

Abstract
Background:
Black and Latina transgender women (BLTW) face significant HIV disparities with estimated HIV prevalence up to 50% and annual incidence rates as high as 2.8 per 100 person-years. However, few studies have evaluated the acceptability and uptake of high-impact HIV prevention interventions among BLTW.
Setting:
Data collection took place in Baltimore, MD and Washington, DC from May 2015-May 2017.
Methods:
This mixed methods study included quantitative interviewer-administered surveys, key informant interviews, and focus group discussions. Rapid HIV testing followed each survey. Logistic regression models tested associations between legal gender affirmation (i.e., desired name and gender marker on identity documents), transgender pride, history of exchange sex, HIV risk perception, and willingness to take pre-exposure prophylaxis (PrEP). Transcripts of qualitative data were coded to identify common themes related to engagement in HIV prevention.
Results:
Among 201 BLTW, 56% tested HIV-positive and 87% had heard of PrEP. Only 18% who had heard of PrEP had ever taken it. Of the 72 self-reported HIV-negative or status-unknown BLTW who had never taken PrEP, 75% were willing to take it. In multivariable analyses, history of exchange sex was associated with willingness to take PrEP, whereas greater HIV knowledge and transgender pride were associated with lower likelihood of willingness to take PrEP. Concern about drug interactions with hormone therapy was the most frequently reported barrier to PrEP uptake.
Conclusion:
Noting the disconnect between PrEP willingness and uptake among BLTW, HIV prevention programs could bridge this gap by responding to identified access barriers and incorporating community-derived strategies.
Keywords: transgender women, pre-exposure prophylaxis, HIV prevention
Introduction
Global research demonstrate great vulnerability to HIV among transgender women, with incidence rates as high 2.8 per 100 person years.1 Black and Latina transgender women (BLTW) in the US are particularly burdened, with an HIV prevalence exceeding 50% in some studies.2 Data on newly diagnosed infections suggest ongoing risk for HIV that begins in adolescence.3,4 However, a limited number of evidence-based HIV prevention interventions have been tested with this population.5 Acceptable, accessible, and effective interventions are needed to address the HIV epidemic in this group.
Daily oral HIV pre-exposure prophylaxis (PrEP) using a combination of tenofovir and emtricitabine (TDF-FTC) has demonstrated efficacy to reduce risk of HIV acquisition by as much as 96% among cisgender (i.e., non-transgender) men who have sex with men (cis-MSM).6 Its efficacy has been confirmed among heterosexual couples7 and people who inject drugs.8 However, two studies of oral PrEP among cisgender women (cis-women) who have sex with men have produced disappointing results, with lack of efficacy attributed to low adherence (<40%) in both studies.9,10
A secondary analysis of data from the seminal iPrEX trial found no efficacy of oral PrEP among TW participants.11 Adherence was low (18%) among TW and negatively associated with use of exogenous hormone therapy. No HIV seroconversions were identified among TW in iPrEX for whom blood levels of tenofovir were consistent with taking at least four doses per week, suggesting efficacy among TW who adhere to daily TDF-FTC for PrEP. Since the US Food and Drug Administration approved oral TDF-FTC for PrEP in 2012, significant racial and gender disparities in PrEP uptake12 and adherence13 have been identified.
Addressing low uptake and adherence to this highly efficacious intervention calls for deeper examination of early aspects of the PrEP care continuum. The PrEP care continuum has been divided into three main stages: awareness, uptake, and adherence.14 Awareness includes both self-perceived HIV risk and awareness of PrEP, and uptake includes access to and initiation of PrEP. While these stages are essential to reaching the goal of PrEP adherence, they are missing important links between awareness and uptake: PrEP willingness.15 In order for individuals who are aware of PrEP to access and initiate it, they must be willing to take it.
Data on PrEP acceptability and willingness among TW are often derived from studies designed for cisgender MSM and include relatively small numbers of TW.16,17 Many of these studies fail to disaggregate findings by gender identity.17–20 TW-specific studies of PrEP are limited.5 Research in Latin America and Asia suggest high acceptability, willingness, and uptake of PrEP among TW.21–24 Findings are less promising in US-based studies, which have found low PrEP acceptability and uptake.25–27 Transgender-specific barriers to PrEP identified in qualitative studies with TW include stigma, exclusion of TW in advertising, concerns about drug interactions with feminizing hormones, and lack of research on TW and PrEP.26,28 A quantitative study of young (16–29 years old) multi-racial TW identified higher PrEP acceptability among participants who reported that providers always or sometimes met their health needs (compared with never or rarely), whereas transactional sex was associated with lower PrEP acceptability.25 These studies provide important information on PrEP among TW; however, gaps remain in research focused specifically on BLTW, who are most vulnerable to HIV.
The overall goals of the STROBE Study (Supporting Transgender Research and Opportunities in the Baltimore/DC Environment) were to identify HIV-related vulnerabilities and assess acceptability and uptake of current and future biomedical prevention interventions among transgender women of color, particularly BLTW. In this analysis, we sought to understand PrEP awareness and uptake among BLTW, as well as assess willingness to engage in current and future HIV prevention interventions, including oral PrEP, post-exposure prophylaxis (PEP), microbicides, and vaccines.
Methods
This mixed methods analysis used a sequential exploratory design.29 Qualitative data were collected first to inform development of the quantitative survey, which followed. During data analysis, we identified themes within the qualitative data that provide insight into ways stakeholders can respond to the HIV prevention needs of BLTW. Therefore, we present the quantitative findings prior to the qualitative findings in the Results section.
Eligibility
Key informants (KI) met the following eligibility criteria: age ≥18 years and ≥ 1 year of experience working or volunteering for an organization that serves the transgender community in Baltimore. All other data collection was limited to transgender women age (assigned male at birth who identified as a female/woman or transgender) age ≥15 years who identified as Black/African-American, Latina/Hispanic, or mixed race and lived in the Baltimore, MD or Washington, DC metropolitan areas.
Recruitment and Data Collection
Qualitative
Qualitative data collection was conducted in English only between May-October 2015 in Baltimore and included KI interviews, focus group discussions (FGDs), and in-depth interviews (IDIs). Potential KIs were recruited purposively through professional networks of the principal investigator and key community stakeholders. KI interviews (n=12) lasted approximately 60 minutes and occurred in private office spaces or other locations of the participants’ choosing. KI discussion topics included: community engagement approaches, sampling and recruitment methods, and perceptions of HIV risk and prevention among BLTW. KIs received $40 for participation.
Three FGDs of 3–8 participants each (n=18) were held in Baltimore. FGD participants were recruited via word-of-mouth and flyers at transgender-serving community organizations, including organizations focused on transgender youth. A trained facilitator used a semi-structured guide to lead discussions about community norms and perceptions related to HIV and prevention interventions. In addition, input on sensitive segments of the planned survey instrument (e.g., sexual behavior questions) were solicited prior to survey launch. Two IDIs were conducted with adolescents. Individual interviews were held in response to adolescent concerns about privacy risks associated with attending FGDs. These IDIs included the same topics discussed in the FGDs with a specific focus on assessing adolescent norms. FGD and IDI participants received $50. All qualitative data were audio-recorded and transcribed verbatim by a professional transcription company.
