

Background:
A second wave of COVID-19 began in late June in Victoria, Australia. Stage 3 then Stage 4 restrictions were introduced in July–August. This study aimed to compare the use of pre-exposure prophylaxis (PrEP) and sexual practices among men who have sex with men taking PrEP between May–June (post-first lockdown) and July–August (second lockdown).
Methods:
This was an online survey conducted among men who have sex with men who had their PrEP managed at the Melbourne Sexual Health Centre, Australia. A short message service with a link to the survey was sent to 503 PrEP clients who provided consent to receive a short message service from Melbourne Sexual Health Centre in August 2020.
Results:
Of the 192 participants completed the survey, 153 (80%) did not change how they took PrEP. Of the 136 daily PrEP users, 111 (82%) continued to take daily PrEP, 3 (2%) switched to on-demand PrEP, and 22 (16%) stopped PrEP in July–August. Men generally reported that they had no partners or decreased sexual activities during second lockdown compared with post-first lockdown; the number of casual sex partners (43% decreased vs. 3% increased) and the number of kissing partners (36% decreased vs. 3% increased). Most men reported no chemsex (79%) or group sex (77%) in May–August. 10% (13/127) of men had ever worn face masks during sex in May–August.
Conclusion:
During the second wave of COVID-19 in Victoria, most men did not change the way they used PrEP but the majority had no risks or reduced sexual practices while one in 10 men wore a face mask during sex.
Key Words: COVID, coronavirus, PrEP, sexual practice, mask, men who have sex with men, HIV
INTRODUCTION
To control the COVID-19 pandemic, Australia introduced restrictions and a national lockdown starting from March 23, 2020.1 These restrictions included the closure of nonessential business, “stay at home” directions, social distancing rules to maintain at least 1.5 meters between people, and restrictions on social gatherings. The daily number of COVID-19 cases declined substantially in late April and these restrictions began to ease from May 13. The COVID-19 pandemic in most of the Australian states and territories has been under control since May. However, the daily number of COVID-19 cases began to rise substantially in late June in Victoria with a peak of 700 cases on August 5.2 Stage 3 restrictions (eg, closure of nonessential business and “stay at home” directions) were applied to metropolitan Melbourne on July 8, and all Victorians were required to wear face masks in public from July 22. From 6 pm on August 2, Victoria moved to Stage 4 restrictions (including a curfew between 8 pm and 5 am, no travel more than 5-km radius from home, and travelling to work was only permitted with a worker permit) in metropolitan Melbourne and Mitchell Shire for 6 weeks.
Under the previous restrictions during the national lockdown in March and April 2020, individuals had reduced their sexual activities, particularly sex with casual partners.3–5 There have been a few Australian and international studies examining pre-exposure prophylaxis (PrEP) use during the COVID-19 pandemic.6–8 Our previous Melbourne-based study reported that one in 4 men who have sex with men (MSM) taking daily HIV PrEP in January–February 2020 (ie, before first lockdown) had stopped taking PrEP in early May.9 Although Victoria had a second, more stringent lockdown and a more severe COVID-19 epidemic in July–October compared with the first lockdown in March–April, it is hypothesized that the proportion of MSM taking PrEP was similar in both lockdowns given there was no change in access to PrEP prescriptions and health care services. This study aimed to explore whether MSM changed their PrEP use and sexual practice in July–August (ie, during the second lockdown hereafter referred to as “second lockdown”) compared with May–June (ie, the period where the first lockdown was lifted and hereafter referred to as “post-first lockdown”).
METHODS
The Melbourne Sexual Health Centre (MSHC) is a major publicly funded HIV/STI clinic in Victoria, Australia. Since 2016, MSHC started an appointment-based PrEP clinic to provide routine clinical care and management for individuals taking PrEP. We identified 503 MSM aged ≥18 years, had their PrEP managed at MSHC in January–June 2020, and consented to receive a short message service (SMS) from MSHC.
