

This randomized clinical trial assesses the efficacy and safety of osimertinib plus bevacizumab vs osimertinib alone in patients with EGFR T790M–mutated lung adenocarcinoma.
Key Points
Question
Can osimertinib plus bevacizumab work synergistically and be tolerable in patients with advanced non–small cell lung cancer (NSCLC) that harbors EGFR T790M mutation?
Findings
In this phase 2 randomized clinical trial of 81 patients with NSCLC with EGFR T790M mutation, osimertinib plus bevacizumab failed to show prolongation of progression-free survival and overall survival compared with osimertinib alone, although toxic effects were tolerable.
Meaning
In patients with NSCLC with EGFR T790M mutation, osimertinib plus bevacizumab was tolerable but not efficacious , which had been suggested by recent single-arm studies.
Abstract
Importance
Although treatment with first-generation epidermal growth factor receptor (EGFR)–tyrosine kinase inhibitor (TKI) plus antiangiogenic inhibitor has shown promising efficacies in patients with EGFR-mutated lung adenocarcinoma, recent single-arm studies have suggested that osimertinib plus antiangiogenic inhibitor might not work synergistically.
Objective
To explore the efficacy and safety of osimertinib plus bevacizumab compared with osimertinib alone in patients with lung adenocarcinoma with EGFR T790M mutation.
Design, Setting, and Participants
Patients with advanced lung adenocarcinoma that progressed with prior EGFR-TKI treatment (other than third-generation TKI) and acquired EGFR T790M mutation were enrolled. This study comprises a lead-in part with 6 patients and a subsequent phase 2 part. In phase 2, patients were randomized to osimertinib plus bevacizumab or osimertinib alone in a 1:1 ratio.
Interventions
The combination arm received oral osimertinib (80 mg, every day) plus intravenous bevacizumab (15 mg/kg, every 3 weeks) until progression or unacceptable toxic effects. The control arm received osimertinib monotherapy.
Main Outcomes and Measures
The primary end point was progression-free survival (PFS) assessed by investigators. Secondary end points consisted of overall response rate, time to treatment failure, overall survival, and safety.
Results
From August 2017 through September 2018, a total of 87 patients were registered (6 in the lead-in part and 81 in the phase 2 part [intention-to-treat population]). Among those randomized, the median (range) age was 68 (41-82) years; 33 (41%) were male; 37 (46%) had an Eastern Cooperative Oncology Group performance status of 0; and 21 (26%) had brain metastasis. Although the overall response rate was better with osimertinib plus bevacizumab than osimertinib alone (68% vs 54%), median PFS was not longer with osimertinib plus bevacizumab (9.4 months vs 13.5 months; adjusted hazard ratio, 1.44; 80% CI, 1.00 to 2.08; P = .20). Median time to treatment failure was also shorter in the combination arm vs the osimertinib arm (8.4 months vs 11.2 months; P = .12). Median overall survival was not different in the combination arm vs osimertinib arm (not reached vs 22.1 months; P = .96). In the combination arm, common adverse events of grade 3 or higher were proteinuria (n = 9; 23%), hypertension (n = 8; 20%).
Conclusions and Relevance
In this randomized clinical trial comparing osimertinib plus bevacizumab vs osimertinib alone, the combination arm failed to show prolongation of PFS in patients with advanced lung adenocarcinoma with EGFR T790M mutation.
Trial Registration
UMIN Clinical Trials Registry Identifier: UMIN000023761
Introduction
Among metastatic non–small cell lung cancer (NSCLC), EGFR mutation is the second most frequent genetic driver. First-generation and second-generation epidermal growth factor receptor (EGFR)–tyrosine kinase inhibitors (TKIs) have shown favorable efficacy over cytotoxic chemotherapy in patients with NSCLC with EGFR mutation.1,2 However, these patients ultimately experience disease progression within 10 to 13 months. Translational analyses revealed that about half of tumors acquired EGFR exon 20 T790M mutation as the most common mechanism of resistance.3
Osimertinib is an orally available covalent third-generation EGFR-TKI that has shown activity in both EGFR sensitizing (exon 19 deletion or exon 21 L858R) and exon 20 T790M mutations in a preclinical study.4 Among patients with NSCLC with EGFR T790M mutation, a phase 3 trial (AURA3)5 showed significant prolongation of progression-free survival (PFS) compared with platinum doublet chemotherapy. However, median PFS with osimertinib was again almost 10 months. Considering the tolerability of osimertinib monotherapy, a novel combination strategy to delay progression has been warranted.
