

Abstract
Background
GDF15 (growth differentiation factor 15) and NT‐proBNP (N‐terminal pro‐B‐type natriuretic peptide) may offer promise as biomarkers for cognitive outcomes, including dementia. We determined the association of these biomarkers with cognitive outcomes in a community‐based cohort.
Methods and Results
Plasma GDF15 (n=1603) and NT‐proBNP levels (n=1590) (53% women; mean age, 68.7 years) were measured in dementia‐free Framingham Offspring cohort participants at examination 7 (1998–2001). Participants were followed up for incident dementia. Secondary outcomes included Alzheimer disease dementia, magnetic resonance imaging structural brain measures, and neurocognitive performance. During a median 11.8‐year follow‐up, 131 participants developed dementia. On multivariable Cox proportional‐hazards analysis, higher circulating GDF15 was associated with an increased risk of incident all‐cause and Alzheimer disease dementia (hazard ratio [HR] per SD increment in natural log‐transformed biomarker value, 1.54 [95% CI, 1.22–1.95] and 1.37 [95% CI, 1.03–1.81], respectively), whereas higher plasma NT‐proBNP was also associated with an increased risk of all‐cause dementia (HR, 1.32; 95% CI, 1.05–1.65). Elevated GDF15 was associated with lower total brain and hippocampal volumes, greater white matter hyperintensity volume, and poorer cognitive performance. Elevated NT‐proBNP was associated with greater white matter hyperintensity volume and poorer cognitive performance. Addition of both biomarkers to a conventional risk factor model improved dementia risk classification (net reclassification improvement index, 0.25; 95% CI, 0.05–0.45).
Conclusions
Elevated plasma GDF15 and NT‐proBNP were associated with vascular brain injury on magnetic resonance imaging, poorer neurocognitive performance, and increased risk of incident dementia in individuals aged >60 years. Both biomarkers improved dementia risk classification beyond that of traditional clinical risk factors, indicating their potential value in predicting incident dementia.
Keywords: biomarker, dementia, vascular cognitive impairment
Subject Categories: Biomarkers, Cognitive Impairment, Cerebrovascular Disease/Stroke, Aging
Nonstandard Abbreviations and Acronyms
- ApoE4
apolipoprotein E4
- DM
diabetes mellitus
- FHS
Framingham Heart Study
- WMHV
white matter hyperintensity volume
Clinical Perspective
What Is New?
This is the first study to report an association between elevated plasma levels of growth differentiation factor 15 and cognitive decline and incident dementia.
Our results validate findings from previous studies reporting an association between elevated circulating NT‐proBNP (N‐terminal pro‐B‐type natriuretic peptide) levels and risk of incident dementia in a community‐based sample of cognitively healthy adults.
Elevated plasma levels of both biomarkers were also cross‐sectionally associated with evidence of vascular injury on magnetic resonance imaging brain (namely, white matter disease hyperintensity volume).
What Are the Clinical Implications?
Both growth differentiation factor 15 and NT‐proBNP improved dementia risk classification beyond that of traditional clinical risk factors, such as hypertension and vascular disease.
Growth differentiation factor 15 and NT‐proBNP offer promise as potential biomarkers for predicting the risk of vascular cognitive impairment and dementia.
Identifying novel biomarkers predictive of increased dementia risk can further our understanding of the complex biological pathways underlying dementia, identify future potential therapeutic targets, and improve overall dementia risk prediction. The plasma biomarkers, GDF15 (growth differentiation factor 15) and NT‐proBNP (N‐terminal pro‐B‐type natriuretic peptide), offer promise as potential biomarkers for adverse cognitive outcomes. GDF15, also known as macrophage inhibitory cytokine‐1, is a member of the transforming growth factor‐b superfamily. Within the nervous system, GDF15 is synthesized by lesioned neurons, microglial cells, and choroid plexus, and plays regulatory roles in inflammation and proapoptosis and antiapoptosis in injured tissues. 1 , 2 , 3 It is also believed to be a marker of vascular stress and endothelial dysfunction, 4 and has previously been associated with cardiovascular outcomes, including myocardial infarction. 5 , 6 Previous studies have reported an association between elevated plasma GDF15 levels and poorer cognitive performance, a trend toward greater short‐term cognitive decline, and an increased burden of white matter disease as well as lower total brain volume. 7 , 8 , 9 However, it is unknown if GDF15 is predictive of an increased risk of cognitive decline over a longer duration of follow‐up or with clinically confirmed dementia.
NT‐proBNP, a marker of ventricular distention, has previously been associated with an increased risk of adverse cognitive outcomes, including incident dementia. 10 , 11 , 12 , 13 , 14 , 15 , 16 , 17 However, some of the prior studies on dementia were limited by small sample sizes, use of registry‐based diagnoses rather than clinically confirmed dementia, and inclusion of older individuals (aged >75 years) or those with diabetes mellitus (DM), in whom the prevalence of cardiac failure is higher. Validating the results of prior studies 13 , 17 in a community‐based cohort of cognitively healthy adults would further support a potential role of NT‐proBNP in dementia risk stratification.
In the present study, we determined the associations of plasma GDF15 and NT‐proBNP levels, individually and jointly, with neurocognitive performance, structural magnetic resonance imaging (MRI) brain measures predictive of dementia, and clinically confirmed all‐cause and Alzheimer disease (AD) dementia, in a community‐based, prospective cohort.
METHODS
Anonymized data and materials have been made publicly available at the National Heart, Lung, and Blood Institute and can be accessed at https://biolincc.nhlbi.nih.gov/home/ and https://www.ncbi.nlm.nih.gov/gap/.
Study Sample
The Framingham Offspring cohort, recruited between 1971 and 1975, is a large, community‐based cohort longitudinally followed up for the development of vascular risk factors, cognitive decline, stroke, and dementia for >40 years. 18 Participants are examined approximately every 4 years from study entry. For this study, we included Framingham Offspring cohort participants attending the seventh examination cycle (1998–2001) who had plasma biomarkers measured at this examination, who were free of a diagnosis of dementia, and who had data available on dementia status on follow‐up. We excluded individuals aged <60 years at baseline (examination 7) because of the negligible number of incident dementia cases in our cohort before the age of 60 years. The Figure shows the flow of cohort participants. All participants provided written informed consent. The study protocols and consent forms were approved by the institutional review board at the Boston University Medical Center.
Figure 1. Flow of cohort participants.