Between August 5 and August 23, 2020, a single SMS invitation was sent to all 503 identified MSM. The SMS explained MSHC was conducting a survey about PrEP use and would like to invite them to participate in an online survey with a link provided. The front page of the survey described the study nature and involvement. A participant information sheet that described the details of the study was provided on the front page of the survey. Informed consent was obtained if the participants selected the “Agree” button on the front page before commencing the survey. Participants had the option to select “Disagree” if they did not want to participate. The survey was closed on August 31, 2020.
The questions in the survey were designed to compare PrEP use between 2 time-periods: (1) May–June (post first lockdown); and (2) July–August (second lockdown). Participants were asked to report whether they had changed their sexual practices in second lockdown compared with post-first lockdown, and whether they had ever worn a face mask during sex between May and August. Ethics approval was obtained from the Alfred Hospital Ethics Committee, Melbourne, Australia (249/20).
Descriptive statistics were used to determine the frequency and proportion of study variables. The 95% confidence intervals (CI) of the proportion of men taking PrEP were calculated using binomial exact methods. All statistical analyses were performed using STATA version 14.
RESULTS
Of the 503 MSM who received the SMS invitation, 193 (38%) men consented to participate in the survey, 308 (61%) did not click the survey link and 2 (0.4%) declined to participate after clicking the survey link. One man consented to participate but did not complete any questions and therefore was excluded from the analysis. The remaining 192 men were included, with a median age of 38 (interquartile range = 32–49), 60% (n = 116) were born in Australia and the median time taking PrEP was 35 (interquartile range = 17–47) months.
During post-first lockdown, 136 (71%; 95% CI: 64% to 77%) took daily PrEP, 17 (9%; 95% CI: 5% to 14%) took on-demand PrEP, and 39 (20%; 95% CI: 15% to 27%) did not take PrEP (Table 1). During second lockdown, 116 (60%; 95% CI: 53% to 67%) took daily PrEP, 15 (8%; 95% CI: 4% to 13%) took on-demand PrEP, and 61 (32%; 95% CI: 25% to 39%) did not take PrEP (Table 1). Of the 136 daily PrEP users during post-first lockdown, 111 (82%; 95% CI: 74% to 88%) continued to take daily PrEP, 3 (2%; 95% CI: 0% to 6%) switched to on-demand PrEP, and 22 (16%; 95 CI: 10% to 23%) stopped taking PrEP during second lockdown. Overall, 153 (80%; 95% CI: 73% to 85%) men did not change how they took PrEP (Table 1). Men who had changed PrEP use during second lockdown had been on PrEP with a shorter time (median 22 vs. 37 months; P = 0.023) compared with those who did not change.
TABLE 1.
The Use Pre-exposure Prophylaxis Among 192 MSM During Post-First Lockdown (May–June) and Second Lockdown (July–August)
| Second Lockdown (July-August) | ||||
| Daily | On-Demand | Stopped | Total | |
| Post first lockdown (May–June) | ||||
| Daily | 111 (58%) | 3 (2%) | 22 (11%) | 136 (71%) |
| On-demand | 2 (1%) | 9 (5%) | 6 (3%) | 17 (9%) |
| Stopped | 3 (2%) | 3 (2%) | 33 (17%) | 39 (20%) |
| Total | 116 (60%) | 15 (8%) | 61 (32%) | 192 |
There were 181 men who completed the questions on sexual practices, 54 (30%; 95% CI: 23% to 37%) men reported no sex in May–August. Of the 127 men who reported having any sexual contacts, 13 (10%; 95% CI: 6% to 17%) reported they had ever used a face mask during sex in May–August.
