

Abstract
Contrast‐enhanced computed tomography angiography reveals “railroad track‐like” calcifications bilaterally from the femoral to the popliteal arteries.

A 67‐year‐old woman, who was a nonsmoker, presented with left neck discomfort during swallowing for three years. She had intermittent claudication for approximately 30 years but had not developed any exacerbations. Other medical conditions included rheumatoid arthritis, which was controlled using 14 mg of weekly methotrexate and 50 mg of daily iguratimod for three years and hypertension, which was controlled using azelnidipine. Physical examination revealed no bilateral cervical masses or carotid bruit. The bilateral femoral artery was palpable; however, the bilateral popliteal and dorsal pedis arteries were not. Laboratory tests showed 21 mg/dL of urea nitrogen, 0.78 mg/dL of creatinine, 94 mg/dL of serum glucose, 4.2 g/dL of albumin, 9.1 mg/dL of calcium, 3.7 mg/dL of phosphate, 36 pg/mL of intact parathyroid hormone (reference range 10‐65), and 0.36 mg/dL of C‐reactive protein. The ankle‐brachial pressure index was 0.57 bilaterally. Contrast‐enhanced computed tomography angiography showed “railroad track–like” calcifications bilaterally from the femoral to the popliteal arteries (Figure 1). Coarse calcification was seen anterior to the left common carotid artery owing to aggregation of small artery calcifications (Figure 2); however, there was no remarkable aortic calcification. Based on these clinical features, she was diagnosed with Mönckeberg's sclerosis. She was prescribed 200 mg of cilostazol per day. Her symptoms have not exacerbated for two years.
FIGURE 1.

Contrast‐enhanced computed tomography angiography reveals “railroad track–like” calcifications bilaterally from the femoral to the popliteal arteries
FIGURE 2.
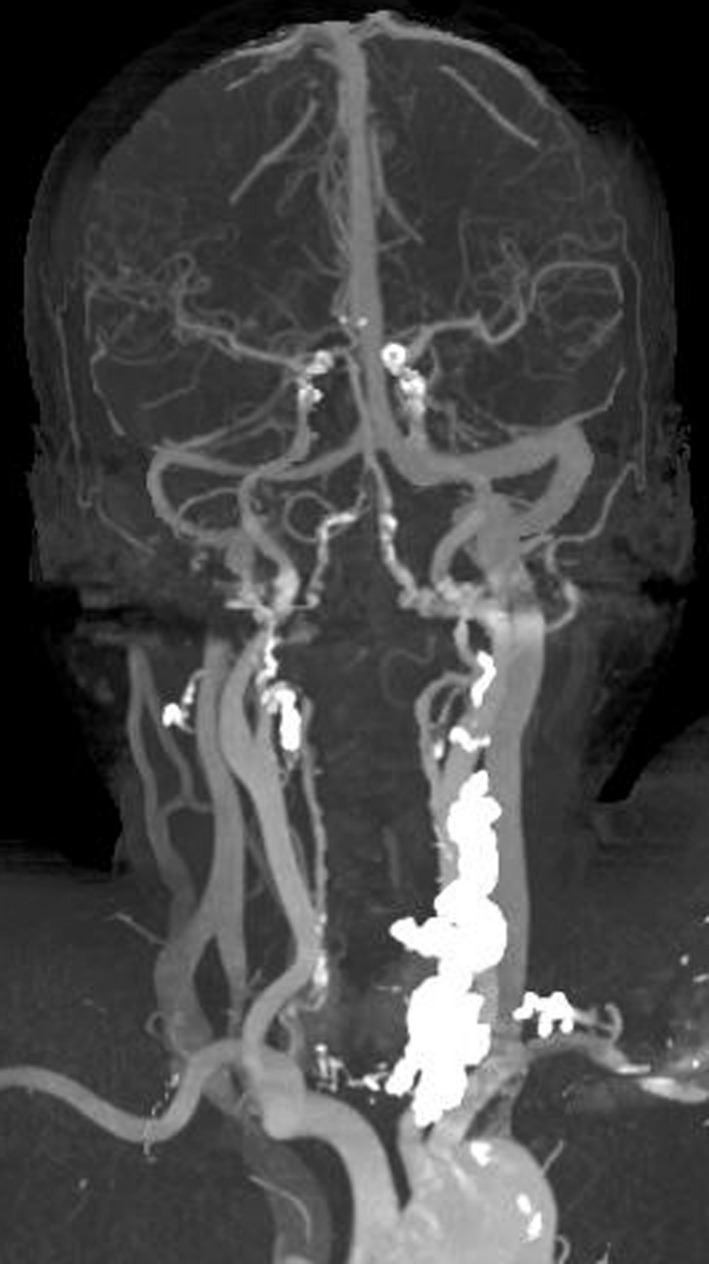
Coarse calcification is seen anterior to the left common carotid artery owing to aggregation of small artery calcification
Mönckeberg's sclerosis, first described in 1903, is a vascular lesion characterized by calcification of the media of the muscular arteries. This lesion is sometimes seen in patients with diabetes mellitus and chronic kidney disease, 1 , 2 but it can also present in young individuals with no underlying disease. 3 The mechanism of vascular calcification is unclear. Patients with this condition are usually considered to be asymptomatic because luminal stenosis is less likely to occur, unlike atherosclerosis. However, it has also been reported that approximately 70% of the leg artery lesions in patients with clinically diagnosed peripheral arterial disease is characterized by calcification of the media rather than by atherosclerosis. 4 . If clinicians suspect peripheral arterial disease in a patient with few risk factors for atherosclerosis, they should consider performing imaging studies to identify the systemic arterial and soft tissue calcifications.
CONFLICT OF INTEREST
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
CONSENT
Written informed consent was obtained from the patient for publication of this clinical image.
ACKNOWLEDGEMENTS
All authors have not received a specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors.
Yamamoto Y, Ishikawa Y, Shimpo M, Matsumura M. Mönckeberg’s sclerosis. J Gen Fam Med 2021;22:55–56. 10.1002/jgf2.380
REFERENCES
- 1. Smith CD, Bilmen JG, Iqbal S, Robey S, Pereira M. Medial artery calcification as an indicator of diabetic peripheral vascular disease. Foot Ankle Int. 2008;29(2):185–90. [DOI] [PubMed] [Google Scholar]
- 2. Abou‐Hassan N, Tantisattamo E, D’Orsi ET, O’Neill WC. The clinical significance of medial arterial calcification in end‐stage renal disease in women. Kidney Int. 2015;87:195–9. [DOI] [PubMed] [Google Scholar]
- 3. Mowafy KA, Soliman M, Hammoda AM, Soliman RM. Bilateral lower limb disabling claudication in a young man: a case of Mönckeberg’s arteriosclerosis. Vasc Endovasc Review. 2019;2(1):48–52. [Google Scholar]
- 4. O’Neill WC, Han KH, Schneider TM, Hennigar RA. Prevalence of nonatheromatous lesions in peripheral arterial disease. Arterioscler Thromb Vasc Biol. 2015;35(2):439–47. [DOI] [PubMed] [Google Scholar]