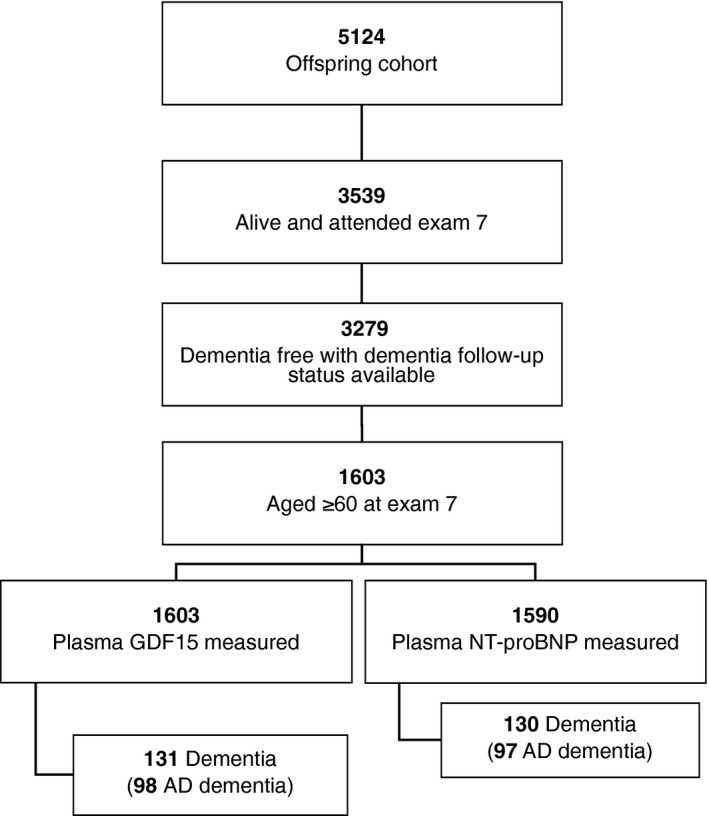
AD indicates Alzheimer disease; GDF15, growth differentiation factor 15; and NT‐proBNP, N‐terminal pro‐B‐type natriuretic peptide.
Outcome Measures
Our primary outcome measure was incident all‐cause dementia developing at any time after the seventh examination and before December 2014. A diagnosis of dementia was based on a review of available neurological examination records, neuropsychological assessments, results of neuroimaging investigations, hospital/nursing home/outpatient clinic records, information from family interviews, and autopsy results (when available) by a committee that included at least one neuropsychologist and one neurologist. Dementia was diagnosed according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria, necessitating impairment in memory and at least one other domain of cognitive function, as well as documented functional disability. AD dementia was included as a secondary outcome measure, and the diagnosis was based on the criteria of the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association for definite, probable, or possible AD. 19 Additional secondary outcomes included cognitive performance at examination 7 and annualized change in performance on select neuropsychological tests between examinations 7 and 8, including the trail making test (parts B and A), Hooper visual organization test, visual reproductions delayed recall, similarities test, and logical memory delayed recall and a weighted global cognitive test score as a measure of general cognition. We also evaluated structural MRI brain measures at examination 7, including white matter hyperintensity volume (WMHV), covert brain infarcts, total brain volume, and hippocampal volume as secondary outcomes. Further details on outcome measures, including neurocognitive testing and MRI brain measures, have previously been published and are included in Data S1. 20 , 21
Laboratory Measurements of GDF15 and NT‐proBNP
GDF15 and NT‐proBNP were measured as part of the Systems Approach to Biomarker Research in Cardiovascular Disease Initiative. 22 We selected GDF15 and NT‐proBNP from this biomarker panel for inclusion in this study on the basis of a priori evidence of a biologically plausible association with cognitive decline and dementia. Blood plasma samples were obtained at the baseline clinical visit (examination 7). Fasting blood samples were drawn in the early morning from the antecubital vein of participants who had been lying supine for 10 minutes. Samples were centrifuged immediately and stored at −80°C until assays were performed. GDF15 and NT‐proBNP were assayed using a modified ELISA sandwich approach, multiplexed on a Luminex xMAP platform (Sigma‐Aldrich, St. Louis, MO). More detailed assay methods have previously been published. 22 For GDF15, the lower detection limit was 40 pg/L and the upper detection limit was 20 600 pg/mL. The interassay coefficient of variation ranged from 6.8% to 11.9%. For NT‐proBNP, the lower and upper detection limits were 9.71 and 30 100 pg/mL, respectively. The interassay coefficient of variation ranged from 10.3% to 13.3%.
Covariates
We adjusted for baseline demographics and clinical covariates (measured at examination cycle 7), which have previously been associated with risk of dementia 23 (variables were selected on the basis of clinical importance and evidence of prior associations), including age, sex, education (self‐reported and categorized as no high school degree, high school degree but no college degree, some college but no degree, and college degree or higher), systolic blood pressure/use of antihypertensive medication, apolipoprotein E4 (ApoE4) carrier status (a carrier was defined as E2/E4, E3/E4, or E4/E4; a noncarrier was defined as E2/E2, E2/E3, or E3/E3), body mass index, current smoking, estimated glomerular filtration rate, prevalent DM, and prevalent cardiovascular disease (CVD; which included peripheral vascular disease [including intermittent claudication]; coronary artery disease [including coronary insufficiency, angina, and myocardial infarction]; cerebrovascular disease [including transient ischemic attack and stroke]; and congestive heart failure]).
Statistical Analysis
To evaluate GDF15 and NT‐proBNP as continuous variables (primary analysis), we natural logarithmically transformed and standardized biomarker values to normalize their distributions and facilitate comparisons. We also calculated tertiles of plasma GDF15 and NT‐proBNP, comparing the top tertiles with the bottom tertile given an apparent threshold effect at this cutoff for GDF15 using cubic spline plots. We used multivariable‐adjusted Cox proportional hazards models to estimate the association between plasma GDF15 and NT‐proBNP levels (natural logarithmically transformed values and tertiles) and risk of incident all‐cause dementia and AD dementia. Participants were followed up from baseline (examination 7) to the time of the incident event. Participants without incident events were followed up to the time of death or date the participant was last confirmed to be event free (up until December 2014). The assumption of proportional hazards was upheld, and results were reported as hazard ratios (HRs) with corresponding 95% CIs. Model 1 adjusted for age and sex; model 2 (primary model) additionally adjusted for education, systolic blood pressure, use of antihypertensive medication, ApoE4 carrier status, body mass index, current smoking, estimated glomerular filtration rate, prevalent DM, and prevalent CVD; and model 3 additionally adjusted for plasma biomarkers (ie, we adjusted for NT‐proBNP in the GDF15 model, and vice versa). We evaluated model discrimination (C‐statistic and integrated discrimination improvement) and improvement in risk prediction (net reclassification improvement index) for incident all‐cause and AD dementia, following the addition of individual and combined biomarkers to the models.