Comparing with post-first lockdown, most men reported they had decreased sexual activities during second lockdown, including the number of times having casual sex (48% decreased vs. 4% increased), number of casual sex partners (43% decreased vs. 3% increased), number of kissing partners (36% decreased vs. 3% increased), number of times meeting new partners face-to-face (34% decreased vs. 5%), number of group sex (12% decreased vs. 3% increased), and number of chemsex (ie, drug use before and/or during sex) (6% decreased vs. 3% increased) (Fig. 1). Most men reported they did not have chemsex (79%) or group sex (77%) and did not meet new partners face-to-face (48%) in May–August. Almost half (48%) reported no change in condom use with casual partners during second lockdown compared with that during post-first lockdown.
FIGURE 1.
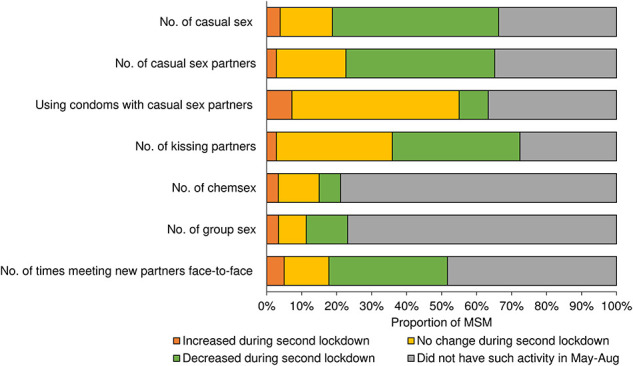
Changes in sexual practices among MSM in second lockdown compared with that post-first lockdown.
DISCUSSION
This survey showed that 82% of MSM taking daily PrEP before the second lockdown continued to take PrEP daily during the second lockdown in July–August. However, one in 6 stopped taking PrEP during the second lockdown and this proportion is similar but slightly lower compared with the period during the first lockdown (ie, one in 4 daily PrEP users stopped taking PrEP).9 Our clinic remained open during the usual operating hours and there was no change in accessing PrEP prescriptions in both lockdowns; this may explain why the proportion of men who discontinued PrEP was similar. Our estimates are slightly lower than the US, which showed about one-third of PrEP users discontinued PrEP during lockdown,8 and this may be because of the fact that the COVID-19 pandemic in the US is more widespread than in Australia. Discontinuing PrEP during lockdown is most likely to be because of reduced sexual risk, but some may have also stopped PrEP because they feared catching SARS-CoV-2 when visiting the clinic for PrEP review and prescriptions.6,9 We found that a substantial proportion of MSM either had no sexual contact or reduced their sexual risk, including group sex, chemsex and the number of casual partners during the second lockdown compared with the period when the first lockdown was eased. Furthermore, one in 10 MSM had ever worn a face mask during sex in the COVID-19 pandemic in May–August.
The Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM) has recommended several harm reduction strategies to prevent SARS-CoV-2 during casual sex and these include reducing the number of casual sex partners and avoiding activities such as group sex, kissing, and close face-to-face contacts.10 These recommendations are similar to those of other international HIV/STI organizations. On August 11, 2020, Terrence Higgins Trust, a leading HIV and sexual health charity in the United Kingdom, provided additional advice on wearing face masks during sex in the COVID-19 pandemic11; however, this advice has not been adopted by any health organizations in Australia to our knowledge. Our findings show that one in 10 MSM had ever worn a face mask during sex in the COVID-19 pandemic and this estimate has not been examined or reported previously. However, the reasons for wearing face masks during sex were not collected in this survey. Some men may wear masks to minimize the risk of catching SARS-CoV-2 during sex. However, it is also possible that some men may wear masks for other reasons such as sexual fetishes, sexual role play, or anonymity, rather than related to the COVID-19 pandemic.12,13 Further studies are required to determine whether face masks use during sex with casual partners would be an acceptable or effective practice in all populations. Previous studies have suggested that MSM derive very substantial pleasure and intimacy from kissing,14 so it may be unlikely it will be widely adopted outside of a large COVID-19 outbreak.
