

Abstract
Metformin is a biguanide that is used as first-line treatment of type 2 diabetes mellitus and is effective as monotherapy and in combination with other glucose-lowering medications. It is generally well-tolerated with minimal side effects and is affordable. Although the safety and efficacy of metformin have been well-established, there is discussion regarding whether metformin should continue to be the first choice for therapy as other anti-hyperglycemic medications exhibit additional advantages in certain populations. Despite a long-standing history of metformin use, there are limited cardiovascular outcomes data for metformin. Furthermore, the available studies fail to provide strong evidence due to either small sample size or short duration. Recent data from glucagon-like peptide-1 receptor agonist and sodium-glucose cotransporter-2 inhibitor cardiovascular and renal outcomes trials demonstrated additional protection from diabetes complications for some high-risk patients, which has impacted the guidelines for diabetes management. Post-hoc analyses comparing hazard ratios for participants taking metformin at baseline versus not taking metformin are inconclusive for these two groups. There are no data to suggest that metformin should not be initiated soon after the diagnosis of diabetes. Furthermore, the initiation of newer glycemic-lowering medications with cardiovascular benefits should be considered in high-risk patients regardless of glycemic control or target HbA1c. However, cost remains a major factor in determining appropriate treatment.
Keywords: first-line therapy, metformin, type 2 diabetes
Introduction
Metformin is a biguanide that is used as first-line treatment of type 2 diabetes mellitus and is effective as monotherapy and in combination with other glucose-lowering medications. It is generally well-tolerated with minimal side effects and is affordable.1 Although the safety and efficacy of metformin have been well-established, there is discussion regarding whether metformin should remain the first choice for therapy in all patients as other anti-hyperglycemic medications have proven to have additional benefits in certain populations. It is important to understand the risks and benefits of metformin and other anti-hyperglycemic medications before making any change in clinical practice.
Historical overview of metformin
Chemical origins of metformin
Guanidine-based remedies were originally derived from the perennial plant Galega officinalis (Figure 1A) and have been used medicinally for centuries.2 Commonly known as Goat’s Rue or French Lilac, the herb was used to treat frequent urination and increased thirst, symptoms now known to be associated with hyperglycemia.3 Of the common biguanide-based medications, including phenformin and buformin, metformin (dimethyl-biguanide, Figure 1B) eventually stood out for its comparative advantage in both safety and efficacy.
Figure 1.
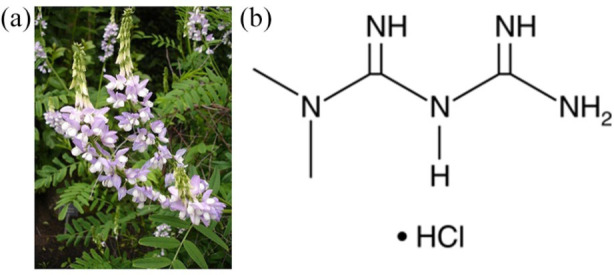
(A) Galega officinalis, commonly known as French lilac; it is rich in galegine, a substance with blood glucose-lowering activity and the foundation for the discovery of metformin. (B) The chemical structure of 1,1-dimethylbiguanide hydrochloride or metformin hydrochloride.
Rediscovery of dimethyl-biguanide
In the 1940s, metformin inadvertently gained recognition for its ability to lower blood glucose—an observation noted when used to treat influenza.4 In 1957, a French physician, Jean Sterne,5 published data which indicated metformin’s superior ability to safely lower blood-glucose levels. Within a year, metformin was prescribed in Europe for the treatment of type 2 diabetes mellitus, and Sterne dubbed the drug “glucophage” for its perceived ability to devour blood glucose.3
While metformin was gaining popularity in Europe, phenformin and buformin were still commonly prescribed for the treatment of diabetes.3 However, these drugs were removed from the market due to a considerable risk of lactic acidosis.6 Clinical trials between 1980 and 1998 focused on the safety and efficacy of metformin3 and showed a significantly lower risk of lactic acidosis compared with other biguanides while still providing meaningful therapeutic benefits.7 Given the available evidence at the time, the Food and Drug Administration (FDA) approved metformin for use in the United States in 1994, and by 1995 it was widely prescribed for the treatment of type 2 diabetes mellitus.8
Metformin in the 21st century
By the end of the 20th century, metformin’s ability to safely lower glucose levels in patients with diabetes had been well-documented on a global scale. In 2002, metformin became the most commonly prescribed oral anti-hyperglycemic medication.3 In 2005, the International Diabetes Foundation published guidelines recommending metformin as a first-line treatment for type 2 diabetes.9 Nearly 50 years after the rediscovery of metformin, the World Health Organization added metformin to its list of essential medications in 2011.10 Numerous clinical trials in the last decade have thoroughly assessed concerns regarding the risk of metformin-induced lactic acidosis in patients with comorbidities such as renal and hepatic dysfunction or congestive heart failure. Results from such trials continue to support metformin as a safe and effective medication for the vast majority of patients.11 In fact, the restriction for using metformin in patients with impaired kidney function has recently been relaxed.12
Metformin mechanism of action
Since metformin was discovered from a plant source and was not originally synthesized to bind to a specific target, some of its actions remain unknown. However, metformin has been shown to improve glycemic control through several mechanisms (Figure 2A). It inhibits hepatic gluconeogenesis, reduces absorption of glucose from the intestines and increases glucose uptake by tissue. One of metformin’s functions is via the non-competitive inhibition of the mitochondrial glycerophosphate dehydrogenase enzyme. The inhibition of this enzyme reduces hepatic gluconeogenesis by reducing the conversion of lactate and glycerol to glucose.13 Additionally, metformin diminishes mitochondrial complex I activity, resulting in decreased adenosine triphosphate and increased adenosine monophosphate content and activation of adenosine monophosphate-activated protein kinase (AMPK) as outlined in Figure 2B.14 AMPK is an enzyme that works as a fuel gauge that becomes activated in situations of energy consumption, resulting in inhibition of gluconeogenesis and increased fatty acid oxidation.14 A 2016 study suggested that most of metformin’s glucose-lowering action takes place in the gastrointestinal tract rather than in circulation.15 Studies have also shown that metformin alters the gut microbiome, increasing GLP-1 secretion and improving glucose homeostasis.16,17 Unlike some other glucose-lowering agents, metformin rarely causes hypoglycemia and is weight neutral.18
Figure 2.

(A) Metformin improves glycemia by inhibiting hepatic gluconeogenesis, reducing absorption of glucose from the intestines, promoting glucose uptake by tissue, and increasing GLP-1 secretion. Additional benefits of metformin include alterations in the gut microbiota, reduction in inflammation, and reductions in cancer and depression. Metformin has also been shown to improve longevity in caenorhabditis elegans (C. elegans). (B) Metformin diminishes mitochondrial complex I activity, resulting in decreased adenosine triphosphate (ATP) and increased adenosine monophosphate (AMP) content and activation of adenosine monophosphate-activated protein kinase (AMPK).
