

Abstract
Objectives
To identify and synthesise available evidence on the impact of transitional care interventions with both predischarge and postdischarge elements on readmission rates in older medical patients.
Design
A systematic review.
Method
Inclusion criteria were: medical patients ≥65 years or mean age in study population of ≥75 years; interventions were transitional care interventions between hospital and home with both predischarge and postdischarge components; outcome was hospital readmissions. Studies were excluded if they: included other patient groups than medical patients, included patients with only one diagnosis or patients with only psychiatric disorders. PubMed, The Cochrane Library, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Web of Science were searched from January 2008 to August 2019. Study selection at title level was undertaken by one author; the remaining selection process, data extraction and methodological quality assessment were undertaken by two authors independently. A narrative synthesis was performed, and effect sizes were estimated.
Result
We identified 1951 records and included 11 studies: five randomised trials, four non-randomised controlled trials and two pre–post cohort studies. The 11 studies represent 15 different interventions and 29 outcome results measuring readmission rates within 7–182 days after discharge. Twenty-two of the 29 outcome results showed a drop in readmission rates in the intervention groups compared with the control groups. The most significant impact was seen when interventions were of high intensity, lasted at least 1 month and targeted patients at risk. The methodological quality of the included studies was generally poor.
Conclusion
Transitional care interventions reduce readmission rates among older medical patients although the impact varies at different times of outcome assessment. High-quality studies examining the impact of interventions are needed, preferably complimented by a process evaluation to refine and improve future interventions.
PROSPERO registration number
CRD42019121795.
Keywords: geriatric medicine, preventive medicine, internal medicine
Strengths and limitations of this study.
Focus on discharge interventions where intervention elements are provided both at the hospital and at home.
High internal validity as Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline has been applied.
Results may under-represent negative study findings as negative impacts often remain unpublished.
Unplanned readmissions were the only outcome assessed in this review.
Introduction
Transitional care interventions (TCIs) may be essential in older medical patients’ transition from hospital to home as they may prevent adverse events and unplanned hospital readmissions. These events can have detrimental consequences for the individual patient.
The global demography is radically changing. In the European Union, elderly above 65 years are estimated to account for 29.1% of the total population in 2080 compared with 19.2% in 2016. Additionally, the fraction of the population above 80 years is expected to double between 2016 and 2080.1 We may therefore expect a dramatic increase in healthcare service demands and costs.2 As these changes will bring substantial challenges to healthcare systems,3 4 the potential need for TCIs will also increase. Older people needing healthcare are often medical patients with several concurrent diseases, reduced physical or mental functionalities, limited ability to provide self-care and they are often living alone and need care from primary or secondary healthcare services.5
Older people with complex comorbid conditions are at high risk of adverse events and safety incidents immediately after their discharge from hospital.6
Unplanned readmission seems to be related to insufficient discharge planning, and unintended events during discharge and transition such as medication errors and inadequate communication between hospital and primary care professionals.7–10 By contrast, optimised, customised and patient-centred discharge planning and transitions may reduce length of hospital stay, risk of readmission, medication discrepancies and mortality; and may as well improve the patients’ activity of daily living and reduce healthcare costs.11
One approach to addressing these challenges is to examine the impact of interventions aimed at reducing readmissions.
Previous systematic reviews have mainly evaluated the impact of hospital-based and/or home-based interventions on readmissions12 13 and included populations with specific conditions or both medical and surgical patients. To our knowledge, no systematic review has been conducted examining the impact of TCIs that take place in both hospital and home on older medical patients’ readmission rates based on recent data.
The purpose of this systematic review is to evaluate the impact of TCIs with both predischarge and postdischarge elements on readmission among older medical patients.
Methods
This review was registered in the PROSPERO database prior to data collection (CRD42019121795).14 It is presented in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).15
Eligibility criteria
We identified studies that aimed to reduce readmission rates through TCIs among older medical patients. The PICO process for framing the research question was applied16 and defined as:
Population: older medical patients discharged from a general medical ward or emergency department (ED).
Intervention: in the transitional phase between hospital and home which examined the impact of the intervention on readmission rates. The interventions had to include both predischarge and postdischarge components.
Comparison: usual care defined as standard care and treatment.
Outcome: unplanned readmission to hospital.
Selecting tool is displayed in online supplemental 1.
bmjopen-2020-040057supp001.pdf (475.8KB, pdf)
Studies were excluded if:
The population was aged under 65 years or the mean age was below 75 years.
They included other patient groups than medical patients (eg, surgical patients).
They included participants with only one medical diagnosis (International Classification of Disease-10th edition).
Studies included participants with psychiatric disorders only.
They compared interventions with anything other than usual care.
Readmission was not an outcome.
Intervention only included either predischarge or postdischarge components; they were reviews, case reports or case studies without comparison groups.
Information sources
To identify eligible studies, we searched the following bibliographic databases: PubMed, The Cochrane Library, Embase, CINAHL and Web of Science from January 2008 to August 2019. An extensive snowball search was performed where the reference lists from relevant studies, systematic reviews and included studies were examined. Additionally, publication lists from prominent researchers within the field were examined. Grey literature was searched in all relevant resources listed by Paez17 from January 2008 to August 2019. Authors from relevant study protocols and grey literature were contacted in order to examine whether the studies were published or study results were available. The Negative Results Scientific Journal was searched.
Search strategy
The search string (online supplemental 2) was developed in collaboration between the authors and a university research librarian. We used key terms, free text-words, subject headings, index terms and appertaining synonyms, which were identified through relevant theory and research. The searches were limited by only including studies published in English or Scandinavian languages. The bibliographic searches were conducted on 13 and 14 December 2018 and the searches were regularly updated until 31 August 2019.
Study selection
First, titles were screened for their potential relevance according to population and outcome by the first author (LFR). Second, two authors independently screened titles and abstracts for intervention eligibility (LFR and MG). Third, an assessment of the full text was performed by two authors independently (always including LFR). In case of disagreement, a third author, who was chosen a priori, was consulted.
Data extraction
The Cochrane Data Extraction Form was modified to fit the present patient group and intervention type.18 Data from the included studies were extracted by two researchers independently (always including LFR). Extracted data included study characteristics and results such as author, year of publication, country, study design, setting, participants, study size, outcomes, follow-up time and impact of intervention in numbers and/or per cent. Only data on the outcome ‘readmission’ were extracted and analysed.
