

Abstract
Background
The impact that the coronavirus disease 2019 (COVID-19)–related early lockdown has had on dietary habits of the population and on food insecurity is unknown.
Objective
The aim of this study was to document the change in diet quality and in food insecurity observed during the COVID-19–related early lockdown. We hypothesized that the lockdown was associated with a deterioration in overall diet quality and an increase in food insecurity.
Methods
Data are from a COVID-19 subsample of NutriQuébec, a web-based cohort destined to study temporal changes in dietary habits among adults in Quebec, Canada. Participants completed questionnaires before (between June 2019 and February 2020) and during (April to May 2020) early lockdown, including a validated web-based 24-h recall (n = 853) and a questionnaire on food security (n = 922). Primary study outcomes were temporal changes in diet quality measured by the Healthy Eating Index (HEI)–2015 and in the prevalence of food insecurity.
Results
There was a small increase in the HEI-2015 during the COVID-19 early lockdown compared with baseline (+1.1 points; 95% CI: 0.6, 1.5), mostly due to small improvements in the intakes of whole grains, greens and beans, refined grains, total vegetables, total dairy, seafood and plant proteins, added sugar, and total protein subscores of the HEI-2015. Exploratory analyses suggested that individuals aged 18–29 y (+3.6 points; 95% CI: 2.4, 4.7), participants with lower education (+1.9 points; 95% CI: 1.3, 2.6), or with obesity (+3.8 points; 95% CI: 2.7, 4.8) showed particularly important increases in the HEI-2015. The prevalence of food insecurity was reduced from 3.8% at baseline to 1.0% during the early lockdown (prevalence ratio = 0.27; 95% CI: 0.08, 0.94).
Conclusions
Contrary to our hypotheses, diet quality has slightly improved and prevalence of food insecurity was reduced in this sample of adults from Quebec during the COVID-19–related early lockdown. These results may be generalizable only to relatively healthy populations.
Keywords: COVID-19, diet quality, eating habits, prospective study, web-based study, 24-hour recalls
See corresponding editorial on page 763 and article on page 924.
Introduction
The coronavirus disease 2019 (COVID-19)–related early lockdown period has had a profound impact on all of human life’s activities worldwide. The mitigation measures implemented in most countries, combined with the shutdown of most industries including restaurants, have forced people to home confinement for many months. There are suggestions that the COVID-19 pandemic may have both direct and indirect impacts on food security and nutrition (1), with outcomes being dependent on the baseline situation of communities, countries, and regions, as well as on their resilience to shocks (2). On the one hand, it is tempting to hypothesize that home confinement due to the COVID-19–related lockdown may have led to improvement in the quality of the diet based on evidence suggesting that the frequency of cooking and eating at home is associated with better overall diet quality (3, 4, 5). However, this has not been a consistent finding (6). Notably, the positive association between eating at home and diet quality has been shown to be stronger among high-income than among low-income adults. Further supporting the hypothesis that diet quality may have improved during the COVID-19–related early lockdown period, half of American adults in nonscientific surveys mentioned cooking more often during the early onset of the lockdown (7, 8). Similar data have been reported in Canada (9).
On the other hand, the COVID-19–related early lockdown has had an immediate and direct impact on food supplies and demand, while also indirectly decreasing financial capacity to purchase foods due to loss of work, even more so among more vulnerable populations (2). This change in paradigm has possibly increased economic and social tensions around eating in vulnerable subgroups, thus leading to worse dietary habits and an overall diet of lesser quality. To the best of our knowledge, the impact that the COVID-19–related early lockdown period has had on dietary habits and on food security has not been yet documented.
The objective of this study was therefore to examine the impact of the COVID-19 early lockdown and related mitigating measures on dietary habits and food security status of adults from the province of Quebec, Canada. For that purpose, we used longitudinal data from the NutriQuébec ongoing cohort study, in which information on dietary intake and food security was obtained prior to and during the early phase of the COVID-19–related lockdown. We hypothesized that overall diet quality worsened and prevalence of food insecurity increased during the COVID-19 early lockdown period. In exploratory analyses, we explored changes in diet quality among different sociodemographic subgroups.
Methods
Study design and recruitment
NutriQuébec is an open cohort that initiated recruitment in June 2019, and which will continue over the next several years (10). Its overarching aim is to provide longitudinal data for the evaluation of the Government Policy on Health Prevention (Politique gouvernementale de prévention en santé – PGPS) and its related action plan on eating and other lifestyle behaviors among adults living in the province of Quebec, Canada. A multimedia campaign, based on a needs-assessment study (11, 12), was initiated in June 2019 to reach the target population—that is, adults aged ≥18 y with a residential address in the province of Quebec. More specifically, television, radio, and print interviews are solicited periodically. The project is advertised on social networks, including on the NutriQuébec Facebook page. Leading figures in the area of food and health are also promoting the project on various media platforms. E-mail lists from Université Laval, other universities in Quebec, community centers, health institutions, and businesses are also used to promote recruitment. All recruitment strategies invite individuals interested in the study to visit the NutriQuébec website for more information and to register. The target sample size is 20,000 adults living in Quebec based on a nonprobabilistic sampling strategy. The only exclusion criteria are not being able to read and understand French or English, not having access to the internet (with a phone, tablet, or computer), not having an active e-mail address, and living outside of the province of Quebec. The NutriQuébec project has been approved by the Ethics Board of Université Laval (2018–042 phase 2 A6-R1/09–04–2020). This substudy on COVID-19 ran from 15 April to 12 May 2020.