Adverse effects of metformin
Gastrointestinal
The most common side effects of metformin are nausea, diarrhea, and abdominal discomfort. Many patients (20–30%) report experiencing at least one of these side effects.19 The gastrointestinal side effects will be less impactful if metformin is taken with a meal and the dose is titrated gradually. Metformin therapy could be initiated at a low dose of 500 mg twice daily and increased by 500 mg daily every 1–2 weeks until the patient reaches the maximum tolerated dose. For those that are unable to tolerate the gastrointestinal (GI) side effects associated with the standard immediate-release formulation, extended-release tablets are available.1 While most patients either tolerate the side effects or switch to the slow-release option, approximately 5% discontinue the drug due to severe GI distress.16 The exact mechanisms of action which result in the common GI side effects are currently unknown. Possible mechanisms may be related to high concentrations of metformin within the GI tract, an increase in serotonin within GI cells, or metformin’s effect on the gut microbiome, leading to opportunistic infections.16,20 Furthermore, it has been proposed that an individual’s unique microbiome might influence metformin tolerance.17,20 Metformin’s relationship with the gut microbiome continues to be a topic of scientific interest.
Lactic acidosis
While the association between metformin and lactic acidosis is notably less significant compared with other biguanides, there is still a slight risk of developing lactic acidosis while taking metformin. Lactic acidosis affects 3–10 per 100,000 persons per year in patients taking metformin.21 Originally, it was thought that people with renal impairment could not take metformin due to an increased risk of developing this potentially lethal side effect. However, in 2016, the FDA deemed the drug safe for people with mild-to-moderate kidney impairment.22 Most current evidence suggests that even in patients with contraindications such as in renal, hepatic, or cardiac failure, lactic acidosis associated with metformin use is considered extremely rare.11
Vitamin B12 deficiency
Malabsorption of vitamin B12 is also linked to metformin use. Several studies have found low vitamin B12 levels in patients taking metformin.1 The major concern with this side effect is its possible association with irreversible neurological consequences.23 Low levels of vitamin B12 could potentially lead to an increased prevalence of peripheral neuropathy.23 As a precaution, regular testing of vitamin B12 levels in patients taking metformin has been suggested.23 In patients with low levels of vitamin B12, an oral supplement may be recommended.1
Metformin: clinical use in type 2 diabetes
Dosing
It has been reported that 500 mg daily of metformin was the minimum dose necessary to yield a clinically significant reduction in glycated hemoglobin (HbA1c) with a mean reduction of 0.9%.24 While 2500 mg is considered the maximum dose of metformin, most providers will prescribe up to 2000 mg daily because increasing the dose from 2000 mg to 2500 mg had minimal impact on HbA1c with a slight increase in adverse events.24 A recent study showed that optimizing metformin to the 2000 mg daily or the maximum tolerated lower dose improves glycemia in type 2 diabetes,25 confirming that the efficacy of metformin is dose dependent.
Metformin and glycemic control
Metformin monotherapy has been shown to decrease mean HbA1c by 1.3%, compared with a 0.4% increase in the placebo group after 29 weeks.8 The United Kingdom Prospective Diabetes Study (UKPDS) not only found a greater improvement in glycemic control in patients taking metformin compared with the conventional treatment arm but also showed that metformin therapy resulted in a reduction in hypoglycemic events and weight gain compared with sulfonylureas and insulin.26
A Diabetes Outcome Progression Trial, comparing monotherapy of rosiglitazone, metformin, and glyburide in patients with newly-diagnosed diabetes, reported that 36% of subjects in the metformin group achieved an A1c <7% as compared with 40% in the rosiglitazone group, and only 26% in the glyburide group,27 suggesting that metformin’s glucose-lowering effects were superior to glyburide but not to rosiglitazone. It should be noted that concerns for adverse events such as edema, weight gain, heart failure, and fractures have led to a significant decrease in use of thiazolidinediones.28
There are few studies comparing metformin with newer anti-hyperglycemic agents. A recent study compared different doses of canagliflozin (100/300 mg) with metformin and combination therapy. While the results indicated that combination therapy was superior in glucose-lowering to the other treatment groups, both doses of the canagliflozin were found to be non-inferior to metformin. However, the canagliflozin groups achieved greater weight loss.29 This study suggests that there might be an additional benefit to choosing a sodium-glucose cotransporter-2 (SGLT-2) inhibitor as first-line therapy or considering combination therapy as initial treatment of type 2 diabetes in certain individuals.
Correlation between type 2 diabetes and cardiovascular disease
The primary goal in the treatment of type 2 diabetes is a reduction in the rate of development or progression of complications associated with diabetes. The risk of cardiovascular disease (CVD)-related death is two-to-four times greater in adults with diabetes compared with those without diabetes.30 Furthermore, over two-thirds of older adults with diabetes die from heart disease.30 While intensive glycemic control decreases the incidence and progression of microvascular complications, it has failed to show a significant reduction in macrovascular complications.26 However, long-term follow-up has suggested that intensive glycemic control early in diabetes treatment and prior to CVD onset can reduce future cardiovascular events; this is known as the legacy effect.31 Given the high risk of morbidity and mortality associated with cardiovascular disease, it is imperative to identify glycemic-lowering therapies that decrease the risk of atherosclerotic cardiovascular disease (ASCVD) while also properly treating comorbidities such as obesity, hypertension, and hyperlipidemia in these high-risk patients.
Cardiovascular effects of metformin
Despite a long-standing history of metformin use, there are limited cardiovascular outcomes data for metformin. Furthermore, the available studies fail to provide strong evidence due to either small sample size or short duration. This section outlines some of the clinical trials relevant to metformin and CVD.