We used logistic and linear regression models to evaluate the cross‐sectional associations between plasma biomarker levels and MRI‐based structural brain measures, including covert brain infarcts, WMHV, total brain volume, and hippocampal volume, adjusting for age, age squared (given age and brain volume show a nonlinear association), sex, time from blood draw to MRI brain, systolic blood pressure, use of antihypertensive medication, body mass index, current smoking, estimated glomerular filtration rate, prevalent DM, and prevalent CVD. We fit linear regression models to examine (1) the cross‐sectional association between plasma biomarker levels and neuropsychological test performance at examination 7 and (2) the association between plasma biomarkers and annualized change in neuropsychological performance between examinations 7 and 8, adjusting for the covariates listed above. We tested for an interaction for all‐cause and AD dementia according to ApoE4 carrier status. We completed sensitivity analyses excluding individuals with a history of stroke (n=42) and those with prevalent congestive heart failure (n=26), as well as using clinical cutoffs (NT‐proBNP, 0–<125, 125–<300, and ≥300 pg/mL), similar to those used in a prior recent study. 17 Finally, we completed a summary meta‐analysis of combined results from the FHS (Framingham Heart Study) and Hisayama cohorts, 17 adjusting for age and sex, using a fixed effects models because of the low level of heterogeneity between studies (I2=29% for dementia analysis and 20% for AD dementia analysis). Results were considered significant if P<0.05 for the main analyses and P<0.10 for tests for interactions. Analyses were conducted using SAS v9.4 (SAS Institute Inc, Cary, NC).
Results
For the primary outcome analysis of dementia, the study cohort included 1603 participants for GDF15 and 1590 participants for NT‐proBNP. The mean age of participants was 68.7 years (SD, 5.7 years), and 52.7% were women (Table 1). Compared with those in the bottom tertile of GDF15, participants in the top tertile had a higher prevalence of vascular risk factors and disease, including CVD, atrial fibrillation, and prior stroke. Participants in the top tertile of NT‐proBNP, compared with the bottom tertile, similarly had an increased vascular risk profile (Table 1). Baseline characteristics according to clinical cutoffs for NT‐proBNP (NT‐proBNP, 0–<125, 125–<300, and ≥300 pg/mL) are presented in Table S1.
Table 1.
Baseline Characteristics
|
Variable |
Overall (n=1603) |
GDF15 | NT‐proBNP | ||||
|---|---|---|---|---|---|---|---|
|
Tertile 1 (n=533) |
Tertile 2 (n=536) |
Tertile 3 (n=534) |
Tertile 1 (n=528) |
Tertile 2 (n=531) |
Tertile 3 (n=531) |
||
| Age, mean (SD), y | 68.7 (5.7) | 68.0 (5.7) | 68.6 (5.7) | 69.5 (5.6) | 68.3 (5.8) | 68.6 (5.7) | 69.1 (5.6) |
| Women | 844 (52.7) | 304 (36.0) | 281 (33.3) | 259 (30.7) | 216 (25.8) | 313 (37.4) | 308 (36.8) |
| Systolic blood pressure, mean (SD), mm Hg | 132.3 (19.2) | 132.0 (19.0) | 132.4 (18.8) | 132.6 (19.9) | 130.2 (15.6) | 132.3 (18.7) | 134.4 (22.2) |
| BMI, median (quartile 1–quartile 3), kg/m2 | 27.4 (24.7–30.9) | 27.1 (24.6–29.9) | 27.3 (24.7–30.7) | 28.0 (24.8–31.7) | 28.2 (25.3–31.1) | 27.5 (24.8–30.4) | 26.7 (23.9–30.6) |
| GDF15, median (quartile 1–quartile 3), pg/mL | 766.0 (602.0–1010.0) | 552.0 (488.0–633.0) | 749.0 (661.0–879.0) | 1165.0 (936.0–1540.0) | 716.5 (577.5–916.5) | 746.0 (593.0–974.0) | 831.0 (656.0–1150.0) |
| NT‐proBNP, median (quartile 1–quartile 3), pg/mL | 272.5 (130.0–538.0) | 224.0 (116.0–412.0) | 265.5 (128.0–495.0) | 364.5 (155.5–798.5) | 95.0 (63.3–130.0) | 265.0 (192.0–366.0) | 752.0 (487.0–1190.0) |
| Education | |||||||
| No high school degree | 101 (6.5) | 22 (21.8) | 31 (30.7) | 48 (47.5) | 28 (27.7) | 30 (29.7) | 43 (42.6) |
| High school degree | 527 (33.8) | 158 (30.0) | 183 (34.7) | 186 (35.3) | 179 (34.2) | 172 (32.9) | 172 (32.9) |
| Some years of college | 452 (29.0) | 148 (32.7) | 158 (35.0) | 146 (32.3) | 150 (33.4) | 158 (35.2) | 141 (31.4) |
| College degree | 478 (30.7) | 188 (39.3) | 155 (32.4) | 135 (28.2) | 155 (32.8) | 160 (33.9) | 157 (33.3) |
| Antihypertensive medication | 702 (43.9) | 187 (26.6 | 219 (31.2) | 296 (42.2) | 189 (27.1) | 217 (31.1) | 292 (41.8) |
| Current smoker | 135 (8.4) | 14 (10.4) | 36 (26.7) | 85 (63.0) | 44 (32.8) | 55 (41.0) | 35 (26.1) |
| ApoE4 allele | 356 (22.5) | 110 (30.9) | 110 (30.9) | 136 (38.2) | 102 (28.9) | 116 (32.9) | 135 (38.2) |
| Prevalent CVD | 303 (18.9) | 54 (17.8) | 95 (31.4) | 154 (50.8) | 57 (19.1) | 71 (23.8) | 171 (57.2) |
| Atrial fibrillation | 95 (5.9) | 17 (17.9) | 34 (35.8) | 44 (46.3) | 12 (12.6) | 14 (14.7) | 69 (72.6) |
| Stroke | 42 (2.6) | 7 (16.7) | 9 (21.4) | 26 (61.9) | 11 (26.8) | 9 (20.0) | 21 (51.2) |
| CHF | 26 (1.6) | 0 (0.0) | 6 (23.1) | 20 (76.9) | 2 (7.7) | 1 (3.9) | 23 (88.5) |
| eGFR, median (quartile 1–quartile 3), mL/min | 77.5 (66.3–87.2) | 81.7 (71.6–89.3) | 78.2 (67.7–87.4) | 70.6 (56.7–83.6) | 79.8 (68.4–88.4) | 78.2 (67.3–87.1) | 74.3 (63.4–85.8) |
| Diabetes mellitus | 263 (16.6) | 59 (22.4) | 59 (22.4) | 145 (55.1) | 92 (35.4) | 75 (28.9) | 93 (35.8) |
Data are given as number (percentage), unless otherwise indicated. Baseline demographic and clinical characteristics were defined at examination 7. Stroke and CHF are included in prevalent CVD. The mean (SD) for natural log‐transformed GDF15 was 6.7 (0.4); and it was 5.6 (1.1) for NT‐proBNP. ApoE4 indicates apolipoprotein E4; BMI, body mass index; CHF, congestive heart failure; CVD, cardiovascular disease; eGFR, estimated glomerular filtration rate; GDF15, growth differentiation factor 15; and NT‐proBNP, N‐terminal pro‐B‐type natriuretic peptide.
