.21 | 1.09-1.35 | 0.001 | |||||
| Subjective health status (0 Very good/Good/Normal, 1 Bad/Very bad) | 1.17 | 1.04-1.32 | 0.009 | 0.90 | 0.78-1.03 | 0.135 | |||||
| Smoking (0 Never smoked/Quit, 1 Current smoker) | 1.23 | 1.10-1.38 | <0.001 | 1.22 | 1.08-1.38 | 0.002 | |||||
| Exercise habit (0 Almost never, 1 Once a week/2-4 times a week/Almost every day) | 1.02 | 0.97-1.06 | 0.503 | ||||||||
| Experience of disaster | |||||||||||
| Experience of tsunami (0 No, 1 Yes) | 1.25 | 1.12-1.40 | <0.001 | 1.06 | 0.93-1.21 | 0.357 | |||||
| Experience of nuclear power plant accident (0 No, 1 Yes) | 1.21 | 1.11-1.33 | <0.001 | 1.03 | 0.93-1.14 | 0.590 | |||||
| Disaster related problems | |||||||||||
| House damage (0 No damage/Partial damage, 1 Partial collapse and severer) | 1.18 | 1.04-1.34 | 0.011 | 1.02 | 0.88-1.17 | 0.822 | |||||
| Loss of family or relatives (0 No, 1 Yes) | 1.32 | 1.18-1.47 | <0.001 | 1.21 | 1.07-1.37 | 0.002 | |||||
| Change in work (0 No, 1 Yes) | 1.33 | 1.21-1.46 | <0.001 | 1.19 | 1.07-1.32 | 0.001 | |||||
| Living arrangement (0 Rental housing/Apartment/Relative’s home/Own home/other, 1 Evacuation shelter/Temporary housing) | 0.93 | 0.79-1.09 | 0.338 | ||||||||
| Psychiatric problems | |||||||||||
| Sleep problem (0 0-2) | |||||||||||
| 3-8 | 1.60 | 1.46-1.76 | <0.001 | 1.45 | 1.30-1.62 | <0.001 | |||||
| Traumatic symptoms(PCL-S) ≧44 (0 No, 1 Yes) | 1.57 | 1.42-1.74 | <0.001 | 1.33 | 1.17-1.51 | <0.001 | |||||
All statistical analyses were conducted using SPSS version 21.0.
Results
Table 1 shows the characteristics of new drinkers. The number of new drinkers was 2,148 (male: 880, female: 1,268), out of 21,454 (male: 5,943, female: 15,511) participants. The proportion of those who became new drinkers was higher among males, in the younger age group, in those with less educational attainment, in smokers, in those less likely to exercise, in those who had experienced the tsunami and NPP accident, in those who experienced more family loss and changes in employment, and in those with accumulated sleep problems and higher PCL-S scores. Pearson’s chi-square test was performed to test statistical significance.
Table 2 shows the results of a comparison between new drinkers and non-drinkers using a logistic regression analysis to examine the relationship between changes in drinking behavior with sleep problems and traumatic symptoms. We controlled for basic characteristics, i.e., age and gender, disaster-related variables, and socioeconomic and other factors. New drinkers had a significantly higher rate of sleep problems. The OR of severe sleep problems was 1.45 (95% CI: 1.30-1.62).
The behavioral change of becoming a new drinker was also significantly correlated with traumatic symptoms, and the OR of traumatic symptoms according to the PCL-S score of 44 and over was 1.33 (95% CI: 1.17-1.51). Furthermore, we obtained sufficient internal consistency in the PCL-S score;Cronbach’s alpha was 0.95.
The results showed that age and gender groups were significantly associated with behavioral change in drinking behavior as well as with psychological distress. The OR of being male was 1.93 (95% confidence interval, CI: 1.74-2.15), and compared with those aged over 65 years, the OR of those aged between 21 and 49 years was 1.85 (95% CI: 1.60-2.13) for the change from non-drinking to drinking. In socioeconomic and other factors, having less educational attainment (OR=1.21, 95% CI: 1.09-1.35) and having a smoking habit (OR=1.22, 95% CI: 1.08-1.38) were statistically significant, but subjective health status did not show significant correlations. Among experience of disaster and related factors, loss of family or relatives (OR=1.21, 95% CI: 1.07-1.37) and change in employment (OR=1.19, 95% CI: 1.07-1.32) increased the likelihood of becoming a new drinker. On the other hand, experience of the tsunami, experience of the NPP accident, and house damage did not have significant correlations with the change in drinking behavior.