The UKPDS suggested there might be cardiovascular benefits with metformin use. In that trial, 753 patients with newly diagnosed type 2 diabetes were assigned to usual care (diet, with sulfonylurea, insulin, and/or metformin added for marked hyperglycemia) or open-label metformin. Drug treatment was added in 44% of usual care patients. Compared with usual care, metformin was associated with fewer deaths [relative risk (RR) 0.64, p = 0.01] and myocardial infarctions (RR 0.61, p = 0.01) with non-significant reductions in stroke and peripheral artery disease events.26 However, the sample size was small, and the study was not powered to prove cardiovascular benefits of metformin.26 The UKPDS results, including glycemic-lowering efficacy, the weight benefits, the low risk for hypoglycemia, and the reduction in macrovascular complications, led to metformin becoming the preferred first-line therapy for treatment of type 2 diabetes. The 10-year follow-up of the UKPDS reported continued benefit after metformin therapy among overweight patients.31
Metformin therapy also showed a reduction in cardiovascular events compared with glipizide in the SPREAD-DIMCAD trial.32 While both groups achieved A1c targets, metformin therapy resulted in a 12% absolute risk reduction of major adverse cardiovascular events whereas the glipizide group experienced more episodes of hypoglycemia and weight gain compared with the metformin group.32
There have been several meta-analyses to investigate the effects of metformin on cardiovascular events, but data have not been particularly conclusive. A meta-analysis of 35 trials indicated lower cardiovascular morbidity and mortality with metformin than with placebo or no treatment (RR 0.79, p = 0.03).33 Another meta-analysis of 40 trials (including some with active comparators) indicated that metformin was associated with lower cardiovascular mortality [RR 0.74, 95% confidence interval (CI) 0.62–0.89].34 A third meta-analysis, involving 40 studies and more than one million patients with coronary artery disease, suggested that there was a significant reduction in cardiovascular mortality (RR 0.81, 95% CI 0.79–0.84) and major adverse cardiovascular event (MACE) rate (RR 0.83, 95% CI 0.78–0.89) with metformin.35 However, a meta-analysis of eight studies failed to show cardio-protective effects for metformin.36 Furthermore, a retrospective study of almost 25,000 Medicare patients showed that metformin did not significantly reduce the risk of death among patients with acute myocardial infarction in the past year.37
It should be noted that these are meta-analyses, and there are unmeasured confounders that may affect the outcomes. Unfortunately, there has never been and likely will never be a placebo-controlled cardiovascular outcomes trial with metformin in patients with type 2 diabetes. However, the ongoing VA-IMPACT trial will examine the effect of metformin on MACEs in individuals with pre-diabetes and established ASCVD.38
Cardiovascular outcomes trials for other glucose-lowering medications
Since the FDA issued guidelines for cardiovascular risk assessment in 2008,36 there are more data available on cardiovascular safety for novel glucose-lowering drugs. Most of these newer medications have been compared with placebo and added to the standard of care. In these cardiovascular outcomes trials, most patients were using metformin as background therapy.39 This section briefly reviews cardiovascular outcomes trials for these newer classes of medications. Table 1 reviews the hazard ratios for each of these trials.
Table 1.
A summary of CVOT results for GLP-1 RAs and SGLT-2 inhibitors including percentage of participants taking metformin at baseline and the HR for the primary endpoint in the entire cohort, in the subgroup taking metformin, and in the subgroup not taking metformin at baseline.
| Study name | Medication | Metformin at baseline (%) | HR |
||
|---|---|---|---|---|---|
| All | Metformin | No metformin | |||
| GLP-1 RAs | |||||
| ELIXA | Lixisenatide | 67 | 1.02 (0.89, 1.17) | Not reported | |
| LEADER | Liraglutide | 76 | 0.87 (0.78, 0.97) | 0.97 (0.85, 1.10) | 0.79 (0.64, 0.97) |
| HARMONY | Albiglutide | 73 | 0.78 (0.68, 0.90) | 0.77 (0.65, 0.92) | 0.79 (0.62, 1.00) |
| EXCEL | Weekly exenatide | 76 | 0.91 (0.83, 1.0) | Not reported | |
| REWIND | Dulaglutide | 81 | 0.88 (0.79–0.99) | Not reported | |
| SUSTAIN 6 | SQ semaglutide | 74 | 0.74 (0.58, 0.95) | Not reported | |
| PIONEER 6 | Oral semaglutide | 77 | 0.79 (0.57, 1.11) | Not reported | |
| SGLT-2 inhibitors | |||||
| EMPA-REG | Empagliflozin | 74 | 0.86 (0.74–0.99) | 0.92 (0.77–1.10) | 0.72 (0.56, 0.93) |
| CANVAS | Canagliflozin | 77 | 0.86 (0.75–0.97) | 0.91 (0.78–1.07) | 0.76 (0.61, 0.94) |
| DECLARE | Dapagliflozin | 82 | 0.83 (0.73, 0.95) | Not reported | |
| VERTIS CV | Ertugliflozin | 76 | 0.97 (0.85, 1.11) | 0.92 (0.79, 1.07) | 1.13 (0.87, 1.48) |
Studies of liraglutide, albiglutide, dulaglutide, subcutaneous semaglutide, empagliflozin, canagliflozin, and dapagliflozin showed a statistically significant reduction in the composite outcome of major cardiovascular events compared with placebo. Post-hoc analyses comparing metformin users and non-users at baseline were not significant for heterogeneity. However, the HRs suggested that there might be better cardio-protection for SGLT-2 inhibitors in those not taking metformin at baseline.
CVOT, Cardiovascular Outcomes Trials; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HR, hazard ratio; SGLT-2, sodium-glucose cotransporter-2; SQ, Subcutaneous.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs)
GLP-1 RAs are incretin mimetics that stimulate insulin secretion in a glucose-dependent manner, delay gastric emptying and suppress appetite.40,41 In addition to improving glycemic control, these medications also cause weight loss. Up to 50% of patients who take GLP-1 RAs experience nausea, vomiting, diarrhea, abdominal pain, or constipation.42 These symptoms are generally transient. Most medications in this class can be initiated at a lower dose and slowly titrated. Additionally, patients should be instructed to avoid eating large or high-fat meals to decrease the risk of more severe gastrointestinal symptoms. Despite these recommendations, 5–10% of patients discontinue GLP-1 RAs due to gastrointestinal side effects.43 Animal studies have also shown an increase in the risk of thyroid c-cell tumors,40,41 but this has not been seen in human studies. Most of the medications in this class are administered by subcutaneous injections. Four GLP-1 RAs have shown a statistically significant reduction in cardiovascular events compared with placebo.