Quality assessment
‘The Quality Assessment Tool for Quantitative Studies’ (EPHPP) (online supplemental 3) was applied to assess bias in each study included in the review. The validated tool is recommended by The Cochrane Collaboration16 19 and provides a standardised means to assess study quality. The Effective Public Healthcare Panacea Project (EPHPP) assesses six methodological dimensions: selection bias, study design, confounders, blinding, data collection as well as withdrawals and dropouts. It distributes the overall methodological rating into a strong, moderate or weak measure of internal validity.20 Quality assessment will be conducted at study level. All studies meeting the inclusion criteria are included in the synthesis regardless of the results of the quality assessments. Quality assessment across studies will be analysed and the impact hereof will be discussed.
Data synthesis
Inspired by Pigott and Shepperd,21 the following aspects that can entail heterogeneity will be assessed: (1) context, (2) target population, (3) intervention, (4) methodological features and (5) researcher characteristics and reporting context. This assessment will result in a descriptive synthesis or a meta-analysis of data. Risk estimates (RR) and their 95% CIs are calculated (section 6.4.1 in Ref. 16) when possible and presented in forest plots stratified by subgroups. Only main results will be presented and discussed according to subgroups based on study—and intervention characteristics and review findings. The certainty of the synthesised results will be assessed using Grading of Recommendations Assessment, Development and Evaluation (GRADE) (section 14-2-1 in Ref. 16).
Patient and public involvement
Patients or the public were not involved in this study.
Results
Study selection
In total, 1951 records were identified. Of those, 1901 records were identified through bibliographic databases and 50 records were found through other sources. After removing duplicates, 1521 records were screened by title and abstract. Seventy-four records were considered for full-text review of which 11 met the eligibility criteria (figure 1). The 63 remaining records were excluded due to participants’ age, population, study design, readmission not listed as an outcome, only predischarge or postdischarge elements in the intervention, not able to obtain data from authors or no ‘usual care’ control group (online supplemental 4).
Figure 1.

Flow chart of the study selection.
Study characteristics
The 11 included studies represented 15 different interventions and 29 outcome assessments measuring readmission rates at different time points. Two studies were multiarm studies.22 23 Study characteristics are shown in table 1. Five of the included studies were randomised trials (RCTs),23–27 four non-randomised controlled trials (NRCTs)22 28–30 and two pre–post cohort studies.31 32
Table 1.
Study characteristic
| Author (year) | Country setting |
Design | Intervention | Study population | Mean age, years (SD) or median (range) | Female n (%) | Outcomes | OA | Readmission (event/total) | RR (CI) |
| Buurman et al24 (2016) | Netherland | RCT | Transitional care bridge programme intervention | T: 674 | I: 79.7 (7.3) | I: 195 (57.9) |
|
182 | I: 106/316 | 1.15 (0.91–1.45) |
| Multicentre study | I: 337 | C: 80.0 (7.8) | C: 195 (57.9) |
|
C: 88/303 | |||||
| C:337 |
|
|||||||||
| Unselected patients |
|
|||||||||
|
||||||||||
|
||||||||||
| Chow and Wong22 (2014) | Hong Kong | NRCT | The nurse case management intervention | T: 312 | Ia: 75.00 (60–92) | Ia: 46 (52.9) |
|
28 | Ia:14/91 | Ia: 0.67 |
| Single-centre study | Ia: 96 | Ib: 75.50 (60–89) | Ib: 52 (54.2) |
|
Ib: 16/100 | (0.37–1.22) | ||||
| Ib: 108 | C: 77.00 (60–89) | C: 49 (50.0) |
|
C: 24/105 | Ib: 0.70 | |||||
| C: 108 |
|
(0.40–1.24) | ||||||||
| Unselected patients | 84 | Ia: 32/97 | Ia: 0.73 | |||||||
| Ib: 30/106 | (0.52–1.03) | |||||||||
| C: 59/130 | Ib: 0.62 | |||||||||
| (0.43–0.89) | ||||||||||
| Courtney et al25 (2009) | Australia | RCT | Older hospitalised patients’ discharge planning and in-home follow-up protocol | T: 128 | I: 78.1 (6.3) | I: 36 (62.1) |
|
28 | I: 2/49 | 0.26 |
| Single-centre study | I: 64 | C: 79.4 (7.3) | C: 40 (62.5) |
|
C: 9/58 | (0.06–1.15) | ||||
| C: 64 |
|
|||||||||
| Patients at risk |
|
84 | I: 10/49 | 0.74 (0.37–1.48) | ||||||
|
C: 16/58 | |||||||||
| 168 | I: 11/49 | 0.48 (0.27–0.87) | ||||||||
| C: 27/58 | ||||||||||
| Finlayson et al23 (2018) | Australia | RCT | NR | T: 222 | Ic: 77.1 (7.64) | Ic: 46 (80.7) |
|
28 | Ic: 4/53 | Ic: 0.31 |
| Multicentre study | Ic: 57 | Id: 77.6 (6.50) | Id: 42 (75.0) | Id: 7/49 | (0.11–0.89) | |||||
| Id:56 | Ie: 77.8 (6.23) | Ie: 37 (68.5) | Ie: 5/49 | Id: 0.58 | ||||||
| Ie:54 | C: 77.9 (6.20) | C: 37 (67.3) | C: 13/53 | (0.25–1.33) | ||||||
| C:55 | Ie: 0.42 | |||||||||
| Patients at risk | (0.16–1.09) | |||||||||
| 84 | Ic: 11/53 | Ic: 0.55 | ||||||||
| Id: 16/44 | (0.29–1.04) | |||||||||
| Ie: 9/48 | Id: 0.96 | |||||||||
| C: 19/50 | (0.57–1.63) | |||||||||
| Ie: 0.49 | ||||||||||
| (0.25–0.97) | ||||||||||
