

1. Introduction
Although age-related chronic illnesses increase exponentially after age 60 (Belikov, 2019), some individuals demonstrate relatively early onset of chronic illness whereas others stave off serious illness well into their 90s (Aishire, Beltran, and Crimmins, 2014). In an attempt to increase healthy aging, medical research has largely focused on identifying causes and treatments for the various diseases of old age. Indeed, this has been the emphasis of the National Institutes of Health as each Institute concentrates on a particular set of diseases (cancer, diabetes, coronary heart disease, dementia, etc.). Increasingly, however, it has become apparent that to increase the span of health (i.e., delay the onset of age related chronic illnesses) requires that we devote more and better research to understanding the basic biology of aging (Kennedy et al. 2014). A few years ago, the NIH Advances-in-Geroscience conference observed that: “The major diseases causing morbidity and mortality have one root cause in common – aging” (Kennedy 2013). This reality argues for more research on the factors, including social factors, that accelerate or decelerate biological aging (Johnson and Acabchuk, 2018; Kennedy et al. 2014; Moffitt et al. 2017).
It is especially important that African American samples be included in such investigations given both their exposure to high levels of stress and disadvantage and their risk for early chronic illness and mortality (Geronimus et al. 2016; Phelan and Link, 2015). Geronimus and her colleagues (Geronimus, 2001; Geronimus and Thompson, 2004; Geronimus et al., 2006; Williams, 2012) use the weathering hypothesis to link these two phenomena. This hypothesis posits that the health inequality suffered by Black Americans is a consequence of institutional racism and the cumulative impact of life in a society where they suffer social, economic, and political exclusion. Although health risk factors such as diet, exercise, and alcohol consumption are seen as having some significance, the fundamental explanation for heath inequalities in the U.S. is seen as the racial divide where Black Americans occupy a marginalized, stigmatized, subordinate status in relation to Whites. The weathering hypothesis views the elevated rates of illness, disability, and mortality seen among Black Americans as a physiological response to the structural barriers, material hardships, stereotypes, and other threats to one’s identity that comprise the Black experience (Geronimus and Thompson, 2004; Geronimus et al., 2016). In other words, the stressors associated with living in a racially charged society give rise to accelerated aging which, in turn, leads to early onset of chronic illness and premature death. The present study tests the weathering hypothesis by examining the link between types of social adversity frequently experienced by Black Americans and accelerated aging
Our investigation uses the newly developed GrimAge index of accelerated biological aging as an indicator of weathering (Lu et al., 2019). This index is an epigenetic measure based upon methylation marks at 1,030 sites scattered throughout the DNA methylome. Findings show it to be a strong predictor of both morbidity and mortality (Lu et al., 2019). Indeed, recent research suggests that it is a more robust predictor of a wide variety of biomarkers of health and of time to death than other epigenetic measures of accelerated aging (Hillary et al. 2020; Lu et al. 2019). Using a sample of 494 middle-age Black Americans, we explore whether low education, limited income, neighborhood disadvantage, and discrimination are associated with accelerated aging, and the extent to which any impact of these social variables on speed of aging is mediated by health risk behaviors such as diet, exercise, and alcohol consumption.
1.1. Accelerated Biological Aging as an Indicator of Weathering
Geronimus and colleagues define weathering as the physiological wear and tear or deterioration that occurs in response to cumulative social and economic adversity and that then gives rise to early illness and death (Geronimus et al., 2006; Geronimus and Thompson, 2004). This deterioration, or accelerated aging, is viewed as a consequence of chronic stimulation of the sympathetic nervous system, the HPA axis, the endocrine system, and the various biological and methylation changes that they foster. While past research has used allostatic load (Geronimus et al. 2006) or inflammation (Simons et al., 2018) as indicators of weathering, recently various epigenetic indices have been developed specifically to assess accelerated aging.
Epigenetic regulation involves biochemical mechanisms that influence genome expression by either up regulating or down regulating particular genes. One of the most pervasive and well-studied of these mechanisms is methylation. This process occurs when a methyl group attaches to a segment of deoxyribonucleic acid (DNA) at a CpG site (i.e., a DNA region where a cytosine nucleotide is positioned next to a guanine nucleotide separated by one phosphate), which causes the inhibition of gene expression. Since the 1960s, researchers have been aware of the strong association between age and DNA methylation (Koch and Wagner, 2011).
Such findings have spurred the development of various epigenetic indices of biological aging. These indices use blood leukocytes to assess the degree of methylation associated with CpG sites scattered throughout the human genome that correlate with age. The Hannum et al. index (2013) is based on 71 sites, the Horvath et al. index (2013) is based on 353 sites, and the Levine et al index (2018) is based on 513 sites. For all three of these measures the correlation between age and the weighted sum of methylation scores is roughly .80 -. 90 (Jyhava et al., 2017). Nearly all of the markers in these indices lay within or near genes with known functions associated with age-related conditions, including Alzheimer's disease, cancer, tissue degradation, DNA damage, and oxidative stress (Hannum et al., 2013; Horvath, 2013).
Importantly, these epigenetic indices can be used as “biological clocks” to assess, at any point during adulthood, the extent to which an individual is experiencing accelerated or decelerated biological aging. This can be done by calculating the discrepancy between a person’s chronological age and the age predicted using the epigenetic index. The resulting difference indicates, in number of years, the extent to which an individual is biologically older or younger than their chronological age (i.e., accelerated or decelerated aging). Importantly, several studies have reported a modest association between these indices and both morbidity and mortality (Fransquet, Wriggesworth, Woods, Ernst, and Ryan, 2019: Jyhava et al., 2017).
Recently, however, a new epigenetic index has been developed using methylation at 1,030 sites (Lu et al., 2019). In contrast to other epigenetic measures, the GrimAge Index was formulated by identifying methylation signatures associated with seven plasma proteins known to be involved in age-related diseases plus pack years of smoking. The index is labeled GrimAge after the Grim Reaper because an accelerated score is grim news (Lu et al., 2019). Like its predecessors, the residuals obtained by regressing GrimAge on chronological age indicate the extent to which an individual is experiencing accelerated/decelerated aging. This instrument has been shown to be superior to other biological clocks in terms of predicting morbidity and mortality (Hillary et al. 2020, Lu et al. 2019). It shows, for example, strong associations with shorter life span, coronary heart disease, diabetes, and co-morbidity, four health outcomes more common among African Americans. Further, it should be noted that GrimAge has been validated with a large African American sample (Lu et al., 2019). Together, these various findings indicate that GrimAge is a robust indicator of speed of aging.