Quantitative
Recruitment began in April 2016 in Baltimore. Due to slow accrual, Washington, DC was added as a site in February 2017. Recruitment continued through May 2017 in both cities. Participants were recruited through posted flyers, social media, promotion at community events, referrals from community-based organizations and healthcare centers, and word-of-mouth. Interested individuals were screened by phone and scheduled for one-hour in-person interviewer-administered surveys in English or Spanish. The Spanish translation process for the survey has been described elsewhere.30
Informed consent processes and data collection took place in a private research office. Participants completed the survey followed by rapid oral HIV antibody screening using OraQuick ADVANCE rapid HIV-1/2 test kits. Trained data collectors provided pre- and post-test counseling, linked participants with a reactive HIV test to confirmatory testing care, and referred HIV-negative participants to PrEP providers. Participants were given the option to be tested without staying to receive results. All study participants were offered condoms, lubricant, and HIV risk reduction information. Each individual who completed study activities received a $50 Visa gift card.
Quantitative Measures
Socio-demographic variables
The survey collected race, ethnicity, educational attainment, employment status, and insurance status. Personal monthly income was collected categorically and subsequently dichotomized as above or below the 2017 Federal Poverty Line (FPL).31 Unstable housing was defined as having experienced one or more unstable housing circumstances in the prior 12 months from a list of 12 options (Supplemental Table 1). Lifetime sex exchange was defined as ever having anal, vaginal, or oral sex for money, shelter, food, drugs, or other material goods.
Psychosocial Factors
Transgender pride was assessed using a sub-scale developed and validated in the Transgender Identity Survey.32 Participants evaluated their level of agreement with eight statements (Supplemental Table 2) using a 3-point Likert scale (0–2). Scores were summed from 0–16, with higher scores reflecting increased pride (α=0.81). Legal gender affirmation was determined by asking participants the extent to which their identification documents list their desired name and gender marker. Participants who reported that neither their desired name nor gender marker were listed on any legal documents were categorized as not having legal gender affirmation.
HIV-Specific Variables
The HIV knowledge index included five multiple-choice questions about sexual risk (Supplemental Table 3).33 A summary score of correct answers was computed with higher scores representing greater knowledge. HIV risk perception was measured on a scale of 1 to 4, with 1 being no risk and 4 being high risk, using one item, “How high do you think your risk is for HIV infection?” Condomless anal sex was defined as sometimes or never using condoms for receptive or insertive anal sex in the prior 12 months. New HIV-positive test result was defined as a reactive result on the study rapid HIV test among participants who reported a negative result at their most recent prior test.
PrEP awareness was measured by asking all participants if they had ever heard of PrEP. Participants who had heard of PrEP were asked if they had ever taken PrEP (uptake); participants who had taken PrEP were then asked if they had taken PrEP within the prior 12 months. We included all participants in the denominator to ensure that we did not exclude participants living with HIV who may have taken PrEP prior to HIV infection. Participants who reported being HIV-negative and had never taken PrEP were asked if they would be willing to take it (willingness). Participants who were unwilling to take PrEP were asked reasons for unwillingness (select all) from a list of potential reasons drawn from prior literature.16,21,34–36 Participants who had taken PrEP were asked to identify experiences (select all) from a list of potential positive and negative experiences with PrEP drawn from prior literature.13,23,37
All participants were asked about PEP awareness, uptake, and willingness. For future interventions (microbicides and vaccines), participants were provided with a brief description of the intervention (Supplemental Table 4), then asked if they would be willing to use it.
Data Analysis
Qualitative
Atlas.ti (Version 7, Scientific Software Development GmbH) was used for management and analysis of transcripts. Data were coded using a priori codes from the semi-structured guides and emergent codes derived during the coding process. Two coders double-coded three transcripts and compared side-by-side to identify and reconcile inconsistences via consensus. The remaining transcripts were coded independently. Codes were then read across transcripts and grouped into emergent themes.38
Quantitative
Data were analyzed using Stata 14 (College Station, TX, USA). Descriptive frequencies were calculated for sociodemographic characteristics, stages of engagement in HIV prevention interventions, and hypothesized correlates. Bivariate logistic regression analyses were performed to identify associations between each covariate on the primary outcome of willingness to take PrEP. Each covariate that was associated with the outcome at p<0.05 in bivariate analyses was included in the multivariable logistic regression model, adjusted for age and city. We did not adjust for language in addition to city since all Spanish-speaking participants resided in DC.
The study received approval from the Johns Hopkins Institutional Review Board.
Results
Quantitative
As listed in Table 1, the 201 BLTW participants ranged in age from 19–82 years with an average age of 38 (median: 34 years). The majority identified as Black or African American (62%), and approximately one-quarter (27%) identified as Latina/Hispanic of any race. Most participants had public health insurance, as well as high levels of unemployment and poverty. Sixty-nine percent had identity documents with their desired name or gender marker, and 78% were currently taking gender-affirming hormones.
Table 1.
Participant Characteristics, N=201
| Variable | n (%) |
|---|---|
| Mean age in years | 38.2 (range: 19–82) |
| Language | |
| English | 161 (80.1) |
| Spanish | 40 (19.9) |
| Location | |
| Baltimore, MD | 55 (27.4) |
| Washington, DC | 146 (72.6) |
| Race | |
| Black/African American | 125 (62.2) |
| Multi-racial | 35 (17.4) |
| Other race | 22 (11.0) |
| Indigenous | 19 (9.5) |
| Latina/Hispanic (of any race) | 54 (26.9) |
| Health insurance | |
| Private | 16 (8.2) |
| Public | 171 (87.2) |
| Uninsured | 9 (4.6) |
| Education | |
| Less than high school | 58 (29.0) |
| High school diploma or GED | 62 (31.0) |
| Some college or vocational | 71 (35.5) |
| College degree or higher | 9 (4.5) |
| Socioeconomics | |
| Unstable housing in prior 12 mo. | 115 (57.2) |
| Income below poverty line | 144 (75.8) |
| Unemployed | 104 (51.7) |
| Current gender affirming hormone use | 156 (77.6) |
| Legal gender affirmation | |
| All documents reflect current gender | 122 (60.7) |
| All documents reflect desired name | 129 (64.2) |
| Any congruent document | 139 (69.2) |
| Condomless anal sex in prior 12 mo. | 82 (40.8) |
| History of exchange sex | 154 (78.6)* |
| HIV test in prior 12 months** | 19 (19.6) |
| HIV-positive rapid oral test result | 112 (55.7) |
| New HIV-positive test result** | 10 (10.2) |
| Scale variable (n=98)** | Median scores (IQR) |
| Transgender pride (possible range: 0–16) | 14.0 (9–16) |
| HIV risk perception (possible range: 1–4) | 3 (2–4) |
| HIV knowledge (possible range: 0–5) | 5 (4–5) |
n=196 because some participants refused to answer.
