

Abstract
Curcumin has a potent antioxidant and anti-inflammatory properties that may suppress inflammatory component of atherosclerosis. It has been demonstrated that curcumin derivatives can reduce the formation of arterial fatty streaks in cholesterol-fed rabbits. Therefore in this study we evaluated the protective effects of Curcumin on the progression of atherosclerosis. 20 mature rabbits were included for this study; they were randomly divided into four groups each of 5. Group 1: (normal control) were fed corn pellets diet and tab water, group 2: (high cholesterol diet control) were kept on cholesterol rich diet (2% cholesterol) and tab water. Group 3: (cholesterol and rosuvastatin treated group) were kept on cholesterol rich diet (2% cholesterol) and 2.5 mg/kg/day Rosuvastatin dispersed in DW and given orally, group 4: (cholesterol and curcumin treated group) were kept on cholesterol rich diet (2% cholesterol) and 0.2% curcumin added with corn pellets. The study continued for 12 weeks then assessment of serum level of high sensitive C-reactive protein, ICAM1, VCAM1 and PCSK9 was carried out at the end of the study. Total antioxidant activity of curcumin was also determined. Histopathological examination of aortic tissues for atherosclerotic changes was also carried out. Atherogenic (cholesterol rich diet) induced an increment in serum level of TC, LDL, VLDL and TG with concomitant decrement in serum level of HDL and increased atherogenic index. Treatment with curcumin produced substantial reduction in serum TC, LDL, TG with no effect on HDL level thus decreased atherogenic index. Rabbits treated with curcumin showed a significant reduction in the serum level of high sensitive C-reactive protein, ICAM1, VCAM, PCSK9 serum expression and aortic total antioxidant capacity. Curcumin has a potent anti-inflammatory and anti- oxidant effects against atherosclerosis so exerts a protective role by decreasing lipid oxidation and inflammatory markers.
Keywords: Curcumin, Hypercholesterolemic, Male, Rabbits, Anti-inflammatory
Introduction
Atherosclerosis occur when there is a deposition and accumulation of low density lipoprotein, cholesterol, platelets, macrophage and white blood cells which will form atheromatous plaque with increased arterial wall thickness [1]. There are many risk factors of atherosclerosis including hypercholesterolemia which is the major risk factor that contribute to the pathogenesis of atherosclerosis, it will cause vascular smooth muscle cell injury and arterial injury that will stimulate inflammatory response and recruitment of immune cells at the site of injury. Diabetes is another risk factor in which there is a disturbance in fatty acids metabolism so increasing the lipoprotein lipase level which will bind to LDL and facilitate accumulation of cholesterol in the arterial wall [2, 3].
In hypertension there will be an increment in the leakage of lipoproteins as well as increased concentration of angiotensin 2 that produce inflammation and accumulation of oxidized LDL in the wall of the artery [3]. Smoking will increase the levels of non-esterified fatty acids in the blood stream which may cause arterial injury and enhance inflammation; obesity is another major risk factor for atherosclerosis and ischemic heart disease [2] Inflammation is an important factor responsible for the disease progression. Elevation in cholesterol, low density lipoprotein and triglycerides will lead to formation of atherosclerotic lesions. Oxidized LDL will trigger vascular-cell manufacturing of M-CSFs and MCP-1 (macrophage colony stimulating factors and monocyte chemoattractant protein-1 respectively) this will increase reactive oxygen species production and increase oxidative stress leading to endothelial dysfunction. Chronic oxidative stress is a major cause of atherosclerosis formation. Oxidative changes that came on LDL will stimulate binding of monocyte to endothelium, increasing the expression of adhesion molecules such as VCAM-1 and ICAM-1 (vascular cell adhesion molecule and the intracellular adhesion molecule respectively [3].