| 168 | Ic: 18/52 | Ic: 0.75 | ||||||||
| Id: 18/42 | (0.46–1.21) | |||||||||
| Ie: 16/47 | Id: 0.93 | |||||||||
| C: 23/50 | (0.59–1.47) | |||||||||
| Ie: 0.74 | ||||||||||
| (0.45–1.22) | ||||||||||
| Koehler et al26 (2009) | USA | RCT (pilot) | Elderly care bundle | T: 41 | I: 77.2 (5.3) | I: 17 (85) |
|
30 | I: 2/20 | 0.26 (0.06–1.08) |
| Single-centre study | I: 20 | C: 79.8 (5.6) | C: 13 (62) |
|
C: 8/21 | |||||
| C:21 | ||||||||||
| Patients at risk | 60 | I: 6/20 | 0.70 (0.30–1.61) | |||||||
| C: 9/21 | ||||||||||
| Lin et al31 (2015) | Hong Kong | Cohort analytic (two groups pre–post study) | Integrated care and discharge support for elderly patients | T: NR | Total: 80.4±7.6 | T: 557 (51.1) |
|
182 pre | NR | NR |
| Multicentre study | I: 1090 | I: NR |
|
182 post | Reports a statistically significant reduction on 47% in readmissions | |||||
| C: NR | C: NR |
|
||||||||
| Patients at risk | ||||||||||
| Nielsen et al28 (2018) | Denmark | NRCT | Elderly activity performance intervention | T: 375 | I: 81 (7.9) | I: 79 (55) |
|
30 | I: 25/139 | 0.76 (0.50–1.16) |
| Single-centre study | I:144 | C: 78 (8.6) | C: 122 (53) |
|
C: 55/231 | |||||
| C: 231 |
|
|||||||||
| Unselected patients |
|
182 | I: 64/144 | 1.04 (0.82–1.32) | ||||||
| C: 99/231 | ||||||||||
| Robinson et al32 (2015) | New Zealand | Cohort analytic (two groups pre–post study) | Integrated transition of care | T: 19 157 | I: 78.2 (9.2) | I: 2486 (48.1) |
|
7 | I: 500/5172 | 1.09 (0.99–1.20) |
| Multicentre study | I: 5172 | C: 77.6 (9.1) | C: 6765 (48.4) |
|
C: 1239/13 985 | |||||
| C:13 985 | 28 | I: 1370/5172 | 1.03 (0.98–1.09) | |||||||
| Patients at risk | C: 3588/13 985 | |||||||||
| 90 | I: 2281/5172 | 1.01 (0.97–1.05) | ||||||||
| C: 6079/13 985 | ||||||||||
| Rottman-Sagebiel et al29 (2018) | USA | NRCT | The geriatrics medication education at discharge project | T: 1624 | I: 74.9 (7.6) | I: 14 (3.6) |
|
30 | NR | NR |
| I: 435 | C: 75.2 (8.35) | C: 26 (2.2) | ||||||||
| Single-centre study | C: 1189 | |||||||||
| Patients at risk | ||||||||||
| Sahota et al27 (2017) | UK | RCT | The community in-reach rehabilitation and care transition | T: 250 | I: 83.6 (6.6) | I: 82 (66) |
|
28 | I: 18/106 | 1.29 (0.68–2.46) |
| Single-centre study | I: 125 | C: 84.5 (5.9) | C: 79 (63) |
|
C: 14/106 | |||||
| C: 125 |
|
|||||||||
| Unselected patients |
|
|||||||||
|
||||||||||
|
||||||||||
|
91 | I: 45/106 | 1.15 (0.82–1.61) | |||||||
| C: 39/106 | ||||||||||
| Voss et al30 (2011) | USA | NRCT | Care transitions intervention | T: 1888 | I: NR | I: NR |
|
30 | NR | NR |
| Multicentre study | I: 1042 | C: NR | C: NR | |||||||
| C: 846 | ||||||||||
| Unselected patients |
ADL, activity of daily living; AED, accident and emergency departments; C, control; CGA, comprehensive geriatric assessment; I, intervention; Ia, ‘Home visit’; Ib, ‘Call’; Ic, EN-HaT (exercise and nurse home visit and telephone follow-up); Id, exercise; Ie, N-HaT (nurse home visit and telephone follow-up); LOS, length of hospital stay; NR, not reported or author could not access the raw data; NRCT, non-randomised controlled trial; OA, readmission outcome assessment in days after hospital discharge; RCT, randomised trial; RR, relative risk; T, total.
Sample sizes of individual studies ranged from 41 to 19 157. Allocation to intervention or control group was performed on an individual level. The majority of studies reported that readmissions were unplanned or acute.23–28 32
Outcome assessments were conducted 7–182 days after discharge. In addition to readmission, the 11 studies assessed outcomes according to physical functioning24 27; cognitive functioning24; quality of life22 25 27; time to either hospital readmission or discharge from nursing homes24 28; self-efficacy22; self-rated health22; visits to EDs, general practitioners or allied health professional25 26 28 31 32; length of stay27 31; comorbidity27; cost-effectiveness27 and mortality.24 28Three studies took place in USA,26 29 30 two in Australia,23 25 two in Hong Kong,22 31 one in the Netherlands,24 one in the UK,27 one in Denmark28 and one in New Zealand.32 The studies were published between 2009 and 2018.
Study population
In total, approximately 24 500 patients were evaluated in our review; 8800 in the intervention groups and 15 700 in the control groups. The mean age of the participants in the intervention groups was approximately 78 years (range 74.9–83.6), while the mean age among the control groups was approximately 79 years (range 75.2–84.5). Approximately 59% (range 3.6–85) of the participants in the intervention groups were women and 52% (range 2.2–67) of the participants in the control group were women.
TCIs
All studies included predischarge and postdischarge components and some included bridging components. The most pronounced difference between the interventions was in the predischarge phase, whereas elements in the bridging and postdischarge phase were somewhat similar. Table 2 outlines the intervention components, and online supplemental 5 contains detailed descriptions of the interventions.
Table 2.