Vascular endothelial growth factor (VEGF) plays a crucial role in cancer through its proliferation or metastasis, and several anti-VEGF inhibitors have already been developed. Bevacizumab is a humanized monoclonal IgG1 antibody that binds to VEGF and has shown clinical efficacy against various types of malignant neoplasms. In a preclinical study, EGFR-TKI plus anti-VEGF inhibitor showed synergistic effect in EGFR T790M xenograft model.6 Moreover, several prospective studies have shown preferable efficacy among patients with EGFR sensitizing7,8 and preexisting T790M variants.9 However, the efficacy and safety of osimertinib in combination with bevacizumab have not yet been elucidated. This study aims to test this combination in patients with EGFR-mutated NSCLC that progressed with prior EGFR-TKI treatment and acquired EGFR T790M mutation.
Methods
Study Design
This open-label, multi-institutional study comprises a lead-in part to assess the feasibility of combination treatment, followed by a randomized phase 2 part. In the lead-in part, 6 patients were treated with a fixed dose of osimertinib (80 mg/d) and bevacizumab (15 mg/kg, every 3 weeks). If more than 2 patients in this cohort experienced dose-limiting toxicity (DLT) in the first cycle, this study would be terminated. The definition of DLT was as follows: (1) nonhematologic toxic effect of grade 3 or greater, (2) hypertension of grade 4, or (3) interstitial lung disease of grade 2 or greater. After confirming the feasibility of this lead-in part, the phase 2 part was initiated, and eligible patients were equally randomized to the osimertinib arm or the combination arm. Randomization was stratified according to sex (male vs female), number of prior cytotoxic chemotherapy treatments (0 vs ≥1), and institution. The primary end point of the phase 2 part was PFS assessed by investigators. Secondary end points were overall response rate (ORR), time to treatment failure (TTF), overall survival (OS), and safety. This study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline.
Ethical Considerations
The study was conducted in compliance with the principles of the Declaration of Helsinki,10 and the institutional review board of each participating institution approved the protocol. Written informed consent was obtained from all patients before any screening or inclusion procedures. The trial protocol is available in Supplement 1.
Eligibility and Exclusion Criteria
Eligible patients were (1) those with pathologically confirmed lung adenocarcinoma with EGFR sensitizing mutation, (2) those diagnosed as stage IIIB or IV in accordance with the seventh version of the American Joint Committee on Cancer staging criteria for lung cancer, or relapsed as metastatic disease after curative treatment, (3) those previously treated with the first-generation or second-generation EGFR-TKI and confirmed radiological progression, (4) those whose cancer was confirmed to acquire EGFR exon 20 T790M mutation after EGFR-TKI treatment, (5) those with Eastern Cooperative Oncology Group performance status of 0 or 1, (6) those with a measurable lesion according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1., (7) those with adequate organ function, and (8) those who provided written informed consent for inclusion in this study. Testing for EGFR mutation was done by local sites using polymerase chain reaction–based methods. Patients were excluded if they had (1) interstitial lung disease at the time of registration, (2) higher risk of bleeding or embolism, (3) uncontrolled hypertension, (4) leptomeningeal disease, or (5) positivity for hepatitis B virus antigen. Those who had brain metastasis were eligible for inclusion unless they were symptomatic at the time of registration. Patients who had a prior history of cytotoxic chemotherapy treatment were also eligible, and those who received radiotherapy to the brain were allowed after a 14-day interval after the last fraction of radiotherapy.
Study Treatment and Assessment Procedures
All patients were orally administered 80 mg of osimertinib every day. Patients who participated in the lead-in part or were allocated to the combination arm in the phase 2 part were intravenously administered 15 mg/kg of bevacizumab on day 1, every 3 weeks. Both drugs were continued until disease progression, but patients were allowed to continue the study treatment beyond radiological progression when it was considered to be clinically beneficial. Osimertinib treatment could be suspended due to toxic effects and resumed at 40 mg per day. Bevacizumab treatment could be suspended due to toxic effects but should be resumed at the same dose. Bevacizumab treatment was discontinued if patients experienced severe toxic effects (ie, gastrointestinal perforation [any grade], thromboembolism, pulmonary hemorrhage [grade ≥2] or other hemorrhages, allergic reaction, or cardiac toxic effects [grade ≥3]). Bevacizumab treatment was also to be discontinued if patients had not recovered within 42 days from a toxic effect requiring suspension (ie, serum creatinine >1.5 mg/dL, proteinuria greater than 2+ or hypertension [grade 4]). These patients were allowed to continue osimertinib treatment.
To assess the efficacy, computed tomography of the chest and upper abdomen was assessed every 6 weeks. Brain magnetic resonance imaging was assessed every 6 weeks if patients had detected brain metastasis at the time of study entry. Adverse events (AEs) were graded using the Common Terminology Criteria for Adverse Events, version 4.0.
Sample Size Calculation
Previous studies7,8 compared the efficacy of adding anti-VEGF inhibitor to the first-generation EGFR-TKIs and showed a hazard ratio (HR) of 0.44 to 0.54 in PFS compared with EGFR-TKI alone. We therefore assumed that osimertinib plus bevacizumab would lead to a PFS about 7.4 months longer than with osimertinib monotherapy, which corresponded to an HR of 0.55. Based on previous studies, 74 patients were required to ensure a statistical power of 0.80 at a 2-sided α error of 0.20. Considering a dropout rate of 8%, 80 patients were finally required.
