

Abstract
Objectives. To examine whether lethal means counseling and provision of cable locks prompt safe firearm storage relative to control among firearm-owning members of the Mississippi National Guard.
Methods. This randomized controlled trial utilized a 2 × 2 factorial design (lethal means counseling vs control, provision of cable locks vs no cable locks). Follow-up assessments took place at 3 and 6 months after baseline. Data were collected (n = 232; 87.5% male; mean age = 35.01 years; 77.2% White) from February 2018 through July 2020.
Results. Relative to control, lethal means counseling and provision of cable locks resulted in greater adoption of several safe storage methods over time. Lethal means counseling outperformed control (3 months: 55.0% vs 39.0%; odds ratio [OR] = 1.91). Cable locks outperformed control at 3 and 6 months on number of storage methods (1.41 vs 1.11; d = 0.29 and 1.34 vs 1.16; d = 0.15, respectively) and locking devices (59.8% vs 29.9%; OR = 3.49 and 58.4% vs 35.8%; OR = 2.52, respectively)
Conclusions. Lethal means counseling and cable locks can result in sustained changes in firearm storage.
Public Health Implications. The military may benefit from lethal means counseling, perhaps administering at point of entry.
Trial Registration. Clinical Trials.gov identifier: NCT03375099.
Firearms account for the majority of US suicides1 and more than 60% of military suicides.2 Suicide mortality is higher in homes with a firearm,3 and statewide firearm ownership rates are correlated with suicide rates even after controlling for other risk factors.4–9 Suicide risk associated with firearm availability may be reduced when firearms are stored safely, however.10,11 Safe firearm storage may be promoted with lethal means counseling, which involves discussing ways to limit an individual’s access to specific methods for suicide. Although lethal means counseling is a recommended best practice for suicide prevention,12 research on its acceptability and effectiveness is limited.13 Preliminary evidence suggests lethal means counseling delivered in an emergency department increases the likelihood that parents of suicidal adolescents will restrict access to suicide methods.14,15 Because 90% of suicide attempts with firearms are fatal,16 lethal means counseling cannot only be offered after a suicidal crisis has emerged, as this would result in many high-risk individuals not being exposed to the intervention. Supporting this perspective is research suggesting that the benefits of safe firearm storage may be most pronounced among individuals without a known mental illness and with low suicidal intent.10
Within the military, a preventive approach may be especially important because military personnel are more likely to own firearms17 but the majority do not use safe storage methods.18–20 Military personnel are also more likely to use firearms when attempting suicide.21,22 Acutely suicidal military personnel are prone to unsafely storing firearms,19 underreporting suicidal thoughts to military or civilian sources,23,24 and failing to disclose access to a firearm.25 Encouraging safe storage among all firearm-owning military personnel, regardless of acute suicide risk level, is therefore critical. The effectiveness of lethal means counseling and related strategies (e.g., distributing cable locks) as a preventive strategy among military personnel remains unknown. The primary aims of the present study were to examine if lethal means counseling and distribution of cable locks increase the use of safe storage practices in a community sample of firearm-owning military personnel. Using a 2 × 2 factorial design, we randomized firearm-owning US National Guard service members to receive lethal means counseling, cable locks, or both. We assessed firearm storage practices 3 and 6 months after baseline. We anticipated that participants who received lethal means counseling or cable locks would exhibit increased safe storage behaviors during follow-up.
METHODS
Participants were 232 firearm-owning members of the Mississippi National Guard. Service members were recruited via online advertising and in person at military-sponsored and community events. To minimize selection bias, the study—titled “Project Safe Guard”—was advertised as a “health and home safety” study. Service members filled out a screening questionnaire to assess eligibility. Those reporting current membership in the Mississippi National Guard and ownership of at least 1 firearm were scheduled for a baseline appointment at the University of Southern Mississippi to complete informed consent procedures. Service members consenting to participate completed a series of structured interviews and self-report questionnaires, after which they were randomized to 1 of 4 groups: (1) lethal means counseling, (2) lethal means counseling plus cable locks, (3) health and stress counseling (HSC), or (4) HSC plus cable locks. Immediately after the intervention, participants completed a second series of self-report questionnaires. Participants were contacted at 3 and 6 months after baseline to complete structured interviews and self-report questionnaires. Participants received $50 for completing the baseline appointment and $75 for each follow-up assessment.
The present study used a 2 × 2 factorial design with randomization stratified by gender and lifetime history of suicidal thoughts. Randomization was achieved by using a computerized algorithm via Qualtrics to minimize bias or human error. Follow-up assessments were conducted at 3 and 6 months after baseline.
Interventions
All interventions were delivered by clinical psychology doctoral students, each of whom completed a standardized 2-day training workshop conducted by 2 of the investigators (A. O. B. and C. J. B.) that included didactics, demonstrations, and role plays with supervision and feedback. After the training, clinicians completed practice sessions that were audio recorded and reviewed by the trainers for fidelity monitoring. At least 2 practice sessions with a minimum 85% fidelity score was required for clinicians to begin administering the interventions to participants. All study interventions were audio recorded and rated by 1 of the trainers with a published fidelity rating scale.26 Supervision and feedback were provided to study clinicians. At the conclusion of the 6-month session, participants were offered all interventions they were not randomized to receive at baseline free of charge.
Lethal means counseling.
Lethal means counseling was administered by using a motivational interviewing–based protocol.26–28 In this protocol, the clinician used a guiding approach to identify methods for safe firearm storage and reflected the participant’s reasons for and against safe firearm storage, with a particular focus on the service member’s verbalized reasons for wanting to adopt or use the identified storage methods. Once a plan for safe firearm storage was identified and agreed upon by the participant and clinician, it was written down and a copy given to the participant. On average, lethal means counseling required approximately 10 to 15 minutes.
