

Abstract
Background
Appropriate management and prevention of both under‐ and overtreatment in older skin cancer patients can be challenging. It could be helpful to incorporate frailty screening in dermato‐oncology care, since frailty is associated with adverse health outcomes.
Objectives
This study aimed to identify and prioritize the requirements a frailty screening tool (FST) should fulfil in dermato‐oncology practice and to select the best existing FST(s) for this purpose.
Methods
A modified two‐round Delphi procedure was performed among 50 Italian and Dutch specialists and patients to review and prioritize a list of potential FST requirements, using a 5‐point Likert scale. Consensus was defined as a mean score of ≥4.0. A systematic literature search was performed to identify existing multidomain FSTs, which were then assessed on the requirements resulting from the modified Delphi procedure.
Results
Consensus was achieved on evaluation of comorbidities (4.3 ± 0.7), polypharmacy (4.0 ± 0.9) and cognition (4.1 ± 0.8). The FST should have appropriate measurement properties (4.0 ± 1.0), be quickly executed (4.2 ± 0.7), clinically relevant (4.3 ± 0.7), and both easily understandable (4.1 ± 1.2) and interpretable (4.3 ± 0.7). Of the 26 identified FSTs, four evaluated the content‐related domains: the Geriatric‐8 (G8), the modified Geriatric‐8 (mG8), the Groningen Frailty Indicator (GFI) and the Senior Adult Oncology Program 2 (SAOP2) screening tool. Of these, the G8 was the most extensively studied FST, with the best psychometric properties and execution within 5 min.
Conclusions
The G8 appears the most suitable FST for assessing frailty in older adults with skin cancer, although clinical studies assessing its use in a dermato‐oncology population are needed to further assess whether or not frailty in this particular patient group is associated with relevant outcomes (e.g. complications and mortality), as seen in previous studies in other medical fields.
Introduction
Physicians are increasingly confronted with older adult patients with skin cancer. The majority of skin cancers are characterized by a relatively low‐malignant potential, but can cause significant morbidity in the long term. Therefore, appropriate management and prevention of both under‐ and overtreatment in this population can be challenging. In current clinical guidelines, treatment choices are mainly based on tumour‐related characteristics, while patient‐related characteristics seem relatively underrepresented. 1 , 2 However, factors as life expectancy and expected patient burden of both the tumour and the treatment are of vital importance to determine to what extent a patient will benefit from a certain therapy, although not always easily predicted. 2
Frailty is a clinical syndrome, defined as a state in which depletion of physiological reserves leads to adverse health outcomes and low tolerability of stress. 3 , 4 In several medical oncology fields, frailty has been demonstrated to be associated with increased disability, functional dependence, institutionalization and the risk of mortality. To detect frailty, a comprehensive geriatric assessment ([C]GA) can be performed, evaluating somatic, psychosocial and functional domains. 3 , 4 , 5 , 6 , 7 However, these assessments are time‐consuming and therefore may not be feasible for the many older adult patients seen in dermatologic practice. 8 , 9 , 10 , 11 , 12 , 13
Multidimensional frailty screening tools (FSTs) can be used as brief evaluations to detect which patients are in need of or most likely to benefit from a more extensive evaluation by a geriatric assessment. 4 There is a wide variety of available FSTs used in oncology patients. Data on selecting a suitable FST in dermatologic oncology patients are currently lacking, although multiple studies conclude that more guidance on medical decision‐making in frail skin cancer patients is needed to improve personalized medical decision‐making and the prevention of both under‐ and overtreatment. 1 , 14
This study aimed to identify and prioritize the most important requirements a multidimensional FST should fulfil in dermato‐oncology care for older adults and to select the best existing FST(s) for this purpose from a systematic review of the available literature.
Methods
A mixed‐methods approach was used combining a modified Delphi procedure and a systematic literature review.
Modified Delphi procedure
Between April 2018 and March 2019, an international modified 2‐phase Delphi procedure was performed to achieve a consensus on the requirements a FST should fulfil for the target population of older adults with skin cancer. 15 The study was facilitated by an online survey methodology (SurveyMonkey Inc., San Mateo, CA, USA). The survey included items related to content, quality and clinical applicability of the FST, based on previous research and experiences of interdisciplinary experts.
In the first round, 22 items were presented followed by a short list of demographic questions. Respondents were encouraged to comment on the relevance of items; missing items could be added, and statements could be rephrased or removed. Suggestions from participants were used to adjust the statements for the second round, in which participants were asked to grade the importance of each FST requirement using a 5‐point Likert scale, a higher score indicating an item was considered more important. Consensus was defined as a group mean score of ≥4.0. Descriptive statistics were performed on demographic variables. Continuous variables were summarized using the mean and standard deviation and categorical variables were expressed as frequencies and percentages. All data were collected using SurveyMonkey and analyzed using SPSS Statistics for Windows, version 25.0 (IBM, Armonk, NY, USA). This study was conducted according to the Standards for Reporting Qualitative Research (SRQR). 16
Participants of the Delphi procedure
A multidisciplinary working group of Dutch and Italian experts and patients was formed. To represent all specialties involved in skin cancer care, the expert group consisted of dermatologists, plastic surgeons, otorhinolaryngologists, oral and maxillofacial surgeons, radiotherapists and geriatricians, who all had extensive clinical experience in skin cancer and/or geriatric care. Age, gender, healthcare setting and years of experience were taken into account to optimize a well‐balanced working group. National guideline committees in the field of dermato‐oncology or frailty were represented by one or multiple members. Seven skin cancer patients from outpatient clinics in both Italy and the Netherlands participated as well; the majority aged 70 years or older.