ELIXA was the first cardiovascular outcomes trial for a GLP-1 RA. In 2015, this study showed that there was not a significantly different rate of cardiovascular events in patients treated with lixisenatide compared with placebo.44 In 2016, liraglutide became the first GLP-1 RA to show cardio-protection, with a relative risk reduction of 13% compared with placebo in the LEADER trial, which included over 9000 participants with established cardiovascular disease for a period of 4 years.45 Exenatide once weekly proved non-inferiority compared with placebo in its cardiovascular outcomes trial but failed to show superiority.46 Albiglutide was the second GLP-1 RA to show cardio-protection.47 However, the manufacturer chose to remove this medication from the market for economic reasons.48
The SUSTAIN-6 trial, with only 3000 participants and a 2-year follow-up period, was not powered to show superiority for subcutaneous semaglutide. However, subcutaneous semaglutide did show a statistically significant reduction in MACEs compared with placebo.49 The PIONEER-6 cardiovascular outcomes trial, with a median duration of approximately 16 months and just under 1600 participants, showed that oral semaglutide was non-inferior to placebo in the MACE rate.50 A much larger trial designed to determine whether semaglutide might offer cardio-protection is currently ongoing.51
The REWIND study was the first cardiovascular outcomes trial to enroll a majority of patients without a history of cardiovascular disease.52 In 2019, this study showed a 12% reduction in the risk of cardiovascular outcomes, suggesting that dulaglutide can be used as primary prevention for cardiovascular disease in patients with type 2 diabetes.52 Based on the results which were outlined in this section, subcutaneous semaglutide, liraglutide, and dulaglutide have been identified as preferred medications for people at high risk for cardiovascular disease.53
Secondary analyses of the GLP-1 RA cardiovascular outcomes trials revealed a potential reduction in renal outcomes for patients randomized to active study medication. The LEADER trial showed a reduction in renal outcomes for patients randomized to liraglutide, which was driven by a reduction in the onset of macroalbuminuria.54 Results were similar for dulaglutide in the REWIND trial.55 The FLOW study, with composite renal outcomes as the primary endpoint for subcutaneous semaglutide versus placebo, is ongoing.56
SGLT-2 inhibitors
SGLT-2 inhibitors prevent glucose reabsorption in the kidneys, causing glucosuria and leading to a reduction in plasma glucose in patients with diabetes. Since excess glucose is excreted in the urine, SGLT-2 inhibitor use is also associated with weight loss. Less than 10% of patients taking SGLT-2 inhibitors develop genital infections, which was 2–3 times more than placebo in clinical trials.57 The risk is higher in women and in people with a history of genitourinary infections. Rare but serious side effects include ketoacidosis, fractures, foot amputations, and genital infections.58–64 People at high risk for these serious adverse events should avoid SGLT-2 inhibitors.
The EMPA-REG OUTCOME study established empagliflozin as the first SGLT-2 inhibitor known to reduce cardiovascular events. The 14% reduction in composite primary outcome was driven by a 38% reduction in cardiovascular death; this study also showed a 35% relative risk reduction for heart failure hospitalizations.65 In 2017, CANVAS showed that canagliflozin was associated with a 14% relative reduction in the rate of MACEs compared with placebo and decreased the rate of hospitalizations for heart failure by 33%.66 Dapagliflozin was non-inferior but not superior to placebo in its cardiovascular outcomes trial.67 Similarly, data from the VERTIS trial were released at the 2020 American Diabetes Association Conference, showing cardiovascular safety, but not additional protection, when ertugliflozin is added to the standard of care.68
Secondary analyses of SGLT-2 inhibitor cardiovascular outcomes trials showed a reduction in hospitalizations for heart failure as a likely class effect independent of the diagnosis of diabetes. In 2019, dapagliflozin was shown to reduce the rate of progression of heart failure or cardiovascular death compared with placebo in patients with and without diabetes.69 Additionally, the CREDENCE study showed a 30% relative risk reduction for the primary composite renal outcome (end-stage renal disease, doubling of serum creatinine levels, and renal or cardiovascular death) with canagliflozin compared with placebo.70
Dipeptidyl peptidase IV (DPP-IV) inhibitors
DPP-IV inhibitors increase insulin release by prolonging the life of incretins such as GLP-1 and glucose-dependent insulinotropic polypeptide (GIP).71 Cardiovascular outcomes trials for saxagliptin,72 alogliptin,73 sitagliptin,74 and linagliptin75 all showed non-inferiority but failed to show superiority compared with placebo. Additionally, there was an increase in rates of hospitalization for heart failure with saxagliptin.72
American Diabetes Association (ADA) standards of care guidelines
In 2008, the first ADA and European Association of the Study of Diabetes (EASD) consensus guidelines on management of hyperglycemia in patients with type 2 diabetes stated that metformin, along with lifestyle interventions, should be used as first-line therapy.76 While the guidelines of pharmacologic treatment for type 2 diabetes in the United States have largely remained the same, recent updates in 2019 and 2020 have added additional components in light of compelling data from cardiovascular and renal outcomes trials. According to the ADA 2020 Standards of Medical Care in Diabetes, metformin remains the preferred first-line pharmacologic treatment for type 2 diabetes unless contraindicated or not tolerated by the patient.53 Other glucose-lowering agents may be added to metformin considering patient preferences, hypoglycemic risk, and comorbidities.53
While the ADA still recommends metformin as first-line therapy, the updated Standards of Care have become more outcomes-focused rather than solely concentrating on glycemic control. For this reason, in patients with certain comorbidities such as high-risk for or established ASCVD, heart failure or chronic kidney disease, it is recommended to consider GLP-1 RAs and SGLT-2 inhibitors independently of baseline HbA1c or individualized HbA1c target.77 In 2019, the European Society of Cardiology, in collaboration with the EASD, went one step further in altering their treatment guidelines. SGLT-2 inhibitors and GLP-1 RAs are now recommended as first-line therapy for patients with established ASCVD or high cardiovascular risk in Europe.78 Metformin should be considered as the first line in patients without CVD and at moderate cardiovascular risk.78
The future role of metformin
The current debate is whether to start patients with high risk of CVD on metformin then add one of the cardio-protective medications independent of their glycemia or bypass metformin and go straight to the newer diabetes medications with proven cardiovascular benefits. To answer this question, one should ponder whether metformin has any additional benefits beyond the glycemic lowering effects or whether the cardio-protective effects of the newer glycemic lowering medications such as SGLT-2 inhibitors and GLP-1 RAs are modified by using metformin as background treatment.
Additional benefits of metformin
Clinical use of metformin changed from influenza treatment to diabetes management and continues to evolve in the modern era. Recent clinical trials have shown promise for numerous other indications (Figure 2A). There are data that suggest that metformin can alter the inflammatory response79–82 to protect cells from damage.83,84 Furthermore, metformin has been shown to improve longevity in caenorhabditis elegans.85,86 The role of metformin in aging is currently being investigated in humans.87 Through epidemiological meta-analysis, metformin has been associated with a decrease in the risk of breast, colon, liver, pancreatic, prostate, endometrial, and lung cancer.88 Improvements in cognitive function89–91 and depressive symptoms92,93 have also been associated with metformin use. Ongoing clinical trials such as DEMFOS, VA-IMPACT, TAME, and ePREDICE are aimed to evaluate the additional benefits of metformin for people without diabetes.38,94–97 If these trials confirm added benefits for metformin, it will make a strong argument for keeping metformin as the first line of therapy.