Health and stress counseling.
HSC was used as an active attention control. In the HSC condition, the clinician used a guiding approach to identify potential methods for enhancing stress management, sleep quality, diet, or exercise; the specific topic discussed was chosen by the participant. Once a plan was identified and agreed upon, it was written down and a copy was given to the participant. On average, HSC required 10 to 15 minutes.
Cable locks.
In the cable lock groups, participants were given cable locks for each of their personal firearms (up to a maximum of 10) after they had completed their assigned counseling intervention. All service members were given instructions on how to utilize the cable locks if they indicated that they did not know how to use them or if they believed they were incompatible with their personal firearms. Cable locks were provided by the Defense Suicide Prevention Office.
Measures
Firearm storage practices.
Service members were asked if they used each of the following firearm storage practices: (1) storing firearms in a gun safe, (2) using a locking device when the firearm is not in use, and (3) storing firearms unloaded. Response options were “yes” or “no.” Participants were directed to answer in a manner that reflected the practice used for their least-secured firearm (e.g., if at least 1 firearm was not stored in a safe, the participant was directed to answer “no” in response to that question). Participants were asked to report their current firearm storage practices at baseline (before the intervention), and 3 months and 6 months after baseline.
Intervention acceptability.
Service members were asked immediately after treatment if they would recommend the intervention to a peer. Responses were coded dichotomously as yes (1) or no (0).
Statistical Analysis
We evaluated the study hypotheses by using intent-to-treat analyses that included all participants enrolled and randomized to each intervention. Missing data during follow-up were low (7.8% at 3 months and 9.9% at 6 months after baseline) and random (Little’s test: χ2(3) = 3.9; P = .269). For all analyses, we used generalized linear mixed modeling (GLMM) with a random intercept, nesting of repeated assessments within participants, and a sandwich variance estimator. Independent variables included counseling group (lethal means counseling vs HSC), cable lock group (given vs not), time (baseline, 3 months, 6 months), all 2-way interactions, and the 3-way interaction. We used a Satterthwaite approximation because simulation studies show the method minimizes type I error rates.29 The primary outcome was firearm storage practices and was modeled as a count variable computed as the sum total of 3 firearm storage practices (i.e., gun safe, locking device, and firearm unloaded) that conformed to a Poisson distribution.
We next constructed a series of GLMMs to examine treatment effects on each firearm storage practice and intervention acceptability as separate binary outcomes. We also conducted a series of sensitivity analyses that repeated these GLMMs in the subset of participants denying the use of each safe storage practice at baseline, thereby enabling us to assess intervention effects and acceptability among those participants who did not use various safe storage practices. We conducted all analyses with SPSS version 25 software (IBM, Somers, NY).