1.2. African Americans and Exposure to Social Adversity
The weathering hypothesis contends that African Americans face a variety of adverse conditions and circumstances that accelerate biological aging and risk for chronic illness. These difficult challenges include, among other things, socioeconomic disadvantage, residing in an impoverished neighborhood, and exposure to personal discrimination.
One of the more powerful predictors of early onset of chronic illness and mortality is socioeconomic status, particularly low income and education (Cockerham, Hamby, and Oates, 2017). This association holds in every country where data are available (Mormot, 2004, 2015). One of the consequences of institutional racism is that Black Americans suffer lower levels of education and income. Nationwide, a quarter of Black students attend schools that fail to offer necessary college preparatory courses (U.S. Department of Education, 2014). Further, the college dropout rate is higher for Black Americans than any other racial/ethnic group and even when they earn a degree their unemployment rate is two-thirds higher and their salary substantially lower than that of White graduates (Brown, 2019). Economically, approximately 1/3 of Black families live near or below the poverty line, and the ratio of Black to White median family income has remained constant (roughly 56%) since the late 1960s (Manduca, 2018), although Whites generally assume that the ratio is roughly 80%. Differences in wealth are even more dramatic as median wealth for White families is 10 times that of Black families (Kijakazi, 2019). Thus Black Americans are much more likely than other ethnic groups to experience chronic economic hardship (Massey, 2007). The weathering hypothesis would suggest that the low education and income that plagues many African Americans likely causes them to experience accelerated aging.
In addition to low education and limited income, African Americans are much more likely to live in a disadvantaged neighborhood (viz., concentrated poverty, low education, high rates of unemployment and single-parent families; Sampson, 2012). More than half of all Black metropolitan residents live in highly segregated, disadvantaged neighborhoods; indeed, no other group in the history of the U.S. has experienced the degree of segregation that has been forced upon Black Americans (Massey, 2017; Sampson, 2012; Wilson, 1987). Blacks in the top quintile of the income distribution often continue to live in neighborhoods with high crime and disorder (Intrator, Tannen, and Massey 2016). Residential segregation is a consequence, in large measure, of institutionalized prejudice and discrimination in the real estate and banking industries, including practices such as profiling, redlining and selective marketing (Massey, 2007). The weathering hypothesis would suggest that the challenges and frustrations of living in a disadvantaged neighborhood likely accelerates biological aging.
Finally, Black Americans often experience incidents of personal discrimination, ranging from subtle insults to flagrantly racist incidents such as harassment by police. While most Americans think of themselves as “color blind”, job application studies (Pager, Bonifkowski and Western, 2009; Gaddis, 2015) and implicit bias research (Sawyer and Gamp, 2018) continues to document much prejudice and discrimination. Exposure to such treatment might be expected to accelerate biological aging.
Based on this literature, it seems reasonable to expect that low income and education, exposure to incidents of personal discrimination, and living in a disadvantaged neighborhood each make a unique contribution to the accelerated aging of African Americans. Although the evidence is limited, prior research provides at least some support for this idea. Past studies have reported that accelerated aging is associated with economic hardship (Simons et al., 2016), living in a disadvantaged neighborhood (Lei et al., 2019), racial discrimination (Brody et al. 2016), and cumulative stress (Zannis et al., 2015). While all of these studies were based on African American samples, they used first-generation measures of accelerated aging (i.e., the Horvath and Hannum indices). Further, each of them focused on a single type of disadvantage without controlling for others.
Given how recently GrimAge was developed, there has been little examination of the extent to which it is associated with social stressors and disadvantage. Using a largely white European sample, Lu et al. (2019) reported significant zero-order correlations between GrimAge and both income and education but no controls were included in their analyses. And, Zhao et al. (2019) found a significant effect for education after controlling for gender and various health behaviors, but their model did not include income, neighborhood disadvantage, or discrimination. Thus, there is a need for research that examines the multivariate effect of various types of disadvantage on GrimAge.
1.3. The Present Study
Using multivariate analysis and GrimAge as an indicator of accelerated aging, the present study investigates the extent to which education, income, neighborhood disadvantage, and exposure to racial discrimination each have a unique effect on biological aging. Further, in addition to investigating the unique effects of each of these four measures of adversity, we also examine their combined effect. The four adversity variables are summed to form a summary index in order to assess the extent to which cumulative social disadvantage is associated with GrimAge.
Having established associations between our measures of adversity and GrimAge, we investigate the extent to which these effects are mediated by health risk behaviors. It may be that one or more of the four adversity measures, or the index of cumulative social disadvantage, elevate speed of aging by increasing the probability of an unhealthy lifestyle. Specifically, we examine whether diet, exercise, or patterns of alcohol consumption are related to accelerated aging and mediate the effects of any of our adversity measures. Lu et al. (2019) reported zero-order correlations between GrimAge and both exercise and alcohol consumption, but they did not investigate whether these variables accounted for the effects of either of the SES measures in their data – income and education. On the other hand, Zhoa et al. (2019) found that alcohol consumption, but not exercise, was related to GrimAge. Their multivariate analysis, however, indicated that controls for alcohol consumption did little to reduce the effect of education, the only social variable included in their study. Thus there is a need for further exploration of the potential mediating effects of lifestyle variables.
The weathering hypothesis, as noted above, asserts that any such effects are likely to be small. It grants that these health risk behaviors may exert some effect on weathering, but avers that the primary cause of weathering and the poor health of Black Americans is the adverse circumstances that accrue as a result of living in a racially charged society. The present study evaluates this contention.
2. Methods
2.1. Participants and Procedures
We investigated our research questions using data collected at Waves 4 and 5 from the caregivers in the Family and Community Health Study (FACHS). FACHS is a longitudinal study of several hundred African American families that was initiated in 1997. All of the families had a 5th grader at study inception. Using a stratified random sampling procedure, the sampling strategy was intentionally designed to generate families representing a range of socioeconomic statuses and neighborhood settings. Details regarding recruitment are described by Gibbons and colleagues (2004) and Simons and colleagues (2011). At Wave 1, about half of the sample resided in Georgia (n = 422) and the other half in Iowa (n = 467). The 4th and 5th Waves of data were collected in 2005 and 2008, respectively. Mean caregiver age at wave 5 was 48.47 years (SD = 9.23), 17.82% had less than a 12th grade education, and 24.8% were married. The majority (68.5%) lived in large urban areas, 12.2% lived in the suburbs, and 19.3 lived in rural areas.