Among HIV-negative and HIV status unknown (n=98)
More than half of the participants (n=112, 56%) tested positive for HIV and 90% of those who tested positive (n=102) were aware of their HIV status. Eighty-nine participants tested HIV-negative, among whom 84% (n=75) were aware of their status based on at least one HIV test in the prior 12 months. Scores for HIV knowledge (median: 5/5), HIV risk perception (median: 3/4), and transgender pride (median: 14/16) were high. Lifetime history of sex work (79%) and condomless anal sex in the prior 12 months (47%) were common.
Most participants had heard of PrEP (87%); of those, 80% knew where to get it and 17% had ever taken it (Table 2). Of those who had ever taken PrEP (n=30), 80% had done so in the prior 12 months. Despite low uptake, 75% of HIV-negative participants reported that they would take PrEP if it were available to them. Fifty-seven percent of participants had heard of PEP, 10% had ever used it; and of those who had used PEP, 36% had done so within the prior 12 months. The most common reasons reported for using PEP was unprotected sex (50%) and being raped (25%) [data not shown]. Almost everyone (96%) was willing to use PEP if they were exposed to HIV. Most participants were willing to use an HIV vaccine (85%) or a microbicide (84%).
Table 2.
Engagement with Prevention Interventions
| Awareness | Know where to get | Ever used | Used in prior 12 mo. | Willing to use | |
|---|---|---|---|---|---|
| n/N (%) | n/N (%) | n/N (%) | n/N (%) | n/N (%) | |
| Available intervention | |||||
| PrEP | 174/201 (86.6) | 139/174 (79.9) | 30/173 (17.3) | 24/30 (80.0) | 54/72 (75.0)1 |
| PEP | 115/201 (57.2) | ---- | 11/115 (9.6) | 4/11 (36.4) | 95/98 (96.4)2 |
| Future intervention | |||||
| Vaccine | ---- | ---- | ---- | ---- | 83/98 (84.7)2 |
| Microbicide | ---- | ---- | ---- | ---- | 169/201(84.1) |
Denominator is HIV negative and status unknown participants who had never taken PrEP
Denominator is HIV negative and status unknown participants
In bivariate analyses, HIV knowledge, transgender pride, legal gender affirmation, history of exchange sex, and HIV risk perception were each significantly associated with willingness to take PrEP (Table 3). Age, city, Hispanic/Latina ethnicity, race, language, recent condomless anal sex, and current hormone therapy were not associated with PrEP willingness. In the multivariable model, which controlled for age and city, increased HIV knowledge (aOR 0.32 [95%CI: 0.10, 0.97]), and legal gender affirmation (aOR 0.10 [95%CI: 0.01, 0.81]) were both associated with lower odds of PrEP willingness. A history of exchange sex (aOR 5.79 [95%CI: 1.00, 33.7]) was associated with higher odds of PrEP willingness.
Table 3.
Predictors of PrEP Willingness1
| Variable | Bivariate | Multivariable | ||
|---|---|---|---|---|
| OR [95% CI] | p-value | aOR [95% CI] | p-value | |
| Age in years2 | 1.01 [0.97, 1.06] | 0.61 | 1.05 [0.98, 1.13] | 0.19 |
| City (DC v. Baltimore) | 0.77 [0.24, 2.42] | 0.65 | 0.29 [0.04, 1.83] | 0.19 |
| Race (Black v. non-Black) | 0.80 [0.27, 2.33] | 0.68 | ---- | |
| Latina/Hispanic ethnicity | 1.43 [0.48, 4.54] | 0.69 | ---- | |
| Language (English v. Spanish) | 0.34 [0.09, 1.32] | 0.12 | ---- | |
| Condomless anal sex in prior 12 mo | 1.74 [0.56, 5.27] | 0.34 | ---- | |
| HIV knowledge2 | 0.30 [0.11, 0.79] | 0.01 | 0.32 [0.10, 0.97] | 0.05 |
| Transgender pride2 | 1.22 [1.07, 1.39] | <0.01 | 1.08 [0.92, 1.28] | 0.33 |
| Legal gender affirmation3 | 0.27 [0.07, 1.04] | 0.06 | 0.10 [0.01, 0.81] | 0.03 |
| Current hormone use | 0.62 [0.18, 2.17] | 0.46 | ---- | |
| History of exchange sex | 3.33 [1.03, 10.7] | 0.04 | 5.79 [1.00, 33.7] | 0.05 |
| HIV risk perception2 | 1.86 [1.08, 3.18] | 0.02 | 1.91 [0.94, 3,86] | 0.07 |
Among HIV negative and status unknown participants who had never taken PrEP
Measured as continuous variable
Any name and/or gender marker change versus none
Among participants who were not willing to take PrEP, the most commonly reported reason (65%) was concern about drug interactions with hormones (Figure 1), followed by side effects (47%) and not wanting to take a pill everyday (41%). Participants who had taken PrEP reported multiple experiences, including people thinking they have HIV (52%), side effects (44%), and feeling like they were not at risk for HIV (38%). The least commonly reported experience was drug interactions with hormones (15%).
Figure 1.