We calculated a priori power and sample size estimates for the primary outcome by using previously reported rates of between-group differences in rates of restricting access to potential suicide methods (Kruesi et al.14; McManus et al.15), which suggested a large effect of lethal means counseling on means restriction behaviors (odds ratios [ORs] > 4). We chose to estimate a more conservative effect (i.e., OR = 2.0–2.5), however, because these studies were conducted with high-risk adolescents receiving treatment in an emergency department after a suicide attempt, and the lethal means counseling was provided to the adolescent’s parents. The present study, by contrast, was conducted in a community sample of adult firearm owners. Assuming a 2-tailed α = 0.05, a total sample of 200 participants (100 per factor level, or 50 per intervention group) was needed to detect a minimum OR of 2 with 80% power. To account for expected attrition, we recruited an additional 8 participants per condition for a total sample of 232.
RESULTS
Demographic characteristics of the sample are summarized in Table 1. Flow of participants through the study is summarized in Figure 1. Dropout rates across the 4 intervention groups did not significantly differ (χ2[3] = 6.2; P = .104): lethal means counseling only (6.8%), lethal means counseling plus cable lock (18.2%), HSC only (5.4%), and HSC plus cable lock (9.7%).
TABLE 1—
Demographics of the Sample Enrolled in the Randomized Controlled Trial Regarding Lethal Means Counseling, Distribution of Cable Locks, and Safe Firearm Storage Practices Among the Mississippi National Guard: February 2018–July 2020
| Full Sample, No. (%) or Mean ±SD | LMC, No. (%) or Mean ±SD | H&S, No. (%) or Mean ±SD | LMC Only, No. (%) or Mean ±SD | LMC + CL, No. (%) or Mean ±SD | H&S Only, No. (%) or Mean ±SD | H&S + CL, No. (%) or Mean ±SD | |
| Sample size | 232 | 114 | 118 | 59 | 55 | 56 | 62 |
| Gender | |||||||
| Male | 203 (87.5) | 99 (86.8) | 104 (88.1) | 49 (83.1) | 50 (90.9) | 49 (87.5) | 55 (88.7) |
| Female | 29 (12.5) | 15 (13.2) | 14 (11.9) | 10 (16.9) | 5 (9.1) | 7 (12.5) | 7 (11.3) |
| Age, y | 35.01 ±10.23 | 36.00 ±10.54 | 34.06 ±9.88 | 36.15 ±10.16 | 35.84 ±11.02 | 31.73 ±8.83 | 36.16 ±10.37 |
| Race | |||||||
| White | 179 (77.2) | 91 (79.8) | 88 (74.5) | 47 (79.7) | 41 (74.6) | 42 (75.0) | 49 (79.0) |
| Black | 51 (22.0) | 24 (21.1) | 27 (22.9) | 12 (20.3) | 12 (21.8) | 14 (25.0) | 13 (21.0) |
| Relationship status | |||||||
| Unmarried | 68 (29.3) | 34 (29.9) | 34 (28.8) | 16 (27.1) | 18 (32.8) | 20 (35.7) | 14 (22.6) |
| Married | 140 (60.4) | 68 (59.6) | 72 (61.0) | 36 (61.0) | 32 (58.1) | 34 (60.7) | 38 (61.3) |
| Divorced or separated | 24 (10.3) | 12 (10.5) | 12 (10.2) | 7 (11.9) | 5 (9.1) | 2 (3.6) | 10 (16.1) |
| Education | |||||||
| High school | 18 (7.8) | 10 (8.8) | 8 (6.8) | 5 (8.5) | 5 (9.1) | 3 (5.4) | 5 (8.1) |
| Some college | 81 (34.9) | 37 (32.5) | 44 (37.3) | 15 (25.4) | 22 (40.0) | 23 (41.1) | 21 (33.9) |
| College degree | 101 (43.5) | 50 (43.8) | 51 (43.3) | 29 (49.1) | 21 (38.2) | 23 (41.0) | 28 (45.2) |
| Advanced degree | 32 (13.8) | 17 (13.8) | 15 (12.7) | 10 (16.9) | 7 (12.7) | 7 (12.5) | 8 (12.9) |
| Household income, $ | |||||||
| < 10 000 | 13 (5.6) | 6 (5.3) | 7 (5.9) | 2 (3.4) | 4 (7.3) | 6 (10.7) | 1 (1.6) |
| 10 001–24 999 | 25 (10.8) | 14 (12.3) | 11 (9.3) | 8 (13.6) | 6 (10.9) | 5 (8.9) | 6 (9.7) |
| 25 000–49 999 | 33 (14.2) | 16 (14.0) | 17 (14.4) | 9 (15.3) | 7 (12.7) | 10 (17.9) | 7 (11.3) |
| 50 000–74 999 | 64 (27.6) | 27 (23.7) | 37 (31.4) | 11 (18.6) | 16 (29.1) | 17 (30.4) | 20 (32.3) |
| 75 000–99 999 | 44 (19.0) | 24 (21.1) | 20 (16.9) | 16 (27.1) | 8 (14.5) | 7 (12.5) | 13 (21.0) |
| ≥ 100 000 | 53 (22.8) | 27 (23.7) | 26 (22.0) | 13 (22.0) | 14 (25.5) | 11 (19.6) | 15 (24.2) |
| Political orientation | |||||||
| Extremely liberal | 1 (0.4) | 0 (0.0) | 1 (0.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (1.6) |
| Somewhat liberal | 9 (3.9) | 3 (2.6) | 6 (5.1) | 2 (3.4) | 1 (1.8) | 3 (5.4) | 3 (4.8) |
| Moderate | 101 (43.5) | 51 (44.7) | 50 (42.4) | 28 (47.5) | 23 (41.8) | 24 (42.9) | 26 (41.9) |
| Somewhat conservative | 93 (40.1) | 49 (43.0) | 44 (37.3) | 26 (44.1) | 23 (41.8) | 22 (39.3) | 22 (35.5) |
| Extremely conservative | 28 (12.1) | 11 (9.6) | 17 (14.4) | 3 (5.1) | 8 (14.5) | 7 (12.5) | 10 (16.1) |
| Rank | |||||||