GDF15, NT‐proBNP, and Dementia
During a median (quartile 1–quartile 3) 11.8 (7.1–13.3) year follow‐up, 131 (8.2%) participants were diagnosed with all‐cause dementia, 98 of whom were diagnosed with AD dementia. On multivariable proportional‐hazards analysis, adjusting for education status, vascular risk factors, and ApoE4 status, GDF15 was associated with an increased risk of all‐cause dementia (HR, 1.54; 95% CI, 1.22–1.95) and AD dementia (HR, 1.37; 95% CI, 1.03–1.81) per SD increment in natural log‐transformed biomarker value. After accounting for NT‐proBNP, the association was further attenuated but remained significant for all‐cause dementia but not AD dementia. Results were consistent on tertile analysis (Tables 2 and 3). There was an interaction according to ApoE4 allele carrier status and risk of AD dementia (P=0.06), with an increased risk in those without the ApoE4 allele (HR, 2.02; 95% CI, 1.22–3.36). NT‐proBNP was associated with an increased risk of dementia (HR, 1.32; 95% CI, 1.05–1.65) but not AD dementia (HR, 1.23; 95% CI, 0.95–1.61) per SD increase in natural log‐transformed value (Tables 2 and 3). There was also a significant interaction with ApoE4 allele carrier status (P=0.085), such that the risk of AD dementia associated with NT‐proBNP was greater in people without the ApoE4 allele (HR, 2.00; 95% CI, 1.17–3.42), in whom vascular factors may play a larger role. Excluding those with prior stroke and those with a history of congestive heart failure did not significantly alter the results (Tables S2 and S3). In analyses based on clinical cutoffs (NT‐proBNP levels of 125–<300 and ≥300 pg/mL, compared with a reference of <125 pg/mL), results were consistent although did not reach significance, likely because of the smaller proportion of individuals with lower NT‐proBNP levels in our cohort (Table S4). In a summary meta‐analysis of the FHS and Hisayama cohorts combined, NT‐proBNP was also associated with an increased risk of dementia (HR, 1.42; 95% CI, 1.30–1.56) and AD dementia (HR, 1.31; 95% CI, 1.16–148) per average SD increment in natural log‐transformed biomarker value (Table S5).
Table 2.
GDF15 and NT‐proBNP and Risk of Incident Dementia
| Biomarker | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
|
HR (95% CI) |
P Value |
HR (95% CI) |
P Value |
HR (95% CI) |
P Value | |
| GDF15 | ||||||
| Per SDU increase | 1.57 (1.30–1.90) | <0.0001 | 1.54 (1.22–1.95) | 0.0004 | 1.45 (1.13–1.85) | 0.003 |
| T2 vs T1 | 1.26 (0.78–2.02) | 0.35 | 1.33 (0.82–2.16) | 0.25 | 1.28 (0.79–2.10) | 0.32 |
| T3 vs T1 | 2.49 (1.61–3.87) | <0.001 | 2.36 (1.45–3.83) | <0.001 | 2.16 (1.31–3.56) | 0.003 |
| NT‐proBNP | ||||||
| Per SDU increase | 1.40 (1.14–1.71) | 0.001 | 1.32 (1.05–1.65) | 0.02 | 1.25 (0.99–1.56) | 0.06 |
| T2 vs T1 | 0.89 (0.56–1.41) | 0.61 | 0.79 (0.49–1.28) | 0.34 | 0.75 (0.47–1.21) | 0.24 |
| T3 vs T1 | 1.82 (1.20–2.75) | 0.005 | 1.62 (1.03–2.55) | 0.04 | 1.43 (0.90–2.28) | 0.13 |
Model 1, adjusted for age and sex. Model 2, adjusted for age, sex, education, systolic blood pressure, use of antihypertensive medication, body mass index, current smoking, estimated glomerular filtration rate, prevalent diabetes mellitus, prevalent cardiovascular disease, and apolipoprotein E4 carrier status. Model 3, model 2+adjustment for GDF15 (NT‐proBNP analysis) and NT‐proBNP (GDF15 analysis). GDF15 and NT‐proBNP were natural logarithmically transformed and standardized. GDF15 indicates growth differentiation factor 15; HR, hazard ratio; NT‐proBNP, N‐terminal pro‐B‐type natriuretic peptide; SDU, SD unit; T1, tertile 1; T2, tertile 2; and T3, tertile 3.
Table 3.
GDF15 and NT‐proBNP and Risk of Incident AD Dementia
| Biomarker | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
|
HR (95% CI) |
P Value |
HR (95% CI) |
P Value |
HR (95% CI) |
P Value | |
| GDF15 | ||||||
| Per SDU increase | 1.48 (1.18–1.86) | <0.001 | 1.37 (1.03–1.81) | 0.03 | 1.28 (0.96–1.72) | 0.09 |
| T2 vs T1 | 0.97 (0.56–1.68) | 0.92 | 1.01 (0.58–1.77) | 0.96 | 0.99 (0.56–1.75) | 0.98 |
| T3 vs T1 | 2.37 (1.45–3.85) | <0.001 | 2.07 (1.20–3.56) | 0.009 | 1.95 (1.12–3.42) | 0.02 |
| NT‐proBNP | ||||||
| Per SDU increase | 1.34 (1.06–1.70) | 0.02 | 1.23 (0.95–1.61) | 0.12 | 1.19 (0.91–1.55) | 0.21 |
| T2 vs T1 | 0.94 (0.56–1.58) | 0.81 | 0.80 (0.47–1.38) | 0.43 | 0.78 (0.45–1.33) | 0.36 |
| T3 vs T1 | 1.60 (0.98–2.61) | 0.06 | 1.37 (0.80–2.32) | 0.25 | 1.23 (0.71–2.13) | 0.45 |
Model 1, adjusted for age and sex. Model 2, adjusted for age, sex, education, systolic blood pressure, use of antihypertensive medication, body mass index, current smoking, estimated glomerular filtration rate, prevalent diabetes mellitus, prevalent cardiovascular disease, and apolipoprotein E4 carrier status. Model 3, model 2+adjustment for GDF15 (NT‐proBNP analysis) and NT‐proBNP (GDF15 analysis). GDF15 and NT‐proBNP were natural logarithmically transformed and standardized. AD indicates Alzheimer disease; GDF15, growth differentiation factor 15; HR, hazard ratio; NT‐proBNP, N‐terminal pro‐B‐type natriuretic peptide; SDU, SD unit; T1, tertile 1; T2, tertile 2; and T3, tertile 3.