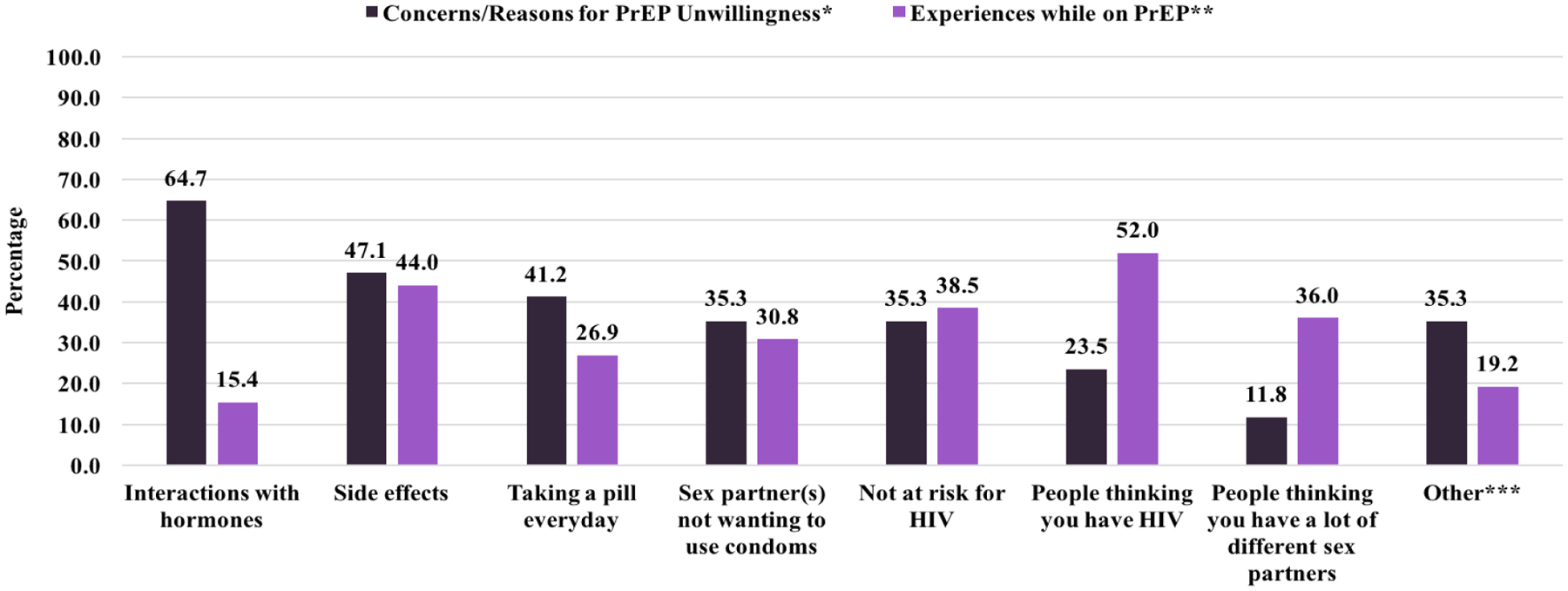
Reasons for PrEP Unwillingness and Experiences while on PrEP
*n=17: HIV-negative BLTW who have never taken PrEP and reported unwillingness to take PrEP if it were available to them
**n=26: BLTW who reported ever taking PrEP
Qualitative
We identified several themes within the qualitative data that provide additional insights on potential reasons for low uptake of PrEP and offer testable approaches for improving engagement in the HIV prevention. These themes (Table 4) include distrust of medical establishments and competing priorities other than HIV as well as concerns about an excessive focus on HIV by health institutions while BLTW desire holistic support, with services ideally provided by transgender people. Participants emphasized the importance of embedding HIV services within social service programs that are responsive to community needs (e.g., violence prevention, employment, housing) to improve access and acceptability. They also recommended regular staff training in transgender competent care (e.g., using correct names and pronouns), recognizing that experiencing stigma in health venues erodes trust and deters BLTW from care seeking.
Table 4.
Qualitative Themes and Example Quotes
| Themes | Example Quotes |
|---|---|
| Distrust of Medical Establishments | “I start thinking about pills. They’re going to try a new drug on me or something and it’s like oh, no.” (Participant 4 FGD3, Black transgender women, support group participant) “I think people know about it [PrEP]. There’s a lot of skepticism in the transgender community… About anything new that comes down the pipe just because of history, and history has been that we’ve been used for a lot of things, and the things that we’ve been used for haven’t necessarily benefitted the community… it hasn’t resulted in jobs for the community, and so they’re always met with a degree of skepticism.” (Key Informant 2, Black transgender woman, advocate and founder of community-based organization) |
| Desire for Holistic Support | “I’m more than just possibly an HIV positive or negative person. And so how are you going to make me or how are you going to really help or support me to become a woman? And that’s more important than whether or not I have HIV.” (Key Informant 12, Black cisgender man, research coordinator) “I think that holistic health services are important, you know, and nutrition because I know people talk a lot about HIV prevention but they don’t talk enough about healthy eating, you know, they don’t talk enough about exercise, and they don’t talk enough about… the intersection between health, HIV, exercise, and mental health, you know, it’s just starting to the forefront now but they are all connected.” (Key Informant 2, Black transgender woman, advocate and founder of community-based organization) |
| Excessive focus on HIV/AIDS | “…We focus so much on the HIV/AIDS piece, it scares them away. If we can do something else and then incorporate the HIV/AIDS piece into it, it would be better.” (Key Informant 5, Black cisgender man, mobile outreach specialist) “…for the longest time I haven’t been able to get services unless I have HIV… Yeah. Three years ago I was homeless, even though I’m a senior, even though I’m transgender, and even though I have a disability, and they have vouchers for transgender women who were seniors and who had a disability, and so when I tried to access these services through the city Homeless Services the first question they asked me did I have HIV, and they said because if you had HIV then we could get you in right now. So, it’s almost like something that you have to be, you have to be HIV positive.” (Key Informant 2, Black transgender woman, advocate and founder of community-based organization) “…the only time we talk about really young Black people particularly in Baltimore young Black MSM or young Black trans women is as it relates to HIV and people know that. And I think they’re burnt out. They’ve HIV’d out. I think they want to be more than just possible vectors of disease. And so I think that’s one challenge that I would be like how do we spin because it is a spin, you know, because ultimately the funding is about AIDS. But how do you make this about their health and their successful identity development.” (Key Informant 12, Black cisgender man, research coordinator) |
| Need for transgender service providers | “I know they’re getting better at but for a while it was a bunch of straight white girls working in case management, and to me I feel like that’s kind of a problem when you’re working in HIV and your clientele is going to be in Baltimore City, mostly people of color and also gay and bisexual and same-gender-loving men and trans women. I think that you need to have individuals who are part of the community serving the community.” (Key Informant 3, White cisgender woman, LGBT programs manager) “I think they would feel comfortable receiving services from other transgender women. In fact I think some people have been waiting to see that.” (Key Informant 2, Black transgender woman, advocate and founder of community-based organization) |
| Competing Priorities | I would also just be aware because there have been so many murders and violence… with trans women of color in Baltimore City. It’s another thing that [is] an issue and.… more of a priority than HIV. (Key Informant 3, White cisgender woman, LGBT programs manager) “HIV is-- it’s sad to say-- in the trans community is not the top concern. The top concern is housing, finding a job, becoming working women, stop working on the streets, surviving. All of that comes before HIV in the trans world, and I’m telling you from what I know, because I’m a trans woman.” (Key Informant 8, Black transgender woman, HIV prevention specialist) |
Discussion
In this mixed methods study of PrEP engagement among BLTW with high HIV knowledge and risk perception as well as high prevalence of exchange sex and recent condomless anal sex, we found high PrEP awareness and willingness but low uptake. These findings are consistent with other studies that indicate low uptake of PrEP among TW.23,26,35,36,39 The most commonly reported reason for being unwilling to take PrEP was concern about drug interactions with gender affirming hormones, a concern that is also a barrier to antiretroviral therapy adherence among TW living with HIV.40 In contrast to high levels of concerns about drug interactions among BLTW unwilling to take PrEP, few PrEP users reported experiencing interactions with hormones.