Questionnaires
Personal characteristics
Participants were asked to report on ethnicity, sex and gender, body weight, household composition (e.g., type of family, number of children, etc.), main occupation, education, and annual household income. Questions were taken from the Canadian Community Health Survey (CCHS) (13), the Quebec Population Health Survey (14), the Canadian Health Measures Survey (15), and the Canada population census (16). All questions have been pre-tested in French and English. For the purpose of the present analyses, sociodemographic characteristics considered were those provided at the baseline time point.
Dietary habits
Dietary habits were assessed using a validated self-administered and automated web-based 24-h dietary recall (R24W) adapted for use on a phone, tablet, and a computer (17, 18, 19, 20, 21, 22). Briefly, the R24W is inspired by the automated multiple-pass method (23) and allows participants to select foods and beverages consumed the day before, by browsing through a structured list of foods or by using a search engine. The R24W includes additional questions about 1) factors that influence nutritional needs (age, sex, pregnancy, and breastfeeding), 2) the level of representativeness of the day’s diet compared with the usual diet, and 3) the consumption of natural health products, vitamins, and mineral supplements. The R24W also includes questions on the context of the meal or snack (time, place, presence of others, and use of electronic devices during the meal), which allows, among other things, the calculation of the number of meals or snacks consumed outside of home. Nutrient intakes were calculated using the most recent Canadian Nutrient File (2015). At recruitment as well as during the COVID-19 early lockdown period, participants were invited by e-mail to complete the R24W on 3 unannounced days (1 weekend day and 2 weekdays) selected randomly by a computer algorithm over a 21- to 30-d period. Participants had until midnight to complete each 24-h dietary recall. The proportion of weekend days during which dietary intake data were collected among participants was similar between the baseline (43.6%) and the COVID-19 (44.6%) time points. Diet quality was assessed using the Healthy Eating Index (HEI)–2015, which measures adherence to recommendations in the 2015–2020 Dietary Guidelines for Americans (24). Data from all recalls at each time point in the study were used for that purpose. The subscores for each component are described in Supplemental Table 1. The total HEI-2015 ranges from 0 to 100, with a value of 100 reflecting perfect adherence to the 2015 dietary guidelines and, hence, optimal diet quality according to these recommendations.
Food insecurity
Household food-security status was assessed in a stand-alone questionnaire that was completed within the 30-d participation window at both time points. Questions were from the CCHS (13), which have been pre-tested in both French and English. The food-security status of the household was determined as described in the Supplemental Methods 1 and Supplemental Table 2. Food insecurity included the “moderate” and “severe” food-insecure categories (13).
Other questionnaires
A health status questionnaire included questions on general health, self-reported height and weight, known presence of high cholesterol and/or high blood pressure and known chronic conditions, use of primary health care services, changes made to improve health, and social provisions (13, 14). The physical activity questionnaire included questions on screen time, active transportation, and work and leisure activities (10). Minutes of vigorous physical activity were calculated as proposed in Wareham et al. (25).
Statistical analyses
To mitigate the impact of within-individual random errors related to dietary intake assessment using 24-h recalls, regression calibrations based on the National Cancer Institute (NCI) method (26, 27) were used while stratifying data by period of data collection (baseline and COVID-19 period). More information on the calibration procedures is presented in Supplemental Methods 2. Prespecified primary outcomes were changes in HEI-2015 and in food-security status during the COVID-19–related early lockdown compared with baseline. Prespecified secondary outcomes were changes in NCI-modeled nutrient intake and food consumption.
Changes in the HEI-2015 and its components were assessed using linear mixed regression models, with random intercept for participants and correlated residuals between the baseline and the COVID-19 lockdown. The covariance structure SP(POW) was used to consider the different lag time between the baseline and COVID-19 period among participants. Mixed models included calibration weights based on recent estimates of provincial sociodemographic proportions (sex, age, census metropolitan area, and education) to increase the generalizability of the results to the Quebec adult target population (Supplemental Table 3). Models were also adjusted for sex, age, census metropolitan area, occupation, marital status, education, smoking, alcohol intake, cannabis use, dietary supplement use, physical activity, screen time, presence of chronic disease, and presence of high cholesterol and/or high blood pressure to address confounding and selection bias. Details on how variables were selected to address confounding and selection bias are provided in Supplemental Methods 3. Under the missing-at-random assumptions, missing data were imputed 30 times by chained equations (fully conditional specification) as described in Supplemental Methods 4. The mixed models’ residuals normality was confirmed by visual inspection of normal QQ plots. In sensitivity analyses, a fixed effect reflecting the time lapse between the baseline measure and the measure taken during the COVID-19 lockdown (in number of calendar days) was introduced in the mixed models to adjust for the potential confounding effect of seasonal variations in diet intake. Exploratory analyses were undertaken to examine changes in diet quality among different sociodemographic subgroups using proper multiplicative terms in the models. Because these analyses were exploratory and descriptive in nature, models only included calibration weights and were not adjusted for other covariables.
Change in food insecurity (other primary outcome) was assessed using generalized linear mixed regression models with inverse-probability weighting (nonresponse weighting considering the probability of participation in the substudy) to simultaneously address confounding and selection bias. This approach was justified by the fact that the prevalence of food insecurity was very low both at baseline and during the COVID-19 lockdown. Details of the models are provided in Supplemental Methods 5. All analyses were performed in SAS Studio v3.8 (SAS Institute) and R (v3.6.2) (R Foundation for Statistical Computing). Examples of models used are provided in Supplemental Methods 6.