Of the caregivers interviewed at Wave 1, 77% were interviewed again at Wave 5. Within two weeks of the wave 5 psychosocial interview, a certified phlebotomist visited the home and collected four tubes of blood (30 ml) from each consenting participant. Given the logistics of scheduling home visits by phlebotomists, only members of the sample still residing in Georgia or Iowa at wave 5 were identified as eligible for the blood draw. Roughly, 80% of these individuals agreed to provide blood: 377 women and 129 men. Comparisons of these caregivers with those who did not provide blood did not reveal any significant differences with regard to either demographic characteristics or the independent variables (e.g., household income, education, or chronological age) at the initial wave of the FACHS study. The only exception was diet. Caregivers who gave blood had a slightly poorer diet than those who did not. After missing data were handled by multiple imputation (Sidi & Harel, 2018), complete data were available for 506 respondents (129 men and 377 women). Rates of missing data ranged from 1.19% for neighborhood disadvantage to 2.17% for binge drinking.
The phlebotomist drew four tubes of blood (30 ml) from each participant; these were shipped on the same day to a laboratory for preparation. Upon receipt, the blood tubes were inspected to ensure anticoagulation and aliquots of blood were diluted 1:1 with phosphate buffered saline (pH 8.0). Mononuclear cell pellets were separated from the diluted blood specimen using a centrifuge with ficoll (400 g, 30 min). The mononuclear cell layer was removed from the tube using a transfer pipette, re-suspended in a phosphate buffered saline solution, and briefly centrifuged again. The resulting cell pellet was re-suspended in a 10% DMSO/RPMI solution and frozen at 8.0 Celsius until use.
The Illumina Infinium HumanMethylationEPIC 850 BeadChip was used to assay genome-wide DNA methylation. Participants were randomly assigned to 16 sample “slides/chips” with groups of eight slides being bisulfite converted in a single plate, resulting in two “batches/plates.” A replicated sample of DNA was included in each plate to aid in assessment of batch variation and to ensure correct handling of specimens. Prior to normalization, methylation data were filtered based on these criteria: (a) samples containing 1% of CpG sites with detection p < .05 were removed, (b) sites were removed if a bead count of < 3 was present in 5% of samples, and (c) sites with a detection p < .05 in 1% of samples were removed. The methylation data was then used to calculate a GrimAge score for each participant through a public online tool (https://dnamage.genetics.ucla.edu/).
2.2. Measures
2.2.1. Outcome variable
Accelerated Epigenetic Aging.
We assessed epigenetic aging using the GrimAge index (Lu et al., 2019). This index estimates an individual’s biological age based on methylation assessments at 1,030 sites scattered across the human genome. In the study sample, GrimAge was correlated .78 with chronological age. To transform GrimAge into an accelerated aging score, we regressed GrimAge on chronological age (Lu et al., 2019). The result is that this measure of accelerated epigenetic aging is adjusted to correlate with chronological age at 0. A positive value on this variable indicates, in years, accelerated epigenetic aging, while a negative value indicates, in years, decelerated aging. As noted above, the GrimAge measure of accelerated aging has been shown to be a more robust predictor of morbidity and mortality than the other epigenetic clocks currently available (Lu et al., 2019).
2.2.2. Predictor variables
Education.
At Wave 4, respondents were asked to report the number of years of education that they had completed. Responses could range from 1 (1st grade) to 20 (doctoral degree), although no one reported completing less than 7th grade.
Income.
Respondents reported on their household income in the past year from all family members and all sources at Wave 4. Categorical response options ranged in roughly $5,000 increments from 0 (none), 1 (less than $10,000), 2 ($10,000 to $14,999) to 15 ($200,000 or more). Total household income was based on the mid-point of these categories. Family per capita income was calculated by dividing the total household income by the number of family members.
Neighborhood disadvantage.
Neighborhood disadvantage was measured at Wave 4 using the data from the U.S. Census Bureau’s American Community Survey 5-Year Estimates (2006-2010), which was mapped onto the geocodes for our study participants’ residential addresses in 2007 (Lei et al., 2019). Following previous studies (Sampson, Raudenbush, & Earls, 1997), the scale consisted of the following items: median household income (reverse coded), the percentage unemployed, percent of residents below the poverty threshold, the percentage of residents with less than a high school degree, the percentage of female-headed households, and the percentage of those receiving public assistance. The six items were standardized and averaged. A higher score represented a more disadvantaged neighborhood. Coefficient alpha for the measure was .87.
Racial discrimination.
At Waves 4, respondents completed 13 items from the Schedule of Racist Events (Landrine & Klonoff, 1996). This instrument has strong psychometric properties and has been used extensively in studies of African Americans (Brody et al, 2006; Burt, Simons, & Gibbons, 2012; Simons et al., 2002). The items assess the frequency (1 = never, 4 = several times) with which various discriminatory events have been experienced in the past year. The items focus, for example, on being the victim of racial slurs, being hassled by the police, disrespectful treatment by sales clerks, false accusations by authority figures, and exclusion from social activities because of being African American. Coefficient alpha for the scale was .934.
Cumulative social disadvantage.
The variables education (reverse coded), per capita income (reverse coded), disadvantaged neighborhood, and discrimination were standardized and summed to form an index of cumulative social disadvantage at Wave 4.
2.2.3. Health risk behaviors.
We used three measures to assess health risk behaviors: regular exercise, healthy diet, and alcohol consumption. Each of these measures was assessed at Wave 5. Unfortunately, Wave 4 assessments for these variables were not available.
Exercise.
Exercise was assessed by an item that asked, “On average, how often do you exercise?” with responses ranging from 1 (never) to 4 (regularly). Such single-item measures of exercise have been shown to perform as well as other short physical activity measures in terms of reliability and concurrent validity (Milton, Bull, and Bauman, 2011), including biomarkers of physical activity such as body-mass index and psychosomatic symptoms (Li, Carlson, and Holm, 2000).
Diet.
Diet was assessed using a three-item scale that asked respondents to report how often in the past seven days (1 = never, 4 = regularly) that they: 1) eat fruits and vegetables)? 2) eat fatty foods like potato chips or ice cream? (reverse coded); and 3) eat fast food? (reverse coded). Scores were averaged to form a measure of healthy diet. Coefficient alpha was .73. Past research indicates that such ratings show significant associations with more burdensome assessments of dietary intake and with biomarkers such as blood pressure and body mass index (Adjoian, Firestone, Eisenbower, and Yi, 2016; Loftfield, Yi, Immerwahr, and Eisenhower, 2015).
Alcohol Consumption.