Intervention components
| Study | Predischarge components | Bridging components | Postdischarge components | ||||||||||||||||||||
| Patient assessment | Personal health record and/or plan | Education | Medication reconciliation | Physical exercise | Address concerns and/or barriers | Counselling | Discharge planning | Nutrition screening | Caregiver involvement | Home visit to assess future needs | Multidisciplinary care | In- person hand -over | Written hand -over | Telephone hand -over | Community -based nurse visits hospital | Communications path unknown | Number of home visits | Number of telephone follow- up | Nurse availability | Referral to additional services | Intensive community support | Intervention intensity | |
| Buurman et al24 | + | + | + | + | + | 5* | 9 | ||||||||||||||||
| Chow et al22† | + | + | + | 2* | 2 | 6 | |||||||||||||||||
| Chow et al22‡ | + | + | + | 4 | 6 | ||||||||||||||||||
| Courtney et al25 | + | + | + | + | + | + | + | 1*§, | 9 | 12 | |||||||||||||
| Finlayson et al23¶ | + | + | + | + | + | 6** | 10 | ||||||||||||||||
| Finlayson et al23†† | + | + | + | + | + | 1*§ | 10 | + | 12 | ||||||||||||||
| Finlayson et al23‡‡ | + | + | + | + | + | + | 1*§ 6** |
10 | + | 12 | |||||||||||||
| Koehler et al26 | + | + | + | + | + | + | + | + | + | 2§§ | 7 | ||||||||||||
| Lin et al31¶¶ | + | + | + | ?*** | ? | 6 | |||||||||||||||||
| Lin et al31††† | + | + | + | +‡‡‡ | + | 5 | |||||||||||||||||
| Nielsen et al28 | + | +‡‡‡ | + | + | 1* | 4 | |||||||||||||||||
| Robinson et al32 | + | +§§§ | +§§§ | + | + | + | +‡‡‡ | 2¶¶¶ | 7 | ||||||||||||||
| Rottman-Sagebiel et al29 | +§§§ | +§§§ | + | + | + | +‡‡‡ | 1 | +‡‡‡ | 6 | ||||||||||||||
| Sahota et al27 | + | + | + | + | + | 1§*** | +‡‡‡ | 3 | |||||||||||||||
| Voss et al30 | + | + | 1* | 3 | 7 | ||||||||||||||||||
?, number not reported.
*First visit within 3 days after discharge.
†Postdischarge home visit group.
‡Postdischarge call group.
§Additional home visits available if needed.
¶Exercise intervention.
**By physiotherapist.
††N-Hat (nurse home visit and telephone follow-up) intervention.
‡‡Ex-Hat (exercise and nurse home visit and telephone follow-up) intervention.
§§One call by nurse and one call by pharmacist.
¶¶ICM case management group.
***Time for first home visit unknown.
†††HST service group.
‡‡‡If deemed necessary.
§§§By pharmacist.
¶¶¶To participants who return to independent living.
Predischarge components
Across studies, predischarge components consisted of health record or plan, discharge planning, involvement of caregivers, concerns or barriers, patient education, physical exercise (physical exercise (muscle strength, stretch, balance and walking), medication reconciliation, counselling, nutritional screening, predischarge home visit or patient assessments (comprehensive geriatric assessment, problem classification scheme, assessment of patients’ performance of daily activities and assessment of motor and process skills).
Bridging components
Bridging components consisted of written handover between hospital and primary sector, telephone handover or in-person handover.
Postdischarge components
Postdischarge components comprised of home visits, telephone follow-up, referral to additional healthcare services (rehabilitation, early specialist follow-up, general practitioner or other community services), nurse availability from hospital discharge until 7 days after discharge or rapid and intensive community support.
Synthesis of results
All five aspects that may introduce heterogeneity were analysed and a pronounced diversity between the included studies was found. Additionally, some studies had incomplete reporting of study effects. Therefore, because of the heterogeneity, a meta-analysis could not be conducted.
Considering the impact on outcome level, 22 of the 29 outcome results (76%) showed a positive impact on readmission in the intervention groups compared with the control groups. Three studies did not report readmission rates but reported a positive impact on readmission rates, and it was not possible to obtain these numbers from the authors.29–31 It was not possible to calculate RRs and their 95% CIs for those studies, and they are therefore not presented in the forest plots.
The impact size (RR) from individual studies was calculated using the reported readmission rates from eight studies. RRs ranged from 0.26 to 1.29. Nineteen outcome results were <1 of which one was close to 1 (RR=0.96). Seven estimates were >1 of which three were close to 1 (RR=1.01, 1.03, 1.04). Of the 29 outcome results, five were statistically significant.22 23 25 26 31
Considering the impact on study level, seven of the 11 studies showed an entirely positive impact on readmissions,22 23 25 26 29–31 while one study presented both a positive impact and no impact,28 and three studies showed no impact at all.24 27
Subgroup analysis
Study population
Online supplemental 6 exhibits impact according to the included study population. There is a clear difference in impacts between the groups. In total, 14 of 17 (82%) interventions including ‘patients at risk’ reported positive impacts on readmission rates. In contrast, only five out of nine (56%) interventions including ‘unselected patients’ reported positive impacts. In addition, the positive impacts were larger among interventions including patients at risk than among interventions with unselected patients. Three of the four statistically significant results are found among the patients at risk group. However, the 95% CIs are wider among patients at risk compared with the unselected patients indicating less precise effect estimates.
Intervention intensity
Calculation of intervention intensity was inspired by Verhaegh et al.33 Ten interventions were categorised as low intensity22 26–32 and five were categorised as high intensity.23–25
Online supplemental 7 illustrates a clear difference. The vast majority of interventions with a high intensity reported a positive impact on readmission rates whereas only half of the interventions with a low intensity showed a positive impact. The impacts were larger and statistically significant among high-intensive interventions.
Length of support
The interventions lasted from enrolment until 1 day to 6 months after hospital discharge. Four studies lasted between 1 and 7 days,28 29 32 two studies lasted 28 and 30 days,30 one study 84 days,31 two 168 days,24 one 182 days25 and one study did not report the duration of the intervention.27 Online supplemental 8 displays the impact on readmission rates according to the duration of the interventions. A short length of support is associated with less or no impact on readmission rates. A length of support of 1 month or more is associated with positive, larger and statistically significant impacts.
Country of origin
Studies conducted outside the European countries seemed to have a greater impact on readmissions than studies conducted within the European Union and all statistically significant results are found in studies conducted in non-European countries (online supplemental 9).
Outcome assessment
The impact on readmissions was largest within 30 days after hospital discharge. The impact decreased hereafter and was similar between 1 month and 6 months after discharge. Most statistically significant results are found when outcomes are assessed between 1 and 3 months (online supplemental 10).
Quality assessment within studies
Of the 11 studies, two studies were assessed to have a strong methodological quality,22 25 three had a moderate24 27 32 and six had a weak methodological quality.23 26 28–31 Of the RCTs, one had a strong,25 two had a moderate24 27 and two had a weak quality.23 26 Of the NRCTs, one study had a strong22 and three had a weak quality.28–30 One of the pre–post cohort studies had a moderate32 and one had a weak quality31 (table 3).
