

Abstract
A 72‐year‐old woman presented with a 1‐day history of acute throat pain, hoarseness. On cervical ultrasonography (transverse view), the epiglottis was swollen with anterior‐posterior diameter of 3.5 and 3.8 mm at right and left edges, respectively. Laryngeal endoscopy showed marked swelling of the epiglottis, and acute epiglottitis was diagnosed.

Keywords: acute epiglottitis, point‐of‐care ultrasound, throat pain
A 72‐year‐old woman visited the emergency department of our hospital with a 1‐day history of acute throat pain, hoarseness, and pain on swallowing. She did not complain of chills. On examination, her body temperature was 38.2°C, respiratory rate was 20 breaths per minute, and oxygen saturation on room air was 95%. Stridor was not heard on auscultation. On cervical ultrasonography (transverse view), the epiglottis was swollen with anterior‐posterior diameter of 3.5 and 3.8 mm at right and left edges, respectively (Figure 1A). Subsequent laryngeal endoscopy by an otorhinolaryngologist showed marked swelling of the epiglottis (Figure 1B), and acute epiglottitis was diagnosed. The patient was admitted to the hospital, and intravenous ceftriaxone was initiated at 2 g/24 hr. Her hoarseness and pain on swallowing gradually decreased and completely resolved after 1 week, when repeat evaluation of the epiglottis showed a 2.2‐mm anterior‐posterior diameter on ultrasonography (Figure 2A) and normal appearance on laryngeal endoscopy (Figure 2B). Subsequently, she was discharged without any complications.
Figure 1.
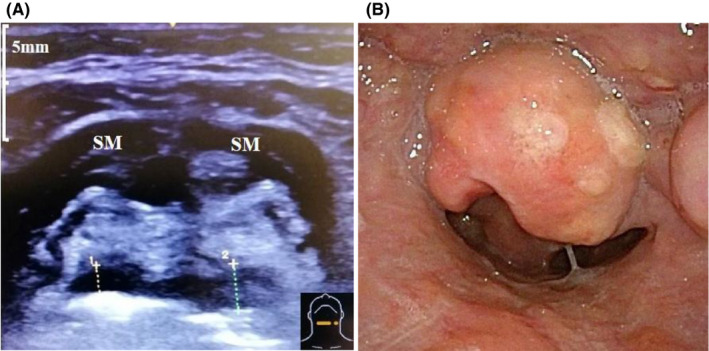
Ultrasound is at the level just below the hyoid bone. Ultrasound image at hospital admission showed that the epiglottis is swollen, with anterior‐posterior diameters of 3.5 mm and 3.8 mm at the left and right edges, respectively (A), and laryngeal endoscopy of the swollen epiglottis (B)
Figure 2.
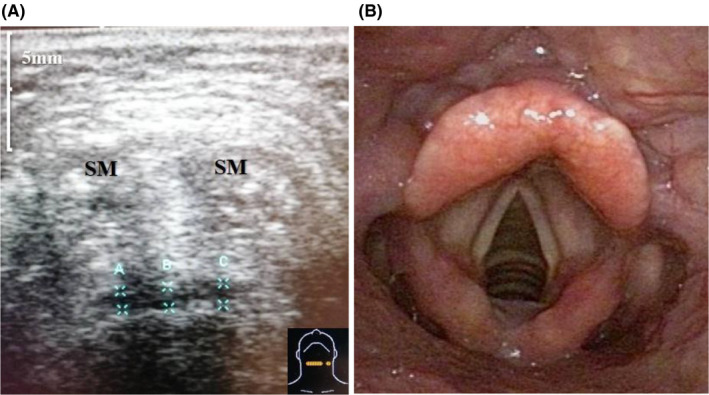
Ultrasonography 1 wk after treatment with intravenous ceftriaxone showed alleviation of the swelling of the epiglottis, with an anterior‐posterior diameter of 2.2 mm (A). Laryngeal endoscopy also shows the resolution of the epiglottic swelling (B)
Acute epiglottitis consists primarily of inflammatory swelling of the epiglottis, associated with an infection. Although vaccination for Haemophilus influenzae type B has reduced the prevalence of acute epiglottitis in infants, reports in adults have been increasing. 1 Delayed treatment can lead to asphyxiation; therefore, prompt diagnosis is extremely important.