Discussion
Similar to other studies25,26), male and younger respondents were more likely to become new drinkers. The results show that young males might have developed inadequate coping skills in response to disaster. In addition, logistic regression analysis revealed that the respondents who did not drink pre-disaster were likely to become new drinkers post-disaster if they had more sleep problems and more severe traumatic symptoms. Those who did not have a drinking habit before the disaster may have begun consuming alcohol to cope with their psychological reactions, such as sleep difficulties or traumatic symptoms. Previous studies show that traumatic experiences and other stressors could lead to higher levels of alcohol consumption9-12) and, furthermore, sleep difficulties are often identified as a significant risk for problematic drinking14,15). The present study also revealed that those who had high traumatic responses and/or sleep difficulties were considered to be vulnerable to alcohol misuse, consistent with findings obtained from past studies. Considering that posttraumatic stress responses are more likely to cause sleep difficulties – including nightmares relating to traumatic events – in order to prevent affected people from starting or restarting problem drinking after a disaster, we firstly need to provide adequate care and psychoeducation for those experiencing traumatic events during disasters.
As is well known, habitual drinking generally contributes to physical illnesses (e.g., diabetes, hypertension, and alcoholic hepatitis) and other mental health issues (e.g., depression, dementia, violence, and suicide)27). In Fukushima Prefecture, the standardized suicide mortality ratio decreased in the first two years after the disaster but increased in the third year after the disaster28) and the number of disaster-related suicide cases was remarkably larger than that in other areas affected mainly by the tsunami, such as coastal Miyagi and Iwate Prefectures29). Evidently, urgent countermeasures to prevent suicide are needed in Fukushima30). Given the significant relationship between suicide and alcohol abuse27), discouraging people from heavy drinking habits can be highly beneficial, especially for the prevention of suicide.
In addition, this study showed that smoking was significantly associated with starting drinking. In previous studies, being a male, being younger, having less educational attainment, changing jobs, and having traumatic symptoms were significantly associated with starting smoking31). Both studies show that those who begin addictive behavior, i.e., drinking and smoking, share very similar characteristics.
As described above, becoming a new drinker was correlated with age and gender, and younger males may be prone to developing new, yet ineffective, coping strategies, such as heavy drinking, to face their difficulties. Introducing preventive approaches through medical professionals for this potentially high-risk group can be challenging, since they do not develop physical illnesses requiring medical attention or take health check-ups to the extent of older cohorts32). A study revealed that young people are especially vulnerable to alcohol marketing33). Therefore, collaborative efforts with the media and alcohol industry, involving various types of educators, could complement other measures to approach this group effectively.
Limitations
This study has several limitations. First, it is critical to point out that this study only assessed drinking status pre-disaster by inquiring about drinking patterns prior to disaster;therefore, this survey did not allow us to distinguish between those who experienced post-disaster relapses following previously remitted disorders from those who did not have a drinking habit pre-disaster or those who were continuing to drink heavily. Secondly, as this study employed a cross-sectional design, it limited the identification of risk factors and clarification of causality. Thirdly, the representativeness of the study could be limited since only about 40% of the study population responded to this survey, and thus, a significant number of evacuees did not participate. Lastly, owing to exclusion criteria, more than 20% of the potential sample size was lost to missing data, and we need to acknowledge the level of incompleteness when interpreting results.
Conclusion
According to the present results, newly developed problem drinking was related to accumulated sleep problems and more severe traumatic symptoms. Experiences of disaster, except loss of family or relatives and changing jobs, were not significantly related to the problem. The relationships of sleep problems, traumatic symptoms, disaster experiences, and changes in drinking behavior have been quite well researched. However, there has been no previous study on new drinkers. With its large sample size, this survey enabled us to analyze the behavioral change that occurred in those who had recently become problematic drinkers and to examine how this was associated with other factors.