| Enlisted | 141 (60.8) | 73 (64.6) | 68 (58.6) | 35 (59.3) | 38 (70.4) | 32 (59.3) | 36 (58.1) |
| NCO | 28 (12.1) | 10 (8.8) | 18 (15.5) | 4 (6.8) | 6 (11.1) | 9 (16.7) | 9 (14.5) |
| Warrant officer | 7 (3.0) | 3 (2.7) | 4 (3.4) | 2 (3.4) | 1 (1.9) | 1 (1.9) | 3 (4.8) |
| Officer | 53 (22.8) | 27 (23.9) | 26 (22.4) | 18 (30.5) | 9 (16.7) | 12 (22.2) | 14 (22.6) |
Note. H&S = health and stress counseling control condition; LMC = lethal means counseling; NCO = noncommissioned officer.
FIGURE 1—
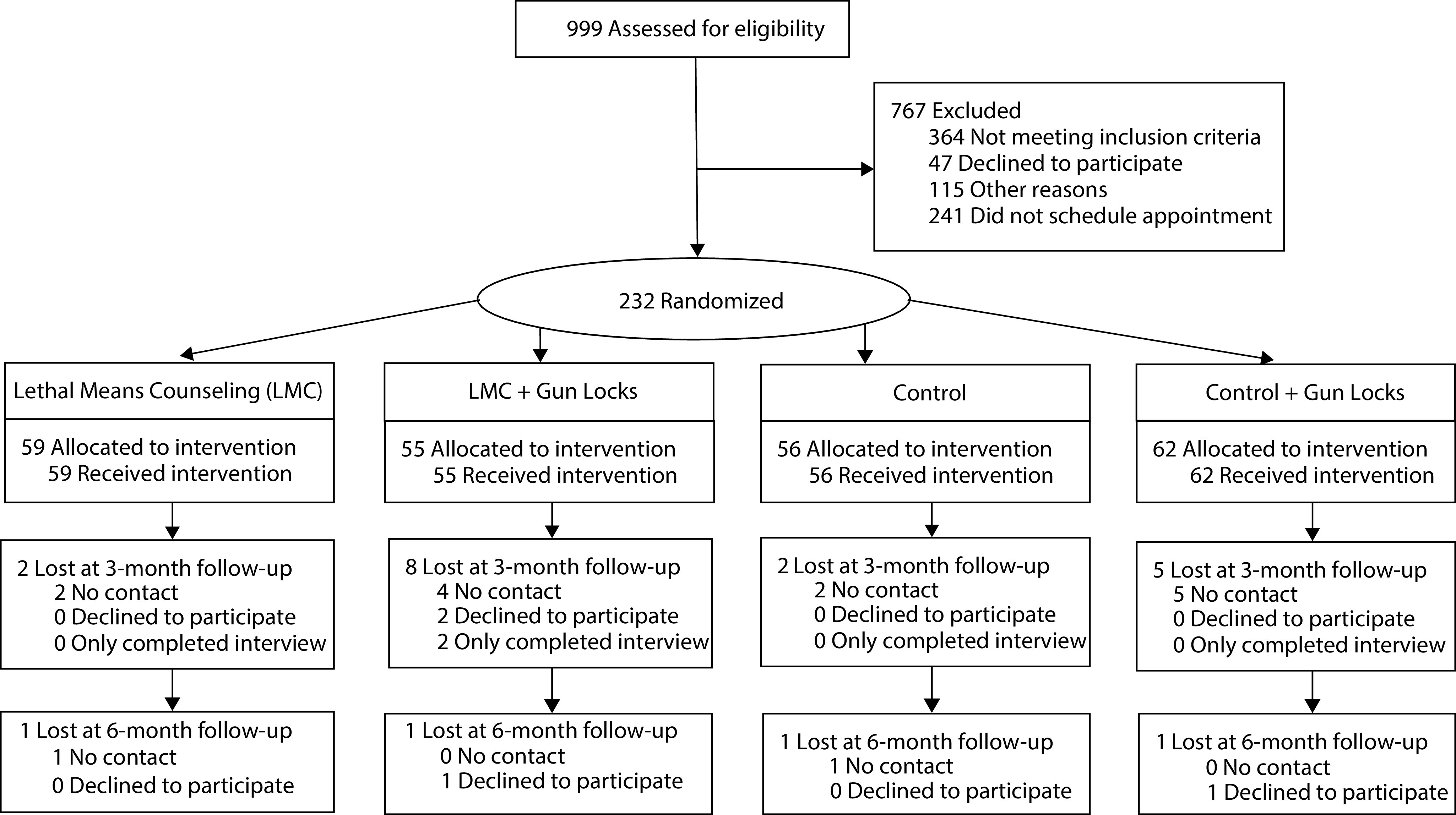
CONSORT Diagram for Individuals Assessed for Eligibility for Trial Regarding Lethal Means Counseling, Distribution of Cable Locks, and Safe Firearm Storage Practices Among the Mississippi National Guard
Cable Lock Distribution and Storage Practices
In the cable lock group, the mean number of firearm storage methods used (F[2643] = 9.1; P < .001) and rate of locking device use (F[2643] = 15.9; P < .001) significantly increased over time. In the control group, the rate of locking devices significantly increased over time (F[2643] = 4.4; P = .013). These increases were larger in the cable lock group (Table 2). At 3 months, participants in the cable lock group reported a slightly higher mean number of firearm storage methods on average (mean = 1.41 [SE = 0.10] vs mean = 1.11 [SE = 0.10]; d = 0.29; 95% confidence interval [CI] = 0.09, 0.49) and were more than twice as likely to use locking devices (59.8% [SE = 6.0%] vs 29.9% [SE = 5.2%]; OR = 3.49; 95% CI = 1.98, 6.14). At 6 months, the difference in mean firearm storage methods used was negligible between groups (mean = 1.34 [SE = 0.10] vs mean = 1.16 [SE = 0.10]; d = 0.15; 95% CI = –0.06, 0.35). The rate of locking device use reduced slightly but was still approximately 1.5 times higher in the cable lock group (58.4% [SE = 6.1%] vs 35.8% [SE = 5.8%]; OR = 2.52; 95% CI = 1.44, 4.40).
TABLE 2—
Firearm Storage Practices Among 232 Firearm-Owning US Military Personnel, by Intervention Group: February 2018–July 2020
| H&S Only, Mean ±SE or No. (%) | H&S + CL, Mean ±SE or No. (%) | LMC Only, Mean ±SE or No. (%) | LMC + CL, Mean ±SE or No. (%) | No CL, Mean ±SE or No. (%) | CL, Mean ±SE or No. (%) | d or ORa (95% CI) | No LMC, Mean ±SE or No. (%) | LMC, Mean ±SE or No. (%) | d or ORa (95% CI) | |
| No. of storage methods | ||||||||||
| Baseline | 0.0 ±0.0 | 1.2 ±0.1 | 0.9 ±0.1 | 1.0 ±0.1 | 1.0 ±0.1 | 1.1 ±0.1 | 0.13 (–0.06, 0.31) | 1.1 ±0.1 | 0.9 ±0.1 | 0.08 (–0.27, 0.10) |
| 3 mo | 0.7 ±0.2 | 1.3 ±0.1 | 1.2 ±0.1 | 1.5 ±0.1 | 1.1 ±0.1 | 1.4 ±0.1 | 0.29 (0.09, 0.49) | 1.2 ±0.1 | 1.3 ±0.1 | 0.12 (–0.08, 0.32) |
| 6 mo | 0.6 ±0.1 | 1.3 ±0.1 | 1.3 ±0.1 | 1.3 ±0.1 | 1.2 ±0.1 | 1.4 ±0.1 | 0.15 (–0.06, 0.35) | 1.2 ±0.1 | 1.3 ±0.1 | 0.13 (–0.08, 0.33) |
| Gun safe | ||||||||||
| Baseline | 0.0 (0.0) | 39.4 (8.2) | 24.2 (6.6) | 18.6 (5.8) | 25.0 (4.8) | 27.8 (5.2) | 1.16 (0.64, 2.07) | 32.2 (5.5) | 21.2 (4.4) | 0.57 (0.31, 1.02) |
| 3 mo | 12.0 (5.1) | 28.2 (7.3) | 33.8 (7.9) | 38.2 (7.9) | 26.8 (5.1) | 33.0 (5.8) | 1.35 (0.75, 2.42) | 24.2 (4.8) | 36.0 (6.0) | 1.76 (0.97, 3.19) |
| 6 mo | 9.7 (4.6) | 35.1 (8.3) | 33.7 (8.0) | 30.9 (8.4) | 26.8 (5.1) | 32.9 (5.9) | 1.34 (0.74, 2.43) | 27.4 (5.3) | 32.2 (5.8) | 1.26 (0.69, 2.28) |
| Locked up | ||||||||||
| Baseline | 0.0 (0.0) | 30.5 (7.0) | 16.3 (5.2) | 23.9 (6.6) | 19.9 (4.2) | 27.1 (4.8) | 1.50 (0.81, 2.76) | 27.1 (4.8) | 19.8 (4.2) | 0.66 (0.36, 1.23) |
| 3 mo | 17.4 (6.1) | 58.1 (8.1) | 31.4 (7.5) | 61.6 (8.8) | 29.9 (5.2) | 59.8 (6.0) | 3.49 (1.98, 6.14) | 42.6 (6.0) | 46.1 (6.3) | 1.15 (0.67, 1.98) |
| 6 mo | 14.9 (5.6) | 61.6 (8.8) | 48.4 (8.6) | 61.5 (9.0) | 35.8 (5.8) | 58.4 (6.1) | 2.52 (1.44, 4.40) | 39.0 (5.9) | 55.0 (6.3) | 1.91 (1.10, 3.32) |
| Unloaded | ||||||||||
| Baseline | 0.0 (0.0) | 48.8 (8.3) | 44.0 (8.2) | 53.3 (8.5) | 47.3 (6.0) | 51.0 (5.9) | 1.16 (0.69, 1.94) | 49.6 (0.6) | 48.6 (6.0) | 0.96 (0.57, 1.61) |