Table 3.
Quality assessment
| Author | Selection bias | Study design | Confounders | Blinding | Data collection methods | Withdrawals and drop-outs | Global rating |
| Buurman et al24 | Moderate | Strong | Strong | Strong | Strong | Weak | Moderate |
| Chow et al22 | Moderate | Strong | Strong | Moderate | Strong | Strong | Strong |
| Courtney et al25 | Moderate | Strong | Strong | Moderate | Strong | Moderate | Strong |
| Finlayson et al23 | Weak | Strong | Strong | Weak | Weak | Moderate | Weak |
| Koehler et al26 | Weak | Strong | Strong | Weak | Strong | Weak | Weak |
| Lin et al31 | Strong | Moderate | Weak | Weak | Weak | Strong | Weak |
| Nielsen et al28 | Strong | Strong | Strong | Weak | Strong | Weak | Weak |
| Robinson et al32 | Strong | Moderate | Strong | Weak | Strong | Strong | Moderate |
| Rottman-Sagebiel et al29 | Weak | Strong | Strong | Weak | Weak | Weak | Weak |
| Sahota et al27 | Strong | Strong | Strong | Weak | Strong | Moderate | Moderate |
| Voss et al30 | Weak | Strong | Strong | Weak | Strong | Weak | Weak |
Quality assessment across studies
The majority of the studies did not meet the criteria in the components selection bias and blinding and were thus rated moderate or weak. The vast majority of studies met the criteria of study design, confounders and data collection and were therefore rated strong (figure 2).
Figure 2.
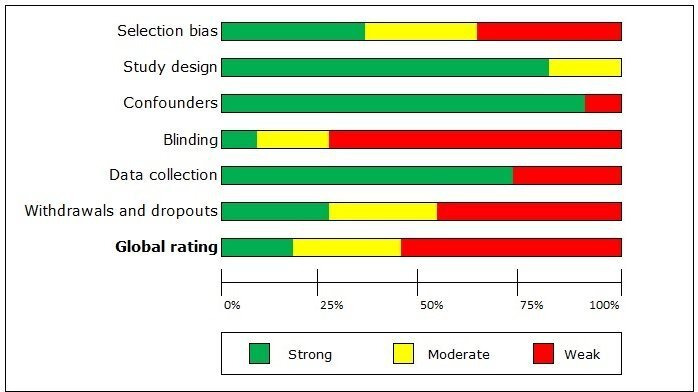
Quality assessment across studies. The green colour indicates strong methodological quality, yellow indicates moderate quality and red indicates weak quality across studies.
Discussion
We found that the majority of interventions in the transitional phase between hospital and home appears to reduce readmission rates among older patients discharged from a medical ward.
However, some studies reported both a positive impact and no impact on the readmission rate following similar care interventions. These divergent results may have several plausible explanations as discussed below.
Explanations related to study characteristics
Country of origin
Studies conducted in European countries have less impact than studies conducted in non-European countries. The impact of complex interventions is, among others, altered by the context of the implementation,34 35 and differences in impact between countries may therefore be explained by diversity in the social, political, economic, clinical and geographical setting. The accessibility, type, character, quality and overall comprehensiveness of healthcare services provided may also play a role.36 The USA and Australia have a long history of discharge planning and transitional care, and these countries therefore have a high quantity of research as well as refined strategies and guidelines.37–39
Study population
The impact on readmissions is greater among patients at risk than among ‘unselected older patients’. This is to be expected as readmission rates are higher among patients at risk than among unselected patients. Furthermore, patients at risk are more frail and may have a higher degree of morbidity, which could have affected the risk of readmission.40
Readmission rates prior to the study
Preintervention readmission rates may mirror differences in impact between studies. It may be assumed that hospitals with low preintervention readmission rates may experience no reduction of postintervention readmission rates as the remaining readmissions may not be preventable. In contrast, it may also be assumed that hospitals with high preintervention readmission rates will achieve a reduction in postintervention readmission rates.
Sample size
Several studies had small sample sizes. As seen in table 1, studies with small sample sizes reported a stronger impact than studies with larger sample sizes. This is in line with Dechartres et al who also reported larger effect sizes in small-to-moderate-sized trials than in larger trials.41 One reason may be that small studies are more prone to publication bias than larger studies.42
Explanations related to review findings
Interventions
Our findings suggest that the intensity of interventions influences the impact on readmission rates as high-intensity interventions generally have a stronger impact than low-intensity interventions. This is in line with previous findings presented by Verhaegh et al.33 The higher quantity of elements means that more aspects in a complex patient cohort and complex settings can be addressed.
Intervention components that at first glance appear to be similar across studies may comprise different features. The diverging impact on readmissions may be affected by differences in intervention contents across studies. It is not possible to make an intervention component analysis across studies that evaluates which components positively affect readmissions. However, some trends are seen in table 2. Interventions with a positive impact on readmission comprise the following components: patient assessment, personal health record or plan, concerns and barriers, discharge planning, caregiver involvement, home visits and telephone follow-up.
Intervention fidelity
The impact on readmission rates may be affected by the fidelity of the interventions.43 However, several studies do not describe intervention fidelity, which may be due to inconsistency in monitoring of the implementation or lack of transparency in reporting the study. These shortcomings thus hinder assessment of whether lack of positive impact is caused by poor implementation of the intervention or if the intervention did not work.
Outcome assessment
The timing of the outcome assessment has an important bearing on the possible preventive readmission rate.44 The findings of this review suggest that interventions have the largest impact within the first 30 days after discharge. A potential impact is likely to have obliterated if outcome is assessed later than 30 days after discharge.
Residual confounding
Several of the included studies did not adjust for potential confounders such as length of stay, fall within the past 12 months, living conditions, prior admissions, poor overall health condition and functional disability.45–47 This could have affected the internal validity and the impact on readmission rates. The lack of analysis adjusting for potential confounders is highlighted in previous studies,48 underlining the problematic trend in this research area.
Risk of bias
Differences in the quality assessment and thus risk of bias may explain the variation in the impact of the included studies.16 Online supplemental 11 shows that studies assessed to have weak and strong methodological quality have a positive impact on readmission rates whereas studies with moderate quality have no impact.
