

Abstract
Background:
Medical specialties have evaluated malpractice claims in residents, but to the best of our knowledge, malpractice claims have not been evaluated in anesthesiology residents.
Methods:
The Westlaw legal database was queried for all malpractice litigation cases involving anesthesiology residents in the United States from January 1959 through December 2018. The cases were divided into 2 cohorts by year (before and after 1990) to account for the differences in patient safety features and monitoring available in the different time periods.
Results:
Ninety cases were included in the analysis. The median (interquartile range) for inflation adjusted payments was $1 140 544 (0 to 4 158 589). There was no association between the year the claim was filled and the payment amount, Spearman rho = −0.17, P = 0.15. In contrast, for claims that occurred in the intraoperative period, there was a moderate negative association between the year of the claim and the inflation adjusted payment, Spearman rho = −0.45, P = 0.003. Payments were greater if the event occurred in the postoperative period, median of $4 250 000 (959 000 to 55 595 000) compared to events that happened in the intraoperative period, median of $1 039 000 (0 to 3 802 000) and preoperative periods, median of $212 000 (0 to $3 982 000), P = 0.02.
Conclusions:
The reduction of liability across the years with malpractice claims that resulted from the intraoperative period suggest that the continued patient safety initiatives implemented by anesthesiology specialty has resulted in less liability to trainees and may stimulate future initiatives targeted to the postoperative period.
Keywords: Malpractice, anesthesiology, litigation, resident, fellow
Introduction
Malpractice claims have been identified as one of the causes for the rising costs of health care.1,2 It has been estimated that the annual costs related to malpractice claims is over 55 billion dollars in the United States alone.3 In addition, malpractice claims can have professional and emotional consequences to physicians.4 Physicians who undergo medical litigation claims may order unnecessary tests or procedures to avoid future claims. In more extreme circumstances, physicians abandon the practice of medicine because of high visibility of malpractice claims, emotional fear of litigation, or mental anguish from past malpractice suits.5
Many US physicians will be named in a malpractice claim during their career. The annual overall rate of paid malpractice claims among all specialties is 14.1 per 1000 physician-years.3 Surgical specialties (ie, neurosurgery, orthopedics, plastic surgery) account for the largest rates of malpractice claims, ranging from 30 to 53.1 per 1000 physicians-years with neurosurgery accounting for the highest paid claims (13%) of over one million dollars. In contrast, anesthesiologists experience an annual rate of paid malpractice claims of 11.7 per 1000 physicians-years with a similar percentage of paid malpractice claims (10%) reaching over one million dollars.
Malpractice claims can have even more profound consequences to medical trainees. Medical trainees are still molding their practice style while trying to build enough confidence to become independent practitioners.6,7 A malpractice claim can not only hinder the development of trainees by provoking anxiety, but it can also make them more prone to develop defensive medicine as a practice style.8 Other medical specialties (eg, surgery, internal medicine) have examined malpractice claims involving residents to better design strategies to reduce the impact of medical litigation on the trainees’ careers.9,10 The practice of anesthesiology deals with life and death circumstances on a daily basis with a significant potential for liability, yet, to the best of our knowledge, no prior study has examined malpractice claims involving anesthesiology residents.
The purpose of this study was to investigate malpractice claims involving anesthesiology residents and fellows using a large national law database. We hypothesized that inflation adjusted payments would decrease over time as shown in previous literature involving the US National Practitioner Data bank registrar.11,12 In addition, we also sought to identify factors associated with greater payments originated from anesthesiology trainees’ claims.
Materials and Methods
The Westlaw legal research database (Thomson Reuters Corporation, New York, New York) is a subscription-based online search engine containing court records of legal cases from both state (Supreme Court, Commonwealth Court, Superior Court, Court of Common Pleas) and federal courts (ie, Circuit Court of Appeals) from all 50 states. As one of the largest providers of US legal information it also includes separate databases (ie, individual state) and numerous secondary sources including descriptive opinions of lower court judges and law journal commentaries. Description of cases are nonuniform but contain the name of the case, the individuals involved, the date of the event, when the case was closed, the legal outcome, and a small summary of the relevant information pertaining to the case. Although the Westlaw database was created for legal professionals, it has been used by other medical specialties to examine malpractice claims involving residents.13,14 Access to Westlaw database was granted via Thomson Reuters (F.G.K., M.C.K., J.S.K.) and the study was deemed exempt by the Lifespan Institutional Review Board and patient consent was not required (registration No. 1441046).