Recent studies have begun to address drug interaction concerns. A pharmacokinetic study among TW in Thailand found that TDF-FTC did not lower blood levels of estrogen in transgender women.41 Levels of tenofovir were 13% lower in the presence of exogenous estrogen but still above the level shown to confer protection in previous studies. This study did not obtain rectal tissue samples, therefore, could not determine if this difference in blood levels correlated to levels at the most common site of infection for TW. However, a US-based pharmacokinetic study collected both blood and rectal tissue.42 Lower concentrations of tenofovir were found in both; however, these differences only reached statistical significance in blood. These studies provide some reassurance that TDF-FTC does not affect exogenous estrogen levels but raise questions about the potential need for TDF-FTC dose adjustment. At minimum, they suggest that event-driven dosing43,44 may not be effective for TW taking estrogen. Given community concerns about drug interactions, it is important to disseminate accurate information on this topic to TW.
While willingness to take oral PrEP was relatively high (75%) in this study, it was not significantly associated with recent condomless sex nor with HIV risk perception. PrEP willingness was associated with a history of exchange sex, suggesting that TW engaged in sex work recognize their risk and see PrEP as a way to reduce their HIV vulnerability.45 TW sex workers should be prioritized for PrEP implementation.
Greater knowledge about HIV risk behavior was associated with lower willingness to take PrEP. One potential explanation for this finding is that BLTW who are most knowledgeable about HIV transmission, may prefer other methods to reduce their HIV risk. Ad hoc post-test counseling discussions with participants revealed that BLTW who had received past HIV prevention education felt condoms were a better approach given their ability to prevent sexually transmitted infections. Further research into health educators and medical providers’ messaging around condom use and PrEP is warranted.
Contrary to expectations, legal gender affirmation was associated with lower willingness to take PrEP. Given qualitative data on lack of TW-focused marketing as a barrier to PrEP uptake,26 it is also possible that TW with legal documents that affirmed their gender were less likely to respond to the largely MSM-focused marketing of PrEP.28 That is, as affirmed women, a product marketed for men may not be seen as relevant to them. It is also feasible that lack of legal gender affirmation and lack of willingness to take PrEP were both related to the distrust in medical and legal establishments described in the qualitative data and in published literature.17 Lack of financial resources may also limit access both to PrEP and to gender-affirming legal identity documents. Given the many possible explanations for this finding, it warrants further exploration in future studies.
Baltimore and Washington, DC have engaged substantial resources into promotion of PrEP for key populations at risk for HIV.46,47 Therefore, it was not surprising that most study participants were aware of PrEP and knew where to get it. However, this awareness did not translate into high uptake. Even with three-fourths of BLTW in the study expressing willingness to take PrEP, less than one-fifth of them had taken it. Qualitative and quantitative findings provide important insights that may explain the gap between willingness and uptake. Among participants who had taken PrEP, more than half reported that people thought they were living with HIV because they were taking an HIV-related medication. More than 35 years into the epidemic, HIV stigma remains strong and may deter PrEP uptake among BLTW who already face stigma and discrimination along axes of gender and race.48,49
The sociodemographic profile and qualitative themes draw attention to contextual factors and community priorities that may minimize BLTW’s focus on HIV. Three quarters of the sample lived in poverty, more than half were unstably housed, and the vast majority relied on public health insurance. Prior research indicates that such structural factors create significant barriers to HIV prevention, including PrEP uptake, even among people who are willing to take it.50,51 While research on PrEP among TW is increasing, there are few evidence-based interventions that address these and other structural forces such as institutionalized stigma and discrimination49, that both increase HIV vulnerability52,53 and serve as barriers to uptake of HIV prevention interventions.5
Qualitative data indicate that centering community priorities, like violence prevention and response, gender affirmation, and holistic support, may be an effective way to address HIV disparities among BLTW. In addition to being a known driver of HIV,54–56 violence against TW is a life-threatening health disparity in itself.57 While few intervention studies have included TW, research with cisgender women suggests that addressing violence may reduce HIV risk and improve uptake of HIV interventions.58–63 Key informants also recommended embedding HIV prevention services within programs that BLTW trust and services that they prioritize. Formative research among TW suggest that such integrated, more holistic, approaches are both acceptable and feasible.64–66 Other strategies suggested by key informants and supported by existing literature include hiring and supporting TW staff in HIV programs, engaging TW in places they already go, respectful and transgender-competent service providers, and partnering with transgender-led organizations.67,68
Limitations
The cross-sectional nature of the study precludes causal inferences and the use of convenience sampling limits generalizability. The small number of participants who provided data on self-reported reasons for PrEP willingness and experiences while taking PrEP impede statistical analyses and thus, limit the reliability of these data. The lack of qualitative data from participants in Washington, DC and the low numbers of adolescent participants prevent a deeper understanding of HIV prevention issues specific to those populations. Even with these limitations, this study provides important data to fill gaps in understanding barriers to engagement of BLTW in the PrEP care continuum.
Conclusion
Expanding the PrEP care continuum to include willingness as a stage between awareness and uptake, allowed this study to identify a gap between willingness and uptake for BLTW. This finding indicates that awareness of HIV risk, awareness of and willingness to take PrEP may be necessary but insufficient for PrEP uptake. While this study was not designed to identify the reasons for low uptake despite high willingness, barriers to provision of PrEP should be considered. Studies with healthcare providers suggest multiple provider barriers to PrEP provision, including racism,69 stigma,15,70 low PrEP knowledge,71 discomfort discussing sex with patients,72 and concerns about risk compensation.71,73 Additional, structural barriers to PrEP uptake include the need for frequent medical visits,74 lack of payor source,50,75 and lack of integration with gender-affirming medical care.76 Further research is needed to better understand reasons for low PrEP uptake among TW with high willingness to use PrEP.
Efforts to improve the uptake of PrEP among TW are needed. HIV prevention programs could better bridge the gap between willingness and uptake of PrEP among BLTW by incorporating strategies voiced by community leaders, recognizing competing priorities, and responding to identified access barriers. The ultimate purpose of PrEP is to prevent HIV and protect the health of populations heavily impacted by HIV. Transgender community leadership, peer support, and collaboration are key to successful HIV prevention efforts.77,78 Of note, the World Health Organization lists community empowerment as an essential strategy for addressing HIV among transgender people.79,80 Future research and interventions should address not only PrEP engagement and structural barriers that limit access, but also ensure that approaches are community-led, empowering, and affirming. The Gender Affirmation Framework represents a community-derived framework that can be used for research and intervention development.52,81 Examples of community-led, gender-affirming healthcare delivery models are available in the U.S.,82 the United Kingdom,83 and Latin America.84
Supplementary Material
Acknowledgements
We are grateful to all study participants as well as the community-based organizations and leaders who promoted the study and provided invaluable access to safe and accessible spaces for data collection. In alphabetical order, these organizations include AIDS Action Baltimore, BESURE Baltimore, Casa Ruby, Chase Brexton Health Services, The DC Center, Emerge Gender Clinic, La Clínica del Pueblo, the Maryland Transgender Response Team, Youth Empowered Society, and Whitman-Walker Health Center.