Respondents were asked to report how often they had had three or more drinks (a glass of wine, a wine cooler, a bottle or can of beer, a shot glass of liquor or a mixed drink) in a sitting during the past 12 months. Responses ranged from 1 (never) to 6 (every day).
2.2.4. Controls.
We control for two variables. First, consonant with the finding that males demonstrate earlier onset of morbidity and death, virtually all studies find that males show higher levels of accelerated aging than females (Zhao el at., 2019). We expect that this will be the case in the current study as well. Thus we included a gender variable coded males = 1 and females = 0. Second, we control for marital status given that being married has been shown to be an important source of social support and may therefore that reduce speed of aging. This variable was coded married = 1 and not married = 0.
2.3. Analytic Approach
Our analyses employ hierarchical regression (Muthén and Muthén, 2015) to address our research questions. First, we regress accelerated aging on the four types of disadvantage, including controls for gender and marital status. Second, we regress accelerated aging on the health risk behaviors. Third, we examine a model that includes all of the study variables as predictors in order to test the extent to which the health risk behaviors reduce (mediate) the effects of the types of disadvantage and gender on accelerated aging. Finally, we examine the extent to which cumulative disadvantage (a composite measure combining education, income, discrimination, and neighborhood disadvantage) predicts accelerated aging after controlling for health risk behaviors, gender, and marital status.
Importantly, our sample included 91 married couples. As a result, the error terms in our regression models may not be independent, thereby leading to an underestimation of standard errors. To avoid this problem, we adjust our standard errors using regression with cluster-robust standard errors (Aronow, Samii, & Assenova, 2015).
3. Results
Descriptive statistics for the study variables are presented in Table 1. All of the study variables show substantial variation. For example, 18% had less than a high school degree but 29% had some college and 14% had a BA or more. Average per capita income is roughly $12,000 but the standard deviation is $12,500. The correlation matrix for the study variables is presented in Table 2. Given the focus of this paper, the most relevant correlations are those presented in column 1 between accelerated aging and the other variables. All of the disadvantage variables (education, income, discrimination, and neighborhood disadvantage), as well as the cumulative disadvantage index, show significant associations with accelerated aging. Of the health risk behaviors, only alcohol consumption is related to accelerated aging. Further, consonant with the fact that men tend to suffer earlier onset of chronic illness and mortality, Table 1 shows that being male is rather strongly associated with accelerated aging.
Table 1.
Descriptive statistics for the study variables
| Variables | % or Mean (SD) |
|---|---|
| Accelerated Grim aging, Mean (SD) | .020 (4.730) |
| Education, % | |
| <12th Grade | 18.2% |
| High school graduate or GED | 39.7% |
| Some college or associate degree | 28.5% |
| Bachelor’s degree | 9.7% |
| Postgraduate | 4.0% |
| Per capita income, Mean (SD) | 12346.900 (12477.090) |
| Racial discrimination, Mean (SD) | 1.807 (.668) |
| Neighborhood disadvantage, Mean (SD) | .000 (1.000) |
| Marriage, % | 38.7% |
| Males, % | 25.5% |
| Healthy diet, Mean (SD) | 2.6 (.649) |
| Fruits and vegetables, % | |
| Never | 15.2% |
| Only occasionally | 27.5% |
| Frequently | 29.5% |
| Regularly | 27.8% |
| Fatty foods, % | |
| Never | 5.9% |
| Only occasionally | 47.3% |
| Frequently | 29.8% |
| Regularly | 17.0% |
| Fast foods, % | |
| Never | 10.1% |
| Only occasionally | 51.5% |
| Frequently | 29.3% |
| Regularly | 9.1% |
| Binge drinking, Mean (SD) | 1.305 (.665) |
| Never, % | 73.7% |
| Less than 1 time a week, % | 19.0% |
| 1 to 2 times a week, % | 3.8% |
| 3 to 4 times a week, % | 3.0% |
| 5 to 6 times a week, % | .2% |
| Every day, % | .2% |
| Exercise, Mean (SD) | 2.471 (1.033) |
| Never, % | 18.4% |
| Only occasionally, % | 38.8% |
| Frequency, % | 20.4% |
| Regularly, % | 22.4% |
Table 2.
Correlation matrix for the study variables (N = 506)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Accelerated GrimAge (W5) | — | |||||||||
| 2. Education (W4) | −.235** | — | ||||||||
| 3. Per capita income (W4) | −.149** | .423** | — | |||||||
| 4. Discrimination (W4) | .109* | .194** | .075† | — | ||||||
| 5. Neighborhood disadv (W4) | .138** | −.123** | −.179** | .066 | — | |||||
| 6. Cumulative disadv (W4) | .277** | −.606** | −.673** | .346** | .609** | — | ||||
| 7. Marriage | −.038 | .140** | .162** | .082† | −.008 | −.101* | — | |||
| 8. Males | .312** | −.051 | .131** | .123** | .007 | .027 | .342** | — | ||
| 9. Healthy diet (W5) | −.067 | .115* | .061 | .100* | −.035 | −.052 | −.014 | −.048 | — | |
| 10. Alcohol consump (W5) | .146** | −.082† | −.028 | −.033 | −.006 | .030 | −.096* | .206** | −.120** | — |
| 11. Exercise (W5) | .041 | .112* | .096* | .140* | −.017 | −.039 | .163** | .242** | .190** | −.001 |
Note: Point-biserial correlations are used to test the dichotomous variables marriage and males.
p ≤ .10;
p ≤ .05;
p ≤ .01 (two-tailed tests).
In addition to these correlations with aging, the table also reports a positive association between discrimination and income, in keeping with the argument that as Black Americans move into more prestigious occupational positions they are more likely to experience discriminatory treatment (Geronimus et al., 2016). Finally, the table shows that being male is associated with higher income, exercise, alcohol consumption, and healthy diet.
Table 3 presents the effects of regressing GrimAge on the various types of disadvantage and health risk behaviors. These results were obtained using regression modeling with cluster-robust standard errors to correct for the dependence in the data created by the fact that 91 of the men and women in the sample were married to each other. Model 1 only includes the four measures of disadvantage plus controls for marriage and gender. Consonant with the correlation matrix, all four of the social disadvantage constructs are significantly related to accelerated aging. As would be expected, the beta coefficients for education (β = −17) and income (β = −.094) are negative whereas they are positive for discrimination (β = .111) and neighborhood disadvantage (β= .090). Consistent with prior research, being male is also significantly association with accelerated aging (β = .344). Surprisingly, marriage, which had no effect at the zero-order level, emerges as significant when being male is entered into the model. This suppression effect appears to be a consequence of the fact that in the current data set males are more likely to be married, as well as to experience accelerated aging. Table 2 shows that being male is correlated .342 with being married. In follow up analyses, we found that the p-value for the regression of Grim Age on being married was .41 without gender in the model but .001 when gender was added. Thus once the association between being male and being married is taken into account, the negative effect of marriage on speed of aging emerges.