Results
Participants in NutriQuébec registered in waves, with peaks in August 2019 (23% of participants) and January/February 2020 (57% of participants) after specific promotion efforts. As of 1 March 2020, 2495 participants had registered to NutriQuébec and were eligible for the COVID-19 substudy. Participants who first registered and who had completed questionnaires after 22 March 2020 were not eligible because this is when most industries (including restaurants) were shut down by public health authorities in the province of Quebec. The time difference between the baseline and the COVID-19 data-collection periods was ∼3 mo (median: 88 d; IQR: 77–237 d). Among all eligible participants, 853 participants completed the R24W at least on 1 occasion and 922 completed the food-security questionnaire during the COVID-19–related early lockdown. Table 1 presents the sociodemographic characteristics at baseline of all eligible participants, those who did not participate in the COVID-19 substudy, and the 853 participants included in the analysis of the change in HEI-2015. Participants in this substudy were, in general, representative of all eligible subjects and of nonparticipants for sex, BMI, smoking, census metropolitan area, education, income, marital status, screen time, and vigorous physical activity. On the other hand, participants were older and hence more likely to be retired than nonparticipants. They also had a higher HEI-2015 and were slightly more likely to use dietary supplements and to have risk factors and chronic diseases than were nonparticipants. Although similar trends and distributions were observed in the subsample (n = 922) used for the analysis of the change in food insecurity, the unadjusted prevalence of food insecurity was lower among participants than among nonparticipants (Supplemental Table 4). After application of calibration weights (Table 1 and Supplemental Table 4), the study population included 50% women and sociodemographic characteristics were consistent with adults living in the province of Quebec with regard to age, educational level, and area of residence.
TABLE 1.
Baseline sociodemographic characteristics of all eligible participants in NutriQuébec, those who did not participate, and those who participated, as well as characteristics of participants after calibration weighting1
| Variable | All eligible (n = 2495), raw n (%) | Did not participate (n = 1642), raw n (%) | Participated (n = 853),raw n(%) | Participants (n = 853), weighted n(%) |
|---|---|---|---|---|
| Sex | ||||
| Female | 2147 (86.1) | 1403 (85.4) | 744 (87.2) | 427 (50.1) |
| Male | 348 (13.9) | 239 (14.6) | 109 (12.8) | 426 (49.9) |
| Age | ||||
| 18–29 y | 357 (14.3) | 263 (16.0) | 94 (11.0) | 154 (18.0) |
| 30–49 y | 881 (35.3) | 660 (40.2) | 221 (25.9) | 272 (31.9) |
| 50–69 y | 1062 (42.6) | 614 (37.4) | 448 (52.5) | 288 (33.8) |
| ≥70 y | 195 (7.8) | 105 (6.4) | 90 (10.6) | 139 (16.2) |
| BMI (kg/m2) | ||||
| Normal weight, <25 | 1291 (51.7) | 847 (51.6) | 444 (52.0) | 383 (45.0) |
| Overweight, 25.0–29.9 | 707 (28.3) | 467 (28.4) | 240 (28.2) | 261 (30.6) |
| Obese, ≥30 | 497 (19.9) | 328 (20.0) | 169 (19.8) | 209 (24.5) |
| Smoking | ||||
| Never | 1608 (64.5) | 1074 (65.4) | 534 (62.6) | 525 (61.6) |
| Former | 759 (30.4) | 475 (28.9) | 284 (33.3) | 280 (32.8) |
| Current | 128 (5.1) | 93 (5.7) | 35 (4.1) | 48 (5.6) |
| Census metropolitan area | ||||
| Quebec | 633 (25.4) | 400 (24.4) | 233 (27.3) | 84 (9.8) |
| Montreal | 978 (39.2) | 636 (38.7) | 342 (40.1) | 431 (50.5) |
| Other | 884 (35.4) | 606 (36.9) | 278 (32.6) | 338 (39.7) |
| Education | ||||
| Trade school, high school, or no diploma | 362 (14.5) | 236 (14.4) | 126 (14.7) | 444 (52.0) |
| CEGEP | 576 (23.1) | 385 (23.5) | 191 (22.4) | 157 (18.4) |
| University | 1558 (62.4) | 1021 (62.2) | 537 (62.9) | 253 (29.6) |
| Household income | ||||
| ≤29,999 $CAD | 195 (7.8) | 137 (8.3) | 58 (6.8) | 82 (9.6) |
| 30,000–59,999 $CAD | 580 (23.2) | 379 (23.1) | 201 (23.6) | 261 (30.6) |
| 60,000–99,999 $CAD | 734 (29.4) | 474 (28.9) | 260 (30.5) | 280 (32.9) |
| ≥100,000 $CAD or more | 985 (39.5) | 652 (39.7) | 333 (39.1) | 230 (26.9) |
| Occupation | ||||
| Full-time worker | 1203 (48.2) | 864 (52.6) | 339 (39.8) | 359 (42.1) |
| Part-time worker | 189 (7.6) | 125 (7.6) | 64 (7.5) | 49 (5.8) |
| Student | 190 (7.6) | 136 (8.3) | 54 (6.4) | 78 (9.2) |
| Retired | 738 (29.6) | 389 (23.7) | 348 (40.8) | 295 (34.6) |
| Other | 175 (7.0) | 128 (7.8) | 47 (5.5) | 71 (8.3) |
| Marital status | ||||
| Married | 803 (32.2) | 500 (30.4) | 303 (35.6) | 292 (34.2) |
| De facto union | 911 (36.5) | 617 (37.6) | 294 (34.5) | 284 (33.3) |
| Widower, separated, divorced | 295 (11.8) | 188 (11.5) | 107 (12.5) | 102 (12.0) |
| Single | 486 (19.5) | 337 (20.5) | 149 (17.5) | 175 (20.5) |