This publication resulted from research supported by the Johns Hopkins University Center for AIDS Research, an NIH funded program (P30AI094189), and by services from the District of Columbia Center for AIDS Research, an NIH funded program (AI117970), which are both supported by the following NIH Co-Funding and Participating Institutes and Centers: NIAID, NCI, NICHD, NHLBI, NIDA, NIMH, NIA, FIC, NIGMS, NIDDK, and OAR. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Footnotes
Parts of these data were presented at the International AIDS Society Conference in Paris, France in July 2017, American Public Health Association in Atlanta, GA in November 2017, and the Conference on Retroviruses and Opportunistic Infections in Boston, Massachusetts in March 2018.
References
- 1.Nuttbrock L, Bockting W, Rosenblum A, et al. Gender abuse, depressive symptoms, and HIV and other sexually transmitted infections among male-to-female transgender persons: a three-year prospective study. American journal of public health. 2013;103(2):300–307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Salazar LF, Crosby RA, Jones J, Kota K, Hill B, Masyn KE. Contextual, experiential, and behavioral risk factors associated with HIV status: a descriptive analysis of transgender women residing in Atlanta, Georgia. International journal of STD & AIDS. 2017;0(0):1–8. [DOI] [PubMed] [Google Scholar]
- 3.Habarta N, Wang G, Mulatu MS, Larish N. HIV Testing by Transgender Status at Centers for Disease Control and Prevention-Funded Sites in the United States, Puerto Rico, and US Virgin Islands, 2009–2011. American journal of public health. 2015;105(9):1917–1925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Reisner SL, Jadwin-Cakmak L, White Hughto JM, Martinez M, Salomon L, Harper GW. Characterizing the HIV Prevention and Care Continua in a Sample of Transgender Youth in the U.S. AIDS and behavior. 2017;21(12):3312–3327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Poteat T, Malik M, Scheim A, Elliott A. HIV Prevention Among Transgender Populations: Knowledge Gaps and Evidence for Action. Current HIV/AIDS reports. 2017;14(4):141–152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Grant RM, Lama JR, Anderson PL, et al. Preexposure Chemoprophylaxis for HIV Prevention in Men Who Have Sex with Men. New England Journal of Medicine. 2010;363(27):2587–2599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Murnane PM, Celum C, Mugo N, et al. Efficacy of preexposure prophylaxis for HIV-1 prevention among high-risk heterosexuals: subgroup analyses from a randomized trial. AIDS (London, England). 2013;27(13):2155–2160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Choopanya K, Martin M, Suntharasamai P, et al. Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. 2013;381(9883):2083–2090. [DOI] [PubMed] [Google Scholar]
- 9.Van Damme L, Corneli A, Ahmed K, et al. Preexposure Prophylaxis for HIV Infection among African Women. New England Journal of Medicine. 2012;367(5):411–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Marrazzo JM, Ramjee G, Richardson BA, et al. Tenofovir-Based Preexposure Prophylaxis for HIV Infection among African Women. New England Journal of Medicine. 2015;372(6):509–518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Deutsch MB, Glidden DV, Sevelius J, et al. HIV pre-exposure prophylaxis in transgender women: a subgroup analysis of the iPrEx trial. Lancet HIV. 2015;2(12):e512–519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Huang YA, Zhu W, Smith DK, Harris N, Hoover KW. HIV Preexposure Prophylaxis, by Race and Ethnicity - United States, 2014–2016. MMWR Morbidity and mortality weekly report. 2018;67(41):1147–1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.van Epps P, Maier M, Lund B, et al. Medication Adherence in a Nationwide Cohort of Veterans Initiating Pre-exposure Prophylaxis (PrEP) to Prevent HIV Infection. Journal of acquired immune deficiency syndromes (1999). 2018;77(3):272–278. [DOI] [PubMed] [Google Scholar]
- 14.Nunn AS, Brinkley-Rubinstein L, Oldenburg CE, et al. Defining the HIV pre-exposure prophylaxis care continuum. AIDS (London, England). 2017;31(5):731–734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Calabrese SK. Interpreting Gaps Along the Preexposure Prophylaxis Cascade and Addressing Vulnerabilities to Stigma. American journal of public health. 2018;108(10):1284–1286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Golub SA, Gamarel KE, Rendina HJ, Surace A, Lelutiu-Weinberger CL. From Efficacy to Effectiveness: Facilitators and Barriers to PrEP Acceptability and Motivations for Adherence Among MSM and Transgender Women in New York City. AIDS patient care and STDs. 2013;27(4):248–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Eaton LA, Kalichman SC, Price D, Finneran S, Allen A, Maksut J. Stigma and Conspiracy Beliefs Related to Pre-exposure Prophylaxis (PrEP) and Interest in Using PrEP Among Black and White Men and Transgender Women Who Have Sex with Men. AIDS and behavior. 2017;21(5):1236–1246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Grant RM, Anderson PL, McMahan V, et al. Uptake of pre-exposure prophylaxis, sexual practices, and HIV incidence in men and transgender women who have sex with men: a cohort study. The Lancet Infectious diseases. 2014;14(9):820–829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Poteat T, German D, Flynn C. The conflation of gender and sex: Gaps and opportunities in HIV data among transgender women and MSM. Global public health. 2016;11(7–8):835–848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Garnett M, Hirsch-Moverman Y, Franks J, Hayes-Larson E, El-Sadr WM, Mannheimer S Limited awareness of pre-exposure prophylaxis among black men who have sex with men and transgender women in New York city. AIDS care. 2018;30(1):9–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jalil EM, Grinsztejn B, Velasque L, et al. Awareness, Willingness, and PrEP Eligibility Among Transgender Women in Rio de Janeiro, Brazil. Journal of acquired immune deficiency syndromes (1999) 2018;79(4):445–452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Oldenburg CE, Le B, Toan T, et al. HIV Pre-exposure Prophylaxis Indication and Readiness Among HIV-Uninfected Transgender Women in Ho Chi Minh City, Vietnam. AIDS and behavior. 2016;20(Suppl 3):365–370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wang Z, Lau JTF, Yang X, et al. Acceptability of Daily Use of Free Oral Pre-exposure Prophylaxis (PrEP) Among Transgender Women Sex Workers in Shenyang,China. AIDS and behavior. 2017;21(12):3287–3298. [DOI] [PubMed] [Google Scholar]
- 24.Zalazar V, Aristegui I, Kerr T, et al. High Willingness to Use HIV Pre-Exposure Prophylaxis Among Transgender Women in Argentina. Transgender health. 2016;1(1):266–273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Restar AJ, Kuhns L, Reisner SL, Ogunbajo A, Garofalo R, Mimiaga MJ. Acceptability of Antiretroviral Pre-exposure Prophylaxis from a Cohort of Sexually Experienced Young Transgender Women in Two U.S Cities. AIDS and behavior. 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rael CT, Martinez M, Giguere R, et al. Barriers and Facilitators to Oral PrEP Use Among Transgender Women in New York City. AIDS and behavior. 2018;22(11):3627–3636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kuhns LM, Reisner SL, Mimiaga MJ, Gayles T, Shelendich M, Garofalo R. Correlates of PrEP Indication in a Multi-Site Cohort of Young HIV-Uninfected Transgender Women. AIDS and behavior. 2016;20(7):1470–1477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sevelius JM, Keatley J, Calma N, Arnold E. ‘I am not a man’: Trans-specific barriers and facilitators to PrEP acceptability among transgender women. Global public health. 2016;11(7–8):1060–1075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Larkin PM, Begley CM, Devane D. Breaking from binaries - using a sequential mixed methods design. Nurse researcher. 2014;21(4):8–12. [DOI] [PubMed] [Google Scholar]
- 30.Yamanis T, Malik M, Del Rio-Gonzalez AM, et al. Legal Immigration Status is Associated with Depressive Symptoms among Latina Transgender Women in Washington,DC. International journal of environmental research and public health. 2018;15(6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.2017. Poverty Guidelines. https://aspe.hhs.gov/2017-poverty-guidelines.