Potential respondents were approached by the investigators, who explained the study and requested participation. Agreeing to participate was construed as informed consent. Participants who did not fill out the survey were sent two reminders by e‐mail, after which all participants were contacted personally or by phone. Interrespondent anonymity was maintained to ensure no respondents were influenced by the identities of other participants.
Systematic literature search
A systematic literature search was conducted to identify available multidimensional FSTs combining the search terms ‘frailty’, ‘screening’ and ‘cancer’. PubMed, EMBASE, Cochrane Library, SUMSearch and Trip Database were searched up to 16 May 2019, as well as websites of relevant organizations, and guidelines on FSTs (Tables S1 and S2). Manual review of the abstracts as well as a full‐text evaluation was independently performed by two reviewers. In case of disagreement, consensus was achieved by discussion. Articles were excluded if written in any language other than English, Dutch, German, French, Spanish or Italian. FSTs assessing a single domain or FSTs including physical, laboratory or imaging techniques were also excluded, as well as conference abstracts or articles of which full‐text remained unavailable after contacting the authors. This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA). 17
Assessment of identified FSTs
All identified FSTs were assessed on the presence of the content‐related items as presented in round 2 of the modified Delphi procedure. FSTs assessing all of the content‐related domains that met consensus were further assessed on psychometric properties with the aid of the Consensus‐based Standards for the selection of health Measurement Instruments (COSMIN) checklist. 18 All related articles on the selected FSTs were evaluated on relevant characteristics. In case of missing data, the FST developers were contacted and if necessary additional measurements were performed by the research team.
Results
Multidisciplinary working group characteristics
Of the 53 working group members who agreed to participate in the study, 50 (94.3%) consented and completed the first round. Only respondents who completed round 1 were invited for the second round, in which a response rate of 92.0% (n = 46) was achieved. The working group characteristics are summarized in Table 1.
Table 1.
Multidisciplinary working group characteristics of this modified Delphi study on requirements a multidimensional frailty screening tool (FST) should fulfil in dermato‐oncology care
| Working group characteristics | Value |
|---|---|
| Age (years), mean ± SD | |
| Specialists | 47.3 ± 8.3 |
| Patients | 73.1 ± 17.2 |
| Gender, n (%) | |
| Male | 25 (50.0) |
| Female | 25 (50.0) |
| Specialists, n (%) | 43 (86.0) |
| Dermatologist | 23 (46.0) |
| Radiation therapist | 4 (8.0) |
| (Facial) surgeons† | 11 (22.0) |
| Geriatrician or elderly care physician | 5 (10.0) |
| Years of experience‡, mean ± SD | 15.8 ± 8.9 |
| Patients, n (%) | 7 (14.0) |
| Healthcare setting, n § (%) | |
| General hospital | 14 (27.5) |
| Academic hospital | 30 (58.8) |
| Private practice | 5 (9.8) |
| Other | 2 (3.9) |
(Facial) surgeons included plastic surgeons, otorhinolaryngologists, or oral and maxillofacial surgeons.
Years of experience in skin cancer care.
Including multiple specialists working in more than one treatment facility.
Composition and prioritization of the list of items
In round 1, both patients and experts were requested to express their thoughts on the initial set of 22 statements presented as possible requirements for a FST. Consequently, 12 items were rephrased, five were deleted, and two were added. In the second round, the final 19‐item list (Table S3) was prioritized by the respondents with an overall mean score of 3.7 ± 0.5.
Consensus was met concerning the evaluation of comorbidities (mean 4.3 ± 0.7), polypharmacy (4.0 ± 0.9) and cognition (4.1 ± 0.8). Other FST characteristics for which consensus was met were appropriate measurement properties (4.0 ± 1.0), easy interpretation of the outcome (4.3 ± 0.7), suitability for low‐literate and low‐educated patients (4.1 ± 1.2), quick completion of the FST (4.2 ± 0.7) and a clinically relevant outcome (4.3 ± 0.7). No consensus was reached on the other potential FST requirements, including whether the screening tool should be filled in by patients or medical workers. A complete overview of the results is provided in Fig. 1. Outcomes were consistent when only responses of dermatologists were analyzed (data not shown).
Figure 1.
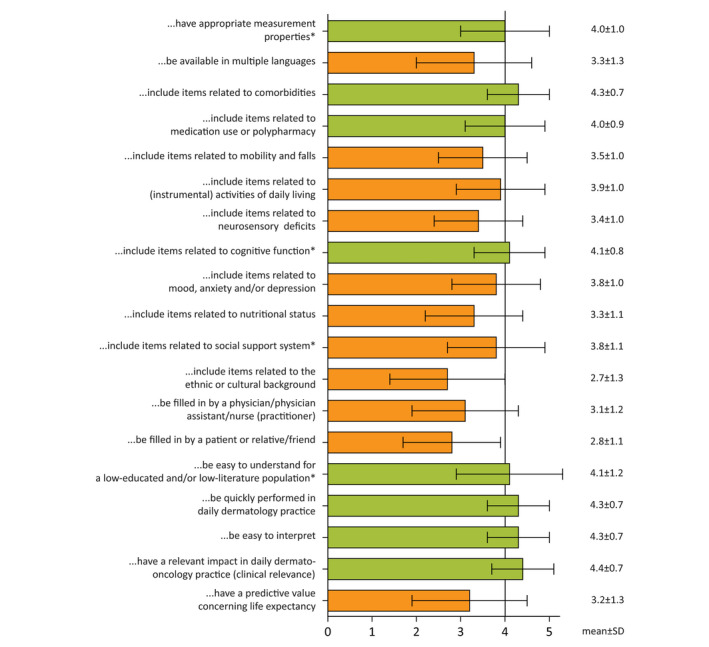
Results of the multidisciplinary modified Delphi study on requirements a multidimensional frailty screening tool (FST) should fulfil in dermato‐oncology practice. Each statement started with ‘The screening tool should…’. Green bars represent those in which consensus was achieved; consensus was defined as a mean score ≥4.0. Orange bars represent items that did not reach consensus, e.g. a mean score of <4.0. *Complete statements can be found in Table S3.