Background metformin use and cardio-protection
Although most of the cardiovascular outcomes trials compared the newer glycemic-lowering agent with placebo, the majority of subjects were on background therapy of metformin.39 Therefore, the beneficial effects of SGLT-2 inhibitors and GLP-1 RAs have been observed mostly in combination with metformin. There have been post-hoc analyses to investigate whether metformin modifies the cardio-protective effects of the newer glycemic lowering medications. A 2017 meta-analysis of DPP-IV inhibitor cardiovascular outcomes studies showed a non-statistically significant correlation between baseline metformin use and reduction in cardiovascular outcomes for patients randomized to DPP-IV inhibitors.98 It was hypothesized that the added benefit might be due to the fact that metformin increases GLP-1 secretion and DPP-IV inhibitors inhibit the degradation of this endogenous enzyme.
Table 1 summarizes the available data on subgroup analyses comparing metformin users and non-users at baseline for SGLT-2 inhibitors and GLP-1 RAs trials. Although some show differences in the hazard ratios between metformin users versus non-users, the analysis for heterogeneity or treatment by subgroup interaction did not reach statistical significance, suggesting that the presence of metformin for the cardio-protective effects is not required.
The post-hoc analysis of the LEADER trial (76% used metformin at baseline) reported that liraglutide cardio-protective benefits were more prominent among baseline metformin non-users.99 In contrast, the HARMONY trial (73% used metformin at baseline) showed that albiglutide cardio-protection was significant in metformin users (Table 1).47
Among SGLT-2 inhibitors, hazard ratios in EMPA-REG and CANVAS studies suggested that cardio-protective effects might be driven by benefit seen in those not taking metformin at baseline. However, the VERTIS trial did not confirm this finding. Overall, further analysis showed that background metformin use is not necessary to reap the cardiovascular benefits of SGLT-2 inhibitors.100,101 Further post-hoc analyses of SGLT-2 inhibitors and GLP-1 RAs are underway to investigate whether background metformin treatment modifies the cardiovascular benefits of GLP-1 RAs or SGLT-2 inhibitors. It should be noted that there were other baseline variables such as estimated glomerular filtration rate that differed between the two groups which need to be adjusted in future analyses.
Conclusion
Since metformin was approved by the FDA in 1994 it has quickly risen to front-line therapy for the treatment of type 2 diabetes mellitus. Metformin has been associated with improvement in glycemic control, weight neutrality, and low cost as well as low risk for hypoglycemia.26 However, recent GLP-1 RA and SGLT-2 inhibitor outcomes trials have impacted the guidelines for diabetes management.
Appropriately, diabetes management has recently become more outcomes-focused, shifting from concentrating exclusively on glycemic control to considering the impact these medications have on complications from diabetes. Results from cardiovascular and renal outcomes trials are already influencing current guidelines. The ADA Standards of Care still recommends metformin as first-line therapy while considering GLP-1 RAs and SGLT-2 inhibitors independently of baseline HbA1c in high-risk patients. Alternatively, the EASD recently recommended considering GLP-1 RAs and SGLT-2 inhibitors as the first line for patients who have certain comorbidities, such as cardiovascular and renal disease. The difference in the optimal diabetes treatment in high-risk, drug-naïve patients will not resolve until we have more data from a head-to-head trial comparing metformin with newer glycemic-lowering medications or conclusive evidence from previous cardiovascular outcomes trials suggesting that metformin mitigates the beneficial effects of GLP-1 RAs and SGLT-2 inhibitors.
While they might seem different, the two guidelines are actually similar in recommending diabetes medications with beneficial cardiovascular effects for certain high-risk patients as early as possible. Despite the current recommendations, there is still only a small portion of eligible patients who are receiving these cardio-protective medications,102 probably due to cost and clinical inertia. Our focus should be on expanding the use of optimal medication with cardiovascular benefits.
In summary, there are no data to suggest that metformin should not be initiated soon after the diagnosis of diabetes. Furthermore, the initiation of newer glycemic-lowering medications with cardiovascular benefits should be considered in high-risk patients regardless of glycemic control or target HbA1c, yet cost remains a major factor in determining appropriate treatment.
Footnotes
Author contributions: Chelsea Baker: Conceptualization, Formal analysis, Investigation, Project administration, Supervision, Visualization, Writing-original draft, Writing-review & editing.
Cimmaron Retzik-Stahr: Conceptualization, Formal analysis, Investigation, Writing-original draft, Writing-review & editing.
Vatsala Singh: Conceptualization, Formal analysis, Investigation, Writing-original draft, Writing-review & editing.
Renee Plomondon: Conceptualization, Formal analysis, Investigation, Writing-original draft, Writing-review & editing.
Victoria Anderson: Formal analysis, Investigation, Writing-original draft, Writing-review & editing.
Neda Rasouli: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing-original draft, Writing-review & editing.
Conflict of interest statement: Neda Rasouli has received research funding and served as a site PI for clinical trials funded by Novo Nordisk, Allergan, Boehringer Ingleheim, Rhythm Pharmaceuticals, and Eli Lilly and has served as a consultant for Novo Nordisk in the past 12 months.
Funding: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Colorado CTSI grant (UL1TR002535).
ORCID iD: Chelsea Baker  https://orcid.org/0000-0002-9807-7115
https://orcid.org/0000-0002-9807-7115
Contributor Information
Chelsea Baker, Department of Medicine, University of Colorado Anschutz Medical Campus, 12401 E. 17th Ave.; Room 353, Aurora, CO 80045, USA.
Cimmaron Retzik-Stahr, Department of Medicine, University of Colorado School of Medicine and Rocky Mountain Regional VA Medical Center, Aurora, CO, USA.
Vatsala Singh, Department of Medicine, University of Colorado School of Medicine and Rocky Mountain Regional VA Medical Center, Aurora, CO, USA.
Renee Plomondon, Department of Medicine, University of Colorado School of Medicine and Rocky Mountain Regional VA Medical Center, Aurora, CO, USA.
Victoria Anderson, Department of Medicine, University of Colorado School of Medicine and Rocky Mountain Regional VA Medical Center, Aurora, CO, USA.
Neda Rasouli, Department of Medicine, University of Colorado and Division of Endocrinology, University of Colorado School of Medicine and Rocky Mountain Regional VA Medical Center, Aurora, CO, USA.