Statistical analysis
Several authors fail to report whether the statistical analysis is performed based on the first readmission. One patient may therefore represent several readmissions within a specific follow-up period. If this is the case, results from those studies may report a higher readmission rate and thus greater impact than studies using unique observations in their statistical analysis.
Quality assessment
The methodological quality of the majority of the included studies was low, thus indicating a high risk of bias. Low global rating can reflect both the methodological quality and insufficient reporting of the methodology. The latter makes it difficult to accurately assess the true quality and thus the risk of bias. If the low rating is caused by insufficient methodological reporting, it may have no effect on the impact. However, if the low rating reflects methodological problems, it probably underestimates the true impact of the interventions.
The component ‘blinding’ represents the weakest rating. Blinding of participants was not always possible due to the nature of the interventions. Blinding is crucial in pharmaceutical trials and in other clinical studies. However, little is known about the benefits or disadvantages of blinding participants in complex interventions and how bias due to blinding may affect the results. Blinding outcome assessors may not be crucial when outcome is collected through digital records.
Comparison with previous research
Prior systematic reviews included other study populations such as surgical patients or patients with only one medical condition. The present review includes a broader population, namely older medical patients. Direct comparison of the present findings with previous findings is therefore difficult. The present review suggests that TCIs reduce the risk of readmission among older medical patients.
These findings are in line with findings in similar reviews that found positive effects of TCIs on hospital readmission.49–51 These reviews also found that the included studies had a very-low-to-moderate methodological quality.
Limitation of included evidence base
Transparency across studies is lacking even if the Consolidated Standards of Reporting Trials statement recommends reporting a sufficient description of interventions.52 A call for more transparency in clinical trials and adherence to appropriate guidelines is also reported elsewhere.53 If the template for the intervention description and replication is followed, the replicability may improve, thus making it possible to build on prior research findings.54
Evaluating TCIs provides insight into whether interventions reduce readmissions among intervention groups compared with control groups. However, we gain no knowledge about causality between exposure and outcome. In complex interventions, such as TCIs, it is difficult to evaluate which mechanisms or components result in change.55 A process evaluation may have captured the fidelity of the interventions and may thus have provided insight into which mechanisms and components actually work.56 Process evaluation has previously been requested,57 stressing the unmet need to identify essential components in TCIs. We have requested missing intervention details and other relevant data from authors; some requests were met while others were not. Lastly, all GRADE domains except one (indirectness of evidence) were assessed and found to downgrade the evidence and hence, lower the certainty of the evidence of this review.
Strengths and limitations of this review
The study has several strengths. This review adhered to PRISMA15 and synthesis without meta-analysis58 which ensures that all important methodological considerations were made. By reducing the risk of bias in this review, systematic errors were minimised during all stages of the process.
Despite these strengths, we note some limitations. The eligibility criteria were somewhat narrow, which limited the number of included studies. This, however, was deemed necessary to meet the need for evidence focusing on clinical settings where a large number of hospital wards are general medical wards.
Only studies published in English, Danish, Norwegian or Swedish were eligible for inclusion in this review. Therefore, studies published in other languages were omitted, potentially excluding useful evidence.
This review only focuses on hospital readmission as an outcome although the included studies evaluated the intervention impact on multiple outcomes. It is therefore possible that some studies report a positive impact in terms of other outcomes than readmission.
Positive findings are more likely to be published in English language journals, whereas negative findings are more often published in local-language journals.59 Publication bias is therefore likely present. During this review process, we have contacted several researchers who had registered TCIs on ClinicalTrials.gov. All researchers who found no or negative impact either struggled to publish or decided not to publish. The above-mentioned issues may result in an underrepresentation of negative results in the evidence base and thus in this present review.
Implications and future research
Future research projects may benefit from the knowledge gained from the present review when designing and developing new studies. Knowing that interventions with a minimum duration of 1 month that have a high intensity and target high-risk patients may result in more effective interventions.
This review highlights an unmet need for studies of high methodological quality that evaluate the impact of TCIs among older medical patients. Therefore, future research can benefit from a higher level of adherence to relevant guidelines and more detailed descriptions of (1) interventions and comparison groups, (2) the implementation process and (3) actions taken to minimise bias and confounding. Further research should be undertaken to investigate the process evaluations of complex interventions to identify how and why interventions either work or do not work. To develop a broader picture of TCIs, additional studies need to focus on psychological outcomes. The societal cost of such interventions versus individual and societal benefits needs to be further evaluated. High-risk patients such as physically disabled, chronically ill patients may benefit from these kinds of interventions regardless of age and comorbidity.60
Conclusion
The majority of TCIs have a positive impact on readmission rates among older medical patients, although the most significant impact was seen within 30 days after hospital discharge. Therefore, we believe that the current evidence supports recommending transitional care that includes both predischarge and postdischarge components. However, no evidence for recommending a specific intervention exists. The key finding shows an apparent pronounced positive impact among patients categorised as patients at risk in ‘high-intensity’ interventions and in interventions with duration of 1 month or more. This, however, should be seen in the light of the fact that only 11 studies met the inclusion criteria and a low certainty of evidence according to the GRADE approach.
Supplementary Material
Footnotes
Contributors: All authors listed have contributed sufficiently to the project to be included as authors according to the Vancouver Guideline. All authors have participated in the development of the study, writing the draft and all have approved the final version. LFR: first author writing the manuscript, screening records for inclusion, data extraction of included studies, quality assessment of included studies. LBG, JL, IB, MG: initial development of the study, screening records for inclusion, data extraction of included studies, quality assessment of included studies, reading and giving feedback on the manuscript and approving the final manuscript.
Funding: This work was supported by the ‘Fund for advancement of health research in Central Denmark Region’. Grant number N/A.
Competing interests: None declared.
Patient consent for publication: Not required.