Systematic literature search and FST selection
An initial search for FSTs generated 1354 publications. A total of 439 duplicates were removed. Of the remaining 915 publications, titles and abstracts were screened for eligibility, after which 54 articles remained for full‐text screening. A total of 26 unique FSTs were identified after full‐text evaluation. 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 47 A flow chart on the literature search and reasons for exclusion can be found in the Fig. S1.
Subsequently, FSTs were assessed for the inclusion of the domains which met consensus in the final Delphi round. Eighteen tools (69.2%) contained items related to comorbidity or self‐reported health assessment, 8 (30.8%) on the evaluation of polypharmacy and 16 (61.5%) on the evaluation of cognitive function. Table 2 lists the domains included in each of the identified FSTs.
Table 2.
Content‐related domains of each frailty screening tool (FST) as identified by the systematic literature search
| Frailty screening tool | Comorbidities | Medication use or polypharmacy | Mobility and falls | (instrumental) Activities of daily living | Neurosensory deficits | Cognitive function | Mood, anxiety, and/or depression | Nutritional status | Social support | Ethnic/cultural background |
|---|---|---|---|---|---|---|---|---|---|---|
| Abbreviated comprehensive geriatric assessment (aCGA) 38 | − | − | + | + | − | + | + | − | − | − |
| Barber questionnaire 24 | +/− | − | − | + | + | − | − | − | + | − |
| Cancer‐specific geriatric assessment (SAKK C‐SGA) 25 | + | − | + | + | − | + | + | + | + | − |
| Clinical Frailty Scale 42 | +/− | − | − | + | − | − | +/− | − | − | − |
| Fatigue, Resistance, Ambulation, Illnesses and Loss of weight scale (FRAIL scale) 23 | + | − | + | − | − | − | − | + | − | − |
| Geriatric‐8 (G8) 19 | +/− | + | + | − | − | + | + | + | − | − |
| Modified G8 (Martinez‐Tapia version) 20 | + | + | + | + | − | + | + | + | − | − |
| Modified G8 (Petit‐Monéger version) 41 | +/− | + | + | + | − | − | − | + | − | − |
| Groningen Frailty Indicator (GFI) 22 , 45 | +/− | + | + | + | + | + | + | + | + | − |
| Identification of Seniors at Risk (ISAR) 34 | − | + | − | + | + | +/− | − | − | − | − |
| Identification of Seniors At Risk‐Hospitalized patients (ISAR‐HP) 30 | − | − | + | + | − | − | − | − | − | − |
| Identification of Seniors At Risk‐Primary Care (ISAR‐PC) screening instrument 46 | − | − | − | + | − | +/− | − | − | − | − |
| International Myeloma Working Group frailty score (IMWG frailty score) 39 | + | − | + | + | − | − | − | − | − | − |
| Kihon checklist (KCL) 26 , 36 , 47 | − | − | + | + | − | + | + | + | − | − |
| Korean Cancer Study Group Geriatric Score (KG‐7) 32 | − | + | + | + | − | + | +/− | +/− | − | − |
| Modified frailty index (Lascano version) 33 | + | − | + | + | − | + | − | + | − | − |
| Modified frailty index (Patel version) 40 | + | − | + | + | − | + | + | − | − | − |
| Program of Research to Integrate Services for the Maintenance of Autonomy Screening Instrument (PRISMA‐7) 29 | +/− | − | + | + | − | − | − | − | + | − |
| Risk analysis index (RAI) 31 | + | − | + | + | − | + | − | + | − | − |
| Rockwood Frailty Scale 43 | − | − | + | + | − | + | − | − | − | − |
| Senior Adult Oncology Program 2 (SAOP2) screening questionnaire 21 | +/− | + | + | + | − | + | + | + | + | − |
| Tilburg Frailty Indicator (TFI) 28 | + | − | + | + | + | +/− | + | + | + | + |
| The Older Persons and Informal Caregivers Survey Frailty Index (TOPICS‐FI38) 27 | + | − | + | + | − | + | + | − | − | − |
| Triage Risk Screening Tool (TRST) 35 | − | + | + | − | − | + | − | − | − | − |
| Vulnerable Elders Survey‐13 (VES‐13) 44 | +/− | − | + | + | − | − | − | − | − | − |
| VES‐13 + anhedonia 37 | +/− | − | + | + | − | − | +/− | − | − | − |
+ indicating the domain was assessed in the screening tool, +/− indicating the domain was assessed, although minimally or self‐rated, − indicating an absence of the domain in the screening tool.
In four FSTs, the assessment of comorbidities/self‐reported health, polypharmacy and cognitive function was included: the Geriatric‐8 (G8), the modified Geriatric‐8 (mG8), the Groningen Frailty Indicator (GFI) and the Senior Adult Oncology Program 2 (SAOP2) screening tool. 19 , 20 , 21 , 22 , 45 The G8 and mG8 can be performed within 5 min; the GFI and SAOP2 can be completed in 10 min. 4 , 6 , 10 , 48 , 49 All four FSTs have clear cut‐off points to identify frail patients in need of more extensive geriatric evaluation. No studies were available on the suitability of the (m)G8, GFI and SAOP2 for low‐literate or low‐educated patients, nor on the clinical relevance and impact of the outcomes in daily dermato‐oncology practice.
Table 3 summarizes general and psychometric characteristics of the selected FSTs, including sensitivity and specificity on predicting frailty with a (C)GA as a reference test. The screening methods included in the reference (C)GA differed among the included studies and the cut‐off point determining frailty varied between ≥1 and ≥2 deficiencies (Table S4). The included studies assessing the G8 and GFI showed the least risk of bias according to the modified COSMIN standards (Table 3).