References
- 1. Sanchez-Rangel E, Inzucchi SE. Metformin: clinical use in type 2 diabetes. Diabetologia 2017; 60: 1586–1593. [DOI] [PubMed] [Google Scholar]
- 2. Bailey CJ, Day C. Metformin: its botanical background. Pract Diabetes Int 2004; 21: 115–117. [Google Scholar]
- 3. Bailey CJ. Metformin: historical overview. Diabetologia 2017; 60: 1566–1576. [DOI] [PubMed] [Google Scholar]
- 4. Garcia EY. Flumamine, a new synthetic analgesic and anti-flu drug. J Philipp Med Assoc 1950; 26: 287–293. [PubMed] [Google Scholar]
- 5. Sterne J. Blood sugar-lowering effect of 1,1-dimethylbiguanide. Therapie 1958; 13: 650–659. [PubMed] [Google Scholar]
- 6. Nattrass M, Alberti KG. Biguanides. Diabetologia 1978; 14: 71–74. [DOI] [PubMed] [Google Scholar]
- 7. Howlett HC, Bailey CJ. A risk-benefit assessment of metformin in type 2 diabetes mellitus. Drug Saf 1999; 20: 489–503. [DOI] [PubMed] [Google Scholar]
- 8. DeFronzo RA, Goodman AM. Efficacy of metformin in patients with non-insulin-dependent diabetes mellitus. The Multicenter Metformin Study Group. N Engl J Med 1995; 333: 541–549. [DOI] [PubMed] [Google Scholar]
- 9. IDF Clinical Guidelines Task Force. Global guideline for type 2 diabetes: recommendations for standard, comprehensive, and minimal care. Diabet Med 2006; 23: 579–593. [DOI] [PubMed] [Google Scholar]
- 10. World Health Organization. WHO model list of essential medications, https://apps.who.int/iris/bitstream/handle/10665/70640/a95053_eng.pdf?sequence=1 (2011, accessed 14 April 2020).
- 11. Tahrani AA, Varughese GI, Scarpello JH, et al. Metformin, heart failure, and lactic acidosis: is metformin absolutely contraindicated? BMJ 2007; 335: 508–512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Inzucchi SE, Lipska KJ, Mayo H, et al. Metformin in patients with type 2 diabetes and kidney disease: a systematic review. JAMA 2014; 312: 2668–2675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Madiraju AK, Erion DM, Rahimi Y, et al. Metformin suppresses gluconeogenesis by inhibiting mitochondrial glycerophosphate dehydrogenase. Nature 2014; 510: 542–546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Zhou G, Myers R, Li Y, et al. Role of AMP-activated protein kinase in mechanism of metformin action. J Clin Invest 2001; 108: 1167–1174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Buse JB, DeFronzo RA, Rosenstock J, et al. The primary glucose-lowering effect of metformin resides in the gut, not the circulation: results from short-term pharmacokinetic and 12-week dose-ranging studies. Diabetes Care 2016; 39: 198–205. [DOI] [PubMed] [Google Scholar]
- 16. Rena G, Hardie DG, Pearson ER. The mechanisms of action of metformin. Diabetologia 2017; 60: 1577–1585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Vallianou NG, Stratigou T, Tsagarakis S. Metformin and gut microbiota: their interactions and their impact on diabetes. Hormones (Athens) 2019; 18: 141–144. [DOI] [PubMed] [Google Scholar]
- 18. Food and Drug Administration. Glucophage, https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/020357s037s039,021202s021s023lbl.pdf (2017, accessed 11 June 2020).
- 19. Kirpichnikov D, McFarlane SI, Sowers JR. Metformin: an update. Ann Intern Med 2002; 137: 25–33. [DOI] [PubMed] [Google Scholar]
- 20. Elbere I, Kalnina I, Silamikelis I, et al. Association of metformin administration with gut microbiome dysbiosis in healthy volunteers. PLoS One 2018; 13: e0204317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Chan NN, Brain HP, Feher MD. Metformin-associated lactic acidosis: a rare or very rare clinical entity? Diabet Med 1999; 16: 273–281. [DOI] [PubMed] [Google Scholar]
- 22. Lipska KJ, Flory JH, Hennessy S, et al. Citizen petition to the US Food and Drug Administration to change prescribing guidelines: the metformin experience. Circulation 2016; 134: 1405–1408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Aroda VR, Edelstein SL, Goldberg RB, et al. Long-term metformin use and vitamin B12 deficiency in the diabetes prevention program outcomes study. J Clin Endocrinol Metab 2016; 101: 1754–1761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Garber AJ, Duncan TG, Goodman AM, et al. Efficacy of metformin in type II diabetes: results of a double-blind, placebo-controlled, dose-response trial. Am J Med 1997; 103: 491–497. [DOI] [PubMed] [Google Scholar]
- 25. Sivitz WI, Phillips LS, Wexler DJ, et al. Optimization of metformin in the GRADE cohort: effect on glycemia and body weight. Diabetes Care 2020; 43: 940–947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352: 854–865. [PubMed] [Google Scholar]
- 27. Kahn SE, Haffner SM, Heise MA, et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med 2006; 355: 2427–2443. [DOI] [PubMed] [Google Scholar]
- 28. Lexicomp. Rosiglitazone: drug information, https://www.uptodate.com/contents/rosiglitazone-drug-information?search=rosiglitazone&usage_type=panel&kp_tab=drug_general&source=panel_search_result&selectedTitle=1~68&display_rank=1 (2020, accessed 27 July 2020).
- 29. Rosenstock J, Chuck L, Gonzalez-Ortiz M, et al. Initial combination therapy with canagliflozin plus metformin versus each component as monotherapy for drug-naive type 2 diabetes. Diabetes Care 2016; 39: 353–362. [DOI] [PubMed] [Google Scholar]
- 30. American Heart Association. Cardiovascular disease and diabetes, https://www.heart.org/en/health-topics/diabetes/why-diabetes-matters/cardiovascular-disease–diabetes (2015, accessed 22 July 2020).