| Use of dietary supplements | ||||
| No | 1229 (49.3) | 861 (52.4) | 368 (43.2) | 398 (46.7) |
| Yes | 1266 (50.7) | 781 (47.6) | 485 (56.8) | 455 (53.3) |
| Risk factors | ||||
| No risk factor | 2018 (80.9) | 1362 (83.0) | 656 (76.9) | 608 (71.3) |
| High cholesterol or high blood pressure | 369 (14.8) | 221 (13.4) | 148 (17.4) | 154 (18.1) |
| High cholesterol and high blood pressure | 108 (4.3) | 59 (3.6) | 49 (5.7) | 90 (10.6) |
| Chronic diseases | ||||
| No | 2154 (86.3) | 1441 (87.8) | 713 (83.6) | 693 (81.3) |
| Yes (cancer, heart disease, stroke, diabetes) | 341 (13.7) | 201 (12.2) | 140 (16.4) | 160 (18.7) |
| Screen time2 | ||||
| <3.0 h/d | 552 (22.1) | 339 (20.6) | 213 (25.0) | 205 (24.1) |
| 3.0–5.5 h/d | 643 (25.8) | 424 (25.8) | 219 (25.7) | 203 (23.8) |
| 5.6–7.5 h/d | 626 (25.1) | 412 (25.1) | 214 (25.1) | 192 (22.5) |
| ≥7.6 h/d | 673 (27.0) | 467 (28.5) | 206 (24.2) | 253 (29.7) |
| Vigorous physical activity3 | ||||
| <0.5 h/wk | 787 (31.6) | 518 (31.5) | 270 (31.6) | 285 (33.4) |
| 0.5–2.0 h/wk | 499 (20.0) | 326 (19.8) | 173 (20.3) | 185 (21.7) |
| >2.0 h/wk | 1209 (48.5) | 799 (48.7) | 410 (48.1) | 383 (44.9) |
| HEI-2015,4 points (/100) | 67.0 ± 15.2 | 66.4 ± 16.2 | 68.3 ± 12.9 | 64.4 ± 15.9 |
Data are specific to the HEI-2015 outcome. Weighted data: calibration based on recent provincial sociodemographic characteristics (sex, age, census metropolitan area, and education). CAD, Canadian dollars; CEGEP, Collège d’Enseignement Général et Professionnel; HEI-2015, Healthy Eating Index 2015; NCI, National Cancer Institute.
Quartiles of screen time.
Tertiles of vigorous physical activity.
Values are means ± SDs. These means are not calibrated for within-individual random errors using the NCI method.
The mean HEI-2015 at baseline was 69.0 points (95% CI: 66.8, 71.2 points). As shown in Figure 1, there was a 1.1-point increase in the HEI-2015 during the COVID-19 early lockdown (95% CI: 0.6, 1.5), which was attributable to small but significant increases in the following components: whole grains, greens and beans, refined grains (reduced consumption), total vegetables, total dairy, seafood and plant proteins, added sugar (reduced consumption), and total proteins. There was no change in the saturated fat component and negative changes in the whole fruits, sodium (increased consumption), fatty acids, and total fruits components of the HEI-2015. Changes in each component are presented in a radar plot in Supplemental Figure 1. Mean ± SEM energy intake at baseline (2356 ± 51 kcal) decreased by −68 kcal (95% CI: −90, −45 kcal) during the COVID-19 early lockdown. There was no change in alcohol intake and in self-reported body weight (data not shown). In sensitivity analyses, the mean change in HEI-2015 was unchanged after adjustment for the time lapse between the baseline measure and the measure taken during the COVID-19 lockdown (adjusted change in HEI-2015: +1.1 point; 95% CI: 0.5, 1.6 points).
FIGURE 1.

Changein HEI-2015 and in individual components of the HEI-2015 in adults (n = 853) from the province of Quebec during the COVID-19–related early lockdown compared with baseline values. Data are presented as absolute scores and subscores (least-square means, left panel) and as mean change estimates (least-square means, right panel) with 95% CIs. Mixed models adjusted for sex, age, and census metropolitan areas, occupation, marital status, education, smoking, alcohol intake, cannabis use, supplement use, vigorous physical activity, screen time, presence of chronic diseases, and presence of high blood cholesterol, and/or hypertension to address confounding and selection bias. Analyses were also calibrated for sociodemographic characteristics (see Methods). Data on the HEI-2015 and its components were modeled for within-individual random errors related to dietary intake assessment using 24-h recalls based on the NCI method (see Methods). COVID-19, coronavirus disease 2019; HEI-2015, Healthy Eating Index 2015; NCI, National Cancer Institute.
Figure 2 shows results from the exploratory analyses of the change in HEI-2015 according to specific sociodemographic characteristics. Because of their exploratory nature, data presented are unadjusted for covariables used in the analysis of the main outcome. This is why the mean absolute HEI-2015 values are slightly higher than data shown in Figure 1. None of the subgroups showed reductions in the HEI-2015 during the COVID-19–related early lockdown compared with baseline values. Subgroups showing particularly important increases in the HEI-2015 were participants aged 18–29 y (+3.6 points; 95% CI: 2.4, 4.7 points), participants with lower education (+1.9 points; 95% CI: 1.3, 2.6 points), and participants with obesity (+3.8 points; 95% CI: 2.7, 4.8 points).