Table 3.
Regression modeling with robust standard errors examining the effects of social adversity and health behaviors on accelerated GrimAge
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|
| b | β | b | β | B | β | b | β | |
| Education (W4) | −.341** (.098) |
−.171 | −.333** (.099) |
−.167 | ||||
| Per capita income (W4) | −.001* (.00001) |
−.094 | −.001* (.00001) |
−.092 | ||||
| Racial discrimination (W4) | .789** (.294) |
.111 | .826** (.296) |
.117 | ||||
| Neighborhood disadvantage (W4) | .646* (.307) |
.090 | .646* (.308) |
.090 | ||||
| Cumulative disadvantage (W4) | 1.192** (.186) |
.252 | ||||||
| Marriage | −1.210** (.417) |
−.124 | −1.125** (.420) |
−.116 | −1.181** (.419) |
−.122 | ||
| Males | 3.731** (.465) |
.344 | 3.561** (.499) |
.328 | 3.634** (.492) |
.335 | ||
| Healthy diet (W5) | −.442 (.335) |
−.061 | −.222 (.307) |
−.030 | −.237 (.303) |
−.033 | ||
| Alcohol Consumption (W5) | .991** (.311) |
.139 | .371 (.289) |
.052 | .386 (.287) |
.054 | ||
| Exercise (W5) | .241 (.207) |
.053 | −.004 (.202) |
−.001 | −.020 (.202) |
−.004 | ||
| Constant | 2.878* (1.250) |
−.726 (1.030) |
2.813* (1.431) |
−.293 (.966) |
||||
| R-squared | .191 | .027 | .195 | .189 | ||||
Note: Unstandardized (b) and standardized coefficients (β) shown with robust standard errors in parentheses.
p ≤ .10,
p ≤ .05,
p ≤ .01 (two-tailed tests); N = 506.
Model 2 regresses accelerated aging on the health risk behaviors. The findings indicate that alcohol consumption increases accelerated aging whereas diet and exercise show no effect. Model 3 includes both the social disadvantage constructs and the health risk behaviors, plus marriage and gender as controls. Of particular interest is the extent to which controlling for the health risk behaviors reduces the impact of the social disadvantage variables and of being male or being married on accelerated aging. Such findings would suggest that an unhealthy life style explains (mediates) the impact of social disadvantage, being married, and gender on accelerated aging. It was unlikely, however, that such a pattern would be evident given that in Model 2 only one health risk behavior, alcohol consumption, showed a significant association with aging. Model 3 shows that all four of the social disadvantage variables, as well as gender and marriage, continue to exert a significant effect on accelerated aging, with the beta coefficients being roughly the same or slightly larger than those obtained in Model 1 which did not include the health risk factors. Thus there is no evidence of a mediating effect. Indeed, once the social disadvantage variables, gender, and marriage are taken into account alcohol consumption no longer has a significant effect on aging.
Model 4 shows a similar pattern of findings when the four adversity measures are combined to form a cumulative index. Cumulative disadvantage is significantly related to GrimAge (β =.252), as is being male (β = .335) and marriage (β = −.122), while none of the health risk behaviors show an effect. Figure 1 presents a graph depicting the association between the cumulative disadvantage index and GrimAge. It shows that a two standard deviation increase in cumulative disadvantage is associated with roughly a two and a half year acceleration in biological aging, whereas a two standard deviation decrease in cumulative disadvantage is associated with roughly a two and a half year deceleration in biological aging. The latter finding is important as it suggests that the combination of high education, high income, living in an advantaged neighborhood, and few experiences of discrimination may serve to decelerate biological aging.
Figure 1.
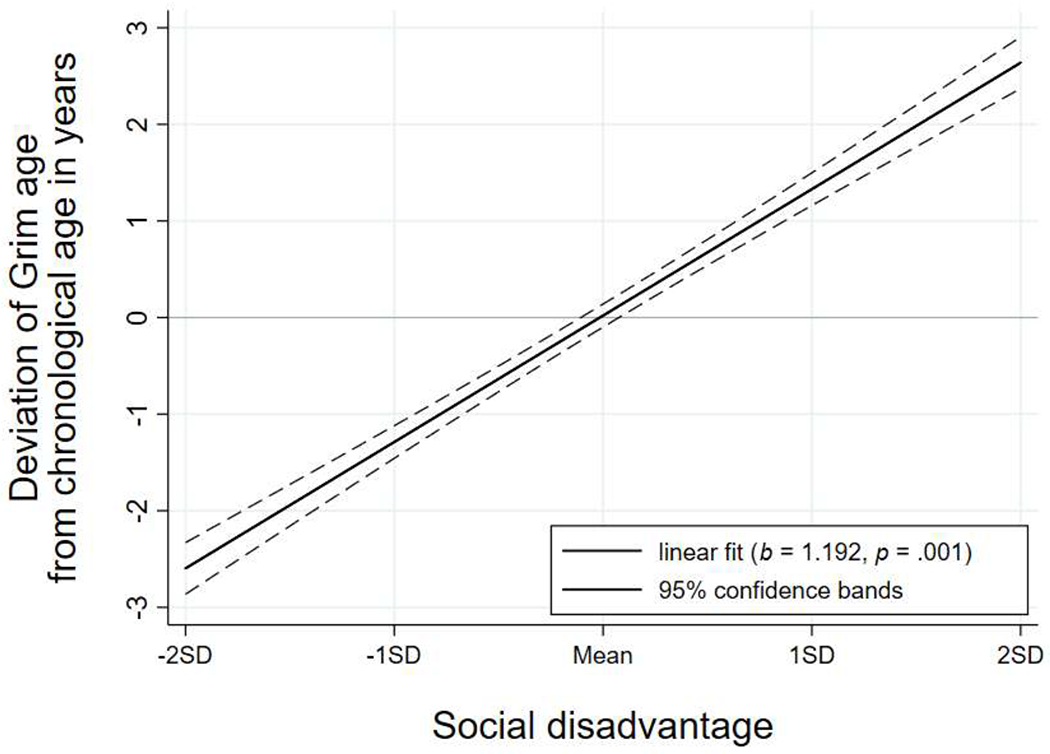
Graph depicting the association between the index of cumulative disadvantage and accelerated Grim aging. The solid line displays the predicted regression line, and the dashed lines are the 95% confidence bands for the fitted line. Predicted scores represent residual biological age after controlling for chronological age.