Provenance and peer review: Not commissioned; externally peer reviewed
Data availability statement: All data relevant to the study are included in the article or uploaded as supplementary information.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
References
- 1.World Health Organisation World report on ageing and health, 2015. [Google Scholar]
- 2.Lehnert T, Heider D, Leicht H, et al. Review: health care utilization and costs of elderly persons with multiple chronic conditions. Med Care Res Rev 2011;68:387–420. 10.1177/1077558711399580 [DOI] [PubMed] [Google Scholar]
- 3.Holm EA, Rønholt F, eds Geriatri (Geriatrics), 2016. [Google Scholar]
- 4.Sundhedsdatastyrelsen Ældre medicinske patienters kontakt med det regionale sundhedsvæsenog den kommunale pleje (older medical patients’ contact to the regional healthcare system and the home care): Afdelingen for Sundhedsanalyser og lægemiddelstatistik, 2016. [Google Scholar]
- 5.Sundheds- og Ældreministeriet Styrket indsats for den ældre medicinske patient. National handlingsplan 2016 (Improved effort for the elderly medical patient. National action plan), 2016. [Google Scholar]
- 6.Coleman EA, Min S-joon, Chomiak A, et al. Posthospital care transitions: patterns, complications, and risk identification. Health Serv Res 2004;39:1449–66. 10.1111/j.1475-6773.2004.00298.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the medicare fee-for-service program. N Engl J Med 2009;360:1418–28. 10.1056/NEJMsa0803563 [DOI] [PubMed] [Google Scholar]
- 8.Mesteig M, Helbostad JL, Sletvold O, et al. Unwanted incidents during transition of geriatric patients from hospital to home: a prospective observational study. BMC Health Serv Res 2010;10 10.1186/1472-6963-10-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.National Transitions of Care Coalition Improving transitions of care. Findings and considerations of the ‘vision of the National of care coalition’, 2010. [Google Scholar]
- 10.Russell L, Doggett J, Dawda P. Patient safety – handover of care between primary and acute care. policy review and analysis. Prepared for the National lead clinicians group by the Australian primary health care research Institute, 2013. [Google Scholar]
- 11.Saleh SS, Freire C, Morris-Dickinson G, et al. An effectiveness and cost-benefit analysis of a hospital-based discharge transition program for elderly Medicare recipients. J Am Geriatr Soc 2012;60:1051–6. 10.1111/j.1532-5415.2012.03992.x [DOI] [PubMed] [Google Scholar]
- 12.Fan L, Lukin W, Zhao J, et al. Interventions targeting the elderly population to reduce emergency department utilisation: a literature review. Emerg Med J 2015;32:738–43. 10.1136/emermed-2014-203770 [DOI] [PubMed] [Google Scholar]
- 13.Linertová R, García-Pérez L, Vázquez-Díaz JR, et al. Interventions to reduce hospital readmissions in the elderly: in-hospital or home care. A systematic review. J Eval Clin Pract 2011;17:1167–75. 10.1111/j.1365-2753.2010.01493.x [DOI] [PubMed] [Google Scholar]
- 14.National Institute for Health Research PRPSPERO International prospective register of systematic reviews. Available: https://www.crd.york.ac.uk/prospero/
- 15.Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009;339:b2535 10.1136/bmj.b2535 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Higgins JPT, Thomas J, Chandler J. Cochrane handbook for systematic reviews of interventions version 6.0 (updated July 2019): cochrane, 2019. [Google Scholar]
- 17.Paez A. Gray literature: an important resource in systematic reviews. J Evid Based Med 2017;10:233–40. 10.1111/jebm.12266 [DOI] [PubMed] [Google Scholar]
- 18.Cochrane Effective Practice and Organisation of Care (EPOC) Data collaction form.: EPOC resources for review authors, 2017. Available: https://epoc.cochrane.org/resources/epoc-resources-review-authorsMarch
- 19.Armstrong R, Waters E, Jackson N. Guidelines for systematic reviews of health promotion and public health interventions. version 2. Australia: Melbourne University, 2007. [Google Scholar]
- 20.Deeks J, Dinnes J, D’Amico R. Evaluating non-randomised intervention studies. 7 Health Technol Assess England, 2003. 10.3310/hta7270 [DOI] [PubMed] [Google Scholar]
- 21.Pigott T, Shepperd S. Identifying, documenting, and examining heterogeneity in systematic reviews of complex interventions. J Clin Epidemiol 2013;66:1244–50. 10.1016/j.jclinepi.2013.06.013 [DOI] [PubMed] [Google Scholar]
- 22.Chow SKY, Wong FKY. A randomized controlled trial of a nurse-led case management programme for hospital-discharged older adults with co-morbidities. J Adv Nurs 2014;70:2257–71. 10.1111/jan.12375 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Finlayson K, Chang AM, Courtney MD, et al. Transitional care interventions reduce unplanned Hospital readmissions in high-risk older adults. BMC Health Serv Res 2018;18:956 10.1186/s12913-018-3771-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Buurman BM, Parlevliet JL, Allore HG. Comprehensive geriatric assessment and transitional care in acutely hospitalized patients the transitional care bridge randomized clinical trial. JAMA Intern Med 2016;176:302–9. [DOI] [PubMed] [Google Scholar]
- 25.Courtney M, Edwards H, Chang A, et al. Fewer emergency readmissions and better quality of life for older adults at risk of hospital readmission: a randomized controlled trial to determine the effectiveness of a 24-week exercise and telephone follow-up program. J Am Geriatr Soc 2009;57:395–402. 10.1111/j.1532-5415.2009.02138.x [DOI] [PubMed] [Google Scholar]
- 26.Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day postdischarge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med 2009;4:211–8. 10.1002/jhm.427 [DOI] [PubMed] [Google Scholar]
- 27.Sahota O, Pulikottil-Jacob R, Marshall F. The community in-reach rehabilitation and care transition (CIRACT) clinical and cost-effectiveness randomisation controlled trial in older people admitted to hospital as an acute medical emergency. Age Ageing 2017;46:26–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Nielsen L, Maribo T, Kirkegaard H, et al. Effectiveness of the elderly activity performance intervention on elderly patients discharge from a short-stay unit at the emergency department: a quasi-experimental trial. Clin Interv Aging 2018;13:737–47. 10.2147/CIA.S162623 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Rottman-Sagebiel R, Cupples N, Wang CP. A pharmacist-led transitional care program to reduce hospital readmissions in older adults. Fed Pract 2018;35:42–50. [PMC free article] [PubMed] [Google Scholar]
- 30.Voss R, Gardner R, Baier R. The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med 2011;171:1232–7. [DOI] [PubMed] [Google Scholar]