Prospective longitudinal research is strongly needed to monitor behavioral changes over a longer period to establish causality among factors such as problem drinking and sleep problems.
Conflict of Interest: None declared.
List of abbreviations
AIS: Athens Insomnia Scale
NPP: The Fukushima Daiichi Nuclear Power Plant
PCL-S: PTSD Checklist - Specific
Declaration
Ethics approval and consent to participate:
This study was approved by the ethics review committee of Fukushima Medical University on September 15th, 2015. The approval number is 1316. Informed consent was documented in writing upon entry in the study.
Consent to publish:
Not applicable.
Availability of data and materials:
Data that support the findings of this study are available from Fukushima Prefecture but restrictions apply to its access;our use was granted specifically for the current study, beyond which the data are not publicly available, but access may be granted from the authors upon reasonable request and with permission of Fukushima Prefecture.
Competing interests:
None declared.
Funding:
No funding was received.
Authors’ Contributions:
AY made substantial contributions to the conception, clinical interpretation of results, and manuscript writing. MM and YS made substantial contributions to the conception, clinical interpretation of results, and manuscript writing. HY, SY, SN, TO, AO, HM, MH, HN and MA made substantial contributions to study design, clinical interpretation of results and study conduct. All authors read and approved the final manuscript.
Acknowledgements
We thank the chairpersons of the Fukushima Health Management Survey Group for conducting this survey and their support efforts: Kenji Kamiya (Director, Radiation Medical Science Center for the Fukushima Health Management Survey), Shunichi Yamashita (Vice Director, Radiation Medical Science Center for the Fukushima Health Management Survey), Makoto Akashi (National Institute of Radiological Sciences), Kazunori Kodama, and Kotaro Ozasa (The Radiation Effects Research Foundation).
We also express our deepest gratitude for the work by other expert committee members, advisors, and staff of the Mental Health and Lifestyle Survey of the Fukushima Health Management Survey: Ohtsura Niwa, Shiro Matsui, Shuntaro Itagaki, Itaru Miura, Hajime Iwasa, Yoko Nakayama, Mitsuru Hisata, Norito Kawakami, Mitsuyoshi Hosoya, Yu-ichi Oikawa, Yuka Ueda, and Naoko Horikoshi.
References
- 1.Wu HC, Chou FH, Su CY, Tsai KY, Ou-Yang WC, Su TT. Survey of quality of life and related risk factors for a Taiwanese village population 3 years post-earthquake. Aust NZJ Psychiatry, 40: 355-361, 2006. doi: 10.1080/j.1440-1614.2006.01802.x. [DOI] [PubMed] [Google Scholar]
- 2.Suzuki Y, Tsutsumi A, Fukasawa M, Honma H, Someya T, Kim Y. Prevalence of Mental Disorders and Suicidal Thoughts among Community-Dwelling Elderly Adults 3 Years after the Niigata-Chuetsu Earthquake. J Epidemiol, 21: 144-150, 2011. doi: 10.2188/jea.JE20100093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shinfuku N. Disaster mental health: Lessons learned from the Hanshin Awaji earthquake. World Psychiatry, 1: 158-159, 2002. [PMC free article] [PubMed] [Google Scholar]
- 4.Norris FH, Friedman MJ, Watson PJ, et al. 60,000 disaster victims speak: part I. An empirical review of the empirical literature, 1981-2001. Psychiatry, 65: 207-239, 2002. [DOI] [PubMed] [Google Scholar]
- 5.Tracy M, Norris FH, Galea S. Differences in the determinants of posttraumatic stress disorder and depression after a mass traumatic event. Depress Anxiety, 28: 666-675, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Grievink L, van der Velden PG, Stellato RK, Dusseldorp A, Gersons BP, Kleber RJ, Lebret E. A longitudinal comparative study of the physical and mental health problems of affected residents of the firework disaster Enschede, The Netherlands. Public Health, 121(5): 367-374, 2007. Epub 2007 Feb 23. [DOI] [PubMed] [Google Scholar]