The Westlaw legal database was queried for all malpractice litigation cases involving anesthesiologists in the United States from January 1959 through December 2018. The Boolean search method involving the terms “Resident trainee fellow/S Anesthesiolog! and malpractice” was used. All state and federal cases involving anesthesiology residents/fellows were included in the analysis. Jury verdicts, depositions, and narrative summaries were evaluated for trainee involvement either named as a participant or as a defendant, time period of alleged malpractice (preoperative, intraoperative, and postoperative) and type of anesthetic performed. Inclusion criteria included all malpractice cases that involved an anesthesiology resident or fellow. Exclusion criteria included cases that did not involve anesthesiology residents or lack of description of an anesthesiology resident.
Two investigators (F.G.K., M.C.K.) individually evaluated each case and extracted data from each individual trial using a predesignated collection form adapted from previous investigations.15,16 Disputes between investigators were finalized by discussion and if a resolution was not met, the final decision was determined by an additional investigator (G.S.D.O.). The variables extracted from the database included the following: surgical specialty, year and state of filing, gender of plaintiff, age of plaintiff, age of defendant, year of trainee, anesthesiology subspecialty, time of event (preoperative, intraoperative, postoperative), plaintiff outcome, reason for litigation (medical decision, lack of supervision by attending physician, lack of informed consent), verdict, and indemnity payment (amount the plaintiff was awarded during a settled case or a case with a plaintiff verdict).
The primary outcome for the study was indemnity payment adjusted by inflation (as of January 2019 using the Consumer Price Index). Secondary outcomes included patient outcome following alleged malpractice claim (eg, recovery or non–life-threatening, permanent injury, or death) and case verdict (eg, for the plaintiff, for the defendant, settlement, unknown). We divided the sample into 2 cohorts by year (before and after 1990) to account for the differences in patient safety features and monitoring available in the different time periods. The emphasis of incorporating anesthesiology patient safety measures such as pulse oximetry/capnography monitoring was considered potentially preventative in a majority of anesthetic-related closed malpractice claims occurring prior to 1990.17 Normally distributed continuous data were presented as means (SD) and analyzed using independent t tests. Nonnormally distributed continuous data was presented as median (interquartile range) and analyzed using the Mann-Whitney U test. Categorical data were presented as counts (n) and analyzed using the Fisher exact test. Spearman rho correlation coefficient was calculated to assess a relationship between mortality risk overestimation and decision conflict scores. Differences in indemnity payment amounts by various case characteristics were conducted using Wilcoxon-Mann-Whitney tests, given nonnormality of indemnity payment distributions. Statistical significance was defined as P < .05. Analyses was performed using Stata version 15 (College Station, Texas).
Results
A total of 2386 cases were identified, and an initial search yielded 288 legal cases relevant to this study. A total of 198 cases were further excluded after detailed examination because of lack of anesthesiology resident involvement, inaccurate or incomplete data, duplicate cases, or lawsuits not pertaining to medical malpractice (Figure 1). A total of 90 cases met the inclusion criteria and were included in the analysis. Claims occurred from January 1959 through December 2018. There were 20 cases that occurred in the time period prior to the advancement of patient safety measures (before 1990) and 70 cases that occurred after 1990. There were 45 cases that involved male patients, 41 that involved female patients, and 4 were unknown. The characteristics of malpractice claims among anesthesiology trainees are shown in Table 1. The median age of patients was 36 (9 to 48) years. All included malpractice claims resulted in a verdict, and no cases were dropped or dismissed with prejudice. The distribution of claims by geographic region in the United States is presented in Figure 2.
Figure 1.