- 31. Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008; 359: 1577–1589. [DOI] [PubMed] [Google Scholar]
- 32. Hong J, Zhang Y, Lai S, et al. Effects of metformin versus glipizide on cardiovascular outcomes in patients with type 2 diabetes and coronary artery disease. Diabetes Care 2013; 36: 1304–1311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Lamanna C, Monami M, Marchionni N, et al. Effect of metformin on cardiovascular events and mortality: a meta-analysis of randomized clinical trials. Diabetes Obes Metab 2011; 13: 221–228. [DOI] [PubMed] [Google Scholar]
- 34. Selvin E, Bolen S, Yeh HC, et al. Cardiovascular outcomes in trials of oral diabetes medications: a systematic review. Arch Intern Med 2008; 168: 2070–2080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Han Y, Xie H, Liu Y, et al. Effect of metformin on all-cause and cardiovascular mortality in patients with coronary artery diseases: a systematic review and an updated meta-analysis. Cardiovasc Diabetol 2019; 18: 96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Griffin SJ, Leaver JK, Irving GJ. Impact of metformin on cardiovascular disease: a meta-analysis of randomised trials among people with type 2 diabetes. Diabetologia 2017; 60: 1620–1629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Inzucchi SE, Masoudi FA, Wang Y, et al. Insulin-sensitizing antihyperglycemic drugs and mortality after acute myocardial infarction: insights from the National Heart Care Project. Diabetes Care 2005; 28: 1680–1689. [DOI] [PubMed] [Google Scholar]
- 38. U.S. National Library of Medicine. Investigation of metformin in pre-diabetes on atherosclerotic cardiovascular outcomes, https://ClinicalTrials.gov/show/NCT02915198 (2020, accessed 30 July 2020)
- 39. Harrington JL, de Albuquerque Rocha N, Patel KV, et al. Should metformin remain first-line medical therapy for patients with type 2 diabetes mellitus and atherosclerotic cardiovascular disease? An alternative approach. Curr Diab Rep 2018; 18: 64. [DOI] [PubMed] [Google Scholar]
- 40. Koliaki C, Doupis J. Incretin-based therapy: a powerful and promising weapon in the treatment of type 2 diabetes mellitus. Diabetes Ther 2011; 2: 101–121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Nauck MA, Kleine N, Orskov C, et al. Normalization of fasting hyperglycaemia by exogenous glucagon-like peptide 1 (7-36 amide) in type 2 (non-insulin-dependent) diabetic patients. Diabetologia 1993; 36: 741–744. [DOI] [PubMed] [Google Scholar]
- 42. Shyangdan DS, Royle P, Clar C, et al. Glucagon-like peptide analogues for type 2 diabetes mellitus. Cochrane Database Syst Rev 2011; 2011: CD006423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Sikirica MV, Martin AA, Wood R, et al. Reasons for discontinuation of GLP1 receptor agonists: data from a real-world cross-sectional survey of physicians and their patients with type 2 diabetes. Diabetes Metab Syndr Obes 2017; 10: 403–412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Pfeffer MA, Claggett B, Diaz R, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 2015; 373: 2247–2257. [DOI] [PubMed] [Google Scholar]
- 45. Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016; 375: 311–322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Holman RR, Bethel MA, Mentz RJ, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med 2017; 377: 1228–1239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Hernandez AF, Green JB, Janmohamed S, et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (harmony outcomes): a double-blind, randomised placebo-controlled trial. Lancet 2018; 392: 1519–1529. [DOI] [PubMed] [Google Scholar]
- 48. S&P Global. GlaxoSmithKline publishes new data for discontinued diabetes drug, https://www.spglobal.com/marketintelligence/en/news-insights/trending/uht9tdwaawg6kn6xg_nf1w2 (2018, accessed 30 July 2020).
- 49. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016; 375: 1834–1844. [DOI] [PubMed] [Google Scholar]
- 50. Husain M, Birkenfeld AL, Donsmark M, et al. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2019; 381: 841–851. [DOI] [PubMed] [Google Scholar]
- 51. ClinicalTrials.gov. A heart disease study of semaglutide in patients with type 2 diabetes (SOUL), https://clinicaltrials.gov/ct2/show/NCT03914326 (2019, accessed 13 August 2020).
- 52. Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet 2019; 394: 121–130. [DOI] [PubMed] [Google Scholar]
- 53. American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes—2020. Diabetes Care 2020; 43(Suppl. 1): S98–S110. [DOI] [PubMed] [Google Scholar]
- 54. Mann JFE, Orsted DD, Brown-Frandsen K, et al. Liraglutide and renal outcomes in type 2 diabetes. N Engl J Med 2017; 377: 839–848. [DOI] [PubMed] [Google Scholar]
- 55. Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and renal outcomes in type 2 diabetes: an exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet 2019; 394: 131–138. [DOI] [PubMed] [Google Scholar]
- 56. ClinicalTrials.gov. A research study to see how semaglutide works compared to placebo in people with type 2 diabetes and chronic kidney disease (FLOW), https://clinicaltrials.gov/ct2/show/NCT03819153 (2019, accessed 30 June 2020).
- 57. Li D, Wang T, Shen S, et al. Urinary tract and genital infections in patients with type 2 diabetes treated with sodium-glucose co-transporter 2 inhibitors: a meta-analysis of randomized controlled trials. Diabetes Obes Metab 2017; 19: 348–355. [DOI] [PubMed] [Google Scholar]
- 58. Kumar S, Costello AJ, Colman PG. Fournier’s gangrene in a man on empagliflozin for treatment of Type 2 diabetes. Diabet Med 2017; 34: 1646–1648. [DOI] [PubMed] [Google Scholar]
- 59. Bersoff-Matcha SJ, Chamberlain C, Cao C, et al. Fournier gangrene associated with sodium-glucose cotransporter-2 inhibitors: a review of spontaneous postmarketing cases. Ann Intern Med 2019; 170: 764–769. [DOI] [PubMed] [Google Scholar]
- 60. Peters AL, Buschur EO, Buse JB, et al. Euglycemic diabetic ketoacidosis: a potential complication of treatment with sodium-glucose cotransporter 2 inhibition. Diabetes Care 2015; 38: 1687–1693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Musso G, Gambino R, Cassader M, et al. A novel approach to control hyperglycemia in type 2 diabetes: sodium glucose co-transport (SGLT) inhibitors: systematic review and meta-analysis of randomized trials. Ann Med 2012; 44: 375–393. [DOI] [PubMed] [Google Scholar]
- 62. Watts NB, Bilezikian JP, Usiskin K, et al. Effects of canagliflozin on fracture risk in patients with type 2 diabetes mellitus. J Clin Endocrinol Metab 2016; 101: 157–166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Ueda P, Svanström H, Melbye M, et al. Sodium glucose cotransporter 2 inhibitors and risk of serious adverse events: nationwide register based cohort study. BMJ 2018; 363: k4365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Chang HY, Singh S, Mansour O, et al. Association between sodium-glucose cotransporter 2 inhibitors and lower extremity amputation among patients with type 2 diabetes. JAMA Intern Med 2018; 178: 1190–1198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015; 373: 2117–2128. [DOI] [PubMed] [Google Scholar]