PCSK9 is an enzyme encoded as PCSK9 gene that expressed in many tissues, it binds to LDL receptors and transport fat molecules to extracellular fluids, thus PCSK9 inhibitors will decrease the concentration of LDL in the blood stream [4]. Curcumin is a yellow chemical product produced by plant Curcuma longa, used as herbal supplement, food flavor, and food coloring substance. It is a natural phenol belongs to the group of curcuminoids. It has been found to exert a potent antioxidant and anti-inflammatory properties. Curcumin derivatives have been found to reduce aortic fatty streak formation in cholesterol-fed rabbits [5]. Rosuvastatin is a HMG-CoA reductase inhibitor used in the treatment of hyperlipidemia, it improves atherosclerosis by decreasing pro-inflammatory cytokines and chemokines [6, 7].
Materials and Methods
Animals
A 20 mature domestic rabbits weighting 1.5–2 kg were included in the study, they were kept in a controlled temperature and humidity conditions as well as 12-h light/dark cycle in the animal house/Faculty of Medicine/University of Kufa. The study carried out after approval of the ethical committee in the faculty of medicine, University of Kufa.
The rabbits were randomly divided into four groups, each group contains five rabbits.
Group (I) (normal control): Rabbits were received ordinary diet (corn pellets and tab water).
Group (II) (Cholesterol rich diet): Rabbits were received 2% cholesterol diet and tab water.
Group (III) (Cholesterol and Rosuvastatin treated): Rabbits were received rosuvastatin (2.5 mg/kg/day) and 2% cholesterol diet with tab water.
Group (IV) (Cholesterol and Curcumin treated): Rabbit were received curcumin 0.2% added with corn pellets and 2% cholesterol diet. Distilled water was used as vehicle for both rosuvastatin and curcumin. Drug treatments were given orally using gastric gavage [7]. The study continued for 12 weeks. Serum levels of cholesterol, triglycerides, LDL, VLDL and HDL were measured at the end of the study. Serum level of high sensitive C-reactive protein, ICAM1, VCAM1 and PCSK9 were measured also at the end of the study. Total antioxidant activity of curcumin was also determined. Aortic tissues were sent for histopathological examination for atherosclerotic changes.
Blood Sampling and Processing
At the 12th week of the study a 3 ml arterial blood was obtained from the central ear artery of each overnight fasted rabbit. Blood samples were left until clotted then centrifuged at 6000 rpm for twelve min to obtain serum for measurement of total lipid profile (TC, HDL, LDL, VLDL, TG). Rabbits were anesthetized and a 5 ml of blood was directly obtained from the heart for the examination of the serum level of hs C-reactive protein, ICAM1, VCAM1 and PCSK9 expression.
Tissue Preparation for Measurement of Total Antioxidant Capacity
Aortic tissue was obtained from each rabbit then froze at − 80 °C. Samples were homogenized by sonication after washing them with phosphate buffer saline. Triton X was added to each sample, then was sonicated in ice box and centrifuged for 30 min at 6000 rpm. Supernatant was obtained and analyzed for total antioxidant capacity [8, 9].
Results
Total Cholesterol Serum Level
At the 12th week of the study rabbits on high cholesterol diet developed hypercholesterolemia with significant increase in total cholesterol level (p < 0.05) in the groups (II, IV) in comparison to zero time (Table 1).
Table 1.
Difference of total serum cholesterol levels in mg/dl of the four group
| Groups | Before treatment | After treatment | p value |
|---|---|---|---|
| Control | 105 ± 7 | 113 ± 3 | 0.6 |
| Cholesterol | 112.25 ± 3.4 | 494.5 ± 16.2 | 0.0001* |
| Cholesterol + curcumin | 110 ± 2 1 | 99.5 ± 10.5 | 0.06 |
| Rosuvastatin + cholesterol | 100 ± 2 1 | 77 ± 7 | 0.04* |
Data expressed as mean ± SEM, paired T test
*p value < 0.05 means statistically significant
The Serum Triglyceride (TG) Level
At the 12th week of the study rabbits on high cholesterol diet have significant increment in serum TG level (p < 0.05) in the group (II) in comparison to zero time (Table 2).
Table 2.