Most men reported a decreased number of casual partners or no casual partners during the second lockdown. This is consistent with previous studies showing a reduction in casual sex during the national lockdown in March–April.3,4,9 It is also important to note that about one-third of MSM reported no casual partners in May–August. HIV postexposure prophylaxis (PEP) prescriptions have been used as a proxy for high-risk practices and studies have shown that there was a significant reduction in PEP prescriptions after the lockdown around March in Australia, the United Kingdom and Spain, where countries have been badly affected by COVID-19.15–17 Over the study period, there was also a 33% reduction (132 in May–June vs. 88 in July–August) of PEP prescription at our service (data not shown). Consistent with these findings, other studies have reported an increase in activities with no risk for HIV and STI, such as masturbation and cybersex during the COVID-19 pandemic.3,18 The reduction in sexual risk can potentially lead to temporal reductions in HIV and other sexually transmitted infections (STI).5,19,20 However, the severity of COVID-19 pandemic in some settings may cause interruptions in delaying and accessing HIV/STI testing.21–23 This is supported by a study conducted in 3 Kenyan counties showing that there was a significant reduction in the number of HIV tests at clinical sites during lockdown although there was an increase in HIV self-testing.24 Timely testing, diagnosis, and treatment are important for HIV prevention. Some mathematical models have predicted the COVID-19 pandemic may lead to an increase in HIV-related mortality because of the disruptions to HIV services and treatment access during the COVID-19 pandemic in some settings.23,25 Further studies are required to explore the impact of COVID-19 on HIV testing, diagnoses, and treatment.
Our study has some limitations. First, the study was conducted among MSM taking PrEP in a sexual health clinic setting. The estimates of changes in sexual practices and using face masks during sex may not be generalizable to all MSM as previous studies have shown that the sexual risk among MSM taking PrEP is different from those who are not taking PrEP.26 Second, recall bias may have occurred in self-reporting PrEP use and sexual practices. Furthermore, social desirability bias may have occurred as some men may report better compliance with the restrictions during lockdown. Third, we were unable to explore the difference in sexual risk between MSM who have ever used masks and those who have never used because of the small sample size in the face masks group (n = 13). Fourth, only 38% of men responded to our survey link. The sexual practices and PrEP use may be different between men who responded and those who did not. Finally, this was a cross-sectional study and thus causality cannot be proven. Although we cannot determine whether any behavioral changes from post-first lockdown to second lockdown are directly caused by the lockdowns themselves or related to other factors such as concerns about catching SARS-CoV-2,9 other studies have also shown reductions in sexual risk during lockdown.6–8
In conclusion, we found that one in 6 MSM taking PrEP daily stopped taking PrEP during the second lockdown and most men stopped or decreased some sexual activities during the second lockdown in Melbourne. The use of face masks during sex in the COVID-19 pandemic was not uncommon among MSM taking PrEP. Public health messages on safe sex practice during the COVID-19 pandemic are required and these messages should reinforce not only the safety precautions to prevent catching SAR-CoV-2 but also HIV and STIs.
ACKNOWLEDGMENTS
The authors would like to thank Afrizal Afrizal from Melbourne Sexual Health Centre for his assistance with data extraction and identifying PrEP clients.
Footnotes
E.P.F.C. and C.K.F. are each supported by an Australian National Health and Medical Research Council (NHMRC) Investigator Grant (GNT1172873 for E.P.F.C. and GNT1172900 for C.K.F.). J.J.O. is supported by an NHRMC Early Career Fellowship (GNT1104781). J.S.H. is supported by an NHMRC Senior Research Fellowship (GNT1136117). E.P.F.C. has received a research grant and honoraria from Gilead Pharmaceuticals on HIV and PrEP research outside the submitted work.
The authors have no conflicts of interest to disclose.