- 7.Kunii Y, Suzuki Y, Shiga T, Yabe H, Yasumura S, Maeda M, et al. Severe psychological distress of evacuees in evacuation zone caused by the Fukushima Daiichi Nuclear Power Plant accident: the Fukushima Health Management Survey. PLoS One, 11(7): e0158821, 2016. doi: 10.1371/journal.pone.0158821. eCollection 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.National Hospital Organization Kurihama Medical and Addiction Center [Internet]. Saigaigo no inshu ni kansuru evidence [Evidence on drinking behavior after disaster] [cited 2016 June 12]. Available from: http://www.kurihama-med.jp/shinsai/1_saigaigo.pdf. [Google Scholar]
- 9.Beaudoin CE. Hurricane Katrina: addictive behavior trends and predictors. Public Health Rep, 126(3): 400-409, 2001. doi: 10.1177/003335491112600314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cerdá M, Tracy M, Galea S. A prospective population based study of changes in alcohol use and binge drinking after a mass traumatic event. Drug Alcohol Depend, 115(1-2): 1-8, 2011. doi: 10.1016/j.drugalcdep.2010.09.011. Epub 2010 Oct 24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Keyes KM, Hatzenbuehler ML, Hasin DS. Stressful life experiences, alcohol consumption, and alcohol use disorders: the epidemiologic evidence for four main types of stressors. Psychopharmacology (Berl), 218(1): 1-17, 2011. doi: 10.1007/s00213-011-2236-1. Epub 2011 Mar 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Flory K, Hankin BL, Kloos B, Cheely C, Turecki G. Alcohol and cigarette use and misuse among Hurricane Katrina survivors: psychosocial risk and protective factors. Subst Use Misuse, 44(12): 1711-1724, 2009. doi: 10.3109/10826080902962128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.North CS, Ringwalt CL, Downs D, Derzon J, Galvin D. Postdisaster course of alcohol use disorders in systematically studied survivors of 10 disasters. Arch Gen Psychiatry, 68(2): 173-180, 2010. doi: 10.1001/archgenpsychiatry.2010.131. Epub 2010 Oct 4. [DOI] [PubMed] [Google Scholar]
- 14.Brower KJ. Insomnia, self-medication, and relapse to alcoholism. Am J Psychiatry, 158(3): 399-404, 2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhabenko N, Wojnar M, Brower KJ. Prevalence and correlates of insomnia in a Polish sample of alcohol-dependent patients. Alcohol Clin Exp Res, 36(9): 1600-1607, 2012. doi: 10.1111/j.1530-0277.2012.01771.x. Epub 2012 Apr 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Volpicelli J, Balaraman G, Hahn J, Wallace H, Bux D. The role of uncontrollable trauma in the development of PTSD and alcohol addiction. Alcohol Res Health, 23(4): 256-262, 1999. [PMC free article] [PubMed] [Google Scholar]
- 17.Ueda Y, Yabe H, Maeda M, Ohira T, Fujii S, Niwa S, et al. Drinking behavior and mental illness among evacuees in Fukushima following the Great East Japan Earthquake: the Fukushima Health Management Survey. Alcohol Clin Exp Res, 40(3): 623-630, 2016. doi: 10.1111/acer.12984. Epub 2016 Feb 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yasumura S, Hosoya M, Yamashita S, Kamiya K, Abe M, Akashi M, et al. Study Protocol for the Fukushima Health Management Survey. Journal of Epidemiology, 22(5): 375-383, 2012. doi: 10.2188/jea.JE20120105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yabe H, Suzuki Y, Mashiko H, Nakayama Y, Hisata M, Niwa S, et al. Psychological distress after the Great East Japan Earthquake and Fukushima Daiichi Nuclear Power Plant accident: results of a mental health and lifestyle survey through the Fukushima Health Management Survey in FY2011 and FY2012. Fukushima J Med Sci, 60(1): 57-67, 2014. [DOI] [PubMed] [Google Scholar]