Differences of serum TG levels in mg/dl of four groups
| Groups | Before treatment | After treatment | p value |
|---|---|---|---|
| Control | 164 ± 6 | 241.5 ± 5.6 | 0.6 |
| Cholesterol | 135.5 ± 6.6 | 241.5 ± 5.6 | 0.002* |
| Cholesterol + curcumin | 136 ± 6 | 143.5 ± 14.5 | 0.05 |
| Rosuvastatin + cholesterol | 150 ± 10 | 147.5 ± 7.5 | 0.9 |
Data expressed as mean ± SEM, paired T test
*p value < 0.05 means statistically significant
The Effects on the Serum Levels of HDL
At the 12th week of the study HDL levels were significantly decreased in the groups (II, IV) which were on fat rich diet in comparison to zero time (Table 3).
Table 3.
Differences in serum levels of HDL in mg/dl of the four group
| Groups | Before treatment | After treatment | p value |
|---|---|---|---|
| Control | 12 ± 1 | 12.2 ± 0.8 | 0.9 |
| Cholesterol | 12 ± 1.1 | 9 ± 0.4 | 0.0001* |
| Cholesterol + curcumin | 9 ± 1 | 9 ± 0 | 1 |
| Rosuvastatin + cholesterol | 11 ± 1 | 47 ± 4 | 0.04* |
Data expressed as mean ± SEM, paired T test
*p value < 0.05 means statistically significant
Serum LDL Level
Following 12 weeks on high cholesterol diet in the groups (II, IV), serum LDL-C levels significantly elevated in comparison to zero time (Table 4; Fig. 1).
Table 4.
Differences in serum LDL levels in mg/dl of the group
| Groups | Before treatment | After treatment | p value |
|---|---|---|---|
| Control | 66.5 ± 1.5 | 63.5 ± 3.5 | 0.7 |
| Cholesterol | 73.25 ± 4.2 | 436.5 ± 16.5 | 0.0001* |
| Cholesterol + curcumin | 77 ± 1 | 160.5 ± 7.5 | 0.07 |
| Rosuvastatin + cholesterol | 58.5 ± 7.5 | 100.5 ± 1.5 | 0.04* |
Data expressed as mean ± SEM, paired T test
*p value < 0.05 means statistically significant
Fig. 1.
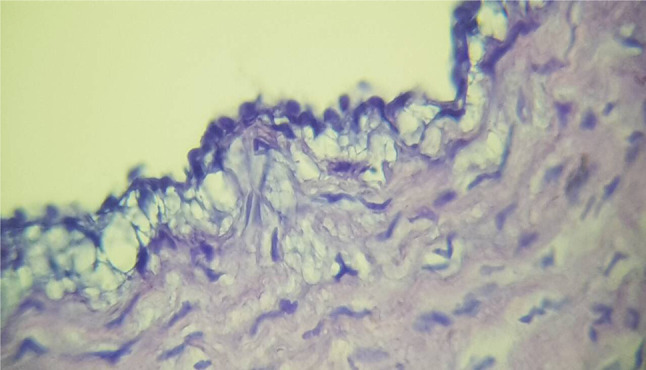
Photomicrograph of histophotometric section of the aortic arch from rabbit fed with 2% cholesterol diet showed accumulation of macrophage that form foams cells on the surface of endothelium
Serum VLDL Level
Following 12 weeks on high cholesterol diet, the VLDL levels have been significantly raised in the groups (II) In comparison to zero time (Table 5).
Table 5.
Differences of serum VLDL levels in mg/dl of the four groups
| Groups | Before treatment | After treatment | p value |
|---|---|---|---|
| Control | 30.5 ± 1.5 | 33.9 ± 3.9 | 0.4 |
| Cholesterol | 27 ± 1.3 | 48.2 ± 1.2 | 0.002* |
| Cholesterol + curcumin | 24 ± 2 | 28.7 ± 2.9 | 0.1 |
| Rosuvastatin + cholesterol | 33.5 ± 1.5 | 29.5 ± 1.5 | 0.4 |
*p value < 0.05 means statistically significant
The Effects on the Atherogenic Index
Following 12 weeks on high cholesterol diet, the Atherogenic index was significantly elevated in the group (II) in comparison to zero time (Table 6).
Table 6.