Risk Prediction for Dementia
The C‐statistic for the model of conventional risk factors for dementia was 0.81 (95% CI, 0.77–0.84), with no significant change following the addition of GDF15, NT‐proBNP, or both to the model. However, addition of GDF15 and NT‐proBNP resulted in a relative integrated discrimination improvement of 15% (95% CI, 7%–24%) compared with the base model. Following the addition of both biomarkers to a conventional risk factor model, 18% of individuals with dementia were correctly assigned a higher predicted risk, whereas 7% of individuals without dementia were correctly assigned a lower predicted risk (overall net reclassification improvement, 0.25; 95% CI, 0.05–0.45) (Table S6).
GDF15, NT‐proBNP, and Structural Brain Measures
Elevated GDF15 was associated with lower total brain volume (−0.38±0.06; P<0.001), hippocampal volume (−0.003±0.002; P=0.046), and greater WMHV (0.07±0.03; P=0.02) per SD unit increment in natural log‐transformed biomarker value. Results were consistent when GDF15 was assessed by tertiles. Elevated plasma NT‐proBNP was associated with increased WMHV (0.05±0.02; P=0.048; per SD unit increment) but not with other structural MRI brain measures (Table 4).
Table 4.
GDF15, NT‐proBNP, and MRI Markers of Structural Brain Injury
| Biomarker | TBV, % | Hippocampal Volume, % | WMHV, %* | Covert Brain Infarcts | ||||
|---|---|---|---|---|---|---|---|---|
| β±SE | P Value | β±SE | P Value | β±SE | P Value | OR (95% CI) | P Value | |
| GDF15 | ||||||||
| Per SDU increase† | −0.38±0.06 | <0.001 | −0.003±0.002 | 0.046 | 0.07±0.03 | 0.02 | 1.14 (0.92–1.40) | 0.23 |
| T2 vs T1 | 0.05±0.10 | 0.61 | 0.002±0.002 | 0.55 | −0.03±0.05 | 0.60 | 0.92 (0.63–1.35) | 0.53 |
| T3 vs T1 | −0.40±0.11 | <0.001 | −0.002±0.003 | 0.59 | 0.12±0.05 | 0.02 | 1.05 (0.70–1.56) | 0.62 |
| NT‐proBNP | ||||||||
| Per SDU increase† | −0.03±0.05 | 0.51 | 0.0001±0.001 | 0.92 | 0.05±0.02 | 0.048 | 1.08 (0.90–1.30) | 0.39 |
| T2 vs T1 | 0.11±0.10 | 0.30 | −0.0003±0.003 | 0.90 | 0.02±0.05 | 0.70 | 1.32 (0.90–1.92) | 0.18 |
| T3 vs T1 | −0.11±0.11 | 0.29 | −0.001±0.003 | 0.82 | 0.10±0.05 | 0.045 | 1.13 (0.76–1.68) | 0.91 |
Model, adjusted for age, age squared, sex, time from blood draw to MRI brain, systolic blood pressure, use of antihypertensive medication, body mass index, current smoking, estimated glomerular filtration rate, prevalent diabetes mellitus, and prevalent cardiovascular disease. GDF15 indicates growth differentiation factor 15; MRI, magnetic resonance imaging; NT‐proBNP, N‐terminal pro‐B‐type natriuretic peptide; OR, odds ratio; SDU, SD unit; T1, tertile 1; T2, tertile 2; T3, tertile 3; TBV, total brain volume; and WMHV, white matter hyperintensity volume.
Natural log transformed.
Natural log transformed and standardized.
GDF15, NT‐proBNP, and Neurocognitive Performance
Elevated circulating GDF15 levels were cross‐sectionally associated with poorer global cognitive performance (ß±SE, −0.08±0.02; P=0.002), as well as poorer performance on individual tests of abstract reasoning (similarities, −0.20±0.10; P=0.04), visual memory (visual reproductions delayed recall, −0.24±0.09; P=0.009), and visuospatial processing (Hooper visual organization test, −0.03±0.01; P=0.02), per SD increment in natural log‐transformed GDF15 value. Higher circulating NT‐proBNP was also cross‐sectionally associated with poorer global cognitive performance (−0.04±0.02; P=0.03) as well as poorer performance on visual reproductions delayed recall (−0.16±0.08; P=0.04), per SD increment in natural log‐transformed NT‐proBNP value (Table S7). Elevated plasma GDF15 levels were also associated with greater annualized decline in performance on tests of global cognition, logical memory, executive function, and visuospatial processing (Table S8).
Discussion
In our study, we observed that elevated plasma levels of GDF15 and NT‐proBNP were associated with an increased risk of incident dementia over a median 12‐year follow‐up. Both biomarkers improved dementia risk classification beyond that of traditional clinical risk factors.
Elevated plasma GDF15 and NT‐proBNP were also associated with increased WMHV and poorer cognitive performance, whereas GDF15 alone was associated with lower total brain volume and cognitive decline.
There exists an important need for valid, reliable biomarkers for vascular cognitive impairment and dementia. 24 , 25 Such biomarkers could be used to monitor disease severity and progression, identify disease at a preclinical stage and serve as surrogate outcomes in early‐phase clinical trials of vascular cognitive impairment and dementia, and improve our understanding of underlying disease mechanisms. Both GDF15 and NT‐proBNP offer promise as potential biomarkers for predicting the risk of vascular cognitive impairment and dementia. We observed an increased risk of clinical all‐cause dementia and AD dementia in association with elevated plasma GDF15 levels. Although previous studies have reported an association between elevated plasma GDF15 levels and poorer cognitive performance and a trend toward short‐term (2‐year) cognitive decline, 8 to our knowledge, this is the first study to report an association between plasma GDF15 and both cognitive decline in cognitively normal middle‐aged and older adults and incident clinical dementia and AD dementia. We also found that elevated plasma GDF15 levels were associated with greater annualized decline in performance on tests of global cognition, logical memory, executive function, and visuospatial processing, suggesting that longer follow‐up of this cohort may result in even stronger associations with incident dementia.
