

Enteroscopy-assisted ERCP (E-ERCP) in patients with surgically altered anatomy usually represents a challenge even within the hands of skilled operators, with a success rate ranging from 70% to 90%.1 Management of difficult hepatolithiasis in such patients, using overtube-assisted digital cholangioscopy (DC) with laser lithotripsy, was previously reported.2 We describe here the use of electrohydraulic lithotripsy (EHL) in a similar fashion; however, this case video focuses mostly on challenges we have faced during this demanding procedure. These challenges are mainly related to the reconstructed anatomy and the procedure technique and therefore may occur in similar patients. In our case, these challenges included the sharply kinked course of the overtube after enteroscope withdrawal with challenging DC passage. In addition, the DC (which lacks the ability to insufflate air) depends on a guidewire to pass through the overtube to access the bilioenteric anastomosis; this guidewire was dislodged from the anastomosis just after passage out of the overtube. Here, we describe simple technical tips and tools that facilitated overcoming these challenges, which may be helpful in future cases.
A 60-year-old man with a history of Roux-en-Y hepaticojejunostomy for pancreaticobiliary maljunction presented with acute cholangitis in the form of jaundice and fever. Abdominal CT (Fig. 1) revealed dilated intrahepatic bile ducts with a large impacted stone. After balloon dilatation of the bilioenteric anastomosis, we attempted balloon sweeping and mechanical lithotripsy through E-ERCP (EC-L600MP7; 9.4 mm diameter, 3.2 mm working channel; Fujifilm, Tokyo, Japan); both were unsuccessful. Hence, EHL through DC (Spyscope DS II; Boston Scientific, Tokyo, Japan), assisted by the enteroscopy overtube, was chosen.
Figure 1.

Abdominal CT showing dilated intrahepatic bile ducts with a large impacted stone (yellow arrow).
After E-ERCP successfully reached the anastomosis site, cannulation with a standard ERCP cannula was achieved with selective intrahepatic insertion of a guidewire, followed by biliary cholangiogram, which revealed large impacted stones. Afterward, the enteroscope was wisely withdrawn from the overtube, leaving the guidewire behind. DC was then introduced over the guidewire through the overtube, which had a sharply kinked course (related to postsurgical reconstruction) with challenging DC passage. In contrast to the ultrathin videoscope, DC with its increased flexibility and decreased friction resistance succeeded in passage without overtube dislocation, assisted by a prolonged process (more than 7 minutes) of tube negotiation and external abdominal compression to adjust tube position (Figs. 2 and 3).
Figure 2.

Balloon-assisted overtube with a sharply kinked course and acute angulations (yellow arrows) after enteroscope withdrawal.
Figure 3.

Digital cholangioscope inside the overtube after successful passage through the sharply kinked portion.
Thereafter, while attempting to admit the DC through the bilioenteric anastomosis, the guidewire accidentally slipped out of the biliary tract, leaving the DC within the collapsed jejunum. The DC’s way was lost through the collapsed lumen because the DC was not designed primarily to insufflate air. To salvage this troublesome situation, we tried to enhance the DC’s ability to directly insufflate CO2, besides its known ability to irrigate saline solution, to regain jejunal lumen patency. A short plastic tube, simply obtained by cutting the distal 3 cm of the conducting tube of an oxygen nasal cannula, was used to directly connect the CO2 pump to the DC working channel (Figs. 4 and 5), through which CO2 was maintained under high pressure. This technique succeeded in maintaining lumen patency and allowed the DC to view the anastomosis site.
Figure 4.

Connecting the digital cholangioscope’s working channel to a CO2 pump by using a short plastic tube (yellow arrow).
Figure 5.

A, The connecting plastic tube was created simply by using an oxygen nasal cannula and scissors. B, Cutting the distal 3 cm of the conducting tube of the nasal cannula. C, Connecting it to the working channel of the digital cholangioscope.
DC direct cannulation through the anastomosis site into the bile ducts was then achieved, followed by EHL for the difficult stones (EHL AUTOLITH TOUCH; Northgate Technologies Inc, Elgin, Ill) (Figs. 6 and 7) with further fragmentation. On the next E-ERCP 1 week later (intended for mechanical lithotripsy of residual stone fragments), the cholangiogram (Fig. 8) revealed no fragments, demonstrating spontaneous passage after the previous EHL session.
Figure 6.

Electrohydraulic lithotripsy fiber outside the digital cholangioscope’s working channel.
Figure 7.

Electrohydraulic lithotripsy (EHL) fiber just before generating EHL sparks against hard stones.
Figure 8.

Biliary cholangiogram using double-balloon enteroscopy 1 week after an electrohydraulic lithotripsy session reveals no stone fragments (spontaneously passed).
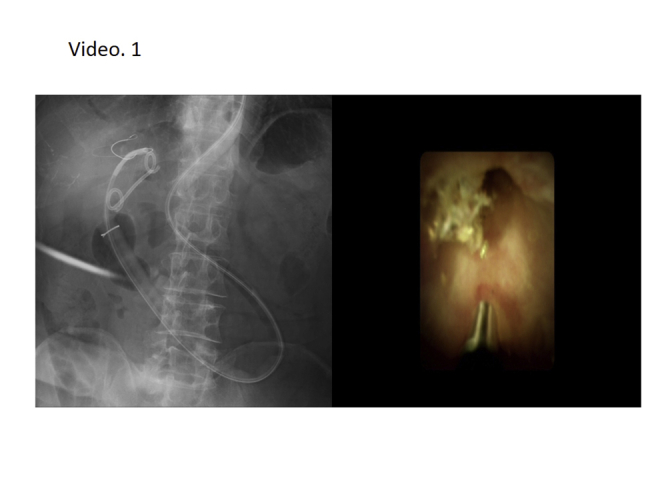
With support of such simple techniques, the challenging overtube-assisted DC and related therapeutic procedures in a patient with surgically altered anatomy were safely and effectively achieved (Video 1, available online at www.VideoGIE.org).
Disclosure
All authors disclosed no financial relationships.
Acknowledgment
This work was supported by JSPS KAKENHI grant numbers JP19K07938 (AS).
Supplementary data
Illustrates challenging points during overtube guided electrohydraulic lithotripsy for difficult biliary stones in a post-operative patient through digital cholangioscopy. Challenges faced included difficult passage through the overtube within the reconstructed anatomy and slippage of the guidewire out of the bilioenteric anastomosis with subsequent loss of the way through a collapsed lumen. Using simple techniques of prolonged abdominal compressions to adjust tube location and enhancing capabilities of digital cholangioscope to directly insufflate CO2 using simple connecting tube, have overcome these challenges.
Slide1.
References
- 1.Krutsri C., Kida M., Yamauchi H. Current status of endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy. World J Gastroenterol. 2019;25:3313–3333. doi: 10.3748/wjg.v25.i26.3313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cho J., Buxbaum J., Sahakian A.B. Balloon overtube-assisted cholangioscopy and laser lithotripsy of large bile duct stones. VideoGIE. 2018;3:217–219. doi: 10.1016/j.vgie.2018.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Illustrates challenging points during overtube guided electrohydraulic lithotripsy for difficult biliary stones in a post-operative patient through digital cholangioscopy. Challenges faced included difficult passage through the overtube within the reconstructed anatomy and slippage of the guidewire out of the bilioenteric anastomosis with subsequent loss of the way through a collapsed lumen. Using simple techniques of prolonged abdominal compressions to adjust tube location and enhancing capabilities of digital cholangioscope to directly insufflate CO2 using simple connecting tube, have overcome these challenges.