E.P.F.C., J.S.H., J.J.O., and C.K.F. contributed to the concept and design of the study and designed the survey. T.S. and A.B. assisted with the survey design. E.P.F.C., E.R., and K.M. were involved in study recruitment by sending SMS invitations to potential participants. E.P.F.C. oversaw the study, performed data analysis, and wrote the first draft of the manuscript. All authors were involved in data interpretation and revising the manuscript for important intellectual content and approved the final version.
Contributor Information
Jane S. Hocking, Email: j.hocking@unimelb.edu.au.
Jason J. Ong, Email: Jason.ong@monash.edu.
Tiffany R. Phillips, Email: TPhillips@mshc.org.au.
Tina Schmidt, Email: TSchmidt@mshc.org.au.
Andrew Buchanan, Email: ABuchanan@mshc.org.au.
Elena Rodriguez, Email: Erodriguez@mshc.org.au.
Kate Maddaford, Email: KMaddaford@mshc.org.au.
Christopher K. Fairley, Email: CFairley@mshc.org.au.
REFERENCES
- 1.COVID-19 National Incident Room Surveillance Team. COVID-19, Australia: epidemiology report 20 (fortnightly reporting period ending 5 July 2020). Commun Dis Intell. 2020;44:1–31. [DOI] [PubMed] [Google Scholar]
- 2.Vicotira State Government. Coronavirus Update for Victoria—5 August 2020. Department of Health and Human Services, State Government of Victoria, Australia; 2020. Available at: https://www.dhhs.vic.gov.au/coronavirus-update-victoria-5-august-2020. Accessed August 23, 2020. [Google Scholar]
- 3.Coombe J, Kong FYS, Bittleston H, et al. Love during lockdown: findings from an online survey examining the impact of COVID-19 on the sexual practices of people living in Australia. Sex Transm Infect 2020. [epub ahead of print]. doi: 10.1136/sextrans-2020-054688. [DOI] [PubMed] [Google Scholar]
- 4.Hammoud MA, Maher L, Holt M, et al. Physical distancing due to COVID-19 disrupts sexual behaviours among gay and bisexual men in Australia: implications for trends in HIV and other sexually transmissible infections. J Acquir Immune Defic Syndr. 2020;85:309–315. [DOI] [PubMed] [Google Scholar]
- 5.Chow EPF, Hocking JS, Ong JJ, et al. Sexually transmitted infection diagnoses and access to a sexual health service before and after the national lockdown for COVID-19 in Melbourne, Australia. Open Forum Infect Dis. 2020:ofaa536. doi: 10.1093/ofid/ofaa536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hammoud MA, Grulich A, Holt M, et al. Substantial decline in use of HIV pre-exposure prophylaxis (PrEP) following introduction of COVID-19 physical distancing restrictions in Australia: results from a prospective observational study of gay and bisexual men. J Acquir Immune Defic Syndr. 2021;86:22–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Krakower D, Solleveld P, Levine K, et al. Impact of COVID-19 on HIV Preexposure Prophylaxis Care at a Boston Community Health Center. Paper presented at: 23rd International AIDS Conference 2020; Virtual.
- 8.Brawley S, Dinger J, Nguyen C, et al. Impact of COVID-19 Related Shelter-In-Place Orders on PrEP Access, Usage and HIV Risk Behaviors in the United States. Paper presented at: 23rd International AIDS Conference 2020; Virtual.