FIGURE 2.

Exploratory analyses of change in the HEI-2015 during COVID-19 among various subgroups of the Quebec adult population (n = 853). Data are presented as mean change estimates (95% CIs) in each subgroup between the COVID-19 early lockdown (April–May 2020) and baseline (June 2019–March 2020). These are a posteriori descriptive analyses and therefore changes within each subgroup must be interpreted with caution. Each model was adjusted using calibration weights and included the terms reflecting the multiplicative interaction (P-interaction) between time point and the sociodemographic variable of interest. Because of their exploratory nature, data presented are unadjusted for covariables used in the analysis of the main outcome. This is why mean absolute HEI-2015 values are slightly higher than data shown in Figure 1. CEGEP is a technical college institution specific to the Quebec educational system. CEGEP, Collège d’Enseignement Général et Professionnel; COVID-19, coronavirus disease 2019; HEI-2015, Healthy Eating Index 2015; CMA, Census metropolitan area.
Further exploratory analyses revealed that the proportion of all meals consumed outside of home decreased from 21.2% at baseline to 3.6% during the COVID-19 early lockdown ( Figure 3). The proportions of lunches (33.3% to 6.7%) and snacks (24.9% to 5.4%) consumed outside of home showed the greatest reduction during the COVID-19 early lockdown.
FIGURE 3.
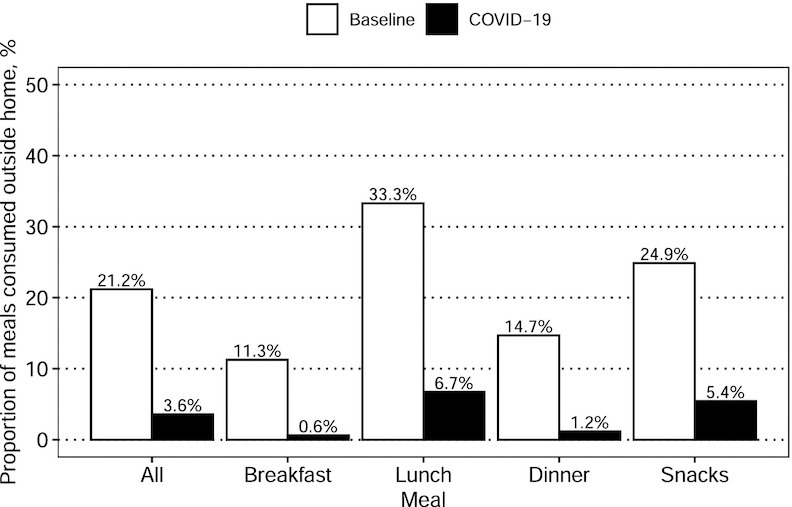
Proportion of meals consumed outside of home prior to (June 2019–March 2020) and during (April–May 2020) the COVID-19 early lockdown in adults from the province of Quebec (n = 853). The ratio of eating-out occasions was calculated as the population mean number of meals eaten outside of home divided by the population mean total number of meals, using data from all 24-h recalls among all individuals at each time point in the study (see Methods). Ratios were weighted using the calibration weights for sociodemographic characteristics, but analyses were not further adjusted because of their descriptive and hypothesis-generating nature. COVID-19, coronavirus disease 2019.
The second primary outcome of this study was the change in food-security status during the COVID-19 early lockdown. As shown in Figure 4, the prevalence of food insecurity at baseline was low (3.8% after calibration for sociodemographic characteristics and after accounting for participation bias). The prevalence of food insecurity was reduced to 1.0% during the COVID-19 early lockdown (prevalence ratio: 0.27; 95% CI: 0.08, 0.94).
FIGURE 4.

Prevalence of food insecurity in adults (n = 922) from the province of Quebec before and during the COVID-19 early lockdown (left panel) and difference between the 2 time points, presented as prevalence ratios (right panel). Food insecurity includes participants in the moderately food-insecure and severely food-insecure categories of the definition proposed by Statistics Canada (Supplemental Methods 1). In the first model (crude) data are unadjusted. In the second model (calibration) data are weighted for sociodemographic characteristics (sex, age, census metropolitan area, and education) to increase the generalizability of the results to the Quebec adult target population. The third model (calibration + nonresponse) further adjusts for the probability of participation in the substudy, hence addressing participation bias (see Methods and Supplemental Methods 1 for details). COVID-19, coronavirus disease 2019.
Discussion
A number of surveys in Canada and in Quebec as well as elsewhere around the world have pointed to qualitatively important effects of the COVID-19–related early lockdown on the dietary habits of populations. For example, in a survey of 1000 adults in the province of Quebec conducted around 20 April 2020, two-thirds of participants indicated that they were cooking meals at home more often during than before the peak home-confinement period of the COVID-19 lockdown (28). Yet, data from other surveys have suggested that alcohol and fast-food consumption may have increased during the early phases of the COVID-19 lockdown in subgroups of the population (29). These results must be interpreted with caution because they are based on nonscientific, non–peer-reviewed surveys and reflect self-perceived dietary changes, not dietary changes per se. Data from the present study suggest that overall diet quality slightly improved among adults during the early lockdown related to COVID-19 in Quebec. Data also indicated that the low prevalence of food insecurity in this cohort was further reduced during the early lockdown, although it is not possible to accurately quantify this change since the CIs are very wide.