The principal symptoms of acute epiglottitis are high fever, severe sore throat, and odynophagia; thus, at an early stage, acute epiglottitis is difficult to distinguish from the common cold. Differentiating acute epiglottitis from other conditions that also present similarly, such as peritonsillar and retropharyngeal abscesses, is essential.
Laryngeal endoscopy is necessary for clinical examination of the epiglottis, which often requires the expertise of an otorhinolaryngologist. Several reports have described that computed tomography, with the radiologic thumb and vallecula signs found in lateral cervical radiography, has high sensitivity and specificity for the diagnosis of acute epiglottitis. 1 , 2 However, it is often not possible to perform radiography and computed tomography without delay at the point‐of‐care in clinical practice.
Ultrasonography is superior to CT because it is available in the clinical setting, free from radiation exposure, inexpensive, and it can be rapidly performed. Ultrasonography is superior to endoscopes because it is less invasive.
Furthermore, ultrasound can diagnose and facilitate the exclusion of other diseases, such as peritonsillar abscess, more quickly than CT and endoscopy in a noninvasive manner, and it is useful for observing the therapeutic effect of epiglottitis by repeating during treatment of the patient.
The following two points are important for diagnosing epiglottitis with ultrasound.
Using a 5‐ to 10‐MHz linear array transducer, in a transverse view of the neck region at the level just below the hyoid bone, the epiglottis is seen as a hypoechoic curvilinear structure. The thickness of the epiglottis should be measured in this view. The average normal range is 2.5 ± 0.15 mm. 3 If the anterior‐posterior diameters at the right and left edges are greater than 3.6 mm, this finding strongly indicates epiglottitis. 4
In the midsagittal view, with a 3.5‐Hz curved transducer, the hyoid bone and swollen epiglottis form a P‐shape. 5
Ultrasonography was thus useful for the prompt diagnosis of acute epiglottitis and monitoring treatment outcomes. This rapid diagnosis enabled the early initiation of medical therapy and avoided the need for intubation and mechanical ventilation.
If the anterior‐posterior diameter of the epiglottis is measured by cervical ultrasonography, and epiglottitis is suspected, the patient can be promptly referred to a otorhinolaryngologist for early diagnosis and treatment.
CONFLICT OF INTEREST
The authors declare no conflict of interests for this article.
INFORMED CONSENT
We have obtained the consent of the patient for publication.
Acknowledgements
The authors would like to thank ENAGO (https://www.enago.jp/) for the English language review.
REFERENCES
- 1. April MD, Donaldson C, Tannenbaum LI, et al Emergency department septic shock patient mortality with refractory hypotension vs hyperlactatemia: a retrospective cohort study. Am J Emerg Med. 2017;35(10):1474–79. [DOI] [PubMed] [Google Scholar]
- 2. Kim KH, Kim YH, Lee JH, et al Accuracy of objective parameters in acute epiglottitis diagnosis: a case‐control study. Medicine (Baltimore). 2018;97(37):e12256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Werner SL, Jones RA, Emerman CL. Sonographic assessment of the epiglottis. Acad Emerg Med. 2004;11(12):1358–1360. [DOI] [PubMed] [Google Scholar]
- 4. Ko DR, Chung YE, Park I, et al Use of bedside sonography for diagnosing acute epiglottitis in the emergency department: a preliminary study. J Ultrasound Med. 2012;31(1):19–22. [DOI] [PubMed] [Google Scholar]
- 5. Hung TY, Li S, Chen PS, et al Bedside ultrasonography as a safe and effective tool to diagnose acute epiglottitis. Am J Emerg Med. 2011;29(3):359.e1–359.e3. [DOI] [PubMed] [Google Scholar]