Posthoc analyses provided no evidence that the effect of any of the four types of adversity on GrimAge was conditioned by gender. Further, it should be noted that, as indicated by the variance inflation factors (VIFs) presented in Table 3, multicollinearity was not a problem in the regression models presented in Table 2.
4. Discussion
4.1. Summary of findings.
Stressful conditions and circumstances such as low education, limited income, living in a disadvantaged neighborhood and exposure to racial discrimination have been linked to increased risk for early onset of illness and death (Phelan, Link, and Tehranifar, 2010). These findings raise questions regarding the mechanisms whereby these social variables get “under the skin” or become “biologically embedded” and foster illness and ultimately death (Hertzman, 2012). One plausible mechanism is accelerated biological aging as several studies have reported that epigenetic measures of biological aging, especially the most recent indices such as GrimAge, are robust predictors of both morbidity and mortality (Levine et al., 2018; Lu et al., 2019). Given the predictive power of these biological clocks, it becomes important to identify the extent to which they are predicted by adversity and social disadvantage.
It is crucial that African Americans be included in such research given their high exposure to stressful social circumstances and their elevated rates of morbidity and mortality. Indeed, such studies might be viewed as a test of the weathering hypothesis which asserts that race-related adversity fosters physiological wear and tear that, in turn, contributes to early illness and death (Geronimus, 1992). The GrimAge measure of accelerated aging would seem to be an excellent indicator of weathering. Accordingly, the present study investigated the extent to which four types of strain often experienced by Black Americans - low education, limited income, discrimination, and living in a disadvantaged neighborhood – are related to GrimAge. Consistent with the weathering hypothesis, all four of these measures of adversity, as well as an index combining the four, were significant predictors of GrimAge (see Table 3). Unexpectedly, marriage, which was included as a control variable, was associated with decelerated aging. This finding is consonant with a large literature linking marriage to better health and mortality (Thoits, 2011). The present findings suggest that marriage does this, at least in part, by reducing speed of aging.
4.2. Limitations
Our analyses provided no support for the contention that health risk behaviors such as diet, exercise, or alcohol consumption account for the effect of any of the four social adversity variables. Indeed, once the adversity variables were in the model none of the health risk behaviors were associated with accelerated aging. We speculate that the marginal impact of these lifestyle variables might be attributable, at least in part, to the well-known challenges of using short, self-report measures to assess them. Although there is some evidence supporting the reliability and validity of brief measures such as the ones used in the present study (Adjoian, Firestone, Eisenbower, and Yi, 2016; Li, Carlson, and Holm, 2000; Loftfield, Yi, Immerwahr, and Eisenhower, 2015), more comprehensive assessments of these health risk behaviors might have resulted in their showing an effect.
Another limitation is that our epigenetic measure of aging, GrimAge, was obtained at a single point in time. Future research should assess biological aging and environmental conditions at multiple time-points so that changes in the environment can be examined in relation to changes in speed of aging. Such an approach would provide more compelling evidence for the role of the environment in accelerating or decelerating biological aging.
Finally, while use of an African American sample is a strength given their elevated risk for accelerated aging and early onset of chronic illness, the findings need to be replicated with with larger and more diverse samples. Of particular interest is the extent to which the findings hold for other stigmatized groups that might be expected to experience weathering such as Latinos, Native Americans, Muslim Americans, and members of the LGBTQ community.
5. Conclusion and Implications
While granting these limitations, overall our findings provide strong support for the weathering perspective (Geronimus et al., 2016) as social disadvantages commonly experienced by Black Americans exhibited both unique and combined effects on accelerated aging. These findings would seem to have important intervention and policy implications. Modern medicine views differences in health risk behaviors as the major cause of chronic illness (Bodai et al. 2018; Mackenzie, Skivington, and Fergie, 2020; Milani and Lavie, 2015). This perspective places the responsibility for reversing health inequalities on Black individuals themselves. The assumption is that Black Americans need to adopt a healthier lifestyle if they are to counter their increased risk for chronic illness. This view would seem to both exaggerate the importance of health risk behaviors as the major cause of racial inequalities in health and to overestimate the power or agency that disadvantaged Black Americans possess in bringing about such lifestyle changes. Even if health risk behaviors exert more of an effect than was found in the present study, there is strong evidence that structural factors such as low income and living in a disadvantaged community, are barriers to a healthy diet or daily exercise (Siddiq, Tiro, and Shuval, 2011; Walker, Kane, and Burke, 2010; Whitaker et al., 2018). Disadvantaged neighborhoods are often food deserts that lack grocery stores. And, when such facilities do exist, the residents often lack the money to buy healthy food. Further, such areas often lack gyms, parks, and safe walking areas, making exercise a challenge.
More importantly, however, the emphasis on heathy life style ignores the importance of adverse conditions common in many African American communities such as low education, limited income, neighborhood disadvantage, and pervasive racism as determinants of health. Findings from the present study indicate that these are important factors in accelerating biological aging, a major risk factor for early onset of illness and death. Notably, these social conditions can only be addressed through social policies and programs that target institutional racism and promote economic equity (Mackenzie et al., 2020; Massey, 2007; 2017; Swope and Herandez, 2019).
On a more positive note, findings from the present study indicate that increased income, educational achievement, living in an advantaged neighborhood, limited exposure to discrimination, and marriage may serve to decelerate aging. These results suggest the importance of future studies that investigate the extent to which social resources such as social capital, a supportive partner, or religiosity serve to decelerate aging, perhaps even buffering the effect of stressors such as financial pressure and residing in a disadvantaged neighborhood on accelerated aging. Past research has focused almost exclusively on the determinants of accelerated aging, while almost completely ignoring social factors that might decelerate aging. This is an important omission as such findings might be helpful in identifying points of leverage for slowing aging and thereby postponing onset of chronic illness.
Table 4.