The increase in HEI-2015 and hence in diet quality during the early lockdown related to COVID-19 refuted our hypothesis. The small but significant increase in HEI-2015 was attributable to both favorable and unfavorable changes in its components. Favorable changes included small increases in the consumption of whole grains, plant-based foods (vegetables, greens and beans, and seafood and plant protein) and dairy and small reductions in the consumption of refined grains and added sugar. Consumption of fruits may have declined and intake of sodium may have increased during the same period, thus blunting to some extent the favorable changes in other HEI-2015 components. Society’s lockdown and social-distancing and home-confinement mitigation measures during the early phase of the COVID-19 pandemic have led to important reductions in the frequency of eating out according to exploratory analyses. We hypothesize that eating out less often may explain, at least to some extent, the small improvement in overall diet during the early lockdown phase of the COVID-19 pandemic in this sample. Indeed, eating outside of home has been associated with a higher total energy intake and more energy from fat according to a recent systematic review of nationally representative or large cohort studies (30). Inversely, eating home-cooked meals more often has been associated with greater adherence to the Dietary Approach to Stop Hypertension (DASH) and Mediterranean diets, greater fruit and vegetable intakes, and higher plasma vitamin C in a cohort of 11,396 adults from the United Kingdom (5). Eating more often at home is not necessarily synonymous with cooking more often. Thus, the hypothesis that eating out less frequently may partly explain the increase in overall diet quality during the early lockdown related to COVID-19 needs to be confirmed.
Exploratory analyses revealed that there was no deterioration in overall diet quality in any of the sociodemographic groups investigated, and that groups known to be more susceptible to having lower diet quality scores, such as younger individuals, those with a lower education, and those with obesity, showed relatively important increases in diet quality during the COVID-19 early lockdown. We stress that these observations are based on descriptive analyses that must be interpreted with caution and that need to be confirmed by other studies.
Based on 2017–2018 CCHS data, 8.8% of households in Quebec are moderately or severely food insecure (31). Using the same definition, food insecurity in this cohort was not as prevalent at baseline in our sample (3.8%). Efforts to calibrate data according to population-representative sociodemographics and to account for participation bias could not completely attenuate these biases. Contrary to our hypothesis, food insecurity was slightly reduced during the COVID-19–related early lockdown. A web-based survey by the Institut National de Santé Publique du Québec that has sampled 1000 Quebec adults daily during the first month of the pandemic showed that the prevalence of food insecurity during the first week of April was at least twice the prevalence before the pandemic (32). The survey also showed a reduction in the prevalence of food insecurity between the beginning of April and mid-May 2020, as the COVID-19 mitigating measures were put in place (32). It is stressed that the definition of food insecurity in these surveys differed from the one used in CCHS and in the current study. Further studies are warranted to assess how lockdowns such as the one related to COVID-19 impact food insecurity in more vulnerable populations.
Strength and weaknesses need to be addressed. Although relatively small, the sample size provided reliable population-based estimates of diet quality. An important strength of this analysis relates to the repeated measures of dietary intake using a validated 24-h recall both before and during the COVID-19 early lockdown. Taking advantage of these repeated measures allowed the modeling of the data for within-individual variations/errors in dietary intake. Data collected using 24-h recalls are subject to systematic errors, although to a lesser extent than other self-reported methods such as FFQs (33). Although participants in this substudy were generally representative of all participants in NutriQuébec, using calibration weights and accounting for confounding and for participation bias most likely did not completely eliminate the general bias of participants towards health in this substudy. Whether a lockdown such as the one related to COVID-19 affects diet quality in more vulnerable populations needs to be investigated further. Despite not being supported by results from sensitivity analyses, the possibility remains that the small changes in diet quality and in food insecurity during the COVID-19 early lockdown are due, at least partly, to seasonal variation in diet intake in this population.
In conclusion, data from this longitudinal observational study suggest that overall diet quality, as measured by an index that reflects adherence to the 2015–2020 Dietary Guidelines for Americans, slightly increased during the early phase of the COVID-19–related lockdown in this sample of adults from the province of Quebec. Food insecurity was also slightly reduced. These results may be generalizable only to relatively healthy populations. The impact of the COVID-19–related early lockdown on diet quality and on food insecurity in more vulnerable populations has yet to be documented.
Acknowledgments
The authors thank the Fonds de recherche du Québec - santé (FRQS)-funded Cardiometabolic Health, Diabetes, and Obesity Research Network (CMDO) for their financial support for the needs-assessment study that preceded the undertaking of NutriQuébec and the NutriQuébec website creation. The authors thank Serge Hercberg and the NutriNet-Santé Study team in France for their support and for sharing their expertise in the process leading to the development of the NutriQuébec project. The contribution and support of all members of the Scientific Committee of NutriQuébec are essential to the success of this project: Lise Gauvin (University of Montreal), Didier Garriguet (Statistics Canada), David Buckeridge (McGill University). Finally, the authors thank the staff of PULSAR at Université Laval for their support and expertise regarding data security and management.
The authors’ responsibilities were as follows—BL, AL, CL, AB-G, SD, SL, and CP: designed the research; CL, AL, MK, and MC: conducted the research; BL and DB: built the analytical plans; DB: performed statistical analysis; BL: drafted the manuscript and had primary responsibility for final content. BL, AB-G, SD, and SL: obtained funding for the project; and all authors: read and approved the final manuscript. The authors report no conflicts of interest.