Differences of atherogenic index levels in mg/dl of the four groups
| Groups | Before treatment | After treatment | p value |
|---|---|---|---|
| Control | 7.75 ± 0.15 | 8.25 ± 0.4 | 0.5 |
| Cholesterol | 8.50 ± 0.7 | 54.5 ± 4.3 | 0.002* |
| Cholesterol + curcumin | 11.35 ± 1.15 | 18.95 ± 1.1 | 0.2 |
| Rosuvastatin + cholesterol | 8.18 ± 1.02 | 2.75 ± 0.15 | 0.1 |
*p value < 0.05 means statistically significant
The Effect of Curcumin and Rosuvastatin on High Sensitive C-Reactive Protein Level
After 12 weeks of high cholesterol diet, hs-CRP was significantly elevated in group II (Cholesterol) compared to the normal control, whereas was significantly decreased in groups III (Cholesterol + Curcumin) and IV(Rosuvastatin + cholesterol) (Table 7).
Table 7.
The differences in hs- CRP Levels
| Group | Mean ± SD | Control | p value |
|---|---|---|---|
| Cholesterol | 7.8242 ± 1.75132 | 4.7963 ± 0.40372 | 0.005* |
| Cholesterol + curcumin | 2.4103 ± 0.29704 | 4.7963 ± 0.40372 | 0.0001* |
| Rosuvastatin + cholesterol | 2.5760 ± 0.14307 | 4.7963 ± 0.40372 | 0.0001* |
*p value < 0.05 means statistically significant
The Effects of Curcumin and Rosuvastatin on Serum Level of ICAM
After 12 weeks, ICAM levels were significantly elevated in groups (II) compared with normal control group while ICAM levels were significantly decreased in group (IV) Table 8.
Table 8.
The differences in ICAM serum Levels
| Groups | Mean ± SD | Control | p value |
|---|---|---|---|
| Cholesterol | 72.7066 ± .56401 | 51.6582 ± 0.94184 | 0.0001* |
| Cholesterol + curcumin | 54.7278 ± 2.14899 | 51.6582 ± 0.94184 | 0.01* |
| Rosuvastatin + cholesterol | 55.3582 ± 2.81922 | 51.6582 ± 0.94184 | 0.0238* |
*p value < 0.05 means statistically significant
The Effects of Curcumin and Rosuvastatin on Serum Level of VCAM
After 12 weeks, VCAM levels were significantly elevated in groups (II, III) compared with normal control group while VCAM levels were significantly decreased in groups (IV) (Table 9).
Table 9.
The changes in VCAM levels
| Groups | Mean ± SD | Control | p value |
|---|---|---|---|
| Cholesterol | 181.8487 ± 0.89489 | 132.9500 ± 2.95000 | 0.0001* |
| Cholesterol + curcumin | 140.9231 ± 2.92310 | 132.9500 ± 2.95000 | 0.002* |
| Rosuvastatin + cholesterol | 126.1750 ± 1.04752 | 132.9500 ± 2.95000 | 0.001* |
*p value < 0.05 means statistically significant
The Effect of Curcumin and Rosuvastatin on Aortic Total Antioxidant Capacity Levels
After 12 weeks, aortic total antioxidants capacity was significantly elevated in groups (III, IV) compared with normal control group while aortic total antioxidant capacity levels was significantly decreased in group (II) compared with normal control group (Table 10).
Table 10.
The changes in aortic total antioxidant capacity levels
| Groups | Mean ± SD | Control | p value |
|---|---|---|---|
| Cholesterol | 0.4333 ± 0.08819 | 1.0022 ± 0.00779 | 0.0001* |
| Cholesterol + curcumin | 1.3341 ± 0.03229 | 1.0022 ± 0.00779 | 0.0001* |
| Rosuvastatin + cholesterol | 1.984 ± 0.11039 | 1.0022 ± 0.00779 | 0.0001* |
The Effect of Curcumin and Rosuvastatin on Serum PCSK 9 Levels
After 12 weeks, serum PCSK9 gene expression was significantly elevated in cholesterol group as well as in rosuvastatin and cholesterol compared with normal control group, whereas significantly reduced in groups(III) (Table 11).