Table 3.
Measurement properties of the frailty screening tools (FSTs) assessing all content‐related domains that met consensus in this modified Delphi study, based on Consensus‐based Standards for the selection of health Measurement Instruments (COSMIN) standards 18
| G8 10 , 11 , 12 , 13 , 19 , 48 , 50 , 51 , 52 , 53 , 54 , 55 , 56 , 57 , 58 , 59 , 60 , 61 , 62 , 63 , 64 , 65 | mG8 20 , 61 | GFI 13 , 49 , 59 , 62 , 66 , 67 , 68 | SAOP2 12 , 21 | ||
|---|---|---|---|---|---|
| General aspects | Questionnaire type | Physician assessed | Physician assessed |
Physician assessed version available Self‐assessed version available |
Partly physician assessed Partly self‐assessed |
| Number of items | 8 | 6 | 15 | 27 | |
| Cut‐off point† | ≤14 | ≥6 | ≥4 | ≥2 | |
| Score range | 0–17 | 0–35 | 0–15 | 0–10§ | |
| Duration of screening‡ | + | + | +/− | +/− | |
| Multilingual support | + | − | + | + | |
| Reliability | Internal consistency | +/− | − | + | − |
| Reliability | + | +/− | + | − | |
| Measurement error | + | − | + | − | |
| Validity | Content validity | +/− | +/− | + | +/− |
| Structural validity | + | +/− | + | +/− | |
| Construct validity | + | +/− | + | +/− | |
| Criterion validity | + | + | + | + | |
| Cross‐cultural validity | + | + | + | + | |
| General measurement properties | Validation | + | + | + | + |
| Sensitivity | 38–100¶ | 89–92 | 39–76 | 94–100 | |
| Specificity | 3–100 | 36–79 | 52–89 | 40–50 |
G8, Geriatric‐8; GFI, Groningen Frailty Index; mG8, modified Geriatric‐8; SAOP2, Senior Adult Oncology Program 2 (SAOP2) screening questionnaire.
Cut‐off determining a positive frailty screening test, indicating necessity of multidisciplinary (C)GA.
+ indicating the FST could be completed within 5 min, +/− indicating the FST could be completed within 10 min, − indicating the FST could be completed in 10 min or more.
No total score available; a total of 10 domains are assessed with varying scoring methods per domain.
69.6% of the included studies assessing the G8 maintained a sensitivity of 80% or higher.
Discussion
Management of skin cancer in older patients can be challenging due to various patient‐related factors influencing treatment decisions and outcomes, such as limited life expectancy and frailty. Frailty screening tools (FSTs) are available to identify patients in need for more extensive geriatric assessment, but are currently rarely used in older patients with cutaneous malignancies. The aim of this study was to identify and prioritize the requirements for a FST in dermato‐oncology daily practice and to select the best‐fitting existing FST(s). A FST could assist dermatologists in selecting those patients in need for a more extensive geriatric assessment, establishing personalized treatment options or include additional preparations to minimize the risk of adverse health outcomes.
According to this modified Delphi study, a FST suitable for dermato‐oncology patients should minimally include evaluation of comorbidities, polypharmacy and cognition. A quick execution of the FST is necessary, and the FST should be suitable for a low‐literate population. Four of the 26 FSTs that were identified by the literature review included the required domains: The Geriatric‐8 (G8), the modified Geriatric‐8 (mG8), the Groningen Frailty Indicator (GFI) and the Senior Adult Oncology Program 2 (SAOP2) screening tool. 19 , 20 , 21 , 22 , 45 The G8 is the most extensively studied tool with appropriate measurement properties when compared to a full GA. 10 , 11 , 12 , 13 , 19 , 48 , 50 , 51 , 52 , 53 , 54 , 55 , 56 , 57 , 58 , 59 , 60 , 61 , 62 , 63 , 64 , 65 In the few articles studying the recently developed mG8, sensitivity (89–92%) and specificity (36–79%) for geriatric impairments detected by GA appear higher than the original G8. 20 , 61 However, the mG8 is currently only available in a limited number of languages. The GFI, although frequently used, has a relatively low sensitivity (39–76%), which is an important shortcoming for a well‐functioning FST. 13 , 49 , 59 , 62 , 66 , 67 , 68 Only two articles could be identified studying the SAOP2 screening tool, which showed a high sensitivity (94–100%) and a low specificity (40–50%). 12 , 21 The SAOP2 is the most time‐intensive tool when compared to the (m)G8 and GFI. None of the articles studying the (m)G8, GFI or SAOP2 provided information on the education level of the patients, nor reviewed whether low‐literate patients understood all questions. Based on the results of this study, the G8 appears the most suitable FST for assessing frailty in older adults with skin cancer, but relevant clinical studies assessing its use in a dermato‐oncology population are currently lacking.
Several studies address the need for implementation of frailty screening in dermatology–oncology care. 1 , 14 , 69 Rogers et al. 14 concluded that comorbidity indices and chronological age alone did not adequately explain survival rate differences in non‐melanoma skin cancer patients. Bras et al., 70 assessed frailty in 90 patients with head‐and‐neck malignancies, including 45 skin cancer patients in need of major surgery, mostly under general anaesthesia. Frailty was associated with a non‐significant lower overall survival rate and no significant differences in complication rates between frail patients and robust patients were seen in this relatively small population with heterogeneous underlying diseases. 70 Valdatta et al., 71 however, did find a higher complication and mortality rate in frail patients undergoing reconstructive surgery after non‐melanoma skin cancer surgery. These studies used various instruments to detect frailty, frequently based on those frailty‐related aspects that were fortuitously available from retrospectively extracted clinical data, which highly limits comparison and generalizability. Many studies have been conducted in other medical fields, including various oncology populations, indicating a strong association between frailty and adverse health outcomes after treatment. 48 , 56 , 72 However, the association of frailty with complications and mortality seen in previous studies might not be applicable to dermato‐oncology. Therefore, more research on the consequences of frailty for dermatological oncology patients is needed.