Data Availability
Data described in the manuscript, code book, and analytic codes will be made available upon request pending application and approval from the authors as well as the funding body.
Footnotes
This work was supported by and developed for the Québec government (2017–2021). The funder had no role in generating the hypothesis statements, in data collection, in data analysis, or in interpretation of the results presented in this paper.
Supplemental Figure 1, Supplemental Tables 1–4, and Supplemental Methods 1–6 are available from the “Supplementary data” link in the online posting of the article and from the same link in the online table of contents at https://academic.oup.com/ajcn/.
BL and DB contributed equally to the preparation of this paper.
SUPPORTING INFORMATION
nqaa363_Supplemental_Files
References
- 1.Nagata JM, Seligman HK, Weiser SD. Perspective: the convergence of coronavirus disease 2019 (COVID-19) and food insecurity in the United States. Adv Nutr. 2020 doi: 10.1093/advances/nmaa126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.High-Level Panel of Experts on Food Security and nutrition (HLPE). Impact of COVID-19 on food security and nutrition (FSN). Version current 24 March 2020; [Internet]. Available from: http://www.fao.org/fileadmin/user_upload/hlpe/COVID-19/HLPE._Impact_of_COVID-19_on_FSN_-_2020-03-24_-_EN4.pdf (accessed 13 July 2020).
- 3.Wolfson JA, Bleich SN. Is cooking at home associated with better diet quality or weight-loss intention? Public Health Nutr. 2015;18(8):1397–1406. doi: 10.1017/S1368980014001943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wolfson JA, Leung CW, Richardson CR. More frequent cooking at home is associated with higher Healthy Eating Index-2015 score. Public Health Nutr. 2020;23:2384. doi: 10.1017/S1368980019003549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mills S, Brown H, Wrieden W, White M, Adams J. Frequency of eating home cooked meals and potential benefits for diet and health: cross-sectional analysis of a population-based cohort study. Int J Behav Nutr Phys Act. 2017;14(1):109. doi: 10.1186/s12966-017-0567-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Clifford Astbury C, Penney TL, Adams J. Comparison of individuals with low versus high consumption of home-prepared food in a group with universally high dietary quality: a cross-sectional analysis of the UK National Diet & Nutrition Survey (2008–2016) Int J Behav Nutr Phys Act. 2019;16(1):9. doi: 10.1186/s12966-019-0768-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hunter. America gets cooking. Version current 9 April 2020; [Internet]. Available from: https://www.hunterpr.com/foodstudy_coronavirus/ (accessed 13 July 2020).
- 8.International Food Information Council. Impact on food purchasing, eating behaviors, and perceptions of food safety. Version current 14 April 2020; [Internet]. Available from: https://foodinsight.org/consumer-survey-covid-19s-impact-on-food-purchasing/ (accessed 13 July 2020).
- 9.Agri-Food Analytics Lab. New survey on COVID-19 grocery shopping suggests 95% of Canadians are taking new precautions when grocery shopping now. Version current 4 May 2020; [Internet]. Available from: https://cdn.dal.ca/content/dam/dalhousie/pdf/sites/agri-food/COVID%20Grocery%20experience%20Mini-Report%20(May%202020)%20EN.pdf (accessed 13 July 2020).
- 10.Lapointe A, Laramée C, Bélanger-Gravel A, Buckeridge D, Desroches S, Garriguet D, Gauvin L, Lemieux S, Plante C, Lamarche B. NutriQuébec: a unique web-based prospective cohort study to monitor the population’s eating and other lifestyle behaviors in the province of Québec. BMJ Open. 2020;10:e039889. doi: 10.1136/bmjopen-2020-039889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cote M, Lapointe A, Laramee C, Lemieux S, Desroches S, Belanger-Gravel A, Lamarche B. Beliefs related to participation in a large web-based prospective survey on diet and health among individuals with a low socioeconomic status: qualitative study. JMIR Form Res. 2019;3(4):e13854. doi: 10.2196/13854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cote M, Harrison S, Lapointe A, Laramee C, Desroches S, Lemieux S, Lamarche B, Belanger-Gravel A. A cross-sectional survey examining motivation and beliefs to participating in a web-based prospective cohort study on nutrition and health among individuals with a low socioeconomic status. BMC Public Health. 2020;20(1):348. doi: 10.1186/s12889-020-08467-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Statistics Canada. Canadian Community Health Survey (CCHS). Version current 27 November 2019; [Internet]. Available from: http://www23.statcan.gc.ca/imdb/p3Instr.pl?Function=getInstrumentList&Item_Id=260675&UL=AV (accessed 13 July 2020).
- 14.Institut de la Statistique du Québec. Québec Population Health Survey (QPHS). 2008; and 2014–2015. Version current 2015 [Internet]. Available from: http://www.stat.gouv.qc.ca/enquetes/fiche_enquete_an.html#171 (accessed 13 July 2020).
- 15.Statistics Canada. Canadian Health Measures Survey. Version current 4 March 2020; [Internet]. Available from: https://www.statcan.gc.ca/eng/survey/household/5071 (accessed 13 July 2020).
- 16.Statistics Canada. Census program. Version current. 9 June 2020; [Internet]. Available from: https://www12.statcan.gc.ca/census-recensement/index-eng.cfm (accessed 13 July 2020).