- 9.Chow EPF, Hocking JS, Ong JJ, et al. Changing the use of HIV pre-exposure prophylaxis Among men who have sex with men during the COVID-19 pandemic in Melbourne, Australia. Open Forum Infect Dis. 2020;7:ofaa275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Michaels J, Riley B, McGill S. Harm Reduction Approaches to Casual Sex during the COVID-19 Pandemic. Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM) COVID-19 Taskforce on HIV, Viral Hepatitis, and Sexual Health. 2020. Available at: https://ashm.org.au/covid-19/clinical-care/harm-minimisation-approaches-to-casual-sex/. Accessed October 30, 2020. [Google Scholar]
- 11.Terrence Higgins Trust. New Advice on Sex while Managing COVID-19 Risk Released. Terrence Higgins Trust; 2020. Available at: https://www.tht.org.uk/news/new-advice-sex-while-managing-covid-19-risk-released. Accessed August 23, 2020. [Google Scholar]
- 12.Carvalheira A, Gomes FA. Cybersex in Portuguese chatrooms: a study of sexual behaviors related to online sex. J Sex Marital Ther. 2003;29:345–360. [DOI] [PubMed] [Google Scholar]
- 13.Kuzmanovic D. Queer race play: kinky sex and the trauma of racism. Interface Prob Boundar. 2018;91:71–88. [Google Scholar]
- 14.Walker S, Bellhouse C, Fairley CK, et al. Pharyngeal gonorrhoea: the willingness of Australian men who have sex with men to change current sexual practices to reduce their risk of transmission-A qualitative study. PLoS One. 2016;11:e0164033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chow EPF, Hocking JS, Ong JJ, et al. Postexposure prophylaxis during COVID-19 lockdown in Melbourne, Australia. Lancet HIV. 2020;7:e528–e529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Junejo M, Girometti N, McOwan A, et al. HIV postexposure prophylaxis during COVID-19. Lancet HIV. 2020;7:e460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sanchez-Rubio J, Velez-Diaz-Pallares M, Rodriguez Gonzalez C, et al. HIV postexposure prophylaxis during the COVID-19 pandemic: experience from Madrid. Sex Transm Infect. 2020. [epub ahead of print]. doi: 10.1136/sextrans-2020-054680. [DOI] [PubMed] [Google Scholar]
- 18.Lehmiller JJ, Garcia JR, Gesselman AN, et al. Less sex, but more sexual diversity: changes in sexual behavior during the COVID-19 coronavirus pandemic. Leis Sci. 2020:1–10 [epub ahead of print]. doi: 10.1080/01490400.2020.1774016. [DOI] [Google Scholar]
- 19.Cusini M, Benardon S, Vidoni G, et al. Trend of main STIs during COVID-19 pandemic in Milan, Italy. Sex Transm Infect. 2020. [epub ahead of print]. doi: 10.1136/sextrans-2020-054608. [DOI] [PubMed] [Google Scholar]
- 20.Latini A, Magri F, Dona MG, et al. Is COVID-19 affecting the epidemiology of STIs? The experience of syphilis in Rome. Sex Transm Infect. 2020. [epub ahead of print]. doi: 10.1136/sextrans-2020-054543. [DOI] [PubMed] [Google Scholar]
- 21.Jiang H, Zhou Y, Tang W. Maintaining HIV care during the COVID-19 pandemic. Lancet HIV. 2020;7:e308–e309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ponticiello M, Mwanga-Amumpaire J, Tushemereirwe P, et al. Everything is a mess: how COVID-19 is impacting engagement with HIV testing services in rural southwestern Uganda. AIDS Behav. 2020;24:3006–3009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jewell BL, Mudimu E, Stover J, et al. Potential effects of disruption to HIV programmes in sub-Saharan Africa caused by COVID-19: results from multiple mathematical models. Lancet HIV. 2020;7:e629–e640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Odinga M, Kuria S, Muindi O, et al. HIV testing amid COVID-19: community efforts to reach men who have sex with men in three Kenyan counties [version 2; peer review: 2 approved]. Gates Open Res. 2020;4:117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hogan AB, Jewell BL, Sherrard-Smith E, et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: a modelling study. Lancet Glob Health. 2020;8:e1132–e1141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Traeger MW, Schroeder SE, Wright EJ, et al. Effects of pre-exposure prophylaxis for the prevention of human immunodeficiency virus infection on sexual risk behavior in men who have sex with men: a systematic review and meta-analysis. Clin Infect Dis. 2018;67:676–686. [DOI] [PubMed] [Google Scholar]