- 31.Lin FO, Luk JK, Chan TC. Effectiveness of a discharge planning and community support programme in preventing readmission of high-risk older patients. Hong Kong Med J 2015;21:208–16. [DOI] [PubMed] [Google Scholar]
- 32.Robinson TE, Zhou L, Kerse N, et al. Evaluation of a new Zealand program to improve transition of care for older high risk adults. Australas J Ageing 2015;34:269–74. 10.1111/ajag.12232 [DOI] [PubMed] [Google Scholar]
- 33.Verhaegh KJ, MacNeil-Vroomen JL, Eslami S, et al. Transitional care interventions prevent hospital readmissions for adults with chronic illnesses. Health Aff 2014;33:1531–9. 10.1377/hlthaff.2014.0160 [DOI] [PubMed] [Google Scholar]
- 34.Pfadenhauer LM, Gerhardus A, Mozygemba K, et al. Making sense of complexity in context and implementation: the context and implementation of complex interventions (CICI) framework. Implementation Sci 2017;12:21 10.1186/s13012-017-0552-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Wells M, Williams B, Treweek S, et al. Intervention description is not enough: evidence from an in-depth multiple case study on the untold role and impact of context in randomised controlled trials of seven complex interventions. Trials 2012;13:95 10.1186/1745-6215-13-95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Krumholz HM, Wang K, Lin Z, et al. Hospital-readmission risk — isolating hospital effects from patient effects. N Engl J Med 2017;377:1055–64. 10.1056/NEJMsa1702321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bixby MB, Naylor MD. The transitional care model (TCM): hospital discharge screening criteria for high risk older adults. Medsurg Nurs 2010;19:62–3. [PubMed] [Google Scholar]
- 38.Naylor M, Brooten D, Jones R. Comprehensive discharge planning for the hospitalized elderly. A randomized clinical trial. Ann Intern Med 1994;120:999–1006. [DOI] [PubMed] [Google Scholar]
- 39.Parry C, Coleman EA, Smith JD, et al. The care transitions intervention: a patient-centered approach to ensuring effective transfers between sites of geriatric care. Home Health Care Serv Q 2003;22:1–17. 10.1300/J027v22n03_01 [DOI] [PubMed] [Google Scholar]
- 40.Stillman GR, Stillman AN, Beecher MS. Frailty is associated with early Hospital readmission in older medical patients. J Appl Gerontol 2019:733464819894926 10.1177/0733464819894926 [DOI] [PubMed] [Google Scholar]
- 41.Dechartres A, Trinquart L, Boutron I, et al. Influence of trial sample size on treatment effect estimates: meta-epidemiological study. BMJ 2013;346:f2304. 10.1136/bmj.f2304 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Slavin R, Smith D. The relationship between sample sizes and effect sizes in systematic reviews in education. Educ Eval Policy Anal 2009;31:500–6. 10.3102/0162373709352369 [DOI] [Google Scholar]
- 43.Horner S, Rew L, Torres R. Enhancing intervention fidelity: a means of strengthening study impact. J Spec Pediatr Nurs 2006;11:80–9. 10.1111/j.1744-6155.2006.00050.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Fahlberg B. Preventing readmissions through transitional care. Nursing 2017;47:12–14. 10.1097/01.NURSE.0000512879.91386.22 [DOI] [PubMed] [Google Scholar]
- 45.Hallgren J, Aslan AKD. Risk factors for hospital readmission among Swedish older adults. Eur Geriatr Med 2018;9:603–11. 10.1007/s41999-018-0101-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hughes LD, Witham MD. Causes and correlates of 30 day and 180 day readmission following discharge from a medicine for the elderly rehabilitation unit. BMC Geriatr 2018;18:197 10.1186/s12877-018-0883-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Pedersen MK, Meyer G, Uhrenfeldt L. Risk factors for acute care hospital readmission in older persons in Western countries: a systematic review. JBI Database System Rev Implement Rep 2017;15:454–85. 10.11124/JBISRIR-2016-003267 [DOI] [PubMed] [Google Scholar]
- 48.Hughes JM, Freiermuth CE, Shepherd‐Banigan M, et al. Emergency department interventions for older adults: a systematic review. J Am Geriatr Soc 2019;67:1516–25. 10.1111/jgs.15854 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Le Berre M, Maimon G, Sourial N, et al. Impact of transitional care services for chronically ill older patients: a systematic evidence review. J Am Geriatr Soc 2017;65:1597–608. 10.1111/jgs.14828 [DOI] [PubMed] [Google Scholar]
- 50.Mabire C, Dwyer A, Garnier A, et al. Effectiveness of nursing discharge planning interventions on health-related outcomes in discharged elderly inpatients: a systematic review. JBI Database System Rev Implement Rep 2016;14:217–60. 10.11124/JBISRIR-2016-003085 [DOI] [PubMed] [Google Scholar]
- 51.Weeks LE, Macdonald M, Martin-Misener R, et al. The impact of transitional care programs on health services utilization in community-dwelling older adults: a systematic review. JBI Database System Rev Implement Rep 2018;16:345–84. 10.11124/JBISRIR-2017-003486 [DOI] [PubMed] [Google Scholar]
- 52.Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMC Med 2010;8:18 10.1186/1741-7015-8-18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Ramírez JH. Lack of transparency in clinical trials: a call for action. Colomb Med 2013;44:243–6. 10.25100/cm.v44i4.1475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348:g1687 10.1136/bmj.g1687 [DOI] [PubMed] [Google Scholar]
- 55.Craig P, Dieppe P, Macintyre S, et al. Developing and evaluating complex interventions: the new medical research council guidance. BMJ 2008;337:a1655. 10.1136/bmj.a1655 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Moore GF, Audrey S, Barker M, et al. Process evaluation of complex interventions: medical research council guidance. BMJ 2015;350:h1258 10.1136/bmj.h1258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Mansah M, Fernandez R, Griffiths R, et al. Effectiveness of strategies to promote safe transition of elderly people across care settings. JBI Libr Syst Rev 2009;7:1036–90. 10.11124/jbisrir-2009-206 [DOI] [PubMed] [Google Scholar]
- 58.Campbell M, McKenzie JE, Sowden A, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ 2020;72:l6890 10.1136/bmj.l6890 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Hopewell S, Loudon K, Clarke MJ. Publication bias in clinical trials due to statistical significance or direction of trial results. Cochrane Database Syst Rev 2009;1:MR000006.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Arbaje AI, Kansagara DL, Salanitro AH, et al. Regardless of age: incorporating principles from geriatric medicine to improve care transitions for patients with complex needs. J Gen Intern Med 2014;29:932–9. 10.1007/s11606-013-2729-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2020-040057supp001.pdf (475.8KB, pdf)