- 66. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017; 377: 644–657. [DOI] [PubMed] [Google Scholar]
- 67. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019; 380: 347–357. [DOI] [PubMed] [Google Scholar]
- 68. Cannon CP. Evaluation of ertugliflozin efficacy and safety cardiovascular outcomes trial—VERTIS CV, https://www.acc.org/latest-in-cardiology/clinical-trials/2020/06/16/11/24/vertis (2020, accessed 20 August 2020). [DOI] [PubMed]
- 69. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med 2019; 381: 1995–2008. [DOI] [PubMed] [Google Scholar]
- 70. Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 2019; 380: 2295–2306. [DOI] [PubMed] [Google Scholar]
- 71. Demuth HU, McIntosh CH, Pederson RA. Type 2 diabetes—therapy with dipeptidyl peptidase IV inhibitors. Biochim Biophys Acta 2005; 1751: 33–44. [DOI] [PubMed] [Google Scholar]
- 72. Scirica BM, Bhatt DL, Braunwald E, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 2013; 369: 1317–1326. [DOI] [PubMed] [Google Scholar]
- 73. White WB, Cannon CP, Heller SR, et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med 2013; 369: 1327–1335. [DOI] [PubMed] [Google Scholar]
- 74. Green JB, Bethel MA, Armstrong PW, et al. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med 2015; 373: 232–242. [DOI] [PubMed] [Google Scholar]
- 75. Rosenstock J, Perkovic V, Johansen OE, et al. Effect of linagliptin vs placebo on major cardiovascular events in adults with type 2 diabetes and high cardiovascular and renal risk: the CARMELINA randomized clinical trial. JAMA 2019; 321: 69–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Nathan DM, Buse JB, Davidson MB, et al. Management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the initiation and adjustment of therapy. Update regarding the thiazolidinediones. Diabetologia 2008; 51: 8–11. [DOI] [PubMed] [Google Scholar]
- 77. Buse JB, Wexler DJ, Tsapas A, et al. 2019 Update to: management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020; 43: 487–493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J 2020; 41: 255–323. [DOI] [PubMed] [Google Scholar]
- 79. Tamariz L, Hare JM. Inflammatory cytokines in heart failure: roles in aetiology and utility as biomarkers. Eur Heart J 2010; 31: 768–770. [DOI] [PubMed] [Google Scholar]
- 80. Saisho Y. Metformin and inflammation: its potential beyond glucose-lowering effect. Endocr Metab Immune Disord Drug Targets 2015; 15: 196–205. [DOI] [PubMed] [Google Scholar]
- 81. Mancini SJ, White AD, Bijland S, et al. Activation of AMP-activated protein kinase rapidly suppresses multiple pro-inflammatory pathways in adipocytes including IL-1 receptor-associated kinase-4 phosphorylation. Mol Cell Endocrinol 2017; 440: 44–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Moiseeva O, Deschênes-Simard X, St-Germain E, et al. Metformin inhibits the senescence-associated secretory phenotype by interfering with IKK/NF-κB activation. Aging Cell 2013; 12: 489–498. [DOI] [PubMed] [Google Scholar]
- 83. Algire C, Moiseeva O, Deschênes-Simard X, et al. Metformin reduces endogenous reactive oxygen species and associated DNA damage. Cancer Prev Res (Phila) 2012; 5: 536–543. [DOI] [PubMed] [Google Scholar]
- 84. Halicka HD, Zhao H, Li J, et al. Potential anti-aging agents suppress the level of constitutive mTOR- and DNA damage-signaling. Aging (Albany NY) 2012; 4: 952–965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Chen J, Ou Y, Li Y, et al. Metformin extends C. elegans lifespan through lysosomal pathway. Elife 2017; 6: e31268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Cabreiro F, Au C, Leung KY, et al. Metformin retards aging in C. elegans by altering microbial folate and methionine metabolism. Cell 2013; 153: 228–239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. ClinicalTrials.gov. Metformin in longevity study (MILES), https://clinicaltrials.gov/ct2/show/NCT02432287 (2018, accessed 26 August 2020).
- 88. Heckman-Stoddard BM, DeCensi A, Sahasrabuddhe VV, et al. Repurposing metformin for the prevention of cancer and cancer recurrence. Diabetologia 2017; 60: 1639–1647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Ng TP, Feng L, Yap KB, et al. Long-term metformin usage and cognitive function among older adults with diabetes. J Alzheimers Dis 2014; 41: 61–68. [DOI] [PubMed] [Google Scholar]
- 90. Hsu CC, Wahlqvist ML, Lee MS, et al. Incidence of dementia is increased in type 2 diabetes and reduced by the use of sulfonylureas and metformin. J Alzheimers Dis 2011; 24: 485–493. [DOI] [PubMed] [Google Scholar]
- 91. Cheng C, Lin CH, Tsai YW, et al. Type 2 diabetes and antidiabetic medications in relation to dementia diagnosis. J Gerontol A Biol Sci Med Sci 2014; 69: 1299–1305. [DOI] [PubMed] [Google Scholar]
- 92. Guo M, Mi J, Jiang QM, et al. Metformin may produce antidepressant effects through improvement of cognitive function among depressed patients with diabetes mellitus. Clin Exp Pharmacol Physiol 2014; 41: 650–656. [DOI] [PubMed] [Google Scholar]
- 93. Wang CP, Lorenzo C, Habib SL, et al. Differential effects of metformin on age related comorbidities in older men with type 2 diabetes. J Diabetes Complications 2017; 31: 679–686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Du Q, Wang YJ, Yang S, et al. A systematic review and meta-analysis of randomized controlled trials comparing pioglitazone versus metformin in the treatment of polycystic ovary syndrome. Curr Med Res Opin 2012; 28: 723–730. [DOI] [PubMed] [Google Scholar]
- 95. Barzilai N, Crandall JP, Kritchevsky SB, et al. Metformin as a tool to target aging. Cell Metab 2016; 23: 1060–1065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. ClinicalTrials.gov. Diet and exercise plus metformin to treat frailty in obese seniors (DEMFOS), https://ClinicalTrials.gov/show/NCT04221750 (2020, accessed 22 July 2020).
- 97. ClinicalTrials.gov. Prevention of microvascular complications in prediabetes e-PREDICE study (ePREDICE), https://ClinicalTrials.gov/show/NCT03222765 (2017, accessed 22 July 2020).
- 98. Crowley MJ, Williams JW, Kosinski AS, et al. Metformin use may moderate the effect of DPP-4 inhibitors on cardiovascular outcomes, https://care.diabetesjournals.org/content/40/12/1787 (2017, accessed 30 June 2020). [DOI] [PubMed]
- 99. Crowley MJ, McGuire DK, Alexopoulos A-S, et al. Effects of liraglutide on cardiovascular outcomes in type 2 diabetes patients with and without baseline metformin use: post hoc analyses of the LEADER trial. Diabetes Care 2020; 43: e108–e110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Inzucchi SE, Fitchett D, Jurisic-Erzen D, et al. Are the cardiovascular and kidney benefits of empagliflozin influenced by baseline glucose-lowering therapy? Diabetes Obes Metab 2020; 22: 631–639. [DOI] [PubMed] [Google Scholar]
- 101. Docherty K, Inzucchi SE, Kosiborod MN, et al. 1112-P: does background T2D therapy modify the benefits of dapagliflozin in heart failure? Analysis of the DAPA-HF trial. Diabetes 2020; 69(Suppl. 1): 1112-P. [Google Scholar]
- 102. McCoy RG, Dykhoff HJ, Sangaralingham L, et al. Adoption of new glucose-lowering medications in the U.S.—the case of SGLT2 inhibitors: nationwide cohort study. Diabetes Technol Ther 2019; 21: 702–712. [DOI] [PMC free article] [PubMed] [Google Scholar]