It should be noted that the items that reached consensus in this modified Delphi study might reflect domains that are already currently considered as important factors in skin cancer care. Domains as malnutrition and mobility were valued as less important, although these have been proven to be vital domains in frailty screening as well as in geriatric oncology. 3 , 7 , 8 , 72 The use of a FST could assist physicians in assessing these domains in addition to other clinically relevant domains as comorbidity, medication and cognitive function. More awareness should be raised for these and other frailty‐related aspects in dermatology, as suggested by previous research. 1 The (m)G8 does not only assess self‐reported health, polypharmacy and dementia, but also reviews additional factors associated with treatment‐related outcomes in several other oncology fields.
In this study, only FSTs that did not require physical or laboratory tests were included. Since dermatologic consultations are often short, it was estimated that a FST would not be used in daily dermatology practice if extensive assessments were required. However, a FST is not meant to replace clinical judgement, nor to include all possible domains that could influence therapy choices. Personalized medical decision‐making should be strived at in every patient, including tumour‐related aspects, patient preferences and patient‐related aspects, of which frailty could be an important factor in prediction of adverse health outcomes.
Frailty screening tools have been developed to identify those patients in need for a more extensive assessment. 4 A full GA was therefore considered as the gold standard for the identification of frailty. 5 However, no consensus exists on the components of a (C)GA nor on the cut‐off point defining frailty, 5 , 7 , 73 which led to heterogeneity among the included studies and outcomes (Table S4). Questionable is whether or not the presented psychometric properties of the FSTs are applicable to a dermato‐oncology setting, since these patients might be in better health in comparison with the populations previously studied. 14 More research is needed to assess the clinical relevance and feasibility of frailty screening in dermato‐oncology and the consequences of frailty on risks associated with dermato‐oncology therapies. Application of frailty screening and geriatric assessments in the busy dermato‐oncology practice may prove challenging, due to the broad spectrum of morbidity associated with skin cancer in older patients and the heterogeneity of clinical settings (outpatient vs. inpatient vs. specialized skin cancer clinics) across different European countries. Nonetheless, a personalized and frailty‐based clinical management in combination with a shared, rational clinimetric framework may support a more patient‐based clinical decision‐making process, especially in the presence of expanding therapeutic options for skin cancer.
Conclusion
More attention for frailty screening in dermato‐oncology is generally desired, but clinical studies are currently limited. Based on this study, the assessment of comorbidities, polypharmacy and cognition should at least be covered by a FST. The FST should have appropriate measurement properties, be quickly executed, clinically relevant, and both easily understandable and interpretable. The G8, mG8, GFI and SAOP2 are possible suitable FSTs, of which the G8 seems the most appropriate existing FST for dermato‐oncology practice. More studies are needed to test the clinical relevance of frailty screening and the use of different FSTs in daily practice.
Supporting information
Table S1. Systematic literature search to identify frailty screening tools.
Table S2. List of relevant websites and organizations included in the systematic search to identify frailty screening tools.
Table S3. Statements as presented in round 2 of the modified Delphi procedure on the requirements a frailty screening tool should fulfil in older dermato‐oncology patients.
Table S4. Sensitivity and specificity of the included frailty screening tools.
Figure S1. Flow‐chart of the systematic search to identify frailty screening tools.
Acknowledgements
We would like to thank all patients who participated in this study. Furthermore, we would like to thank the other working group members from the Italian Group of Dermato‐oncology (GIDO) of the Italian Society of Dermatology and Venereology (SIDeMaST) and the Dutch Society of Dermatology and Venerology (NVDV). In particular, we would like to thank all specialists who participated in this study: H. Alkemade, G. Argenziano, P. Arnold, L. Atzori, G. Babino, R. Borgonjen, F. Bussu, P. Calzavara‐Pinton, A. Campanati, M. Concetta Fargnoli, A. Conti, E. Corten, G. Damen, J. Eikelboom, R. van Es, A. Ferrini, S. Festen, P. Gentile, S. Gentileschi, R. Gerritsen, S. den Hengst, M. van Hezewijk, K. Ingels, N. Kelleners‐Smeets, G. Krekels, D. La Carpia, F. Lacarrubba, V. Lancellotta, T. Merkx, E. Migliano, R. Mommers, A. Moro, C. Mouës‐Vink, M. Olde Rikkert, N. Pimpinelli, P. Quaglino, F. Ricci, M. van Rossum, R. Saraceno, M. Tjioe, L. Vicenzi, B. Visch and E. Zwijnenburg.
Conflicts of interest
The authors declare no conflict of interest.
Funding source
None.