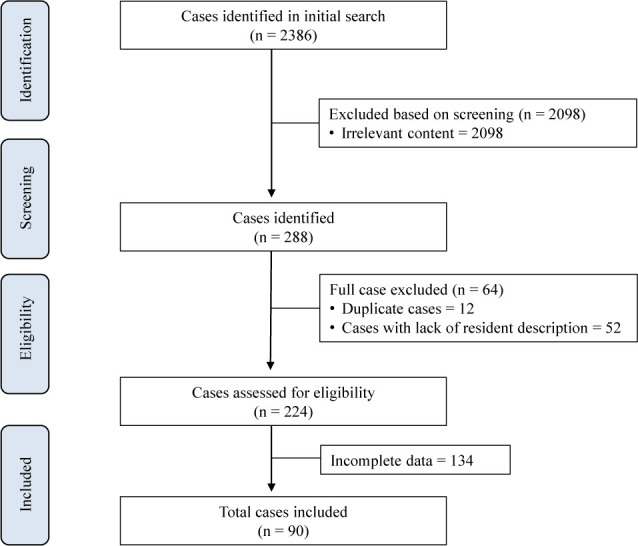
Flow chart of the selection of cases.
Table 1.
Characteristics of Malpractice Claims Involving Anesthesiology Trainees a
| Jan 1, 1959 to Dec 31, 1989 (n = 20) | Jan 1, 1990 to Dec 31 2018 (n = 70) | P Value | |
|---|---|---|---|
| Patient gender | .61 | ||
| Male | 9 (45) | 36 (51) | |
| Female | 11 (55) | 30 (43) | |
| Not reported | 0 | 4 (6) | |
| Patient age, y | 10 (6 to 35) | 39 (18 to 49) | .02 |
| Is the resident named as the defendant? | .34 | ||
| Yes | 12 (60) | 51 (73) | |
| No | 8 (40) | 17 (24) | |
| Unknown | 0 | 2 (3) | |
| Is a non-anesthesiology physician named as the defendant? | .64 | ||
| Yes | 8 (40) | 20 (28) | |
| No | 12 (60) | 48 (69) | |
| Unknown | 0 | 2 (3) | |
| Verdict | .26 | ||
| Plaintiff | 12 (60) | 32 (46) | |
| Defendant | 7 (35) | 20 (28) | |
| Settlement | 1 (5) | 9 (13) | |
| Not reported/in-progress | 0 | 9 (13) | |
| Anesthesia type | .91 | ||
| General | 14 (70) | 45 (64) | |
| Regional | 5 (25) | 16 (23) | |
| Sedation | 0 | 2 (3) | |
| Not reported | 1 (5) | 7 (10) | |
| Patient outcome | .52 | ||
| Recovery | 1 (5) | 5 (7) | |
| Permanent injury/disability | 13 (65) | 31 (44) | |
| Death/vegetative state | 6 (30) | 25 (36) | |
| Nonlife-threating | 0 | 3 (4) | |
| Not reported | 0 | 6 (9) | |
| Alleged injury location | .02 | ||
| Preoperative | 2 (10) | 15 (21) | |
| Intraoperative | 17 (85) | 36 (52) | |
| Postoperative | 1 (5) | 19 (27) | |
| Indemnity payment, $b | 2 167 207 (196 055 to 17 118 646) | 974 095 (0 to 4 091 638) | .16 |
| Trial outcome | .85 | ||
| Went to trial | 10 (50) | 30 (43) | |
| Settled | 6 (30) | 23 (33) | |
| Not reported | 4 (20) | 17 (24) |
a Data presented as n (%) or median (interquartile range).
b Adjusted for inflation as of January 2019 Consumer Price Index.
Figure 2.
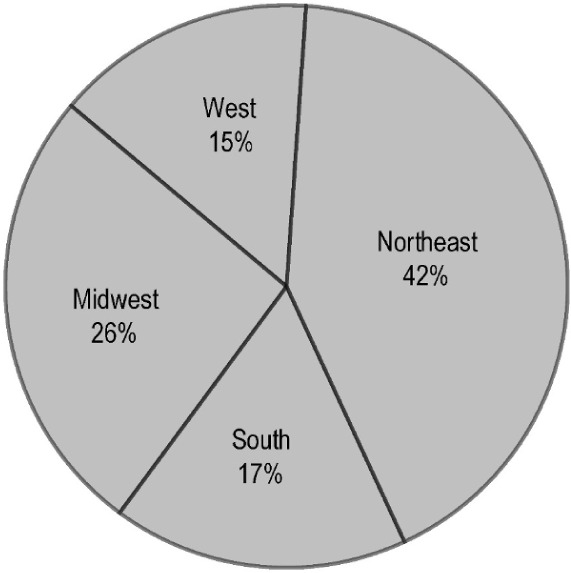
The occurrence of malpractice claims among anesthesia trainees by region in the United States.