Table 11.
The changes in serum PCSK9 gene expression
| Groups | Mean ± SD | Control | p value |
|---|---|---|---|
| Cholesterol | 78.5921 ± 0.89677 | 67.2071 ± 0.12285 | 0.0001* |
| Cholesterol + curcumin | 73.0476 ± 0.28572 | 67.2071 ± 0.12285 | 0.0001* |
| Rosuvastatin + cholesterol | 79.1429 ± 1.19491 | 67.2071 ± 0.12285 | 0.0001* |
Histophotometric Sections of the Aortic Arch After 12 weeks in the Four Groups
Cholesterol Group
At the end of study rabbits fed 2% cholesterol diet (Induced untreated) for 12 weeks had showed accumulation of macrophages that form foams cells on the surface of endothelium (Fig. 1).
Cholesterol and Curcumin Group
Histological section from rabbits in this group showed focal area of foam cell collected under aortic endothelium (Fig. 2).
Fig. 2.
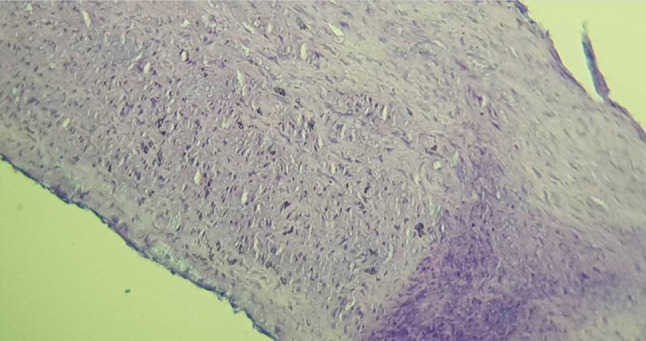
Photomicrograph of histophotometric section of the aortic arch showed focal area of foam cell collected under aortic endothelium
Cholesterol and Rosuvastatin
Histological section from rabbits in this group showed intact aortic endothelium (Fig. 3).
Fig. 3.
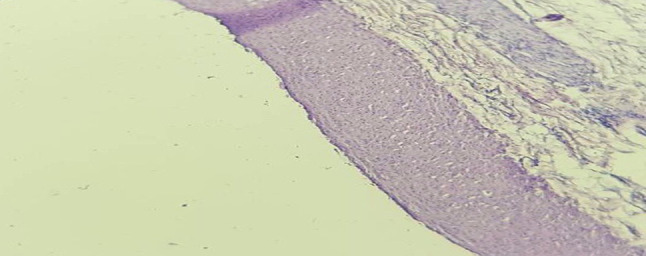
Photomicrograph of histophotometric section of the arch of aorta showed intact aortic endothelium
Discussion
Atherosclerosis is a major cause of cardiac ischemia that leads to myocardial infarction, angina and heart failure. Cholesterol and saturated fatty acids are the main contributors for development of atherosclerosis by adding to cholesterol in the arterial wall that will causes arterial narrowing with consequent reduction in oxygen supply to the heart [10].
Effect on Lipid Profile
At the end of the study; serum cholesterol, TG, LDL, VLDL were significantly decreased in hyperlipidemic rabbits treated with rosuvastatin while HDL levels were significantly high. This is in accordance with Yamazaki D et al. 2013 who showed that rosuvastatin has an effective role either alone or in combination in lowering lipid profile parameters and inflammatory markers with improvement in serum HDL level. [6] Rabbits treated with curcumin got significant reduction in total cholesterol, triglyceride, LDL and VLDL levels with improvement in HDL levels but less than that with rosuvastatin-treated rabbits this is in accordance with Shin et al. [6, 11].
Effect on Inflammatory Markers
Serum hs C-reactive protein, ICAM and VCAM levels were significantly increased in cholesterol fed group when compared with normal control group, this is going with Mazidi et al. [12]. Treatment of rabbits with either curcumin or rosuvastatin was significantly decreased serum hs C-reactive protein, ICAM and VCAM levels in hyperlipidemic rabbits which is in accordance with several studies. [13–15].