- 32.Testa RJ, Habarth J, Peta J, Balsam K, Bockting W. Development of the Gender Minority Stress and Resilience Measure. Psychology of Sexual Orientation and Gender Diversity. 2015;2(1):65. [Google Scholar]
- 33.Fay H, Baral SD, Trapence G, et al. Stigma, Health Care Access, and HIV Knowledge Among Men Who Have Sex With Men in Malawi, Namibia, and Botswana. AIDS and behavior. 2011;15(6):1088–1097. [DOI] [PubMed] [Google Scholar]
- 34.Auerbach JD, Kinsky S, Brown G, Charles V. Knowledge, Attitudes, and Likelihood of Pre-Exposure Prophylaxis (PrEP) Use Among US Women at Risk of Acquiring HIV. AIDS patient care and STDs. 2014;29(2):102–110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Eaton LA, Matthews DD, Driffin DD, Bukowski L, Wilson PA, Stall RD. A Multi-US City Assessment of Awareness and Uptake of Pre-exposure Prophylaxis (PrEP) for HIV Prevention Among Black Men and Transgender Women Who Have Sex with Men. Prevention science : the official journal of the Society for Prevention Research. 2017;18(5):505–516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hoagland B, De Boni RB, Moreira RI, et al. Awareness and Willingness to Use Pre-exposure Prophylaxis (PrEP) Among Men Who Have Sex with Men and Transgender Women in Brazil. AIDS and behavior. 2017;21(5):1278–1287. [DOI] [PubMed] [Google Scholar]
- 37.Grinsztejn B, Hoagland B, Moreira RI, et al. Retention, engagement, and adherence to pre-exposure prophylaxis for men who have sex with men and transgender women in PrEP Brasil: 48 week results of a demonstration study. Lancet HIV. 2018;5(3):e136–e145. [DOI] [PubMed] [Google Scholar]
- 38.Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nursing & Health Sciences. 2013;15(3):398–405. [DOI] [PubMed] [Google Scholar]
- 39.Mehrotra ML, Rivet Amico K, McMahan V, et al. The Role of Social Relationships in PrEP Uptake and Use Among Transgender Women and Men Who Have Sex with Men. AIDS and behavior. 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Braun HM, Candelario J, Hanlon CL, et al. Transgender Women Living with HIV Frequently Take Antiretroviral Therapy and/or Feminizing Hormone Therapy Differently Than Prescribed Due to Drug-Drug Interaction Concerns. LGBT health. 2017;4(5):371–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Hiransuthikul A, Himmad K, Kerr S, et al. Drug-drug interactions between the use of feminizing hormone therapy and pre-exposure prophylaxis among transgender women: The iFACT study. Paper presented at: AIDS 2018; Amsterdam, The Netherlands. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Shieh E, Marzinke M, Fuchs E, et al. Transgender Women on Estrogen Have Significantly Lower Tenofovir/Emtricitabine Concentrations During Directly Observed Dosing When Compared to Cis Men. Paper presented at: HIV Research for Prevention2018; Madrid, Spain. [Google Scholar]
- 43.Reyniers T, Nostlinger C, Laga M, et al. Choosing Between Daily and Event-Driven Pre-exposure Prophylaxis: Results of a Belgian PrEP Demonstration Project. Journal of acquired immune deficiency syndromes (1999). 2018;79(2):186–194. [DOI] [PubMed] [Google Scholar]
- 44.Bekker LG, Roux S, Sebastien E, et al. Daily and non-daily pre-exposure prophylaxis in African women (HPTN 067/ADAPT Cape Town Trial): a randomised, open-label, phase 2 trial. Lancet HIV. 2018;5(2):e68–e78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Poteat T, Wirtz AL, Radix A, et al. HIV risk and preventive interventions in transgender women sex workers. Lancet (London, England). 2015;385(9964):274–286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Project PRIDE. https://www.cdc.gov/hiv/research/demonstration/projectpride.html.
- 47.DC Health: DC PrEP Drug Assistance Program. https://dchealth.dc.gov/DCPrEPDAP.