References
- 1. Lubeek SF, Borgonjen RJ, van Vugt LJ et al Improving the applicability of guidelines on nonmelanoma skin cancer in frail older adults: a multidisciplinary expert consensus and systematic review of current guidelines. Br J Dermatol 2016; 175: 1003–1010. [DOI] [PubMed] [Google Scholar]
- 2. Linos E, Parvataneni R, Stuart SE et al Treatment of nonfatal conditions at the end of life: nonmelanoma skin cancer. JAMA Int Med 2013; 173: 1006–1012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Clegg A, Young J, Iliffe S et al Frailty in elderly people. Lancet 2013; 381: 752–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Decoster L, Van Puyvelde K, Mohile S et al Screening tools for multidimensional health problems warranting a geriatric assessment in older cancer patients: an update on SIOG recommendationsdagger. Ann oncol 2015; 26: 288–300. [DOI] [PubMed] [Google Scholar]
- 5. Extermann M, Aapro M, Bernabei R et al Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005; 55: 241–252. [DOI] [PubMed] [Google Scholar]
- 6. Dent E, Kowal P, Hoogendijk EO. Frailty measurement in research and clinical practice: a review. Eur J Int Med 2016; 31: 3–10. [DOI] [PubMed] [Google Scholar]
- 7. Soto‐Perez‐de‐Celis E, Li D, Yuan Y et al Functional versus chronological age: geriatric assessments to guide decision making in older patients with cancer. Lancet Oncol 2018; 19: e305–e316. [DOI] [PubMed] [Google Scholar]
- 8. Balducci L, Extermann M. Management of cancer in the older person: a practical approach. Oncologist 2000; 5: 224–237. [DOI] [PubMed] [Google Scholar]
- 9. Kenis C, Decoster L, Van Puyvelde K et al Performance of two geriatric screening tools in older patients with cancer. J Clin Oncol 2014; 32: 19–26. [DOI] [PubMed] [Google Scholar]
- 10. Soubeyran P, Bellera C, Goyard J et al Screening for vulnerability in older cancer patients: the ONCODAGE Prospective Multicenter Cohort Study. PLoS One 2014; 9: e115060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Dubruille S, Libert Y, Roos M et al Identification of clinical parameters predictive of one‐year survival using two geriatric tools in clinically fit older patients with hematological malignancies: major impact of cognition. J Geriatr Oncol 2015; 6: 362–369. [DOI] [PubMed] [Google Scholar]
- 12. Russo C, Giannotti C, Signori A et al Predictive values of two frailty screening tools in older patients with solid cancer: a comparison of SAOP2 and G8. Oncotarget 2018; 9: 35056–35068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Baitar A, Van Fraeyenhove F, Vandebroek A et al Evaluation of the Groningen Frailty Indicator and the G8 questionnaire as screening tools for frailty in older patients with cancer. J Geriatr Oncol 2013; 4: 32–38. [DOI] [PubMed] [Google Scholar]
- 14. Rogers EM, Connolly KL, Nehal KS et al Comorbidity scores associated with limited life expectancy in the very elderly with nonmelanoma skin cancer. J Am Acad Dermatol 2018; 78: 1119–1124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Linstone HA, Turoff M. Delphi Method: Techniques and Applications, Addison‐Wesley, Reading, MA, 1975. [Google Scholar]
- 16. O'Brien BC, Harris IB, Beckman TJ et al Standards for reporting qualitative research: a synthesis of recommendations. Acad Med 2014; 89: 1245–1251. [DOI] [PubMed] [Google Scholar]
- 17. Moher D, Liberati A, Tetzlaff J et al Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. PLoS Medicine 2009; 6:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Mokkink LB, Terwee CB, Patrick DL et al The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res 2010; 19:539–549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Bellera CA, Rainfray M, Mathoulin‐Pelissier S et al Screening older cancer patients: first evaluation of the G‐8 geriatric screening tool. Ann Oncol 2012; 23: 2166–2172. [DOI] [PubMed] [Google Scholar]
- 20. Martinez‐Tapia C, Canoui‐Poitrine F, Bastuji‐Garin S et al Optimizing the G8 screening tool for older patients with cancer: diagnostic performance and validation of a six‐item version. Oncologist 2016; 21: 188–195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Extermann M, Green T, Tiffenberg G et al Validation of the Senior Adult Oncology Program (SAOP) 2 screening questionnaire. Crit Rev Oncol Hematol 2009; 69: 185. [Google Scholar]
- 22. Schuurmans H, Steverink N, Lindenberg S et al Old or frail: what tells us more? J Gerontol A Biol Sci Med Sci 2004; 59: M962–M965. [DOI] [PubMed] [Google Scholar]
- 23. Abellan van Kan G, Rolland Y, Bergman H et al The I.A.N.A task force on frailty assessment of older people in clinical practice. J Nutr Health Aging 2008; 12: 29–37. [DOI] [PubMed] [Google Scholar]
- 24. Barber JH, Wallis JB, McKeating E. A postal screening questionnaire in preventive geriatric care. J R Coll Gen Pract 1980; 30: 49–51. [PMC free article] [PubMed] [Google Scholar]
- 25. Clough‐Gorr KM, Noti L, Brauchli P et al The SAKK cancer‐specific geriatric assessment (C‐SGA): a pilot study of a brief tool for clinical decision‐making in older cancer patients. BMC Med Inform Decis Mak 2013; 13: 93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Fukutomi E, Okumiya K, Wada T et al Importance of cognitive assessment as part of the "Kihon Checklist" developed by the Japanese Ministry of Health, Labor and Welfare for prediction of frailty at a 2‐year follow up. Geriatr Gerontol Int 2013; 13: 654–662. [DOI] [PubMed] [Google Scholar]
- 27. Geessink N, Schoon Y, van Goor H et al Frailty and quality of life among older people with and without a cancer diagnosis: findings from TOPICS‐MDS. PLoS One 2017; 12: e0189648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Gobbens RJ, van Assen MA, Luijkx KG et al The Tilburg Frailty Indicator: psychometric properties. J Am Med Direct Assoc 2010; 11: 344–355. [DOI] [PubMed] [Google Scholar]