Effect on Aortic Antioxidant Capacity
Aortic antioxidant capacity level was significantly decreased in cholesterol group (II) when compared with normal diet group (I).However, treatments of rabbits with either rosuvastatin (group III) or curcumin (group IV) significantly increased antioxidant capacity level when compared with untreated cholesterol diet group [16, 17].
Effect on PCSK9 Expression
Raised PSCK9 serum level in hypercholesterolemic rabbits compared with normal untreated group is in an agreement with Page and Watts [18] who demonstrated that hypercholesterolemia cause PCSK9 gene mutation and increase its expression leads to degradation of LDL receptor on the surface of hepatocytes and decrease uptake of LDL and increase its level in the circulation. In similar way Lin et al. [19] demonstrated that PCSK9 is an important therapeutic target for decreasing LDL-C. PCSK9 decreases LDL intake from blood stream by enhancing LDL receptor degradation and blocking their passage to the cell surface [19]. Many studies have demonstrated that dietary curcumin as a powder has a good effect in the treatment of atherosclerosis and hyperlipidemia in addition to that it is safe with low toxicity [11, 13].
Serum level of PCSK9 was decreased significantly in curcumin exposed group compared with cholesterol group and this result is similar to Tai et al. [20] who elucidated the effect of curcumin in down-regulation of gene expression at the level of cell surface so increase uptake of LDL in the liver hepatocytes. Serum PCSK9 level was reduced in Rosuvaststin treated group which was similar to Nozue et al. [21] who explained the effect of statins in decreasing hepatic intracellular cholesterol, so the number of LDL receptors were elevated and level of PCSK9 protein also elevated in hepatic cell. When doses of statin are for long time, it will increase the level of circulating PCSK9 due to a decline in intracellular cholesterol in liver that elevated SREBP2 (sterol regulatory element binding protein 2) which is responsible for increment in gene expression of PCSK9, Increase in the level of PCSK9 in circulation, and increase activation of LDL receptors [21].
Funding
None.
Compliance with Ethical Standards
Conflict of interest
All authors declare no conflict of interests.
Ethical Standards
All the procedures performed in this study were in accordance with the ethical standards of the Institutional Ethical and research committee.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Ilhan F, Kalkanli ST. Atherosclerosis and the role of immune cells. World J Clin Cases. 2015;16:345–352. doi: 10.12998/wjcc.v3.i4.345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Boamponsem AG. The role of inflammation in atherosclerosis. Pelagia Res Libr. 2011;2:194–207. [Google Scholar]
- 3.Wu MY, Li CJ, Hou MF, Chu PY. New insights into the role of inflammation in the pathogenesis of atherosclerosis. Int J Mol Sci. 2017;22(18):2034. doi: 10.3390/ijms18102034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Druce I, Abujrad H, Ooi TC. PCSK9 and triglyceride-rich lipoprotein metabolism. J Biomed Res. 2015;20:29. doi: 10.7555/JBR.29.20150052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Olszanecki R, Jawień J, Gajda M, Mateuszuk L, Gebska A, Korabiowska M, et al. Effect of curcumin on atherosclerosis in apoE/LDLR-double knockout mice. J Physiol Pharmacol. 2005;56:627–635. [PubMed] [Google Scholar]