- 48.Perez-Brumer A, Nunn A, Hsiang E, et al. “We don’t treat your kind”: Assessing HIV health needs holistically among transgender people in Jackson, Mississippi. PloS one. 2018;13(11):e0202389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.James SE, Herman JL, Rankin S, Keisling M, Mottet L, Anafi M. The Report of the 2015 U.S. Transgender Survey Washington, DC: National Center for Transgender Equality; 2016. [Google Scholar]
- 50.Marks SJ, Merchant RC, Clark MA, et al. Potential Healthcare Insurance and Provider Barriers to Pre-Exposure Prophylaxis Utilization Among Young Men Who Have Sex with Men. AIDS patient care and STDs. 2017;31(11):470–478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Sevelius JM, Reznick OG, Hart SL, Schwarcz S. Informing interventions: the importance of contextual factors in the prediction of sexual risk behaviors among transgender women. AIDS education and prevention : official publication of the International Society for AIDS Education. 2009;21(2):113–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Sevelius JM. Gender Affirmation: A Framework for Conceptualizing Risk Behavior among Transgender Women of Color. Sex roles. 2013;68(11–12):675–689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Fletcher JB, Kisler KA, Reback CJ. Housing status and HIV risk behaviors among transgender women in Los Angeles. Arch Sex Behav. 2014;43(8):1651–1661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.De Santis JP, Patsdaughter CA. The dangerous intersection of violence and HIV infection. J Assoc Nurses AIDS Care. 2014;25(1 Suppl):S1–4. [DOI] [PubMed] [Google Scholar]
- 55.Raiford JL, Hall GJ, Taylor RD, Bimbi DS, Parsons JT. The Role of Structural Barriers in Risky Sexual Behavior, Victimization and Readiness to Change HIV/STI-Related Risk Behavior Among Transgender Women. AIDS and behavior. 2016;20(10):2212–2221. [DOI] [PubMed] [Google Scholar]
- 56.Raiford JL, Hall GJ, Taylor RD, Bimbi DS, Parsons JT. Erratum to: The Role of Structural Barriers in Risky Sexual Behavior, Victimization and Readiness to Change HIV/STI-Related Risk Behavior Among Transgender Women. AIDS and behavior. 2017;21(7):2215–2215. [DOI] [PubMed] [Google Scholar]
- 57.Wirtz AL, Poteat TC, Malik M, Glass N. Gender-Based Violence Against Transgender People in the United States: A Call for Research and Programming. Trauma, violence & abuse. 2018:1524838018757749. [DOI] [PubMed] [Google Scholar]
- 58.Jewkes RK, Dunkle K, Nduna M, Shai N. Intimate partner violence, relationship power inequity, and incidence of HIV infection in young women in South Africa: a cohort study. The Lancet. 2010;376(9734):41–48. [DOI] [PubMed] [Google Scholar]
- 59.Pronyk PM, Hargreaves JR, Kim JC, et al. Effect of a structural intervention for the prevention of intimate-partner violence and HIV in rural South Africa: a cluster randomised trial. 2006;368(9551):1973–1983. [DOI] [PubMed] [Google Scholar]
- 60.Roberts ST, Haberer J, Celum C, et al. Intimate Partner Violence and Adherence to HIV Pre-exposure Prophylaxis (PrEP) in African Women in HIV Serodiscordant Relationships: A Prospective Cohort Study. Journal of acquired immune deficiency syndromes (1999) 2016;73(3):313–322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Braksmajer A, Leblanc NM, El-Bassel N, Urban MA, McMahon JM. Feasibility and acceptability of pre-exposure prophylaxis use among women in violent relationships. AIDS care. 2018:1–6. [DOI] [PubMed] [Google Scholar]
- 62.Gilbert L, Raj A, Hien D, Stockman J, Terlikbayeva A, Wyatt G. Targeting the SAVA (Substance Abuse, Violence, and AIDS) Syndemic Among Women and Girls: A Global Review of Epidemiology and Integrated Interventions. Journal of acquired immune deficiency syndromes (1999). 2015;69 Suppl 2:S118–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Collier KL, Colarossi LG, Hazel DS, Watson K, Wyatt GE. Healing Our Women for Transgender Women: Adaptation, Acceptability, and Pilot Testing. AIDS education and prevention : official publication of the International Society for AIDS Education. 2015;27(5):418–431. [DOI] [PubMed] [Google Scholar]
- 64.Reisner SL, Perez-Brumer AG, McLean SA, et al. Perceived Barriers and Facilitators to Integrating HIV Prevention and Treatment with Cross-Sex Hormone Therapy for Transgender Women in Lima, Peru. AIDS Behav. 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Hood JE, Eljallad T, Abad J, et al. Getting pre-exposure prophylaxis to high-risk transgender women: lessons from Detroit, USA. Sexual health. 2018;15(6):562–569. [DOI] [PubMed] [Google Scholar]
- 66.Melendez RM, Pinto RM. HIV prevention and primary care for transgender women in a community-based clinic. J Assoc Nurses AIDS Care. 2009;20(5):387–397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Reback CJ, Ferlito D, Kisler KA, Fletcher JB. Recruiting, Linking, and Retaining High-risk Transgender Women into HIV Prevention and Care Services: An Overview of Barriers, Strategies, and Lessons Learned. The international journal of transgenderism. 2015;16(4):209–221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Andrasik MP, Yoon R, Mooney J, et al. Exploring barriers and facilitators to participation of male-to-female transgender persons in preventive HIV vaccine clinical trials. Prevention science : the official journal of the Society for Prevention Research. 2014;15(3):268–276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Calabrese SK, Earnshaw VA, Underhill K, Hansen NB, Dovidio JF. The impact of patient race on clinical decisions related to prescribing HIV pre-exposure prophylaxis (PrEP): assumptions about sexual risk compensation and implications for access. AIDS and behavior. 2014;18(2):226–240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Calabrese SK, Tekeste M, Mayer KH, et al. Considering Stigma in the Provision of HIV Pre-Exposure Prophylaxis: Reflections from Current Prescribers. AIDS patient care and STDs. 2019;33(2):79–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Blackstock OJ, Moore BA, Berkenblit GV, et al. A Cross-Sectional Online Survey of HIV Pre-Exposure Prophylaxis Adoption Among Primary Care Physicians. Journal of general internal medicine. 2017;32(1):62–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Calabrese SK, Magnus M, Mayer KH, et al. Putting PrEP into Practice: Lessons Learned from Early-Adopting U.S. Providers’ Firsthand Experiences Providing HIV Pre-Exposure Prophylaxis and Associated Care. PloS one. 2016;11(6):e0157324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Calabrese SK, Earnshaw VA, Underhill K, et al. Prevention paradox: Medical students are less inclined to prescribe HIV pre-exposure prophylaxis for patients in highest need. Journal of the International AIDS Society. 2018;21(6):e25147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Meyers K, Golub SA. Planning ahead for implementation of long-acting HIV prevention: challenges and opportunities. Current opinion in HIV and AIDS. 2015;10(4):290–295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Schwartz J, Grimm J. PrEP on Twitter: Information, Barriers, and Stigma. Health communication. 2017;32(4):509–516. [DOI] [PubMed] [Google Scholar]
- 76.Sevelius JM, Deutsch MB, Grant R. The future of PrEP among transgender women: the critical role of gender affirmation in research and clinical practices. Journal of the International AIDS Society. 2016;19(7(Suppl 6)):21105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Wolf RC, Adams D, Dayton R, et al. Putting the t in tools: a roadmap for implementation of new global and regional transgender guidance. J Int AIDS Soc. 2016;19(3 Suppl 2):20801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Perez-Brumer AG, Reisner SL, McLean SA, et al. Leveraging social capital: multilevel stigma, associated HIV vulnerabilities, and social resilience strategies among transgender women in Lima, Peru. Journal of the International AIDS Society. 2017;20(1):21462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.World Health Organization. Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations–2016 update. World Health Organization; 2016. [Google Scholar]
- 80.Poteat T, Keatley J. Transgender People and HIV: Policy Brief. Geneva, Switzerland: World Health Organization; 2015. [Google Scholar]
- 81.Sevelius J, Murray LR, Martinez Fernandes N, Veras MA, Grinsztejn B, Lippman SA. Optimising HIV programming for transgender women in Brazil. Culture, health & sexuality. 2019;21(5):543–558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Reisner SL, Bradford J, Hopwood R, et al. Comprehensive transgender healthcare: the gender affirming clinical and public health model of Fenway Health. Journal of urban health : bulletin of the New York Academy of Medicine. 2015;92(3):584–592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.CliniQ. 2019; https://cliniq.org.uk/. Accessed 15 May 2019.
- 84.Educación. ACISy. Gender-Affirmative Transgender Care to Improve the HIV Treatment Cascade. 2018; https://clinicaltrials.gov/ct2/show/NCT03757117. Accessed 15 May 2019.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.