GDF15 is believed to be a marker of vascular stress and impaired endothelial function. 4 Elevated circulating GDF15 has previously been associated with cardiovascular outcomes, including myocardial infarction, 5 , 6 suggesting that GDF15 levels may reflect an elevated vascular risk profile. Indeed, in our cohort, individuals in the top tertile of GDF15 had a higher prevalence of vascular risk factors, including current smoking, DM, CVD, and stroke, compared with those in the bottom tertiles. In addition, we observed a cross‐sectional association between elevated plasma GDF15 levels and greater white matter disease burden, which has also previously been reported at a different examination cycle in the Framingham cohort. 7 However, after accounting for the effects of vascular risk factors as well as NT‐proBNP, the association between plasma GDF15 levels and dementia and AD dementia remained significant. In addition, we observed no association between covert brain infarct volume and GDF15 levels. Thus, it is unlikely that increased vascular risk factor burden and subclinical vascular brain injury solely account for these associations. Interestingly, we observed an interaction between circulating GDF15 levels and risk of AD dementia, but not overall dementia, according to ApoE4 carrier status, with an increased risk of AD dementia in those without the ApoE4 allele compared with those with this allele, suggesting that the association with clinical disease in these people is not mediated through ApoE‐related pathways. GDF15 is also known to play a role in inflammation and apoptosis in damaged tissues. 1 , 2 , 3 Elevated GDF15 may be a marker of a proinflammatory environment predisposing to increased white matter disease and subsequent dementia. In a Drosophila model of the neurodegenerative condition, Huntington disease, GDF15 was reported to be upregulated under conditions of stress. Use of pharmacological inhibition and RNA interference to normalize GDF15 function resulted in marked protection against stress‐induced apoptosis as well as Huntington disease–related neurodegeneration (slowing of neuronal loss), suggesting GDF15 may be a potential therapeutic target to modulate the risk of other neurodegenerative diseases, including dementia and AD dementia. 26
We also observed an association between elevated circulating NT‐proBNP levels and risk of clinically confirmed incident dementia but not AD dementia. Previous studies have reported similar associations in an older population and in patients with DM 11 , 12 as well as in 2 larger cohorts of community‐dwelling individuals. 13 , 17 In the Hisayama cohort, serum NT‐proBNP levels of ≥300 pg/mL, compared with ≤54 pg/mL, were associated with an increased risk of all‐cause dementia, after accounting for age and sex (HR, 3.02; 95% CI, 2.08–4.37). 17 In our study, plasma NT‐proBNP levels of ≥300 pg/mL, compared with <125 pg/mL, were not associated with risk of all‐cause dementia after accounting for age and sex, although the trend approached significance (HR, 1.66; 95% CI, 0.95–2.92). Given the small number of individuals with NT‐proBNP ≤54 pg/mL in our study (n=100; 6% of the sample), we were unable to adopt the same reference category used in the Hisayama cohort. Furthermore, >50% of the individuals in our cohort had NT‐proBNP levels ≥300 pg/mL, compared with 11.6% in the Hisayama cohort, further precluding a direct comparison of our results. However, our findings do validate the results of these previous studies among a community‐based population of cognitively healthy adults whose dementia diagnoses were confirmed on the basis of clinical assessments, medical record review by a behavioral neurologist, and rigorous application of standardized criteria. In addition, in a combined summary meta‐analysis of our results with those of the Hisayama cohort, results remained significant with minimal variation in effect sizes attributable to differences between studies.
NT‐proBNP is a marker of left ventricular distention in patients with heart failure and is associated with an increased risk of cardiovascular events, including ischemic stroke and atrial fibrillation. Thus, the association between NT‐proBNP and dementia risk is likely mediated through increased vascular risk and subclinical vascular disease. Indeed, in our cohort, participants in the top tertile of NT‐proBNP, compared with the bottom tertile, had higher baseline systolic blood pressures, and were more likely to be on antihypertensive medication or have a history of atrial fibrillation, CVD, or stroke. Furthermore, we found that NT‐proBNP was associated with MRI brain measures predictive of vascular dementia, including a greater burden of white matter disease, as well as with poorer performance on tests of visual memory and global cognition. The association between plasma NT‐proBNP levels and both dementia and AD dementia was attenuated, and no longer significant, after accounting for vascular risk factors and GDF15 levels, also supporting a vascular‐mediated hypothesis. In 2 previous studies, 13 , 17 elevated serum NT‐proBNP was associated with an increased risk of AD dementia; thus, it is also possible that our study was underpowered to detect an association with AD dementia. Plasma NT‐proBNP is readily available in a clinical setting and offers potential prognostic value as a candidate biomarker for more accurately predicting risk of dementia in cognitively healthy adults, including those without congestive heart failure, although appropriate clinical cutoffs need to be determined.
When looking at the relative integrated discrimination improvement index, we found that addition of GDF15 and NT‐proBNP resulted in a relative integrated discrimination improvement index of 15% compared with the base model, indicating that measurement of these biomarkers provides incremental predictive value beyond that of conventional risk factors. Addition of both biomarkers to conventional risk factors improved dementia risk classification, in that 18% of individuals with dementia were correctly assigned a higher predicted risk of dementia, whereas 7% of individuals without dementia were correctly assigned a lower predicted risk, supporting a potential role for circulating GDF15 and NT‐proBNP as biomarkers for predicting dementia risk.
Our study has several strengths, including a population confirmed to be free of clinical dementia at the baseline examination, use of intensive surveillance procedures to detect new cases of dementia or cognitive decline, comprehensive phenotyping of the cohort, a large number of individuals with measured plasma biomarker values, and a relatively long duration of follow‐up. An important limitation is the predominantly White population, which limits the generalizability of our findings to other ethnicities. In addition, our analyses did not adjust for a history of sleep apnea or cancer. Finally, we were unable to account for changes in plasma biomarker values over time, as data on repeated measures were not available.
Conclusions
Elevated plasma GDF15 and NT‐proBNP are associated with a greater burden of white matter disease, increased brain atrophy (GDF15 alone), poorer cognitive performance, and an increased risk of clinically confirmed dementia and AD dementia (GDF15 alone) in individuals aged >60 years. Both biomarkers improve dementia risk classification beyond that of traditional clinical risk factors. GDF15 and NT‐proBNP may be useful circulating biomarkers for vascular brain injury and dementia in the general population.
Sources of Funding
The FHS (Framingham Heart Study) is supported by the National Heart, Lung, and Blood Institute (NHLBI) (contract Nos. N01‐HC‐25195, HHSN268201500001, and 75N92019D00031). This research was supported by an Alzheimer's Association Clinician Scientist Fellowship (AACSF‐18‐566570), NHLBI grants R01 HL60040 and R01 HL70100, grants from the National Institute on Aging (R01 AG054076, R01 AG049607, R01 AG033193, U01 AG049505, and U01 AG052409), and grants from the National Institute of Neurological Disorders and Stroke (NS017950 and UH2 NS100605). Additional funding for the Systems Approach to Biomarker Research in Cardiovascular Disease initiative was provided by the Division of Intramural Research, NHLBI, and the Population Sciences Branch, NHLBI. None of the funding entities had any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Disclosures
None.
Supporting information
Acknowledgments
The authors would like to acknowledge the contribution of the FHS (Framingham Heart Study) participants. Dr McGrath had full access to all the data in the study and takes responsibility for their integrity and the data analysis.
(J Am Heart Assoc. 2020;9:e014659 DOI: 10.1161/JAHA.119.014659.)
Supplementary materials for this article are available at https://www.ahajournals.org/doi/suppl/10.1161/JAHA.119.014659
*Current address: Turner Institute, Monash University, Clayton, Victoria, Australia and Harvard University, Boston, MA.For Sources of Funding and Disclosures, see page 9.