Statistical Analysis
The PFS was estimated using Kaplan-Meier curves. Median PFS with 95% CI was reported for each treatment arm. The difference in PFS between the 2 treatment arms was examined at the significance level of 0.20 using a stratified log-rank test using the stratification factors (sex, number of prior cytotoxic chemotherapy treatments, and institution). A Cox regression model was used to estimate the adjusted HR stratified by sex (male/female) and history of cytotoxic chemotherapy treatment (yes/no) and its 80% and 95% CIs. All tests for the secondary end points were carried out at a 5% α level. The TTF and OS were analyzed in a similar way to PFS. For the ORR, the point estimates and the 95% CI with the Pearson-Clopper method were provided. Difference in the ORR was estimated using the χ2 test. Characteristics of the 2 arms were compared using the χ2 test or analysis of variance. Statistical analyses were conducted with JMP software, version 11 (SAS Institute) and GraphPad Prism, version 7.00 for Windows (GraphPad Software). A P value less than .05 was considered to be significant.
Results
The flowchart of the participants is shown in Figure 1. From August 2017 through September 2018, a total of 87 patients were registered (6 in the lead-in part and 81 in the phase 2 part [intention-to-treat population]). Of 81 patients registered in the phase 2 part, 41 were allocated to the osimertinib arm, and 40 were allocated to the combination arm. All received at least 1 dose of study treatment; they were therefore analyzed as a safety population. At the time of data cutoff, all patients in the lead-in part finished study treatment, while 26 patients were still receiving treatment in the phase 2 part. The median (range) follow-up time in the phase 2 part was 16.2 (2.8-24.0) months in the osimertinib arm and 16.0 (2.4-22.6) months in the combination arm.
Figure 1. Patient Flow of the Trial.

Lead-in Part
Baseline characteristics of the 6 patients are shown in eTable 1 in Supplement 2. No DLT was observed during the first cycle, and AEs during the whole study period were mostly grade 1 or 2 (eTable 2 in Supplement 2). Grade 3 AEs were hypertension, decreased neutrophil count, rash, and anemia (2 cases each). One patient had interstitial lung disease on day 31 but finally improved on day 46. Regarding efficacy, there were 5 patients with partial responses and 1 patient with stable disease. The median PFS was 11.5 months (95% CI, 3.7 months to not reached; eFigure 1 in Supplement 2).
Phase 2 Part
Baseline characteristics of the 81 patients are summarized in the Table. The median (range) age was 68 (41-82) years; 33 (41%) were male; 4 (5%), 59 (73%), and 18 (22%) had a clinical stage IIIB, IV, and recurrence, respectively; 37 patients (46%) had an Eastern Cooperative Oncology Group performance status of 0 or and 44 (54%) had a status of 1; and 21 patients (26%) had brain metastasis. A total of 17 patients (21%) had prior history of cytotoxic chemotherapy treatment and 12 (15%) had prior history of anti-VEGF therapy. About 20% (n = 18) of the patients were diagnosed with EGFR T790M–mutated disease using peripheral blood samples, and about 12% (n = 10) were diagnosed using pleural effusion samples. There were no significant differences between the arms, but the combination arm tended to have fewer patients with recurrence after curative therapy or never received anti-VEGF therapy.
Table. Patient Characteristics in Phase 2 Part.
| Characteristic | No. (%) | P value | |
|---|---|---|---|
| Osimertinib (n = 41) | Osimertinib + bevacizumab (n = 40) | ||
| Age, median (range), y | 70 (41-82) | 68 (43-82) | .57 |
| Sex | |||
| Male | 17 (41) | 16 (40) | .58 |
| Female | 24 (59) | 24 (60) | |
| Smoking status | |||
| Never | 20 (49) | 21 (53) | .91 |
| Smoker or former smoker | 21 (51) | 19 (48) | |
| ECOG performance status | |||
| 0 | 17 (42) | 20 (50) | .58 |
| 1 | 24 (58) | 20 (50) | |
| Clinical stage | |||
| IIIB | 2 (5) | 2 (5) | .11 |
| IV | 26 (63) | 33 (83) | |
| Recurrence | 13 (32) | 5 (12) | |
| Previous EGFR-TKI | |||
| 1st Generation | 35 | 36 | .81 |
| 2nd Generation | 11 | 10 | |
| No. of prior cytotoxic chemotherapy treatments | |||
| 0 | 34 (83) | 30 (75) | .54 |
| ≥1 | 7 (17) | 10 (25) | |
| Types of EGFR mutation | |||
| Exon 20 T790M | 41 (100) | 40 (100) | Exon 19del vs exon 21 L858R: .32 |
| Exon 19del | 28 (68) | 22 (55) | |
| Exon 21 L858R | 13 (32) | 18 (45) | |
| Prior anti-VEGF inhibitor | |||
| Yes | 4 (10) | 8 (20) | .22 |
| No | 36 (88) | 31 (78) | |
| Unknown | 1 (2) | 1 (2) | |
| Brain metastasis | |||
| Yes | 9 (22) | 12 (30) | .46 |
| No | 32 (78) | 28 (70) | |
| Sites of detecting EGFR exon 20 T790M | |||
| Peripheral blood | 10 (24) | 8 (20) | |
| Lung | 19 (46) | 18 (45) | |
| Pleural effusion | 4 (10) | 6 (15) | |
| Liver | 1 (2) | 1 (3) | |
| Mediastinal lymph node | 4 (10) | 1 (3) | |
| Pleura | 2 (5) | 0 | |
| Other | 1 (2) | 6 (15) | |
Abbreviations: ECOG, Eastern Cooperative Oncology Group; EGFR-TKI, epidermal growth factor receptor–tyrosine kinase inhibitor; VEGF, vascular endothelial growth factor.