In 44 out of 90 cases (49%), the cases were in favor of the plaintiff, 27 out of 90 (30%) were in favor of the defendant, 10 out 90 (11%) were settled, and the remaining 9 out 90 (10%) were unknown or remain open. The majority of claims involved first-year clinical anesthesia residents (CA-1; 34 out of 66, 73%) and occurred in the intraoperative period, 53 out of 90 (59%). Malpractice claims involving anesthesiology trainees during the perioperative period are presented in Table 2. The median for inflation adjusted payments was $1 140 544 ($0 to $4 158 589). Most claims, 75 out of 90 (83%), were because of patients who suffered death or permanent injury (malpractice harm). Malpractice harms involving anesthesiology trainees are presented in Table 3. The payments according to the perioperative period, type of anesthesia, and anesthesiology trainees are presented in Table 4. The median payments associated with verdicts in favor of the plaintiff was $3 673 000 ($1 111 000 to $14 071 000), while the median of payments resulted from settlements was $1 162 000 ($939 000 to $3 602 000), P = .14.
Table 2.
Malpractice Claims Involving Anesthesiology Trainees During the Perioperative Period
| Jan 1, 1959 to Dec 31, 1989 (n = 20) | Jan 1, 1990 to Dec 31, 2018 (n = 70) | |
|---|---|---|
| Preoperative (n = 17) | Peripheral nerve block (1) Neuraxial nerve block (1) | Neuraxial nerve block (6) Peripheral nerve block (3) Consent issue (2) Invasive procedures (2) Unknown (2) |
| Intraoperative (n = 53) | Intubation (5) Invasive procedures (1) Positioning (1) Induction (2) Neuraxial nerve block (1) Monitoring (1) Fluid management (1) Extubation (1) Unknown (4) | Intubation (9) Neuraxial nerve block (4) Positioning (4) Fluid management (5) Induction (3) Invasive procedures (4) Fire (1) Peripheral nerve block (1) Surgical error (4) Unknown (1) |
| Postoperative (n = 20) | Surgical complication (1) | Invasive procedures (2) Neuraxial nerve block (4) Intubation (7) Monitoring (2) Communication (1) Unknown (3) |
Table 3.
Malpractice Harms a Involving Anesthesiology Trainees
| Permanent Injury/Disability (n = 44) | Death/Vegetative State (n = 31) | |
|---|---|---|
| Jan 1, 1959 to Dec 31, 1989 | Nerve injury (3) Anoxic brain injury (10) | Hypoxia (4) Renal failure (1) Unknown (1) |
| Jan 1, 1990 to Dec 31, 2018 | Nerve injury (10) Anoxic brain injury (17) Complications due to retained procedural instrument (1) Ocular injury (1) Psychiatric disorder (1) Unknown (1) | Hypoxia (15) Arrhythmia (2) Seizure (3) Hypovolemic shock (1) Unknown (4) |
a Malpractice harms refers to malpractice cases that result in death or permanent disability as a result of medical treatment or management.
Table 4.
Malpractice Claims Showing Indemnity Payments According to Perioperative Period
| Indemnity Payments, median (interquartile range), $ | P Value | |
|---|---|---|
| Anesthesia type | .16 | |
| General | 1 943 000 (53 000 to 8 900 000) | |
| Regional | 959 000 (0 to 3 802 000) | |
| Alleged injury location | .02 | |
| Preoperative | 212 000 (0 to 3 982 000) | |
| Intraoperative | 1 039 000 (0 to 3 802 000) | |
| Postoperative | 4 250 000 (959 000 to 55 595 000) | |
| Training year | .33 | |
| CA-1/CA-2 | 1 595 000 (0 to 8 890 000) | |
| CA-3/Fellow | 1 140 000 (0 to 3 682 000) |
Abbreviation: CA, clinical anesthesia resident (first-year, second-year, third-year).