Collinearity diagnostics of the models for accelerated GrimAge
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|
| VIF | Tolerance | VIF | Tolerance | VIF | Tolerance | VIF | Tolerance | |
| Education | 1.31 | .764 | 1.32 | .756 | ||||
| Per capita income (W4) | 1.29 | .777 | 1.29 | .776 | ||||
| Racial discrimination (W4) | 1.07 | .936 | 1.08 | .923 | ||||
| Neighborhood disadvantage | 1.04 | .961 | 1.04 | .960 | ||||
| Cumulative disadvantage | 1.02 | .984 | ||||||
| Marriage | 1.17 | .853 | 1.22 | .823 | 1.20 | .834 | ||
| Males | 1.19 | .842 | 1.33 | .754 | 1.28 | .783 | ||
| Healthy diet (W5) | 1.05 | .949 | 1.07 | .931 | 1.06 | .941 | ||
| Alcohol consumption (W5) | 1.02 | .985 | 1.10 | .911 | 1.10 | .913 | ||
| Exercise (W5) | 1.04 | .963 | 1.14 | .880 | 1.12 | .892 | ||
Note: VIF = Variance inflation factors.
Acknowledgments
This work was supported by the National Institute on Aging (R01 AG055393); the National Heart, Lung, Blood Institute (R01 HL118045); the National Institute on Child Health and Human Development (R01 HD080749); and the National Institute on Drug Abuse (R21 DA034457). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Contributor Information
Ronald L. Simons, Department of Sociology, University of Georgia, 324 Baldwin Hall, Athens, GA 30602
Man-Kit Lei, Center for Family Research, University of Georgia, 1095 College Station Road, Athens, GA 30605.
Eric Klopack, Department of Sociology, University of Georgia, 104 Baldwin Hall, Athens, GA 30602.
Steven R. H. Beach, Department of Psychology, University of Georgia, 157 IBR Psychology Building, Athens GA 30602
Frederick X. Gibbons, Department of Psychological Sciences, University of Connecticut, 406 Babbidge Road, Storrs, CT 06269
Robert A. Philibert, Department of Psychiatry, University of Iowa, 2-126B Medical Education Building, Iowa City, IA 52242
References
- Adjoian TK, Firestone MJ, and Eisenhower D, and Yi SS (2016). Validation of self-rated Overall diet quality by Healthy Eating index-2010 score among New York City adults, 2013. Preventive Medicine Reports, 3, 127–131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ailshire JA, Beltran-Sanchez H, and Crimmins EM (2015). Becoming centenarians: Disease and functioning trajectories of older U.S. adults as they survive to 100. Journal of Gerontology: Series B, Biological and Medical Sciences, 70, 193–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aronow PM, Samii C, & Assenova VA (2015). Cluster–robust variance estimation for dyadic data. Political Analysis, 23, 564–577. [Google Scholar]
- Belikov AV (2019). Age-related diseases as vicious cycles. Ageing Research Reviews. 49, 11–26. [DOI] [PubMed] [Google Scholar]
- Brody GH, Miller GE, Yu T, Beach S.R.Hf., & Chen E (2016). Supportive family environments ameliorate the link between racial discrimination and epigenetic aging. Psychological Science, 27, 530–541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown S (2019). Nearly half of undergraduates are students of color. But Black students lag behind. The Chronical of Higher Education. February 14. [Google Scholar]
- Cockerham W, Hamby BW, and Oates GR (2017). The social determinants of chronic disease. American Journal of Preventative Medicine, 52, S5–S12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fransquet PD, Wrigglesworth J, Woods RL, Ernst ME, and Ryan J (2019). The epigenetic clock as a predictor of disease and mortality risk: A systematic review and meta-analysis. Cinical Epigenetics, 11:62 doi.org/0.1186/s13148-019-0656-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geronimus AT (2001). Understanding and eliminating racial inequalities in women’s health in the United States: The role of the weathering conceptual framework. Journal of the American Medical Women’s Association, 56, 133–136. [PubMed] [Google Scholar]
- Geronimus AT, Hicken M, Keene D, & Bound J (2006). “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. American Journal of Public Health, 96(5), 826–833. doi: 10.2105/ajph.2004.060 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geronimus AT, Hicken MT, Pearson JA, Seashols SJ, Brown KL, & Cruz TD (2010). Do US black women experience stress-related accelerated biological aging? Human Nature, 21, 19–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geronimus AT, James S, Destin M, Graham L, Hatzenbuehler M,Murphy M, Pearson J, Omari A, & Thompson J, J.P. (2016). Jedi Public Health: Co-Creating an Identity-Safe Culture to Promote Health Equity. Social Science and Health-Population Health, 2, 105–116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geronimus AT, & Thompson JP (2004). To denigrate, ignore, or disrupt: Racial inequality in health and the impact of policy-induced breakdown of African American communities. Du Bois Review, 1(2): 247–279. [Google Scholar]
- Gibbons FX, Gerrard M, Cleveland MJ, Wills TA, & Brody G (2004). Perceived discrimination and substance use in African American parents and their children: A panel study. Journal of Personality and Social Psychology, 86(4), 517–529. doi: 10.1037/0022-3514.86.4.517 [DOI] [PubMed] [Google Scholar]
- Hannum G, Guinney J, Zhao L,….Zhang K (2013). Genome-Wide Methylation Profiles Reveal Quantitative Views of Human Aging Rates. Molecular Cell 49(2), 359–367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horvath S (2013). DNA methylation age of human tissues and cell types. Genome Biology, 14(10), 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson BT, & Acabchuk RL (2018). What are the keys to a longer, happier life? Answers from five decades of health psychology research. Social Science & Medicine, 196, 218–226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jyhava Juulia, Pedersen Nancy, & Hagg Sara. 2017. Biological Age Predictors. EBioMedicine 21, 29–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kennedy BK (2013). NIH Conference on Advances in Geroscience: Impact on Health Span and Chronic disease. October, National Institutes of Health, Bethesda, MD. [Google Scholar]
- Kennedy BK, Berger S, Brunet A…Sierra F (2014). Geroscience: Linking Aging to Chronic Disease. Cell 159, 709–713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koch CM,, and Wagner W (2011). Epigenetic-aging-signiture to determine age in different tissues. Aging, 10, October; 3(10): 1018–1027. doi: 10.18632/aging.100395 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kraus MW, Rucker JM, and Richeson JA(2017). Americans misperceive racial equality. Proceedings of the National Academy of Science, 114, 10324–10331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lei M-K, Simons RL, Beach SRH, and Philibert RA (2019). Neighborhood disadvantage and biological aging. Journals of Gerontology: Series B, 74, e50–59. 10.1093/geronb/gbx015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lei M-K, Simons RL, Edmond MB, Simons LG, and Cutrona CE (2014). The effect of neighborhood disadvantage, social ties, and genetic variation on the antisocial behavior of African American women: A multilevel analysis. Development and Psychopathology, 26, 1113–1128, [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levine ME, Lu1 AT, Quach A, Chen BH, Assimes TL, Bandinelli S, …. Horvath S (2018). An epigenetic biomarker of aging for lifespan and healthspan. Aging. 10, 4. doi: 10.18632/aging.101414 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li S, Carlson E, and Holm K (2000). Validation of a single-item measure of usual physical activity. Perception and Motor Skills, 91, 593–602. [DOI] [PubMed] [Google Scholar]