Although ORR was higher in the combination arm (71.8%; 95% CI, 50.9%-81.4%) than in the osimertinib arm (55.0%; 95% CI, 37.4%-69.3%; Figure 2), it did not contribute to prolongation of PFS (13.5 months in the osimertinib arm vs 9.4 months in the combination arm; adjusted HR, 1.44; 80% CI, 1.00-2.08, and 95% CI, 0.83-2.52, respectively; P = .20; Figure 3A). Any subset analysis did not show significant difference in PFS (eFigure 2 in Supplement 2). Of those, prior history of anti-VEGF inhibitor seemed to have a detrimental effect on the combination treatment. In the combination arm, patients who had any history of anti-VEGF therapy showed significantly shorter PFS than those who did not (4.6 months vs 11.1 months; HR, 0.41; 95% CI, 0.13-1.27; P = .03; Figure 3B) while prior exposure of anti-VEGF therapy did not affect PFS in the osimertinib arm (15.1 months vs 13.7 months; HR, 1.19; 95% CI, 0.31-4.61; P = .85). The TTF was also longer in the osimertinib arm than in the combination arm (11.2 months vs 8.4 months; adjusted HR, 1.54; 95% CI, 0.90-2.69; P = .12; Figure 4A). Finally, median OS was not different between the arms (22.1 months in osimertinib arm vs not reached in the combination arm; adjusted HR, 1.02; 95% CI, 0.43-2.44; P = .96; Figure 4B).
Figure 2. Waterfall Plot of Each Arm Showing Best Percentage Change in Tumor Burden From Baseline.
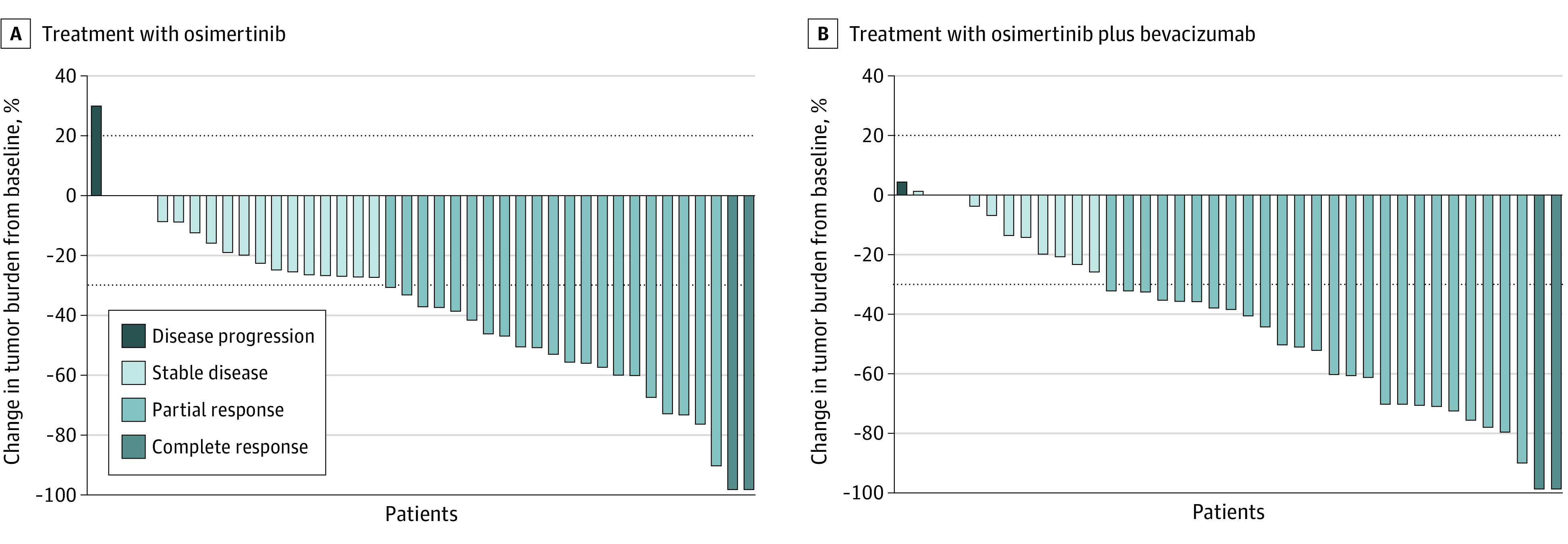
A, Complete response (n = 2), partial response (n = 21), stable disease (n = 17), and disease progression (n = 1). B, Complete response (n = 2), partial response (n = 25), stable disease (n = 11), disease progression (n = 1), not evaluable (n = 1).