| 3 mo | 31.2 (10.0) | 54.5 (8.5) | 55.6 (8.3) | 64.3 (8.7) | 56.8 (5.9) | 59.5 (6.2) | 1.11 (0.65, 1.93) | 56.2 (6.0) | 60.0 (6.1) | 1.17 (0.68, 2.01) |
| 6 mo | 27.0 (9.4) | 54.0 (8.6) | 61.3 (8.2) | 47.9 (9.3) | 59.1 (5.9) | 50.9 (6.3) | 1.39 (0.81, 2.41) | 55.4 (6.1) | 54.7 (6.3) | 0.97 (0.56, 1.68) |
Note. CI = confidence interval; CL = cable locks; H&S = health and stress counseling control condition; LMC = lethal means counseling; OR = odds ratio.
The no. of storage methods results are d, the remainder are OR.
Results of our sensitivity analyses yielded statistically significant between-group differences for locking device use (Table 3). Using a gun safe was less common in the cable lock group at 3 months (0.0% [SE = 0.0%] vs 15.3% [SE = 0.0%]) but rates of use were comparable across groups at 6 months (15.3% [SE = 4.4%] vs 13.4% [SE = 4.4%]; OR = 1.17; 95% CI = 046, 2.98). In the cable lock group, the rate of locking device use was approximately 3 times more common at 3 months (42.6% [SE = 6.7%] vs 15.3% [SE = 3.9%]; OR = 4.11; 95% CI = 1.93, 8.74) and 1.9 times more common at 6 months (22.9% [SE = 5.0%] vs 42.8% [SE = 6.8%]; OR = 2.52; 95% CI = 1.26, 5.05).
TABLE 3—
Results of Sensitivity Analyses by Intervention Group: February 2018–July 2020
| H&S Only, Mean ±SE or No. (%) | H&S + CL, Mean ±SE or No. (%) | LMC Only, Mean ±SE or No. (%) | LMC + CL, Mean ±SE or No. (%) | No CL, Mean ±SE or No. (%) | CL,Mean ±SE or No. (%) | d or ORa (95% CI) | No LMC, Mean ±SE or No. (%) | LMC, Mean ±SE or No. (%) | d or ORa (95% CI) | |
| No. of storage methods | ||||||||||
| Baseline (Ref) | 0.0 ±0.0 | 0.0 ±0.0 | 0.0 ±0.0 | 0.0 ±0.0 | 0.0 ±0.0 | 0.0 ±0.0 | 0 | 0.0 ±0.0 | 0.0 ±0.0 | 0 |
| 3 mo | 0.7 ±0.2 | 0.8 ±0.2 | 0.9 ±0.2 | 1.1 ±0.2 | 0.8 ±0.1 | 1.0 ±0.1 | 0.16 (–0.28, 0.61) | 0.8 ±0.1 | 1.0 ±0.1 | 0.29 (–0.16, 0.74) |
| 6 mo | 0.6 ±0.1 | 1.0 ±0.2 | 1.1 ±0.2 | 1.0 ±0.2 | 0.8 ±0.1 | 1.0 ±0.2 | 0.20 (–0.26, 0.65) | 0.8 ±0.1 | 1.0 (0.1 | 0.26 (–0.19, 0.72) |
| Gun safe | ||||||||||
| Baseline (Ref) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 1 | 0.0 (0.0) | 0.0 (0.0) | 1 |
| 3 mo | 12.0 (5.1) | 0.0 (0.0) | 19.2 (6.6) | 26.8 (7.6) | 15.3 (4.1) | 0.0 (0.0) | b | 0.0 (0.0) | 22.8 (5.0) | b |
| 6 mo | 9.7 (4.6) | 12.2 (5.7) | 18.3 (6.4) | 19.1 (6.7) | 13.4 (3.9) | 15.3 (4.4) | 1.17 (0.46, 2.98) | 10.9 (3.6) | 18.7 (4.6) | 1.88 (0.72, 4.88) |
| Locked up | ||||||||||
| Baseline (Ref) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 1 | 0.0 (0.0) | 0.0 (0.0) | 1 |
| 3 mo | 17.4 (6.1) | 41.2 (9.0) | 13.4 (5.1) | 44.1 (9.9) | 15.3 (3.9) | 42.6 (6.7) | 4.11 (1.93, 8.74) | 27.7 (5.6) | 25.9 (5.7) | 0.91 (0.45, 1.85) |
| 6 mo | 14.9 (5.6) | 38.1 (8.9) | 33.5 (7.9) | 47.6 (10.1) | 22.9 (5.0) | 42.8 (6.8) | 2.52 (1.26, 5.05) | 24.7 (5.4) | 40.4 (6.5) | 2.07 (1.04, 4.11) |
| Unloaded | ||||||||||
| Baseline (Ref) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | 1 | 0.0 (0.0) | 0.0 (0.0) | 1 |
| 3 mo | 31.2 (10.0) | 22.7 (8.4) | 33.5 (9.5) | 35.1 (11.1) | 32.4 (6.9) | 32.9 (7.0) | 1.02 (0.45, 2.30) | 26.7 (6.5) | 34.3 (7.3) | 1.43 (0.62, 3.29) |
| 6 mo | 27.0 (9.4) | 22.7 (8.4) | 39.5 (10.1) | 12.4 (3.7) | 28.5 (7.0) | 16.9 (5.7) | 0.51 (0.20, 1.32) | 24.8 (6.3) | 23.3 (7.0) | 0.92 (0.37, 2.28) |
Note. CI = confidence interval; CL = cable locks; HSC = health and stress counseling control condition; LMC = lethal means counseling; OR = odds ratio.
The no. of storage methods results are d, the remainder are OR.
OR could not be calculated because of empty cell.
Lethal Means Counseling and Storage Practices
In the lethal means counseling group, the mean number of storage methods used (F[2643] = 11.3; P < .001), rate of gun safe use (F[2643] = 3.9; P = .020), and rate of locking device use (F[2643] = 17.7; P < .001) significantly increased over time. In the control group, there was no change in any outcome variable. The observed increases were only slightly larger in the lethal means counseling group (Table 2). At 6 months, the participants in the lethal means counseling group were approximately 30% more likely to use a locking device (55.0% [SE = 6.3%] vs 39.0% [SE = 5.9%]; OR = 1.91; 95% CI = 1.10, 3.32).