References
- 1. Bootcov MR, Bauskin AR, Valenzuela SM, Moore AG, Bansal M, He XY, Zhang HP, Donnellan M, Mahler S, Pryor K, et al. MIC-1, a novel macrophage inhibitory cytokine, is a divergent member of the TGF‐beta superfamily. Proc Natl Acad Sci USA. 1997;94:11514–11519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Xu X, Li Z, Gao W. Growth differentiation factor 15 in cardiovascular diseases: from bench to bedside. Biomarkers. 2011;16:466–475. [DOI] [PubMed] [Google Scholar]
- 3. Unsicker K, Spittau B, Krieglstein K. The multiple facets of the tgf‐beta family cytokine growth/differentiation factor-15/macrophage inhibitory cytokine‐1. Cytokine Growth Factor Rev. 2013;24:373–384. [DOI] [PubMed] [Google Scholar]
- 4. Lind L, Wallentin L, Kempf T, Tapken H, Quint A, Lindahl B, Olofsson S, Venge P, Larsson A, Hulthe J, et al. Growth‐differentiation factor-15 is an independent marker of cardiovascular dysfunction and disease in the elderly: results from the Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) study. Eur Heart J. 2009;30:2346–2353. [DOI] [PubMed] [Google Scholar]
- 5. Kempf T, Bjorklund E, Olofsson S, Lindahl B, Allhoff T, Peter T, Tongers J, Wollert KC, Wallentin L. Growth‐differentiation factor-15 improves risk stratification in ST‐segment elevation myocardial infarction. Eur Heart J. 2007;28:2858–2865. [DOI] [PubMed] [Google Scholar]
- 6. Wollert KC, Kempf T, Lagerqvist B, Lindahl B, Olofsson S, Allhoff T, Peter T, Siegbahn A, Venge P, Drexler H, et al. Growth differentiation factor 15 for risk stratification and selection of an invasive treatment strategy in non ST‐elevation acute coronary syndrome. Circulation. 2007;116:1540–1548. [DOI] [PubMed] [Google Scholar]
- 7. Andersson C, Preis SR, Beiser A, DeCarli C, Wollert KC, Wang TJ, Januzzi JL Jr, Vasan RS, Seshadri S. Associations of circulating growth differentiation factor-15 and ST2 concentrations with subclinical vascular brain injury and incident stroke. Stroke. 2015;46:2568–2575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Fuchs T, Trollor JN, Crawford J, Brown DA, Baune BT, Samaras K, Campbell L, Breit SN, Brodaty H, Sachdev P, et al. Macrophage inhibitory cytokine‐1 is associated with cognitive impairment and predicts cognitive decline—the Sydney Memory and Aging Study. Aging Cell. 2013;12:882–889. [DOI] [PubMed] [Google Scholar]
- 9. Chai YL, Hilal S, Chong JP, Ng YX, Liew OW, Xu X, Ikram MK, Venketasubramanian N, Richards AM, Lai MK, et al. Growth differentiation factor-15 and white matter hyperintensities in cognitive impairment and dementia. Medicine. 2016;95:e4566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Tynkkynen J, Laatikainen T, Salomaa V, Havulinna AS, Blankenberg S, Zeller T, Hernesniemi JA. NT‐proBNP and the risk of dementia: a prospective cohort study with 14 years of follow‐up. J Alzheimers Dis. 2015;44:1007–1013. [DOI] [PubMed] [Google Scholar]
- 11. Kerola T, Nieminen T, Hartikainen S, Sulkava R, Vuolteenaho O, Kettunen R. B‐type natriuretic peptide as a predictor of declining cognitive function and dementia—a cohort study of an elderly general population with a 5‐year follow‐up. Ann Med. 2010;42:207–215. [DOI] [PubMed] [Google Scholar]
- 12. Feinkohl I, Keller M, Robertson CM, Morling JR, Williamson RM, Nee LD, McLachlan S, Sattar N, Welsh P, Reynolds RM, et al. Clinical and subclinical macrovascular disease as predictors of cognitive decline in older patients with type 2 diabetes: the Edinburgh Type 2 Diabetes Study. Diabetes Care. 2013;36:2779–2786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Mirza SS, de Bruijn RF, Koudstaal PJ, van den Meiracker AH, Franco OH, Hofman A, Tiemeier H, Ikram MA. The N‐terminal pro B‐type natriuretic peptide, and risk of dementia and cognitive decline: a 10‐year follow‐up study in the general population. J Neurol Neurosurg Psychiatry. 2016;87:356–362. [DOI] [PubMed] [Google Scholar]
- 14. Ferguson IT, Elbejjani M, Sabayan B, Jacobs DR Jr, Meirelles O, Sanchez OA, Tracy R, Bryan N, Launer LJ. N‐terminal pro‐brain natriuretic peptide and associations with brain magnetic resonance imaging (MRI) features in middle age: the CARDIA brain MRI study. Front Neurol. 2018;9:307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Sabayan B, van Buchem MA, Sigurdsson S, Zhang Q, Meirelles O, Harris TB, Gudnason V, Arai AE, Launer LJ. Cardiac and carotid markers link with accelerated brain atrophy: the AGES‐Reykjavik Study (Age, Gene/Environment Susceptibility‐Reykjavik). Arterioscler Thromb Vasc Biol. 2016;36:2246–2251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Wijsman LW, Sabayan B, van Vliet P, Trompet S, de Ruijter W, Poortvliet RK, van Peet PG, Gussekloo J, Jukema JW, Stott DJ, et al. N‐terminal pro‐brain natriuretic peptide and cognitive decline in older adults at high cardiovascular risk. Ann Neurol. 2014;76:213–222. [DOI] [PubMed] [Google Scholar]
- 17. Nagata T, Ohara T, Hata J, Sakata S, Furuta Y, Yoshida D, Honda T, Hirakawa Y, Ide T, Kanba S, et al. NT‐proBNP and risk of dementia in a general Japanese elderly population: the Hisayama study. J Am Heart Assoc. 2019;8:e011652 DOI: 10.1161/JAHA.118.011652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Feinleib M, Kannel WB, Garrison RJ, McNamara PM, Castelli WP. The Framingham Offspring Study: design and preliminary data. Prev Med. 1975;4:518–525. [DOI] [PubMed] [Google Scholar]
- 19. McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS‐ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology. 1984;34:939–944. [DOI] [PubMed] [Google Scholar]
- 20. Au R, Seshadri S, Wolf PA, Elias M, Elias P, Sullivan L, Beiser A, D'Agostino RB. New norms for a new generation: cognitive performance in the Framingham offspring cohort. Exp Aging Res. 2004;30:333–358. [DOI] [PubMed] [Google Scholar]