Figure 3. Kaplan-Meier Curves of Progression-Free Survival.

A, Kaplan-Meier curves of progression-free survival in the osimertinib arm (n = 41) and combination arm (n = 40). B, Subgroup analysis according to any history of anti–vascular endothelial growth factor (VEGF) therapy.
Figure 4. Kaplan-Meier Curves of Time to Treatment Failure and Overall Survival.
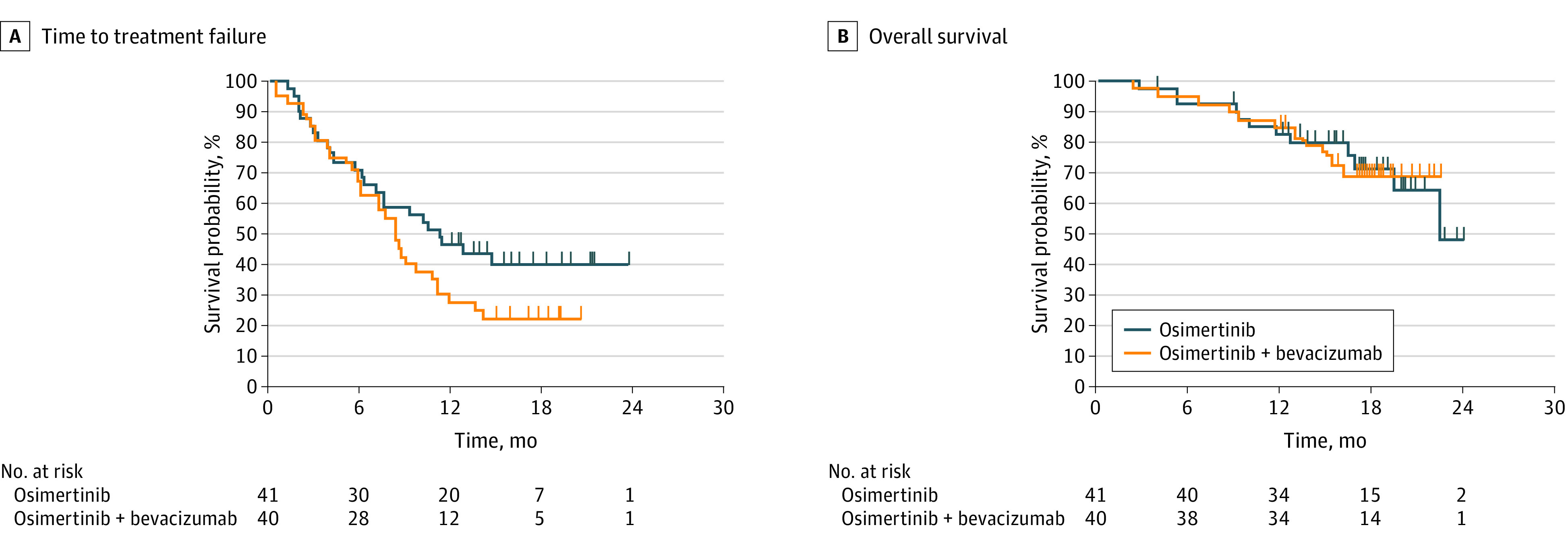
Kaplan-Meier curves of time to treatment failure (A) and overall survival (B) in the osimertinib arm (n = 41) and combination arm (n = 40).
Adverse events are shown in eTable 3 in Supplement 2. Like those observed in the lead-in part, most AEs were generally mild (grade 1 or 2). Common AEs observed in the combination arm were proteinuria (grade 1-2, n = 22, 55%; and grade 3, n = 9, 23%) and hypertension (grade 1-2, n = 16, 40%; and grade ≥3, n = 8; 20%). The rates of proteinuria (n = 31; 78%) and hypertension (n = 24; 60%) were significantly higher in the combination arm, while the incidence of anemia (n = 27; 66%)was significantly higher in the osimertinib arm. The number of hematologic toxic effects and skin-related AEs was not increased by adding bevacizumab. There was no serious bleeding or embolism in the combination arm. About 11% (9 patients) of the entire population experienced interstitial lung disease, but all were grade 1 or 2.