- 17.Lafreniere J, Laramee C, Robitaille J, Lamarche B, Lemieux S. Assessing the relative validity of a new, web-based, self-administered 24 h dietary recall in a French-Canadian population. Public Health Nutr. 2018;21(15):2744–2752. doi: 10.1017/S1368980018001611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jacques S, Lemieux S, Lamarche B, Laramee C, Corneau L, Lapointe A, Tessier-Grenier M, Robitaille J. Development of a web-based 24-h dietary recall for a French-Canadian population. Nutrients. 2016;8(11):724. doi: 10.3390/nu8110724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lafreniere J, Laramee C, Robitaille J, Lamarche B, Lemieux S. Relative validity of a web-based, self-administered, 24-h dietary recall to evaluate adherence to Canadian dietary guidelines. Nutrition. 2019;57:252–256. doi: 10.1016/j.nut.2018.04.016. [DOI] [PubMed] [Google Scholar]
- 20.Savard C, Lemieux S, Lafreniere J, Laramee C, Robitaille J, Morisset AS. Validation of a self-administered web-based 24-hour dietary recall among pregnant women. BMC Pregnancy Childbirth. 2018;18(1):112. doi: 10.1186/s12884-018-1741-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lafrenière J, Couillard C, Lamarche B, Laramée C, Vohl M, Lemieux S. Associations between self-reported vegetable and fruit intake assessed with a new web-based 24-hour dietary recall and serum carotenoids in free living adults: a relative validation study. J Nutr Sci. 2019;8:e26. doi: 10.1017/jns.2019.23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lafrenière J, Lamarche B, Laramée C, Robitaille J, Lemieux S. Validation of a newly automated web-based 24-hour dietary recall using fully controlled feeding studies. BMC Nutr. 2017;3:34. doi: 10.1186/s40795-017-0153-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Moshfegh AJ, Rhodes DG, Baer DJ, Murayi T, Clemens JC, Rumpler WV, Paul DR, Sebastian RS, Kuczynski KJ, Ingwersen LA, et al. The US Department of Agriculture automated multiple-pass method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008;88(2):324–332. doi: 10.1093/ajcn/88.2.324. [DOI] [PubMed] [Google Scholar]
- 24.Reedy J, Lerman JL, Krebs-Smith SM, Kirkpatrick SI, Pannucci TE, Wilson MM, Subar AF, Kahle LL, Tooze JA. Evaluation of the Healthy Eating Index-2015. J Acad Nutr Diet. 2018;118(9):1622–1633. doi: 10.1016/j.jand.2018.05.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wareham NJ, Jakes RW, Rennie KL, Schuit J, Mitchell J, Hennings S, Day NE. Validity and repeatability of a simple index derived from the short physical activity questionnaire used in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Public Health Nutr. 2003;6(4):407–413. doi: 10.1079/PHN2002439. [DOI] [PubMed] [Google Scholar]
- 26.Kipnis V, Midthune D, Buckman DW, Dodd KW, Guenther PM, Krebs-Smith SM, Subar AF, Tooze JA, Carroll RJ, Freedman LS. Modeling data with excess zeros and measurement error: application to evaluating relationships between episodically consumed foods and health outcomes. Biometrics. 2009;65(4):1003–1010. doi: 10.1111/j.1541-0420.2009.01223.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Tooze JA, Midthune D, Dodd KW, Freedman LS, Krebs-Smith SM, Subar AF, Guenther PM, Carroll RJ, Kipnis V. A new statistical method for estimating the usual intake of episodically consumed foods with application to their distribution. J Am Diet Assoc. 2006;106(10):1575–1587. doi: 10.1016/j.jada.2006.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Observatoire de la Consommation Responsable. Vigie Conso COVID-19. Version current 2020; [Internet]. Available from: https://ocresponsable.com/vigie-conso-covid-19/ (accessed 13 July 2020).
- 29.Statistics Canada. Canadian Perspectives Survey Series 2: monitoring the effects of COVID-19, May 2020. Version current 4 June 2020 [Internet]. Available from: https://www150.statcan.gc.ca/n1/daily-quotidien/200604/dq200604b-eng.htm?HPA=1 (accessed 13 July 2020).
- 30.Lachat C, Nago E, Verstraeten R, Roberfroid D, Van Camp J, Kolsteren P. Eating out of home and its association with dietary intake: a systematic review of the evidence. Obesity Rev. 2012;13(4):329–346. doi: 10.1111/j.1467-789X.2011.00953.x. [DOI] [PubMed] [Google Scholar]
- 31.Tarasuk V, Mitchell A. Household food insecurity in Canada 2017–2018. Version current. 2018 [Internet]. Available from: https://proof.utoronto.ca/wp-content/uploads/2020/03/Household-Food-Insecurity-in-Canada-2017-2018-Full-Reportpdf.pdf (accessed 13 July 2020). [Google Scholar]
- 32.Institut National de Santé Publique du Québec. COVID-19—pandémie et insécurité alimentaire. Version current 29 June 2020; [Internet]. Available from: https://www.inspq.qc.ca/sites/default/files/publications/3027-sondage-pandemie-insecurite-alimentaire-covid19.pdf (accessed 13 July 2020).
- 33.Freedman LS, Commins JM, Moler JE, Arab L, Baer DJ, Kipnis V, Midthune D, Moshfegh AJ, Neuhouser ML, Prentice RL, et al. Pooled results from 5 validation studies of dietary self-report instruments using recovery biomarkers for energy and protein intake. Am J Epidemiol. 2014;180(2):172–188. doi: 10.1093/aje/kwu116. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
nqaa363_Supplemental_Files
Data Availability Statement
Data described in the manuscript, code book, and analytic codes will be made available upon request pending application and approval from the authors as well as the funding body.