- 20.Fukushima Prefecture. [Handout #4 for The 10th Prefectural Oversight Committee Meeting for the Fukushima Health Management Survey: report on mental health lifestyle survey] [cited 2016 June 12]. Available from: http://www.pref.fukushima.lg.jp/uploaded/attachment/6457.pdf. Japanese. [Google Scholar]
- 21.Okajima I, Nakajima S, Kobayashi M, Inoue Y. Development and validation of the Japanese version of the Athens Insomnia Scale. Psychiatry Clin Neurosci, 67(6): 420-425, 2013. doi: 10.1111/pcn.12073. Epub 2013 Aug 5. [DOI] [PubMed] [Google Scholar]
- 22.Iwasa H, Takebayashi Y, Suzuki Y, Yagi A, Zhang W, Harigane M, et al. Psychometric evaluation of the simplified Japanese version of the Athens Insomnia Scale: The Fukushima Health Management Survey. J Sleep Res, e12771, 2018. doi: 10.1111/jsr.12771. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Blanchard EB, Jones-Alexander J, Buckley TC, Forneris CA. Psychometric properties of the PTSD checklist (PCL). Behavioral Research & Therapy, 34: 669-673, 1996. [DOI] [PubMed] [Google Scholar]
- 24.Suzuki Y, Yabe H, Horikoshi N, Yasumura S, Kawakami N, Ohtsuru A, et al. Diagnostic accuracy of Japanese posttraumatic stress measures after a complex disaster: The Fukushima Health Management Survey. Asia Pac Psychiatry, 9(1), 2017. doi: 10.1111/appy.12248. Epub 2016 Aug 9. [DOI] [PubMed] [Google Scholar]
- 25.Lin Y, Kikuchi S, Tamakoshi A, Wakai K, Kawamura T, Iso H, et al. Alcohol consumption and mortality among middle-aged and elderly Japanese men and women. Ann Epidemiol, 15(8): 590-597, 2005. Epub 2005 Jan 23. [DOI] [PubMed] [Google Scholar]
- 26.Tokyo Fire Department. [Acute alcohol intoxication is your own concern] [cited 2017 January 9]. Available from: http://www.tfd.metro.tokyo.jp/lfe/kyuu-adv/201312/chudoku/. Japanese. [Google Scholar]
- 27.Pompili M, Serafini G, Innamorati M, Dominici G, Ferracuti S, Kotzalidis GD, et al. Suicidal Behavior and Alcohol Abuse. Int J Environ Res Public Health, 7(4): 1392-1431, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ohto H, Maeda M, Yabe H, Yasumura S, Bromet EE. Suicide rates in the aftermath of the 2011 earthquake in Japan. The Lancet, 385(9979): 1727, 2015. doi: http://dx.doi.org/10.1016/S0140-6736(15)60890-X. [DOI] [PubMed] [Google Scholar]
- 29.Cabinet Office, Government of Japan. Higashi nihon daishinsai ni kanrensuru jisatsushasuu, Heisei 27 nen [Number of suicides related to Great East Japan Earthquake, 2015]. 2016 August 31. Available from: http://www.mhlw.go.jp/file/06-Seisakujouhou-12200000-Shakaiengokyokushougaihokenfukushibu/h27kakutei-shinsai_3.pdf. [Google Scholar]
- 30.Maeda M, Oe M, Bromet E, Yasumura S, Ohto S. Fukushima, mental health and suicide. J Epidemiol Community Health, 2016. doi: 10.1136/jech-2015-207086. [DOI] [PubMed] [Google Scholar]
- 31.Nakano H, Ohira T, Maeda M, Yabe H, Ohtsuru A, Suzuki Y, et al. Associations of disaster-related and psychosocial factors with changes in smoking status after a disaster: a cross-sectional survey after the Great East Japan Earthquake. BMJ Open, 8(6): e018943, 2018. doi: 10.1136/bmjopen-2017-018943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ministry of Health, Labour and Welfare. [Health, labour and welfare whitepaper, 2014] [Cited 2017 January 10]. Available from: http://www.mhlw.go.jp/wp/hakusyo/kousei/14/dl/1-02-1.pdf. Japanese. [Google Scholar]
- 33.Babor TF, Robaina K, Noel JK, Ritson EB. Vulnerability to alcohol-related problems: a policy brief with implications for the regulation of alcohol marketing. Addiction, 2016. doi: 10.1111/add.13626. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data that support the findings of this study are available from Fukushima Prefecture but restrictions apply to its access;our use was granted specifically for the current study, beyond which the data are not publicly available, but access may be granted from the authors upon reasonable request and with permission of Fukushima Prefecture.