Treatment exposure is summarized in eTable 4 in Supplement 2. Twenty-seven patients (33%) experienced dose interruption with osimertinib, but the proportion was similar between the arms (13 in the osimertinib arm vs 14 in the combination arm). Of the 55 patients who discontinued study treatment, 37 were due to disease progression and 15 were due to toxic effects. In the combination arm, 11 patients (28%) discontinued bevacizumab due to AEs, and median (range) number of bevacizumab administrations was 7.5 (1-28). However, post-hoc analysis showed that discontinuation of bevacizumab due to AEs did not affect PFS in the combination arm (eFigure 3 in Supplement 2).
At the data cutoff time, 53 patients finished study treatment and about 45 of them (85%) received poststudy treatment (eTable 5 in Supplement 2). Common treatment regimens were platinum doublet chemotherapy (22 patients) and EGFR-TKI rechallenge (21 patients).
Discussion
To our knowledge, this is the first randomized clinical trial to explore the efficacy of adding anti-VEGF inhibitor to osimertinib. Although ORR was slightly better in the combination arm, we could not show advantages in PFS and OS. Previous reports have suggested that EGFR-TKI plus anti-VEGF inhibitor might be more beneficial in patients with brain metastasis11 or pleural effusion12; however, none of our subgroup analyses could identify its advantage.
In patients with advanced NSCLC with EGFR mutation, 1 randomized-phase 2 trial13 and 2 phase 3 trials7,8 showed benefits in PFS with erlotinib plus anti-VEGF inhibitor compared with erlotinib alone. On the other hand, a recent phase 2 randomized clinical trial14 had negative results (median PFS, 17.9 months vs 13.5 months; HR, 0.81; P = .39), and similar unfavorable results have been reported in single-arm trials9,15 (median PFS, 13.2 months and 14.4 months, respectively). Regarding osimertinib, 2 single-arm studies reported the preliminary results of combining anti-VEGF inhibitors. Among 49 treatment-naive patients with EGFR sensitizing variants, osimertinib plus bevacizumab demonstrated an ORR of 80% and a median PFS of 18.4 months.16 Another phase 2 study of osimertinib plus ramucirumab in 25 patients with EGFR T790M variant showed an ORR of 76% and median PFS of 11.0 months.17 Considering the efficacy data of osimertinib monotherapy in pivotal trials (18.9 months among EGFR-TKI–naive patients and 10.1 months among patients with EGFR T790M–mutated disease),5,18 these phase 2 results were not so intriguing. The present study provided more reliable evidence by adopting a randomized study design. Our control arm showed outstanding PFS (median, 13 months), but this was comparable with the Japanese subset of AURA3.19
The reason why every single study did not show advantages with osimertinib plus anti-VEGF inhibitor has not been fully discussed. Both Paz-Ares et al17 and the present study enrolled patients who had progression despite prior EGFR-TKI treatment; it is therefore possible to speculate that exposure to prior treatment and tumor regrowth could confer microenvironmental changes of the tumor that lead to resistance to anti-VEGF agents. Another possible explanation indicated from the subset analysis is that prior exposure to anti-VEGF inhibitor may induce a different tumor environment that prevents synergy between osimertinib and bevacizumab. Based on prior evidence,20 we allowed inclusion of patients who had prior anti-VEGF inhibitor treatment. However, as shown in Figure 3B, prior exposure to anti-VEGF inhibitor had a detrimental effect in the combination arm. Nonetheless, the PFS among those without any history of anti-VEGF inhibitor in the combination arm was not superior to that in patients receiving osimertinib monotherapy. Indeed, these hypotheses may not be applicable to the result from the first-line trial by Yu et al.16 We did not prepare any collections of tissue or plasma samples before and after treatment, so we could not discuss any potential resistance mechanism with bevacizumab21,22 in the current study.
Limitations
Our trial has several limitations. First, owing to the small number of patients, this single study may not be conclusive. However, we think it is important that this randomized study clearly replicated the findings from previous single-arm studies. The data will draw attention to the development of osimertinib plus anti-VEGF inhibitors in any lines of treatment while several trial groups are conducting larger studies. Second, regarding toxic effects, our participants showed relatively higher incidence of proteinuria. Previously, Japanese patients with NSCLC were more likely to show a higher rate of proteinuria with anti-VEGF inhibitors. For example, the incidence of proteinuria with chemotherapy plus anti-VEGF inhibitor was much higher in Japanese studies (any grade, 26%-50%; grade 3-4, 4%) than in global studies (any grade, 4%; grade 3-4, 1%),20,23,24 and similar tendency was observed between Yu et al16 and the current study. This racial difference could affect the feasibility of bevacizumab to some extent; however, post-hoc analysis (eFigure 3 in Supplement 2) denied its influence on PFS. Nevertheless, the current study provides meaningful information; adding anti-VEGF to osimertinib did not have the desired affect among patients with EGFR T790M–mutated disease.