- 6.Yamazaki D, Ishida M, Watanabe H, Nobori K, Oguma Y, Terata Y, et al. Comparison of anti-inflammatory effects and high-density lipoprotein cholesterol levels between therapy with quadruple-dose rosuvastatin and rosuvastatin combined with ezetimibe. Lipids Health Dis. 2013;12:9. doi: 10.1186/1476-511X-12-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Almeida E, Blaquer D, Michiko H, Wilson R, Núñez R. Endothelium function, lipid peroxidation, plasmatic and tissue cholesterol evaluations in mixed dyslipidemia in rabbits treated with Rosuvastatin and atorvastatin. Clínica e Investigaciónen Arteriosclerosis. 2009;21:263–267. doi: 10.1016/S0214-9168(09)72954-7. [DOI] [Google Scholar]
- 8.Hietanen E, Aitio A, Koivusaari U, Kilpiö J, Nevalainen T, Närhi M, et al. Tissue concentrations and interaction of zinc with lead toxicity in rabbits. Toxicology. 1982;25:113–127. doi: 10.1016/0300-483X(82)90023-3. [DOI] [PubMed] [Google Scholar]
- 9.Oguntoye CO, Oke BO. A comparison of xylazine/ketamine, diazepam/ketamine and acepromazine/ketamine anaesthesia in rabbit. Sokoto J Vet Sci. 2014;12:21–25. doi: 10.4314/sokjvs.v12i3.4. [DOI] [Google Scholar]
- 10.Zhao Y, Fukao K, Zhao S, Watanabe A, Hamada T, Yamasaki K, et al. Irbesartan attenuates atherosclerosis in Watanabe heritable hyperlipidemic rabbits: noninvasive imaging of inflammation by 18F-fluorodeoxyglucose positron emission tomography. Mol Imaging. 2015 doi: 10.2310/7290.2015.00004. [DOI] [PubMed] [Google Scholar]
- 11.Shin SK, Ha TY, McGregor RA, Choi MS. Long-term curcumin administration protects against atherosclerosis via hepatic regulation of lipoprotein cholesterol metabolism. Mol Nutr Food Res. 2011;55:1829–1840. doi: 10.1002/mnfr.201100440. [DOI] [PubMed] [Google Scholar]
- 12.Mazidi M, Gao HK, Vatanparast H, Kengne AP. Impact of the dietary fatty acid intake on C-reactive protein levels in US adults. Medicine. 2017;96(7):e5736. doi: 10.1097/MD.0000000000005736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wojcik M, Krawczyk M, Wojcik P, Cypryk K, Wozniak LA. Molecular mechanisms underlying curcumin-mediated therapeutic effects in type 2 diabetes and cancer. Oxid Med Cell Longev. 2018 doi: 10.1155/2018/9698258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rohilla A, Rohilla S, Kumar A, Khan MU, Deep A. Pleiotropic effects of statins: a boulevard to cardioprotection. Arab J Chem. 2016;9:21–27. doi: 10.1016/j.arabjc.2011.06.025. [DOI] [Google Scholar]
- 15.Hussein SA, El-Senosi YA, Ragab MR, Hammad MF. Hypolipidemic effect of curcumin in hyper-cholesterolemic rats. Benha Vet Med J. 2014;27:277–289. [Google Scholar]
- 16.Aldosari S, Awad M, Harrington EO, Sellke FW, Abid MR. Subcellular reactive oxygen species (ROS) in cardiovascular pathophysiology. Antioxidants (Basel) 2018 doi: 10.3390/antiox7010014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Liu Z, Huang P, Law S, Tian H, Leung W, Xu C. Preventive effect of curcumin against chemotherapy-induced side-effects. Front Pharmacol. 2018;9:1374. doi: 10.3389/fphar.2018.01374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Page MM, Watts GF. PCSK9 inhibitors–mechanisms of action. Aust Prescr. 2016;39:164. doi: 10.18773/austprescr.2016.060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lin XL, Xiao LL, Tang ZH, Jiang ZS, Liu MH. Role of PCSK9 in lipid metabolism and atherosclerosis. Biomed Pharmacother. 2018;104:36–44. doi: 10.1016/j.biopha.2018.05.024. [DOI] [PubMed] [Google Scholar]
- 20.Tai MH, Chen PK, Chen PY, Wu MJ, Ho CT, Yen JH. Curcumin enhances cell-surface LDLR level and promotes LDL uptake through downregulation of PCSK9 gene expression in HepG2 cells. Mol Nutr Food Res. 2014;58:2133–2145. doi: 10.1002/mnfr.201400366. [DOI] [PubMed] [Google Scholar]
- 21.Nozue T. Lipid lowering therapy and circulating PCSK9 concentration. J Atheroscler Thromb. 2017;24:895–907. doi: 10.5551/jat.RV17012. [DOI] [PMC free article] [PubMed] [Google Scholar]