There was no association between the year that the claim was filed and the payment amount, Spearman rho = −0.17, P = .15. For claims that occurred in the intraoperative period, there was a moderate negative association between the year of the claim and the inflation adjusted payment, Spearman rho = −0.45, P = .003. Payments did not differ if surgical cases were performed under general anesthesia, median of $1 943 000 ($53 000 to $8 900 000) compared to regional anesthesia, median of $959 000 ($0 to $3 802 000), P = .16. In addition, payments did not differ if residents were at the early stage of their training (CA-1/CA-2), median of $1 595 000 ($0 to $8 890 000) compared to later stages of training (CA-3/Fellow), median of $1 140 000 ($0 to $3 682 000), P = .33.
The largest payments to claims were encountered in pediatrics, median of $10 658 000 ($2 314 000 to $37 936 000). Payments provided to younger patients (<18 years old) were greater, median of $8 763 00 ($297 000 to $38 528 000) compared to older patients (≥18 years old), median of $959 000 ($0 to $3 664 000), P = .01. In addition, payments were greater if the event happened in the postoperative period, median of $4 250 000 ($959 000 to $55 595 000) compared to events that happened in the intraoperative period, median of $1 039 000 ($0 to $3 802 000), and preoperative periods, median of $212 000 ($0 to $3 982 000), P = .02.
Discussion
The most important finding of this study was the identification of events at the postoperative period as the highest risk for larger payments involving anesthesiology residents. Although most claims occurred in the intraoperative period, larger payments were rendered in claims that occurred in the postoperative period. In addition, we also identified pediatric patients as the highest risk population for larger payments. Our current results suggest that residency program efforts to reduce liability associated with residents should target safety efforts in the postoperative period and in the care of pediatric patients.18
Our results are clinically important since prior studies examining liability resulted from anesthesiology claims of nontrainees have frequently identified the intraoperative period and obstetric patients as high-risk populations.19–21 The Accreditation Council for Graduate Medical Education 2:1 supervision rule during the intraoperative period may reduce the attribution of severe unexpected outcomes to anesthesiology trainees.22 Procedures that are commonly performed in the operating room under direct supervision (eg, central lines, intubations) may be done outside the operating room under indirect supervision, and this may result in malpractice claims in which physician trainees were directly involved in the harm events.23
Another important finding of our investigation was the lack of correlation between inflation-adjusted payments and year the claim was filed. In contrast, inflation-adjusted payments that occurred in the intraoperative period were inversely associated with the year of the claim. The occurrence of malpractice claims decreased in the intraoperative period after 1990 compared to prior years. However, we observed an increase in malpractice claims in the postoperative period, suggesting the postoperative period is a potential target for further safety improvements for anesthesiology training programs.
Since the late 1980s and early 1990s, the advancements to improve patient safety in the practice of anesthesiology have been remarkable. The incorporation of real-time continuous monitoring of oxygen delivery and patient ventilation, anesthesia machine checkout protocol, pharmacological improvements in anesthesia medications, and use of realistic patient simulators are a few of the major safety developments.24 The emphasis to develop advancements in medical equipment technology, improving communication among team members, adhering to national guidelines and engaging in continuing medical education continue to improve the safety and quality in not only anesthesia management but also in perioperative care.
It was also interesting to note that claims for pediatric patients carried a greater risk for higher inflation-adjustment payments. This finding is similar to other specialties such as pediatric neurosurgery and is not surprising as a substantial proportion of claims that resulted in payments were because of death or permanent disability and pediatric patients would carry a greater loss of productive years.16 In addition, the cost for caring for a disabled pediatric patient is often greater because of the larger number of years.16
Other medical specialties have also used the Westlaw database to evaluate malpractice claims on residents and nontrainees. Thiels et al13 recently evaluated 87 claims related to general surgery residents (median payment $900 000) and, similar to our findings, they identified junior residents as needing quality supervision during training. Svider et al15 examined claims involving oculoplastic claims (average payment $455 703), and the authors identified the informed consent process as an improvement target. Thomas et al16 investigated malpractice claims in nontrainees involving neurosurgery (median payment $2 550 000) and reported that procedural error accounted for 45% of litigation cases.