The results may also have implications for the choice of first-line regimen in patients with EGFR variant. Recent studies reported comparable PFS data between osimertinib alone (18.9 months in the FLAURA trial18) and erlotinib plus anti-VEGF inhibitors (16.9 months in the NEJ026 trial7 and 19.4 months in the RELAY trial8). The current study’s data suggested that the prior exposure to anti-VEGF inhibitors clearly had detrimental effect on second-line osimertinib plus bevacizumab. More importantly, this combination itself is no longer effective in patients with EGFR T790M–mutated disease. Reflecting the results of the current trial, the efficacy of osimertinib plus anti-VEGF therapy should be explored as first-line treatment. Several randomized studies (ie, WJOG 9717L trial [UMIN000030206] and NCT04181060) are ongoing, and these results are anticipated with interest.
Conclusions
Compared with osimertinib monotherapy, osimertinib plus bevacizumab failed to show prolongation of PFS in patients with EGFR T790M–mutated advanced lung adenocarcinoma.
Trial Protocol
eTable 1. Patients’ characteristics in lead-in part
eTable 2. Adverse events in lead-in part (more than 33%)
eTable 3. Adverse events in each arm (more than 20% or special interest)
eTable 4. Treatment exposure and reasons of interruption or discontinuation
eTable 5. Post-study treatment
eFigure 1. Kaplan-Meier curve of progression-free survival in lead-in part
eFigure 2. Subgroup analysis of progression-free survival in phase II
eFigure 3. Post-hoc analysis of progression-free survival in arm B depending on discontinuation of bevacizumab
Data Sharing Statement
References
- 1.Lee CK, Davies L, Wu YL, et al. Gefitinib or erlotinib vs chemotherapy for EGFR mutation-positive lung cancer: individual patient data meta-analysis of overall survival. J Natl Cancer Inst. 2017;109(6). doi: 10.1093/jnci/djw279 [DOI] [PubMed] [Google Scholar]
- 2.Sequist LV, Yang JC, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31(27):3327-3334. doi: 10.1200/JCO.2012.44.2806 [DOI] [PubMed] [Google Scholar]
- 3.Sequist LV, Waltman BA, Dias-Santagata D, et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci Transl Med. 2011;3(75):75ra26. doi: 10.1126/scitranslmed.3002003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yver A. Osimertinib (AZD9291)—a science-driven, collaborative approach to rapid drug design and development. Ann Oncol. 2016;27(6):1165-1170. doi: 10.1093/annonc/mdw129 [DOI] [PubMed] [Google Scholar]
- 5.Mok TS, Wu Y-L, Ahn M-J, et al. ; AURA3 Investigators . Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med. 2017;376(7):629-640. doi: 10.1056/NEJMoa1612674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Naumov GN, Nilsson MB, Cascone T, et al. Combined vascular endothelial growth factor receptor and epidermal growth factor receptor (EGFR) blockade inhibits tumor growth in xenograft models of EGFR inhibitor resistance. Clin Cancer Res. 2009;15(10):3484-3494. doi: 10.1158/1078-0432.CCR-08-2904 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Saito H, Fukuhara T, Furuya N, et al. Erlotinib plus bevacizumab versus erlotinib alone in patients with EGFR-positive advanced non-squamous non-small-cell lung cancer (NEJ026): interim analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Oncol. 2019;20(5):625-635. doi: 10.1016/S1470-2045(19)30035-X [DOI] [PubMed] [Google Scholar]
- 8.Nakagawa K, Garon EB, Seto T, et al. ; RELAY Study Investigators . Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(12):1655-1669. doi: 10.1016/S1470-2045(19)30634-5 [DOI] [PubMed] [Google Scholar]
- 9.Rosell R, Dafni U, Felip E, et al. ; BELIEF Collaborative Group . Erlotinib and bevacizumab in patients with advanced non-small-cell lung cancer and activating EGFR mutations (BELIEF): an international, multicentre, single-arm, phase 2 trial. Lancet Respir Med. 2017;5(5):435-444. doi: 10.1016/S2213-2600(17)30129-7 [DOI] [PubMed] [Google Scholar]
- 10.World Medical Association . WMA Declaration of Helsinki: ethical principles for medical research involving human subjects. 64th WMA General Assembly, Fortaleza, Brazil. October 2013. Accessed November 30, 2020. https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/