- 29. Hébert R, Durand PJ, Dubuc N et al Frail elderly patients. New model for integrated service delivery. Can Fam Physician 2003; 49: 992–997. [PMC free article] [PubMed] [Google Scholar]
- 30. Hoogerduijn JG, Buurman BM, Korevaar JC et al The prediction of functional decline in older hospitalised patients. Age Ageing 2012; 41: 381–387. [DOI] [PubMed] [Google Scholar]
- 31. Johnson MS, Bailey TL, Schmid KK et al A frailty index identifies patients at high risk of mortality after tracheostomy. Otolaryngology–Head Neck Surg 2014; 150: 568–573. [DOI] [PubMed] [Google Scholar]
- 32. Kim JW, Kim S‐H, Kim YJ et al A novel geriatric screening tool in older patients with cancer: the Korean cancer study group geriatric score (KG)‐7. PLoS One 2015; 10: e0138304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Lascano D, Pak JS, Kates M et al Validation of a frailty index in patients undergoing curative surgery for urologic malignancy and comparison with other risk stratification tools. Urol Oncol 2015; 33: 426.e1–426.e12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. McCusker J, Bellavance F, Cardin S et al Screening for geriatric problems in the emergency department: reliability and validity. Identification of Seniors at Risk (ISAR) Steering Committee. Acad Emerg Med 1998; 5: 883–893. [DOI] [PubMed] [Google Scholar]
- 35. Meldon SW, Mion LC, Palmer RM et al A brief risk‐stratification tool to predict repeat emergency department visits and hospitalizations in older patients discharged from the emergency department. Acad Emerg Med 2003; 10: 224–232. [DOI] [PubMed] [Google Scholar]
- 36. Ogawa K, Fujiwara Y, Yoshida H et al [The validity of the "Kihon Check‐list" as an index of frailty and its biomarkers and inflammatory markers in elderly people]. Nihon Ronen Igakkai Zasshi 2011; 48: 545–552. [DOI] [PubMed] [Google Scholar]
- 37. Okuyama T, Sugano K, Iida S et al Screening performance for frailty among older patients with cancer: a cross‐sectional observational study of two approaches. J Natl Compr Cancer Netw 2015; 13: 1525–1531. [DOI] [PubMed] [Google Scholar]
- 38. Overcash JA, Beckstead J, Extermann M et al The abbreviated comprehensive geriatric assessment (aCGA): a retrospective analysis. Crit Rev Oncol Hematol 2005; 54: 129–136. [DOI] [PubMed] [Google Scholar]
- 39. Palumbo A, Bringhen S, Mateos M‐V et al Geriatric assessment predicts survival and toxicities in elderly myeloma patients: an International Myeloma Working Group report. Blood 2015; 125: 2068–2074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Patel KV, Brennan KL, Brennan ML et al Association of a modified frailty index with mortality after femoral neck fracture in patients aged 60 years and older. Clin Orthop Relat Res 2014; 472: 1010–1017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Petit‐Moneger A, Rainfray M, Soubeyran P et al Detection of frailty in elderly cancer patients: improvement of the G8 screening test. J Geriatr Oncol 2016; 7: 99–107. [DOI] [PubMed] [Google Scholar]
- 42. Rockwood K, Song X, MacKnight C et al A global clinical measure of fitness and frailty in elderly people. CMAJ 2005; 173: 489–495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Rockwood K, Stadnyk K, MacKnight C et al A brief clinical instrument to classify frailty in elderly people. Lancet 1999; 353: 205–206. [DOI] [PubMed] [Google Scholar]
- 44. Saliba D, Elliott M, Rubenstein LZ et al The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community. J Am Geriatr Soc 2001; 49: 1691–1699. [DOI] [PubMed] [Google Scholar]
- 45. Steverink N, Slaets JPJ, Schuurmans H et al Measuring frailty: developing and testing the GFI (Groningen Frailty Indicator). Gerontologist 2001; 41(Special Issue 1): 236. [Google Scholar]
- 46. Suijker JJ, Buurman BM, van Rijn M et al A simple validated questionnaire predicted functional decline in community‐dwelling older persons: prospective cohort studies. J Clin Epidemiol 2014; 67: 1121–1130. [DOI] [PubMed] [Google Scholar]
- 47. Tomata Y, Hozawa A, Ohmori‐Matsuda K et al [Validation of the Kihon Checklist for predicting the risk of 1‐year incident long‐term care insurance certification: the Ohsaki Cohort 2006 Study]. Nihon Koshu Eisei Zasshi 2011; 58: 3–13. [PubMed] [Google Scholar]
- 48. Dottorini L, Catena L, Sarno I et al The role of Geriatric screening tool (G8) in predicting side effect in older patients during therapy with aromatase inhibitor. J Geriatr Oncol 2019; 10: 356–358. [DOI] [PubMed] [Google Scholar]
- 49. Kellen E, Bulens P, Deckx L et al Identifying an accurate pre‐screening tool in geriatric oncology. Crit Rev Oncol Hematol 2010; 75: 243–248. [DOI] [PubMed] [Google Scholar]
- 50. Hamaker ME, Mitrovic M, Stauder R. The G8 screening tool detects relevant geriatric impairments and predicts survival in elderly patients with a haematological malignancy. Ann Hematol 2014; 93: 1031–1040. [DOI] [PubMed] [Google Scholar]
- 51. Hentschel L, Rentsch A, Lenz F et al A questionnaire study to assess the value of the vulnerable elders survey, G8, and predictors of toxicity as screening tools for frailty and toxicity in geriatric cancer patients. Oncol Res Treat 2016; 39: 210–216. [DOI] [PubMed] [Google Scholar]
- 52. Holmes HM, Des Bordes JK, Kebriaei P et al Optimal screening for geriatric assessment in older allogeneic hematopoietic cell transplantation candidates. J Geriatr Oncol 2014; 5: 422–430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Joshi A, Tandon N, Patil VM et al Agreement analysis between three different short geriatric screening scales in patients undergoing chemotherapy for solid tumors. J Cancer Res Ther 2017; 13: 1023–1026. [DOI] [PubMed] [Google Scholar]