Results of our sensitivity analyses yielded a statistically significant between-group difference only for locking device use (Table 3). Using a gun safe was more common in the lethal means counseling group at 3 months (22.8% [SE = 5.0%] vs 0.0% [SE = 0.0%]) but rates of use were comparable across groups at 6 months (18.7% [SE = 4.6%] vs 10.9% [SE = 3.6%]; OR = 1.88; 95% CI = 0.72, 4.88). In the lethal means counseling group, locking device use was comparable at 3 months (25.9% [SE = 5.7%] vs 27.7% [SE = 5.6%]; OR = 0.91; 95% CI = 0.45, 1.85) and 1.6 times higher at 6 months (40.4% [SE = 6.5%] vs 24.7% [SE = 5.4%]; OR = 2.07; 95% CI = 1.04, 4.11).
DISCUSSION
In the present study, we examined the effectiveness of a single session of lethal means counseling and the distribution of cable locks for prompting safe storage practices in a community sample of US National Guard personnel using a primary prevention framework wherein participants were recruited on the basis of firearm ownership rather than suicide risk. Several results were consistent with expectations. First, service members who received lethal means counseling reported a larger increase in the number of safe storage practices used over time, specifically the use of gun safes and locking devices, relative to those randomized to HSC. Second, service members who received 1 or more cable locks were more likely to use locking devices over time as compared with those who received no cable locks. Our results did not support the superiority of lethal means counseling and gun locks in combination beyond the effects of either intervention alone.
These results are promising when we consider that our method for assessing use of firearm storage practices utilized a conservative criterion wherein all firearms in the household had to be stored with a given practice to be considered present. If any firearm within the home was unlocked, for example, the criterion for safe storage was not met. In this sense, these results could underestimate the impact of lethal means counseling and cable lock distribution by disregarding incremental behavior changes wherein some, but not all, firearms were more safely stored after intervention.
The appropriateness of each intervention likely differs by setting. Distributing cable locks, for instance, may be more scalable but may increase only 1 storage method. Lethal means counseling, by contrast, may increase a wider range of storage options but is less scalable. In our sensitivity analyses, individuals who did not use gun safes and received a cable lock were less likely than those who did not receive a gun lock to store all of their firearms in a gun safe. It is possible, for instance, that the distribution of locking devices reduces the perceived utility or value of gun safes.
The speed with which participants adopted various storage practices was notable. Among those who did not use locking devices, 42.6% of those who received a cable lock versus 15.3% of those who did not reported using locking devices on all firearms within 3 months. Lethal means counseling, by contrast, showed a slower adoption rate for locking devices (approximately 26% by 3 months and 40% by 6 months after baseline), but a faster adoption rate for gun safes. The speed with which a particular storage method is adopted may vary within lethal means counseling in part because this particular intervention is not focused on a single method and also because this protocol involves working within the values and motivations of individuals rather than prescribing a particular set of actions.