The current study can only be interpreted within the context of its limitations. First, the Westlaw database is not a complete record of lawsuits. Despite being commonly used in research of medical malpractice by medical and law researchers, the medical data records in the database can be incomplete and the details are ambiguous. Second, claims settled prior to the initiation of a lawsuit are not entered into the database. Therefore, the claims examined in this study likely represent a small but unknown proportion of all claims filed nationally. Third, we choose the 2 cohorts by year to account for the differences in patient safety features and monitoring that began to become more routine care throughout the 1990s. Nonetheless, the development and implementation of anesthesiology patient safety measures have existed for a long time before modern advances in the quality of care and patient safety. Last, the medical malpractice payments are limited because of tort reform and state-based efforts to cap malpractice liability. Over half of the states (US) have passed legislation that has placed a limit on the compensation a plaintiff can be awarded following a successful lawsuit.
In summary, we found that early-stage anesthesiology trainees (CA-1/CA-2) and pediatric cases are potential improvement targets for anesthesiology training programs to reduce liability from malpractice claims. In addition to the technological advances in medical monitoring, the continued supervision in the early stages of anesthesiology training are warranted to provide improved patient outcomes. Moreover, advances in improving patient safety implemented by the anesthesiology specialty have resulted in less liability and may stimulate future initiatives targeted to the postoperative period.
Footnotes
Conflict of Interest: None.
Disclosures: None.
References
- 1.Myers LC, Skillings J, Heard L, et al. Medical malpractice involving pulmonary/critical care physicians. Chest. 2019;156(5):907–14. doi: 10.1016/j.chest.2019.04.102. [DOI] [PubMed] [Google Scholar]
- 2.Cardin JL, Johanet H. Malpractice claims and abdominal wall hernia repair. J Visc Surg. 2019;156(suppl 1):S57–S60. doi: 10.1016/j.jviscsurg.2019.03.005. [DOI] [PubMed] [Google Scholar]
- 3.Schaffer AC, Jena AB, Seabury SA, et al. Rates and characteristics of paid malpractice claims among US physicians by specialty, 1992–2014. JAMA Intern Med. 2017;177(5):710–8. doi: 10.1001/jamainternmed.2017.0311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gómez-Durán EL, Vizcaíno-Rakosnik M, Martin-Fumadó C, et al. Physicians as second victims after a malpractice claim: an important issue in need of attention. J Healthc Qual Res. 2018;33(5):284–9. doi: 10.1016/j.jhqr.2018.06.002. [DOI] [PubMed] [Google Scholar]
- 5.Durrance CP, Hankins S. Medical malpractice liability exposure and OB/GYN physician delivery decisions. Health Serv Res. 2018;53(4):2633–50. doi: 10.1111/1475-6773.12813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Heitkamp DE, Ford JM, Madden CM, et al. Transitioning to independent practice: a successful fourth-year radiology resident curriculum. J Am Coll Radiol. 2017;14(12):1603–6. doi: 10.1016/j.jacr.2017.06.010. [DOI] [PubMed] [Google Scholar]
- 7.Daly Guris RJ, Duarte SS, Miller CR, et al. Training novice anaesthesiology trainees to speak up for patient safety. Br J Anaesth. 2019;122(6):767–75. doi: 10.1016/j.bja.2019.01.017. [DOI] [PubMed] [Google Scholar]
- 8.Houry D, Shockley LW. Evaluation of a residency program’s experience with a one-week emergency medicine resident rotation at a medical liability insurance company. Acad Emerg Med. 2001;8(7):765–7. doi: 10.1111/j.1553-2712.2001.tb00203.x. [DOI] [PubMed] [Google Scholar]