- 54. Kenig J, Zychiewicz B, Olszewska U et al Screening for frailty among older patients with cancer that qualify for abdominal surgery. J Geriatr Oncol 2015; 6: 52–59. [DOI] [PubMed] [Google Scholar]
- 55. Osborne GEC, Appleyard SA, Gilbert DC et al Comprehensive geriatric assessment in men aged 70 years or older with localised prostate cancer undergoing radical radiotherapy. Clin Oncol 2017; 29: 609–616. [DOI] [PubMed] [Google Scholar]
- 56. van Walree IC, Scheepers E, van Huis‐Tanja LH et al A systematic review on the association of the G8 with geriatric assessment, prognosis and course of treatment in older patients with cancer. J Geriatr Oncol 2019; 10: 847–858. [DOI] [PubMed] [Google Scholar]
- 57. Velghe A, Petrovic M, De Buyser S et al Validation of the G8 screening tool in older patients with aggressive haematological malignancies. Eur J Oncol Nurs 2014; 18: 645–648. [DOI] [PubMed] [Google Scholar]
- 58. Yokom DW, Alibhai SMH, Sattar S et al Geriatric oncology screening tools for CGA‐based interventions: results from a phase II study of geriatric assessment and management for older adults with cancer. J Geriatr Oncol 2018; 9: 683–686. [DOI] [PubMed] [Google Scholar]
- 59. Smets IH, Kempen GI, Janssen‐Heijnen ML et al Four screening instruments for frailty in older patients with and without cancer: a diagnostic study. BMC Geriatr 2014; 14: 26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Luce S, De Breucker S, Van Gossum A et al How to identify older patients with cancer who should benefit from comprehensive geriatric assessment? J Geriatr Oncol 2012; 3: 351–358. [Google Scholar]
- 61. Pamoukdjian F, Canoui‐Poitrine F, Longelin‐Lombard C et al Diagnostic performance of gait speed, G8 and G8 modified indices to screen for vulnerability in older cancer patients: the prospective PF‐EC cohort study. Oncotarget 2017; 8: 50393–50402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. van Loon IN, Goto NA, Boereboom FTJ et al Frailty screening tools for elderly patients incident to dialysis. Clin J Am Soc Nephrol 2017; 12: 1480–1488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. de Thezy A, Lafargue A, d'Arailh L et al Relevance of G8 scale in referring elderly patients with aortic stenosis requiring a TAVI for a geriatric consultation. Geriatr Psychol Neuropsychiatr Vieil 2017; 15: 357–363. [DOI] [PubMed] [Google Scholar]
- 64. Liuu E, Canoui‐Poitrine F, Tournigand C et al Accuracy of the G‐8 geriatric‐oncology screening tool for identifying vulnerable elderly patients with cancer according to tumour site: the ELCAPA‐02 study. J Geriatr Oncol 2014; 5: 11–19. [DOI] [PubMed] [Google Scholar]
- 65. Pottel L, Boterberg T, Pottel H et al Determination of an adequate screening tool for identification of vulnerable elderly head and neck cancer patients treated with radio(chemo)therapy. J Geriatr Oncol 2012; 3: 24–32. [Google Scholar]
- 66. Braun T, Gruneberg C, Thiel C. German translation, cross‐cultural adaptation and diagnostic test accuracy of three frailty screening tools: PRISMA‐7, FRAIL scale and Groningen Frailty Indicator. Z Gerontol Geriatr 2018; 51: 282–292. [DOI] [PubMed] [Google Scholar]
- 67. Xiang W, Cheng Y, Li Z et al Cross‐cultural adaptation and validation of the Groningen Frailty Indicator in Chinese nursing home residents. Aging Clin Exp Res 2019; Online ahead of print. https:/doi.org/10.1007/s40520‐019‐01178‐7. [DOI] [PubMed] [Google Scholar]
- 68. Hamaker ME, Seynaeve C, Wymenga AN et al Baseline comprehensive geriatric assessment is associated with toxicity and survival in elderly metastatic breast cancer patients receiving single‐agent chemotherapy: results from the OMEGA study of the Dutch breast cancer trialists' group. Breast 2014; 23: 81–87. [DOI] [PubMed] [Google Scholar]
- 69. Linos E, Chren MM, Covinsky K. Geriatric dermatology‐a framework for caring for older patients with skin disease. JAMA Dermatol 2018; 154: 757–758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Bras L, Peters TT, Wedman J et al Predictive value of the Groningen Frailty Indicator for treatment outcomes in elderly patients after head and neck, or skin cancer surgery in a retrospective cohort. Clin Otolaryngol 2015; 40: 474–482. [DOI] [PubMed] [Google Scholar]
- 71. Valdatta L, Perletti G, Maggiulli F et al FRAIL scale as a predictor of complications and mortality in older patients undergoing reconstructive surgery for non‐melanoma skin cancer. Oncol Lett 2019; 17: 263–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Hamaker ME, Vos AG, Smorenburg CH et al The value of geriatric assessments in predicting treatment tolerance and all‐cause mortality in older patients with cancer. Oncologist 2012; 17: 1439–1449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Rodriguez‐Manas L, Feart C, Mann G et al Searching for an operational definition of frailty: a Delphi method based consensus statement: the frailty operative definition‐consensus conference project. J Gerontol A Biol Sci Med Sci 2013; 68: 62–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Systematic literature search to identify frailty screening tools.
Table S2. List of relevant websites and organizations included in the systematic search to identify frailty screening tools.
Table S3. Statements as presented in round 2 of the modified Delphi procedure on the requirements a frailty screening tool should fulfil in older dermato‐oncology patients.
Table S4. Sensitivity and specificity of the included frailty screening tools.
Figure S1. Flow‐chart of the systematic search to identify frailty screening tools.