- Loftfield E, Yi Stella, Immerwahr S, and Eisenhower D (2015). Construct validity of a single-item, self-rated question of diet quality. Journal of Nutrition Education and Behavior. 47, 181–187. [DOI] [PubMed] [Google Scholar]
- Lu AT, Quach A, Wilson JG, Reiner AP, Aviv A, ….Horvalth S (2019). DNA methylation GrimAge strongly predicts lifespan and healthspan. Aging, 11, 303–327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackenzie M, Sivington K, and Fergie G (2020). “The state They’re in”: Unpicking fantasy paradigms of health improvement interventions as tools for addressing health inequalities. Social Science and Medicine, 256, 113047. Doi.org/10.1016/j.socscimed.2020.113047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manduca R (2018). Income inequality and the persistence of racial economic disparities. Sociological Science, 5, 182–205. [Google Scholar]
- Massey DS (2007). Categorically Unequal: The American Stratification System. New York: Russell Sage Foundation. [Google Scholar]
- Massey DS (2017). Why death haunts black lives. Proceedings of the National Academy of Science, 114, 800–802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milton K, Bull FC, and Bauman A (2011). Reliability and vaidity testing of a single-item physical activity measures. British Journal of Sports Medicine, 45, 203–208. [DOI] [PubMed] [Google Scholar]
- Mormat M (2004). The Status Syndrome. NY: Holt and Company. [Google Scholar]
- Mormat M (2015). The Health Gap: The Challenge of an Unequal World. NY: Bloomsbury. [Google Scholar]
- Muthén LK, & Muthén BO (2015). Mplus User’s Guide. Los Angeles, Muthén and Muthén. [Google Scholar]
- Moffitt T, Belsky D, Danese A, Poulton R, & Capsi A (2016). The longitudinal study of aging in human young adults: knowledge gaps and research agenda.” Journals of Gerontology: A Medical Sciences 72, 210–215. doi: 10.1093/gerona/glw191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ornish D, Lin J, Chan JM Epel E, Kemp C, Wieidner G…………..Blackburn E (2013). Effect of comprehensive lifestyle changes on telomerase activity and telomere length in men with biopsy-proven low-risk prostate cancer: 5-year follow-up of a descriptive pilot study. Lancct Oncology, 14, 1112–1120. doi: 10.1016/S1470-2045(13)70366-8 [DOI] [PubMed] [Google Scholar]
- Pager D, Bonikowski B, and Western (2009). Discrimination in a low-wage labor market: A field Experiment. American Sociological Review, 74, 777–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phelan JC, & Link BG (2015). Is racism a fundamental cause of inequalities in health? Annual Review of Sociology, 41, 311–330. [Google Scholar]
- Phelan Jo, Link B, & Tehranifar P (2010). Social conditions as fundamental causes of health Inequalities: theory, evidence, and policy implications.” Journal of Health and Social Behavior 51, S28–S40. doi: 10.1177/0022146510383498 [DOI] [PubMed] [Google Scholar]
- Sampson RJ (2011). The Great American City. Chicago: University of Chicago Press. [Google Scholar]
- Sampson RJ, Raudenbusch SW, and Earls F (1997). Neighborhoods and violent crime: A multilevel study of collective efficacy. Science, 277, 918–24. [DOI] [PubMed] [Google Scholar]
- Sawyer J, and Gampa A (2018). Implicit and explicit racial attitudes changed during Black Lives Matter. Personality and Social Psychology Bulletin, 44, 1039–1059. [DOI] [PubMed] [Google Scholar]
- Siddiqi Z, Tiro JA, and Shuval Kerem (2011). Understanding impediments and enablers to physical activity among African American adults: A systematic review of qualitative studies. Heath Education Research, 26, 1010–1024. [DOI] [PubMed] [Google Scholar]
- Simons RL, Lei MK, Beach SRH, Brody GH, Philibert RA, & Gibbons FX (2011). Social environment, genes, and aggression: Evidence supporting the differential susceptibility perspective. American Sociological Review, 76(6), 883–912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons RL, Lei M-K, Beach SRH, Barr AB, Simons LG, Gibbons FX, & Philibert RA Philibert. (2018). Discrimination, segregation, and chronic inflammation: Testing the weathering explanation for the poor health of black Americans. Developmental Psychology, 54, 1993–2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons RL, Lei MK, Bearch SRH, Philibert RA, Cutrona CE, Gibbons FX, & Barr A (2016). Economic hardship and biological weathering: The epigenetics of aging in a U.S. sample of black women. Social Science and Medicine, 150, 192–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swope CB, and Herandez D (2019). Housing as a determinant of health equity: A conceptual model. Social Science and Medicine, 243, 112571.doi: 10.1016/j.socscimed.2019.112571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thoits PA (2011). Mechanisms linking Social ties and Support to Physical and Mental Health. Journal of Health and Social Behavior, 52(2), 145–162. [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau (2014). Living in near poverty in the United States: 1966–2012. https://www.census.gov/hhes/wwwj/poverty/about/overview/
- Walker RE, Kean CR, and Burke JG (2010). Disparities and access to healthy food in the United States: A review of feel deserts literature. Health and Place, 16, 876–884. [DOI] [PubMed] [Google Scholar]
- Williams DR (2012). Miles to go before we sleep: Racial inequities in health. Journal of Health and Social Behavior, 53: 279–295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson WJ (1987). The Truly Disadvantaged. Chicago: University of Chicago Press. [Google Scholar]
- Zannas AS, Arloth J, Carrillo-Roa T, Lurato S, Roh Simone….Mehta D (2015). Lifetime stress accelerates epigenetic aging in an urban, African American cohort: relevance of glucocorticoid signaling. Genome Biology 16, 266 doi: 10.1186/s13059-015-0828-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhoa W, Ammous F, Ratliff S Liu J, Yu M, Mosley TH, Kardia LRS, and Smith JA (2019). Education and lifestyle factors are associated with DNA methylation clocks in older African Americans. International Journal f Environmental Research and Public Health, 16, 3141. [DOI] [PMC free article] [PubMed] [Google Scholar]