In addition to examining the efficacy of the intervention, we also examined acceptability. Our decision to conduct this trial using a politically conservative sample of individuals in a high-firearm-ownership state represents a strength. High rates of acceptability would thus serve as a sign that productive conversations on this topic are possible even in difficult circumstances. We considered acceptability by using 2 variables: attrition rate and self-reported likelihood of recommending the intervention to peers. Retention rates for the study were high, with 90.9% of the baseline sample completing the entire protocol. Furthermore, attrition rates did not differ across conditions. In addition, across the entire protocol, only 1 participant indicated that he or she would not recommend the intervention, and that individual was randomized to the HSC-only condition, meaning that all individuals who received lethal means counseling or a cable lock indicated that they would recommend their intervention.
Limitations
A limitation of our study involved variability across treatment groups on baseline firearm storage practices. Although not statistically significant, participants randomized to the HSC plus cable lock group were approximately twice as likely to use gun safes as participants randomized to the lethal means counseling plus cable lock group (39% vs 19%). To assess the potential impact of this variability on our results, we conducted sensitivity analyses wherein we repeated our analyses in the subset of participants who did not endorse this storage practice at baseline. The results of these analyses did not differ from our primary analyses, however, suggesting that this limitation did not adversely affect our results. Stratifying by storage practices at baseline is recommended for future studies. Another limitation is our use of self-report to assess firearm storage practices, although there is no reason to think that accurate self-disclosure would be nonrandomly distributed across intervention groups. The generalizability of our results beyond members of the Mississippi National Guard may also be limited. Our use of doctoral students—albeit with limited clinical experience—to conduct lethal means counseling may limit our understanding of the potential broader reach of lethal means counseling when provided by health care professionals, commanders, and other community members.
Conclusions
Despite these limitations, these results highlight that lethal means counseling and the provision of cable locks can facilitate meaningful and sustained changes in firearm storage practices. It is difficult to estimate the number of lives that would be saved if these protocols were broadly implemented, as data demonstrating that adoption of safe storage prevents otherwise likely suicide deaths are lacking. Given the frequency with which firearms are used in military suicides, promoting safe firearm storage may represent an invaluable tool for military suicide prevention. These results suggest that lethal means counseling and cable lock distribution could positively address this issue, even among firearm-owning service members not seeking out either intervention. Pending replication, broader implementation of lethal means counseling and cable lock distribution within the US military may represent an important step toward lowering the military suicide rate.
ACKNOWLEDGMENTS
This work was in part supported by the Military Suicide Research Consortium (MSRC), an effort supported by the Office of the Assistant Secretary of Defense for Health Affairs under award W81XWH-16-2-0003.
The authors would like to acknowledge the invaluable contributions of graduate students and project managers who contributed to the project through recruitment, service as recruitment and retention coordinators, and as study clinicians. These included Claire Houtsma, Sarah Butterworth, Samantha Daruwala, Shelby Bandel, Allison Bond, Brian Bauer, Olivia Preston, Rachel Martin, Nicole Smith, Nicole Caulfield, Aleksandrs Karnick, Kayla Wagler, Sydney Waitz-Kudla, and Paula Floyd.
Note. Opinions, interpretations, conclusions, and recommendations are those of the authors and are not necessarily endorsed by the MSRC or the Department of Defense.
CONFLICTS OF INTEREST
M. D. Anestis receives personal income from book royalties related to firearms and suicide as well as speaking and consulting fees on these topics. C. J. Bryan receives personal income from trainings on lethal means counseling.
HUMAN PARTICIPANT PROTECTION
Approval was received and annually renewed from the University of Southern Mississippi institutional review board and the US Army Medical Research and Materiel Command Human Research Protection Office.
Footnotes
See also McCourt, p. 185.
REFERENCES
- 1.Centers for Disease Control and Prevention. Web-based inquiry statistics query and reporting system (WISQARS) 2020. Available at: http://www.cdc.gov/injury/wisqars/index.html. Accessed July 10, 2020.
- 2.Department of Defense. Department of Defense Suicide Event Report (DoDSER): calendar year 2018 annual report. 2018. Available at: https://www.pdhealth.mil/sites/default/files/images/docs/TAB_B_2018_DoDSER_Annual_Report-508%20final-9MAR2020.pdf. Accessed July 20, 2020.