- 9.Gurley KL, Grossman SA, Janes M, et al. Comparison of emergency medicine malpractice cases involving residents to nonresident cases. Acad Emerg Med. 2018;25(9):980–6. doi: 10.1111/acem.13430. [DOI] [PubMed] [Google Scholar]
- 10.Berlin L. Medicolegal-malpractice and ethical issues in radiology: malpractice vulnerability of radiology residents and fellows. AJR Am J Roentgenol. 2013;201(2):W358. doi: 10.2214/AJR.13.10757. [DOI] [PubMed] [Google Scholar]
- 11.Kain ZN. The National Practitioner Data Bank and anesthesia malpractice payments. Anesth Analg. 2006;103(3):646–9. doi: 10.1213/01.ane.0000226218.55224.53. [DOI] [PubMed] [Google Scholar]
- 12.Reich J, Schatzberg A. Empirical comparisons of malpractice claims of different medical specialties. J Public Health Aspects. 2015;2:2. [Google Scholar]
- 13.Thiels CA, Choudhry AJ, Ray-Zack MD, et al. Medical malpractice lawsuits involving surgical residents. JAMA Surg. 2018;153(1):8–13. doi: 10.1001/jamasurg.2017.2979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wegman B, Stannard JP, Bal BS. Medical liability of the physician in training. Clin Orthop Relat Res. 2012;470(5):1379–85. doi: 10.1007/s11999-012-2244-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Svider PF, Blake DM, Husain Q, Mauro AC. In the eyes of the law: malpractice litigation in oculoplastic surgery. Ophthalmic Plast Reconstr Surg. 2014;30(2):119–23. doi: 10.1097/IOP.0000000000000025. [DOI] [PubMed] [Google Scholar]
- 16.Thomas T, Gupta R, Griessenauer CJ et al. Medical malpractice in neurosurgery: a comprehensive analysis. World Neurosurg. 2018110:e552–e559. doi: 10.1016/j.wneu.2017.11.051. [DOI] [PubMed] [Google Scholar]
- 17.Tinker JH, Dull DL, Caplan RA, et al. Role of monitoring devices in prevention of anesthetic mishaps: a closed claims analysis. Anesthesiology. 1989;71(4):541–6. doi: 10.1097/00000542-198910000-00010. [DOI] [PubMed] [Google Scholar]
- 18.Hesse S, Kreuzer M, Hight D, et al. Association of electroencephalogram trajectories during emergence from anaesthesia with delirium in the post-anaesthesia care unit: an early sign of postoperative complications. Br J Anaesth. 2019;122(5):622–34. doi: 10.1016/j.bja.2018.09.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ranum D, Ma H, Shapiro FE, et al. Analysis of patient injury based on anesthesiology closed claims data from a major malpractice insurer. J Healthc Risk Manag. 2014;34(2):31–42. doi: 10.1002/jhrm.21156. [DOI] [PubMed] [Google Scholar]
- 20.Staender S, Schaer H, Clergue F, et al. A Swiss anaesthesiology closed claims analysis: report of events in the years 1987–2008. Eur J Anaesthesiol. 2011;28(2):85–91. doi: 10.1097/EJA.0b013e3283414fea. [DOI] [PubMed] [Google Scholar]
- 21.Mihai R, Scott S, Cook TM. Litigation related to inadequate anaesthesia: an analysis of claims against the NHS in England 1995–2007. Anaesthesia. 2009;64(7):829–35. doi: 10.1111/j.1365-2044.2009.05912.x. [DOI] [PubMed] [Google Scholar]
- 22.De Oliveira GS, Jr, Rahmani R, Fitzgerald PC, et al. The association between frequency of self-reported medical errors and anesthesia trainee supervision: a survey of United States anesthesiology residents-in-training. Anesth Analg. 2013;116(4):892–7. doi: 10.1213/ANE.0b013e318277dd65. [DOI] [PubMed] [Google Scholar]
- 23.Myers LC, Gartland RM, Skillings J, et al. An examination of medical malpractice claims involving physician trainees. Acad Med. 2020;95(8):1215–22. doi: 10.1097/ACM.0000000000003117. [DOI] [PubMed] [Google Scholar]
- 24.Lagasse RS. Anesthesia safety: model or myth: A review of the published literature and analysis of current original data. Anesthesiology. 2002;97(6):1609–17. doi: 10.1097/00000542-200212000-00038. [DOI] [PubMed] [Google Scholar]