- 11.Chikaishi Y, Kanayama M, Taira A, et al. Effect of erlotinib plus bevacizumab on brain metastases in patients with non-small cell lung cancer. Ann Transl Med. 2018;6(20):401. doi: 10.21037/atm.2018.09.33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hosomi Y, Seto T, Nishio M, et al. Erlotinib plus bevacizumab (EB) versus erlotinib alone (E) as first-line treatment for advanced non-squamous non–small-cell lung cancer (NSCLC) with activating EGFR mutation (mt): JO25567 exploratory subgroup analysis. Abstract 420O. Ann Oncol. 2015;26(suppl 9):ix125. doi: 10.1093/annonc/mdv532.04 [DOI] [Google Scholar]
- 13.Seto T, Kato T, Nishio M, et al. Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol. 2014;15(11):1236-1244. doi: 10.1016/S1470-2045(14)70381-X [DOI] [PubMed] [Google Scholar]
- 14.Stinchcombe TE, Jänne PA, Wang X, et al. Effect of erlotinib plus bevacizumab vs erlotinib alone on progression-free survival in patients with advanced EGFR-mutant non-small cell lung cancer: a phase 2 randomized clinical trial. JAMA Oncol. 2019;5(10):1448-1455. doi: 10.1001/jamaoncol.2019.1847 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ichihara E, Hotta K, Nogami N, et al. Phase II trial of gefitinib in combination with bevacizumab as first-line therapy for advanced non-small cell lung cancer with activating EGFR gene mutations: the Okayama Lung Cancer Study Group Trial 1001. J Thorac Oncol. 2015;10(3):486-491. doi: 10.1097/JTO.0000000000000434 [DOI] [PubMed] [Google Scholar]
- 16.Yu HA, Schoenfeld AJ, Makhnin A, et al. Effect of osimertinib and bevacizumab on progression-free survival for patients with metastatic EGFR-mutant lung cancers: a phase 1/2 single-group open-label trial. JAMA Oncol. 2020;6(7):1048-1054. doi: 10.1001/jamaoncol.2020.1260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Paz-Ares L, Planchard D, Yang JC, et al. CNS activity of ramucirumab in combination with osimertinib in patients with advanced T790M-positive EGFR-mutant NSCLC. J Thorac Oncol. 2018;13(10)(suppl):S453-S454. doi: 10.1016/j.jtho.2018.08.545 [DOI] [Google Scholar]
- 18.Soria JC, Ohe Y, Vansteenkiste J, et al. ; FLAURA Investigators . Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113-125. doi: 10.1056/NEJMoa1713137 [DOI] [PubMed] [Google Scholar]
- 19.Akamatsu H, Katakami N, Okamoto I, et al. Osimertinib in Japanese patients with EGFR T790M mutation-positive advanced non-small-cell lung cancer: AURA3 trial. Cancer Sci. 2018;109(6):1930-1938. doi: 10.1111/cas.13623 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Garon EB, Ciuleanu TE, Arrieta O, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomised phase 3 trial. Lancet. 2014;384(9944):665-673. doi: 10.1016/S0140-6736(14)60845-X [DOI] [PubMed] [Google Scholar]
- 21.Bergers G, Hanahan D. Modes of resistance to anti-angiogenic therapy. Nat Rev Cancer. 2008;8(8):592-603. doi: 10.1038/nrc2442 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Itatani Y, Kawada K, Yamamoto T, Sakai Y. Resistance to anti-angiogenic therapy in cancer-alterations to anti-VEGF pathway. Int J Mol Sci. 2018;19(4):E1232. doi: 10.3390/ijms19041232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yoh K, Hosomi Y, Kasahara K, et al. A randomized, double-blind, phase II study of ramucirumab plus docetaxel vs placebo plus docetaxel in Japanese patients with stage IV non-small cell lung cancer after disease progression on platinum-based therapy. Lung Cancer. 2016;99:186-193. doi: 10.1016/j.lungcan.2016.07.019 [DOI] [PubMed] [Google Scholar]
- 24.Takeda M, Yamanaka T, Seto T, et al. Bevacizumab beyond disease progression after first-line treatment with bevacizumab plus chemotherapy in advanced nonsquamous non-small cell lung cancer (West Japan Oncology Group 5910L): an open-label, randomized, phase 2 trial. Cancer. 2016;122(7):1050-1059. doi: 10.1002/cncr.29893 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eTable 1. Patients’ characteristics in lead-in part
eTable 2. Adverse events in lead-in part (more than 33%)
eTable 3. Adverse events in each arm (more than 20% or special interest)
eTable 4. Treatment exposure and reasons of interruption or discontinuation
eTable 5. Post-study treatment
eFigure 1. Kaplan-Meier curve of progression-free survival in lead-in part
eFigure 2. Subgroup analysis of progression-free survival in phase II
eFigure 3. Post-hoc analysis of progression-free survival in arm B depending on discontinuation of bevacizumab
Data Sharing Statement