- 3.Simon RI. Gun safety management with patients at risk for suicide. Suicide Life Threat Behav. 2007;37(5):518–526. doi: 10.1521/suli.2007.37.5.518. [DOI] [PubMed] [Google Scholar]
- 4.Anestis MD, Houtsma C. The association between gun ownership and statewide overall suicide rates. Suicide Life Threat Behav. 2018;48(2):204–217. doi: 10.1111/sltb.12346. [DOI] [PubMed] [Google Scholar]
- 5.Miller M, Barber C, White RA, Azrael D. Firearms and suicide in the United States: is risk independent of underlying suicidal behavior? Am J Epidemiol. 2013;178(6):946–955. doi: 10.1093/aje/kwt197. [DOI] [PubMed] [Google Scholar]
- 6.Miller M, Lippmann SJ, Azrael D, Hemenway D. Household firearm ownership and rates of suicide across the 50 United States. J Trauma. 2007;62(4):1029–1034. doi: 10.1097/01.ta.0000198214.24056.40. [DOI] [PubMed] [Google Scholar]
- 7.Miller M, Swanson SA, Azrael D. Are we missing something pertinent? A bias analysis of unmeasured confounding in the firearm-suicide literature. Epidemiol Rev. 2016;38(1):62–69. doi: 10.1093/epirev/mxv011. [DOI] [PubMed] [Google Scholar]
- 8.Miller M, Warren M, Hemenway D, Azrael D. Firearms and suicide in US cities. Inj Prev. 2015;21(e1):e116–e119. doi: 10.1136/injuryprev-2013-040969. [DOI] [PubMed] [Google Scholar]
- 9.Opoliner A, Azrael D, Barber C, Fitzmaurice G, Miller M. Explaining geographic patterns of suicide in the US: the role of firearms and antidepressants. Inj Epidemiol. 2014;1(1):6. doi: 10.1186/2197-1714-1-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Brent DA. Firearms and suicide. Ann N Y Acad Sci. 2001;932(1):225–239. doi: 10.1111/j.1749-6632.2001.tb05808.x. [DOI] [PubMed] [Google Scholar]
- 11.Shenassa ED, Rogers ML, Spalding KL, Roberts MB. Safer storage of firearms at home and risk of suicide: a study of protective factors in a nationally representative sample. J Epidemiol Community Health. 2004;58(10):841–848. doi: 10.1136/jech.2003.017343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lethal Means & Suicide Prevention: A Guide for Community & Industry Leaders. Washington, DC: Education Development Center; 2020. National Action Alliance for Suicide Prevention, Lethal Means Stakeholder Group. [Google Scholar]
- 13.Barber CW, Miller MJ. Reducing a suicidal person’s access to lethal means of suicide: a research agenda. Am J Prev Med. 2014;47(3):S264–S272. doi: 10.1016/j.amepre.2014.05.028. [DOI] [PubMed] [Google Scholar]
- 14.Kruesi MJP, Grossman J, Pennington JM, Woodward PJ, Duda D, Hirsch JG. Suicide and violence prevention: parent education in the emergency department. J Am Acad Child Adolesc Psychiatry. 1999;38(3):250–255. doi: 10.1097/00004583-199903000-00010. [DOI] [PubMed] [Google Scholar]
- 15.McManus BL, Kruesi MJ, Dontes AE, Defazio CR, Piotrowski JT, Woodward PJ. Child and adolescent suicide attempts: an opportunity for emergency departments to provide injury prevention education. Am J Emerg Med. 1997;15(4):357–360. doi: 10.1016/S0735-6757(97)90124-8. [DOI] [PubMed] [Google Scholar]
- 16.Spicer RS, Miller TR. Suicide acts in 8 states: incidence and case fatality rates by demographics and method. Am J Public Health. 2000;90(12):1885–1891. doi: 10.2105/AJPH.90.12.1885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lambert MT, Fowler D. Suicide risk factors among veterans: risk management in the changing culture of the Department of Veterans Affairs. J Ment Health Adm. 1997;24(3):350–358. doi: 10.1007/BF02832668. [DOI] [PubMed] [Google Scholar]
- 18.Anestis MD, Bandel SL, Butterworth SE, Bond AE, Daruwala SE, Bryan CJ. Suicide risk and firearm ownership and storage behavior in a large military sample. Psychiatry Res. 2020;291:113277. doi: 10.1016/j.psychres.2020.113277. [DOI] [PubMed] [Google Scholar]
- 19.Bryan CJ, Bryan AO, Anestis MD et al. Firearm availability and storage practices among military personnel who have thought about suicide: a cross-sectional study. JAMA Netw Open. 2019;2(8):e199160. doi: 10.1001/jamanetworkopen.2019.9160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of US veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49(3):653–664. doi: 10.1111/sltb.12463. [DOI] [PubMed] [Google Scholar]
- 21.Mahon MJ, Tobin JP, Cusack DA, Kelleher C, Malone KM. Suicide among regular-duty military personnel: a retrospective case–control study of occupation-specific risk factors for workplace suicide. Am J Psychiatry. 2005;162(9):1688–1696. doi: 10.1176/appi.ajp.162.9.1688. [DOI] [PubMed] [Google Scholar]
- 22.Mills PD, Huber SJ, Vince Watts B, Bagian JP. Systemic vulnerabilities to suicide among veterans from the Iraq and Afghanistan conflicts: review of case reports from a National Veterans Affairs database. Suicide Life Threat Behav. 2011;41(1):21–32. doi: 10.1111/j.1943-278X.2010.00012.x. [DOI] [PubMed] [Google Scholar]
- 23.Anestis MD, Green BA. The effect of varying levels of confidentiality on disclosure of suicidal thoughts in a sample of United States National Guard personnel. J Clin Psychol. 2015;71(10):1023–1030. doi: 10.1002/jclp.22198. [DOI] [PubMed] [Google Scholar]
- 24.Vannoy SD, Andrews BK, Atkins DC, Dondanville KA, Young-McCaughan S, Peterson AL STRONG STAR Consortium. Underreporting of suicide ideation in US Army population screening: an ongoing challenge. Suicide Life Threat Behav. 2017;47(6):723–728. doi: 10.1111/sltb.12318. [DOI] [PubMed] [Google Scholar]
- 25. Bryan CJ, Bryan AO, May AM, et al. Depression, suicide risk, and declining to answer firearm-related survey items among military personnel and veterans. Suicide Life Threat Behav. In press. [DOI] [PubMed]
- 26.Bryan CJ, Rudd MD. Brief Cognitive–Behavioral Therapy for Suicide Prevention. New York, NY: Guilford Press; 2018. [Google Scholar]
- 27.Britton PC, Bryan CJ, Valenstein M. Motivational interviewing for means restriction counseling with patients at risk for suicide. Cognit Behav Pract. 2016;23(1):51–61. doi: 10.1016/j.cbpra.2014.09.004. [DOI] [Google Scholar]
- 28.Bryan CJ, Stone S, Rudd MD. A practical, evidence-based approach for means restriction counseling with suicidal patients. Prof Psychol Res Pr. 2011;42(5):339–346. doi: 10.1037/a0025051. [DOI] [Google Scholar]
- 29.Luke SG. Evaluating significance in linear mixed-effects models in R. Behav Res Methods. 2017;49(4):1494–1502. doi: 10.3758/s13428-016-0809-y. [DOI] [PubMed] [Google Scholar]