- 21. McGrath ER, Himali JH, Levy D, Connor SC, Beiser A, Courchesne P, Satizabal C, Pase MP, Vasan RS, Beiser AS, et al. Circulating IGFBP-2: a novel biomarker for incident dementia. Ann Clin Transl Neurol. 2019;6:1659–1670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Ho JE, Lyass A, Courchesne P, Chen G, Liu C, Yin X, Hwang SJ, Massaro JM, Larson MG, Levy D. Protein biomarkers of cardiovascular disease and mortality in the community. J Am Heart Assoc. 2018;7:e008108 DOI: 10.1161/JAHA.117.008108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. McGrath ER, Beiser AS, DeCarli C, Plourde KL, Vasan RS, Greenberg SM, Seshadri S. Blood pressure from mid- to late life and risk of incident dementia. Neurology. 2017;89:2447–2454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Smith EE, Cieslak A, Barber P, Chen J, Chen YW, Donnini I, Edwards JD, Frayne R, Field TS, Hegedus J, et al. Therapeutic strategies and drug development for vascular cognitive impairment. J Am Heart Assoc. 2017;6:e005568 DOI: 10.1161/JAHA.117.005568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Corriveau RA, McGavern L, Albert MS, Arfanakis K, Arvind C, DeCarli CS, Fornage M, Helmer KG, Jicha GA, Kashani AH, et al. MARKVCID phase II: prioritized candidate small vessel VCID biomarkers selected for multi‐site testing and validation. Alzheimers Dement. 2018;14:P1670–P1671. [Google Scholar]
- 26. Varadarajan S, Breda C, Smalley JL, Butterworth M, Farrow SN, Giorgini F, Cohen GM. The transrepression arm of glucocorticoid receptor signaling is protective in mutant huntingtin‐mediated neurodegeneration. Cell Death Differ. 2015;22:1388–1396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Seshadri S, Wolf P, Beiser A, Au R, McNulty K, White R, D'agostino R. Lifetime risk of dementia and Alzheimer's disease the impact of mortality on risk estimates in the Framingham study. Neurology. 1997;49:1498–1504. [DOI] [PubMed] [Google Scholar]
- 28. Aljabar P, Heckemann RA, Hammers A, Hajnal JV, Rueckert D. Multi‐atlas based segmentation of brain images: atlas selection and its effect on accuracy. Neuroimage. 2009;46:726–738. [DOI] [PubMed] [Google Scholar]
- 29. Rueckert D, Aljabar P, Heckemann RA, Hajnal JV, Hammers A. Diffeomorphic registration using B‐splines. Med Image Comput Comput Assist Interv. 2006;9:702–709. [DOI] [PubMed] [Google Scholar]
- 30. Kochunov P, Lancaster JL, Thompson P, Woods R, Mazziotta J, Hardies J, Fox P. Regional spatial normalization: toward an optimal target. J Comput Assist Tomogr. 2001;25:805–816. [DOI] [PubMed] [Google Scholar]
- 31. Fletcher E, Carmichael O, Decarli C. MRI non‐uniformity correction through interleaved bias estimation and B‐spline deformation with a template. Conf Proc IEEE Eng Med Biol Soc. 2012;2012:106–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Rajapakse JC, Giedd JN, DeCarli C, Snell JW, McLaughlin A, Vauss YC, Krain AL, Hamburger S, Rapoport JL. A technique for single‐channel MR brain tissue segmentation: application to a pediatric sample. Magn Reson Imaging. 1996;14:1053–1065. [DOI] [PubMed] [Google Scholar]
- 33. Fletcher E, Singh B, Harvey D, Carmichael O, Decarli C. Adaptive image segmentation for robust measurement of longitudinal brain tissue change. Conf Proc IEEE Eng Med Biol Soc. 2012;2012;5319–5322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. DeCarli C, Miller BL, Swan GE, Reed T, Wolf PA, Garner J, Jack L, Carmelli D. Predictors of brain morphology for the men of the NHLBI twin study. Stroke. 1999;30:529–536. [DOI] [PubMed] [Google Scholar]
- 35. Vercauteren T, Pennec X, Perchant A, Ayache N. Non‐parametric diffeomorphic image registration with the demons algorithm. Med Image Comput Comput Assist Interv. 2007;10:319–326. [DOI] [PubMed] [Google Scholar]
- 36. Boccardi M, Bocchetta M, Ganzola R, Robitaille N, Redolfi A, Duchesne S, Jack CR Jr, Frisoni GB; EADC‐ADNI Working Group on The Harmonized Protocol for Manual Hippocampal Segmentation and for the Alzheimer's Disease Neuroimaging Initiative . Operationalizing protocol differences for EADC‐ADNI manual hippocampal segmentation. Alzheimers Dement. 2015;11:184–194. [DOI] [PubMed] [Google Scholar]
- 37. Frisoni GB, Bocchetta M, Chetelat G, Rabinovici GD, de Leon MJ, Kaye J, Reiman EM, Scheltens P, Barkhof F, Black SE, et al. Imaging markers for Alzheimer disease: which vs how. Neurology. 2013;81:487–500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Boccardi M, Bocchetta M, Apostolova LG, Barnes J, Bartzokis G, Corbetta G, DeCarli C, deToledo‐Morrell L, Firbank M, Ganzola R, et al. Delphi definition of the EADC‐ADNI harmonized protocol for hippocampal segmentation on magnetic resonance. Alzheimers Dement. 2015;11:126–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Bocchetta M, Boccardi M, Ganzola R, Apostolova LG, Preboske G, Wolf D, Ferrari C, Pasqualetti P, Robitaille N, Duchesne S, et al. Harmonized benchmark labels of the hippocampus on magnetic resonance: the EADC‐ADNI project. Alzheimers Dement. 2015;11:151–160. [DOI] [PubMed] [Google Scholar]
- 40. Frisoni GB, Jack CR. HarP: the EADC‐ADNI harmonized protocol for manual hippocampal segmentation: a standard of reference from a global working group. Alzheimers Dement. 2015;11:107–110. [DOI] [PubMed] [Google Scholar]
- 41. Wang H, Suh JW, Das SR, Pluta J, Craige C, Yushkevich PA. Multi‐atlas segmentation with joint label fusion. IEEE Trans Pattern Anal Mach Intell. 2013;35:611–623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Wang H, Yushkevich PA. Dependency prior for multi‐atlas label fusion. Proc IEEE Int Symp Biomed Imaging. 2012;2012:892–895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Massaro JM, D'Agostino RB Sr, Sullivan LM, Beiser A, DeCarli C, Au R, Elias MF, Wolf PA. Managing and analysing data from a large‐scale study on Framingham Offspring relating brain structure to cognitive function. Stat Med. 2004;23:351–367. [DOI] [PubMed] [Google Scholar]
- 44. DeCarli C, Massaro J, Harvey D, Hald J, Tullberg M, Au R, Beiser A, D'Agostino R, Wolf PA. Measures of brain morphology and infarction in the Framingham Heart Study: establishing what is normal. Neurobiol Aging. 2005;26:491–510. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.